
Abstract
Objective:
To evaluate the efficacy and safety of ketamine or ketorolac compared to opioids in painful vaso-occlusive crisis (VOC).
Data resources:
A systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) criteria and used Embase, MEDLINE, and Cochrane Central to obtain data that evaluated the efficacy and safety of ketamine or ketorolac compared to opioids in acute painful VOC in July of 2025.
Study selection and data extraction:
The primary endpoints were meaningful reduction of pain on pain scales, reduction in opioid requirements, and the incidence of adverse effects reported in the studies. A P-value of <0.05 was considered statistically significant, and heterogeneity among the studies was reported as the I2 value.
Data synthesis:
Eight randomized controlled trials were included. Ketorolac showed a statistically significant pain reduction compared to opioids (standard mean difference [SMD]: 0.58 [95% CI: 0.31-0.85, P < 0.0001]), whereas ketamine showed no statistically significant difference in pain reduction (MD: −0.17 [95% CI: −0.53 to 0.18, P = 0.34]). A statistically significant reduction in opioid requirements was demonstrated in both intervention groups (MD: 3.23 [95% CI: −4.40 to −2.06, P < 0.0001]). Regarding safety, ketorolac showed a lower risk of adverse effects compared to opioids (risk ratio [RR]: 0.54 [95% CI: 0.36-0.79, P = 0.0019]), while ketamine demonstrated a higher risk of adverse effects (RR: 9.90 [95% CI: 4.30-22.82, P < 0.0001]).
Relevance to patient care and clinical practice:
Ketamine or ketorolac demonstrated effective reduction in pain and opioid requirements, with ketorolac showing a greater pain relief and a favorable safety profile compared to ketamine. These findings demonstrate their use as either nonopioid analgesics or opioid-sparing agents.
Conclusion:
Ketamine or ketorolac may not only reduce opioid requirements but may also serve as nonopioid treatment options, supporting safer and individualized pain-management strategies in painful VOC.
Background
Sickle cell disease (SCD) is a common genetic blood disorder of the hemoglobin that impacts millions of people worldwide. 1 It is prevalent among individuals with ancestry from regions where malaria is common including Sub-Saharan Africa, South Asia, Middle East, and Mediterranean regions. 1 Approximately 100,000 people in the United States have SCD. 1 It occurs in approximately 1 out of every 365 Black or African American births. 1
Vaso-occlusive crisis (VOC) is a common complication of SCD. It happens when sickled red blood cells aggregate together and interact with other blood cells, including leukocytes, as well as the vascular endothelial cells resulting in VOC. 2 Given the disruption of blood flow to tissues and organs, this occlusion leads to serious complications such as acute episodes of pain which have various intensity and frequency. 2 Pain can take place in any part of the body but commonly the extremities, back and chest areas. 3 In the United States, over 230,000 hospital admissions are associated with SCD annually and 95% of them are related to VOC. 4
As part of a standardized protocol, the American Society of Hematology (ASH) suggests personalized opioid dosing for adults and children presenting with acute painful VOC, for whom opioid therapy is indicated, based on baseline opioid therapy and previous effective therapy. 5 In terms of nonopioid therapies, ASH suggests a short course, 5 to 7 days, of nonsteroidal anti-inflammatory drugs (NSAIDs) in addition to opioids for acute pain management. 5 NSAIDs offer low to moderate potential benefits in acute painful VOC such as improved pain control, reduced opioid use, and decreased length of stay. 5 Ketorolac is a NSAID that exhibits analgesic activity mediated by peripheral effects. 6 It acts more potently against Cyclooxygenase-1 (COX-1) than Cyclooxygenase-2 (COX-2). 7 In addition, ketorolac is indicated for the short-term management of moderately severe acute pain, up to 5 days, that requires analgesia at the opioid level. 6 It is important to note that ketorolac has a black box warning stating that its use is not indicated for pediatrics, however, it is commonly used off-label in this population. 6 Before initiating NSAID therapy, it is critical to consider individual assessment of risk including renal, vascular, and gastrointestinal (GI) toxicity. 5 In addition, potential risks during pregnancy should be cautiously evaluated before considering NSAID therapy. Patients with history of peptic ulcer disease, renal dysfunction, or on full-dose anticoagulation, as well as pregnant patients, are at increased risk for adverse effects. In these populations, the benefit of NSAIDs may not outweigh the risk. A single retrospective study of 197 children/adolescents with acute painful VOC who received ketorolac for pain, 33 of them experienced acute kidney injury (AKI) following ketorolac administration. It was concluded in the study that both total days and doses of ketorolac were associated with AKI. 8
For hospitalized adults and children with acute painful VOC, ASH suggests a subanesthetic ketamine infusion as adjunctive treatment of pain that is refractory with opioids alone. 5 Ketamine binds to N-methyl-D-aspartate (NMDA) receptors in the central nervous system, interacts with opiate receptors at central and spinal sites, and interacts with norepinephrine, serotonin, and muscarinic cholinergic receptors. 9 The potential benefits of subanesthetic ketamine in improving pain control and reducing opioid use are small to moderate. 5 In terms of safety, ketamine was associated with central nervous system depression effects including nystagmus, visual hallucinations, dizziness and dysphoria. 5 The effect at NMDA receptors may be responsible for the analgesic as well as psychiatric effects of ketamine. 9
Ketamine or ketorolac has conditional recommendations based on very low certainty in the evidence about efficacy. 5 There is a lack of high-quality data in the current literature regarding the efficacy and safety of ketamine or ketorolac in acute painful VOC episodes. In general, patients presenting with acute VOC are typically managed with opioids. 10 Opioids may have risks associated with tolerance and addiction in patients with frequent pain crises and may lead to serious complications including respiratory depression. Given the fact that opioids can cause respiratory depression, their use during painful VOC episodes has been associated with the risk of acute chest syndrome, which is the leading cause of early mortality in these patients.11,12 Thus, the objective of this study was to evaluate the efficacy and safety of ketamine or ketorolac compared to opioids in acute painful VOC management.
Methods and Materials
Trial Selection and Search Strategy
This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) criteria to identify randomized controlled trials evaluating the use of ketamine or ketorolac in acute VOC. 13 A comprehensive search strategy was conducted in July of 2025 through Embase, MEDLINE, and Cochrane Central Register of Controlled Trials. The search strategy was constructed with the assistance of an experienced research librarian and consisted of subject headings, keywords, and phrases related to the research topic. A summary of the search terminology can be found in Supplementary Appendix Table 1.
Eligibility Criteria
Inclusion criteria for study selection included randomized controlled trials evaluating the efficacy and safety of ketamine or ketorolac compared to opioids in patients diagnosed with acute painful VOC. Exclusion criteria included non-randomized studies, studies that looked at these agents in non-VOC pain, and studies exploring these agents as adjunctive form of a multimodal analgesia regimen. Figure 1 illustrates the search strategy and literature identification methodology.
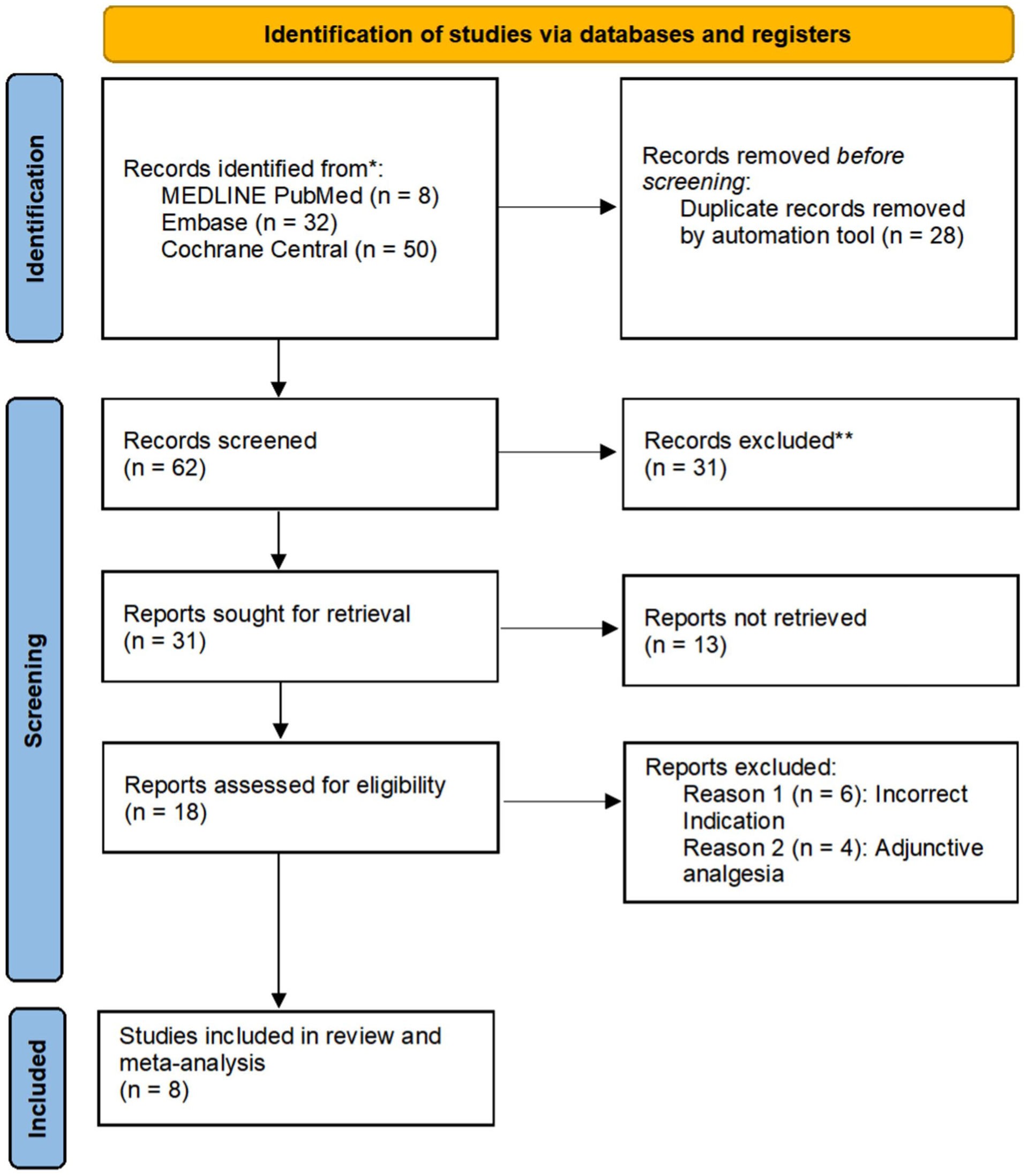
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. 13
Efficacy and Safety Endpoints
Meaningful pain reduction on pain scales and reduction in opioid requirements, defined as morphine milligram equivalents (MME), were considered efficacy endpoints. Safety endpoint included the incidence of adverse effects reported by the authors in the studies.
Data Extraction and Quality Assessment
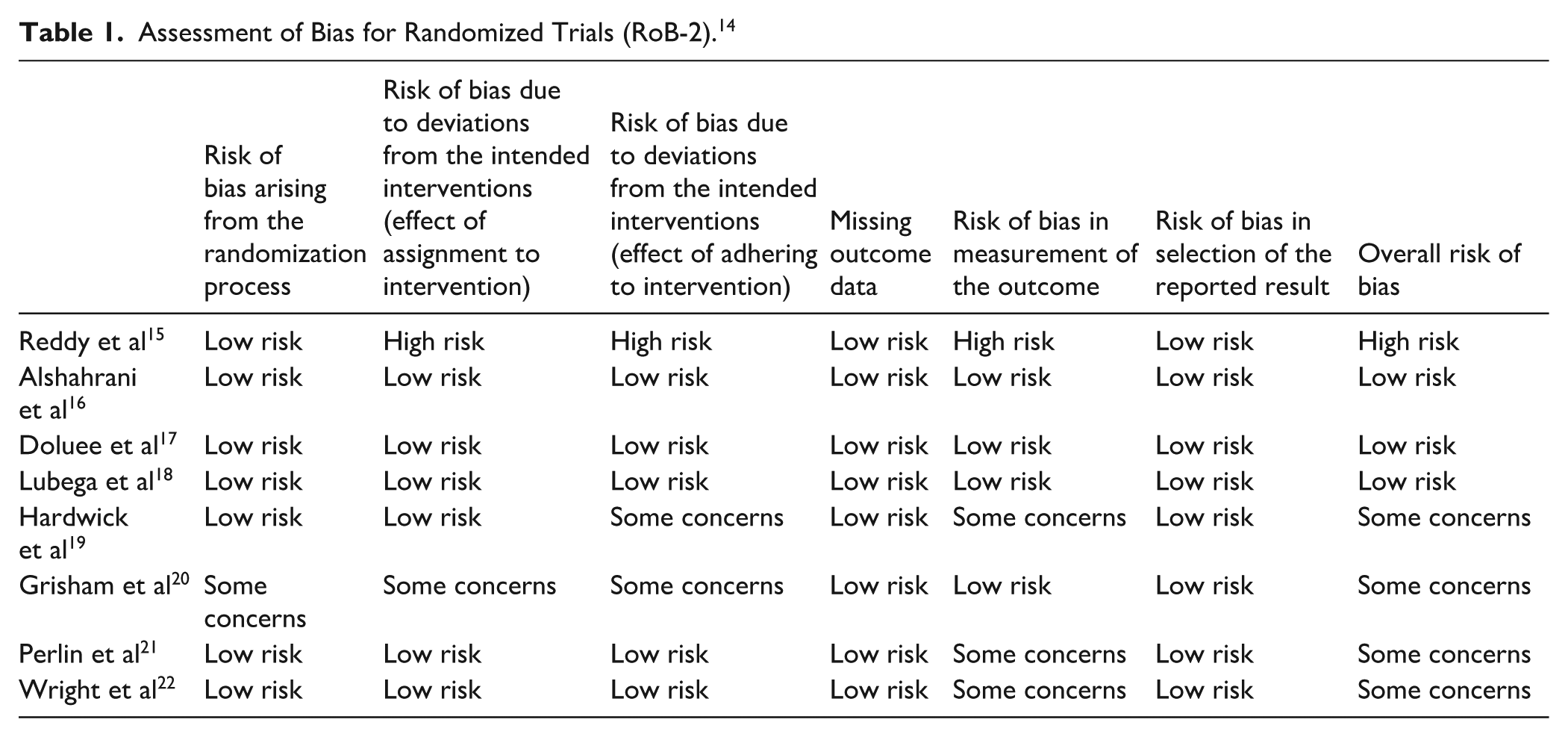
The literature review, analysis, and bias screening were conducted by both authors (MMS and JPR) who independently reviewed each study for bias and mutually agreed on all bias assessments. The risk of bias was calculated using the Risk of Bias Tool for Randomized Trials (RoB-2) which can be found in Table 1. 14
Assessment of Bias for Randomized Trials (RoB-2). 14
Statistical Analysis
A meta-analysis was conducted using Meta-Mar (v4.2.0). 23 Meaningful pain reduction on pain scales, reduction in opioid requirements, and reported safety outcomes were analyzed. A P-value of <0.05 was considered statistically significant. Heterogeneity amongst the studies was reported as the I 2 value. The efficacy endpoints were analyzed through a continuous outcomes analysis. The standard mean difference (SMD) was reported for meaningful pain reduction with ketorolac, and the mean difference (MD) was reported for both meaningful pain reduction with ketamine and reduction in opioid requirements endpoints. SMD was used to analyze meaningful pain reduction with ketorolac to account for differing input variables, as the pain scales utilized among the ketorolac studies varied. Safety events were counted in aggregate, and safety data was analyzed through a binary outcomes analysis and reported as the relative risk.
Efficacy Data Calculations
For meaningful pain reduction on pain scales, the standard deviation (SD) of change was calculated using an online calculator (Meta-Converter), and the results were verified using the SD of change formula.24,25 In the study by Perlin et al, SD was not reported for pre- and post-treatment pain scores, but confidence interval was provided with a range. SD was calculated from the confidence interval using the standard error formula and then multiplied by the square root of the sample size to calculate the SD. For reduction in opioid requirements, all reported opioid mean doses were standardized to MME using conversion factors to allow for direct comparison across different opioid agents.26,27
The studies included in our analysis used different pain scales. To account for this variation, we established thresholds for clinically meaningful pain reduction for each pain scale. For visual analog scale (VAS) 100 mm, a reduction of 13 mm or more in pain is considered to be clinically meaningful. 28 A reduction of 3 cm or more is considered to be a clinically meaningful reduction in VAS 10 cm, corresponding to 30% decrease or more from baseline. 29 For numerical pain rating score (NPRS), a reduction of 3 points or more in pain is considered to be clinically meaningful as well as for facial pain scale (FPS), capturing at least 30% reduction from baseline as well. 29
Results
After initial screening and removal of duplicates, 18 randomized controlled trials (RCTs) were identified and assessed for eligibility. Out of the 18 studies, 8 were included in this systematic review and meta-analysis based on inclusion and exclusion criteria. Of those 8 RCTs, 2 are related to ketamine in acute painful VOC compared to morphine.16,18 The other 6 RCTs investigated ketorolac in acute painful VOC in comparison with opioids.15,17,19-22 The 8 included studies were compromised of 748 patients including pediatrics and adults. Four of these studies were conducted in pediatric populations.18,15,19,20 One study compared ketorolac to morphine in pediatrics who presented with acute painful VOC. 15 Another study compared ketorolac to placebo (IV normal saline) in pediatric patients with morphine provided initially and as needed based on the patients’ acute VOC pain severity during a 6-hour observation period. 19 One study compared ketorolac to meperidine in pediatric patients with acute painful VOC. 20 Additional two studies compared ketorolac to placebo (IV normal saline) in adults, with meperidine administered as needed.21,22 Alshahrani et al 16 compared ketamine to morphine in adults with acute VOC, while Lubega et al 18 compared low-dose ketamine to morphine in pediatrics with acute VOC. Table 2 summarizes the efficacy and safety outcomes from the eight RCTs evaluating the use of ketamine or ketorolac in acute painful VOC management.
Summary of Efficacy and Safety Outcomes.
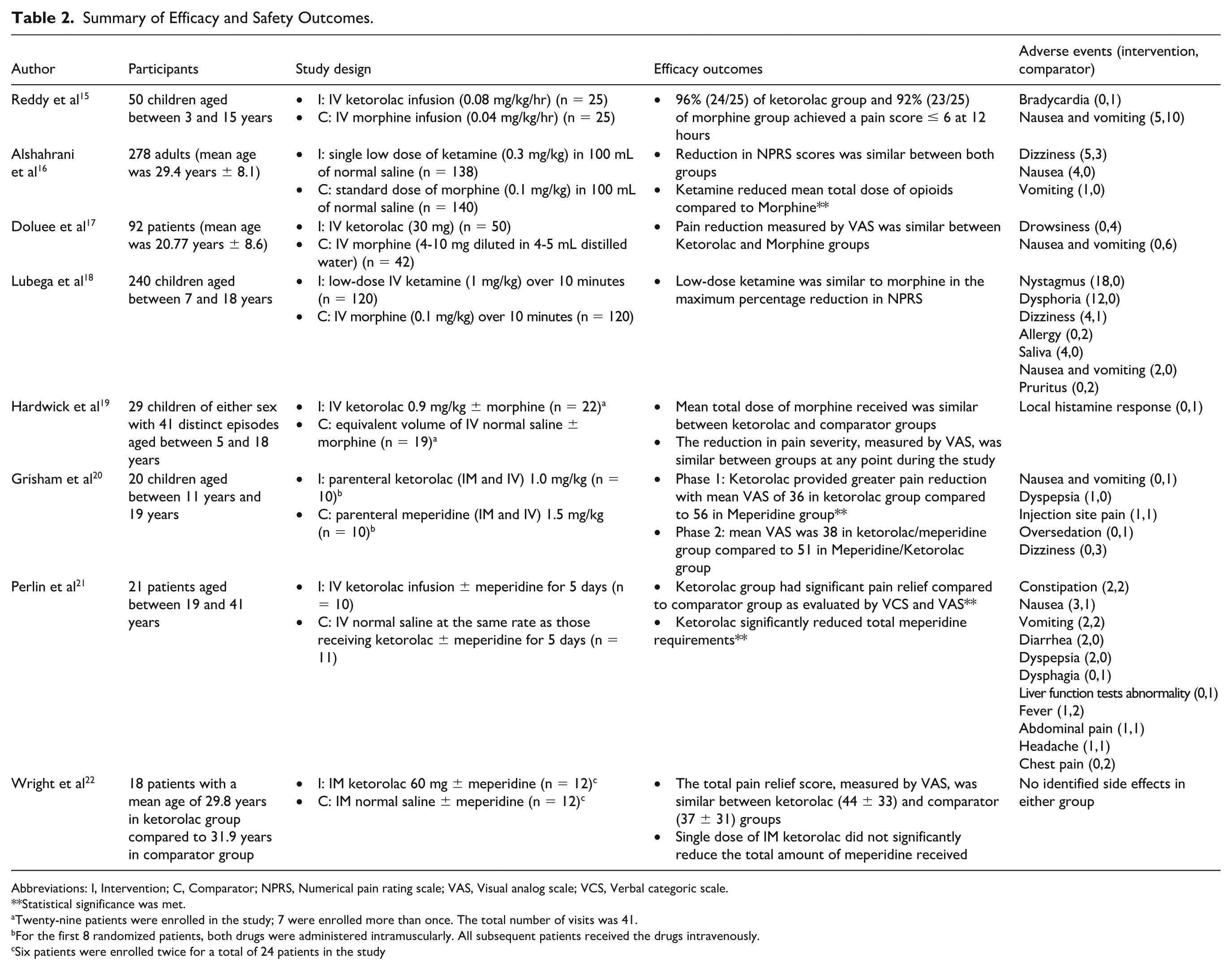
Abbreviations: I, Intervention; C, Comparator; NPRS, Numerical pain rating scale; VAS, Visual analog scale; VCS, Verbal categoric scale.
Statistical significance was met.
Twenty-nine patients were enrolled in the study; 7 were enrolled more than once. The total number of visits was 41.
For the first 8 randomized patients, both drugs were administered intramuscularly. All subsequent patients received the drugs intravenously.
Six patients were enrolled twice for a total of 24 patients in the study
Subgroup analyses were conducted to assess the efficacy of ketamine or ketorolac compared with opioids in meaningful pain reduction on pain scales. Alshahrani et al 16 and Lubega et al 18 were the two RCTs included in the ketamine subgroup analysis. The mean difference (MD) in pain reduction was −0.17 (95% CI: −0.53 to 0.18, P = 0.3413), showing no statistically significant difference between ketamine and opioid groups in meaningful pain reduction as illustrated in Figure 2. There was no observed heterogeneity between studies, demonstrating consistency in the results. In contrast, 5 RCTs were included in the ketorolac subgroup analysis.15,17,19,21,22 The analysis showed a statistically significant reduction in pain with ketorolac compared to opioid groups with an SMD of 0.58 (95% CI: 0.31-0.85, P < 0.0001), as shown in Figure 2. The findings were consistent throughout the studies, as evidenced by the low heterogeneity.
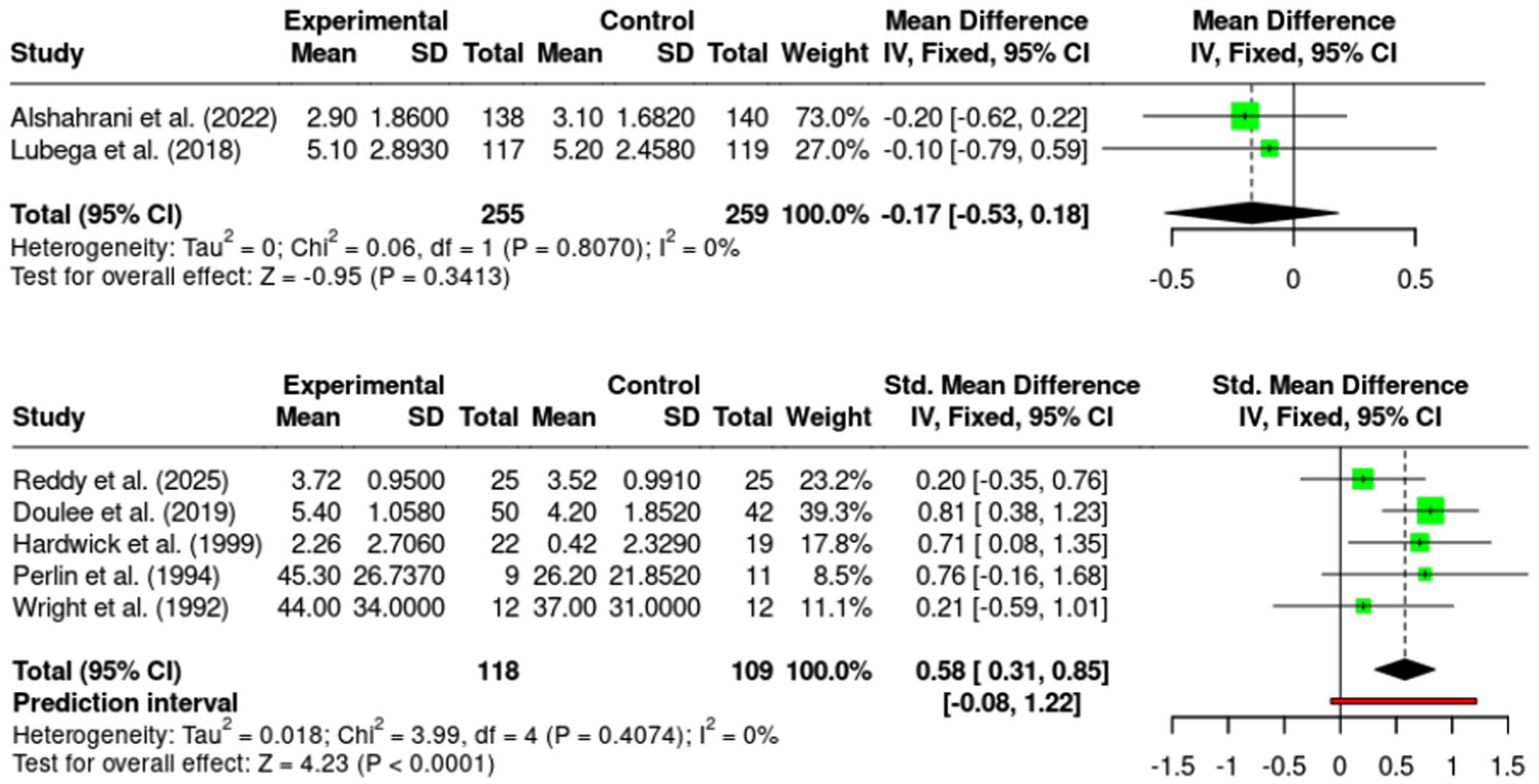
Subgroup analyses of meaningful pain reduction from pain scales of ketamine or ketorolac versus comparator.
Four studies were included in the analysis evaluating the reduction in opioid requirements following treatment with ketamine or ketorolac in patients with acute painful VOC. Alshahrani et al assessed ketamine, while the remaining 3 studies assessed ketorolac for this efficacy endpoint. This meta-analysis showed that ketamine or ketorolac significantly reduced opioid requirements. The mean difference was −3.23 (95% CI: −4.40 to −2.06, P < 0.0001) demonstrating a significant opioid-sparing effect, as demonstrated in Figure 3.
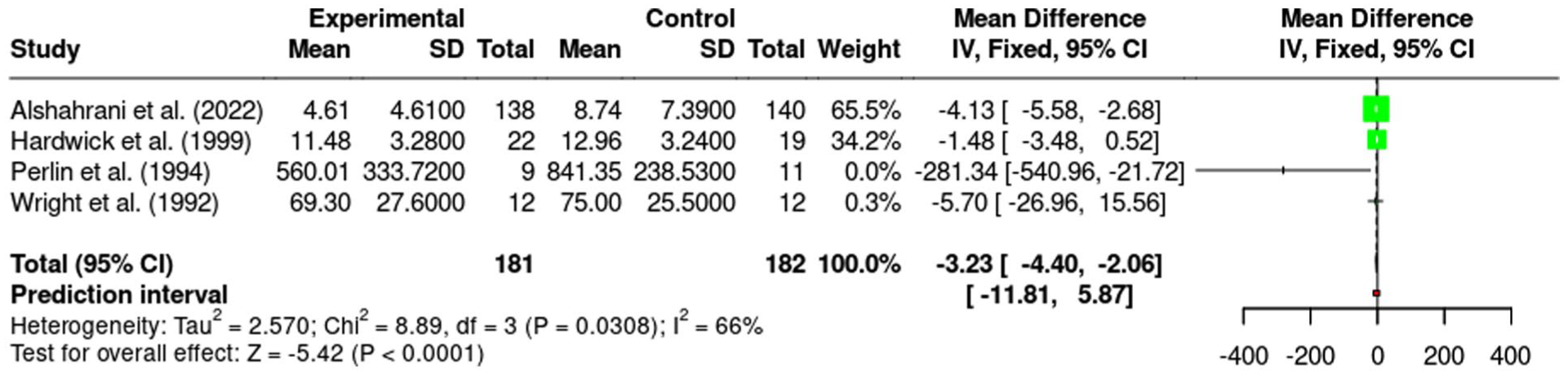
Meta-analysis of reduction in opioid use following treatment with ketamine or ketorolac versus comparator.
A subgroup analysis was conducted to evaluate the risk of adverse effects of ketorolac compared to opioid groups. The overall risk ratio (RR) was 0.54 (95% CI: 0.36-0.79; P = 0.0019), indicating a statistically significant lower risk of adverse effects with ketorolac as shown in Figure 4. Both GI adverse effects and nausea and vomiting subgroups showed statistically significant lower risks with ketorolac with RR of 0.53 (P = 0.0445) and 0.52 (P = 0.0438), respectively. In contrast, dyspepsia subgroup analysis did not show a statistically significant difference across both groups with a greater RR of 4.20 (P = 0.1817).
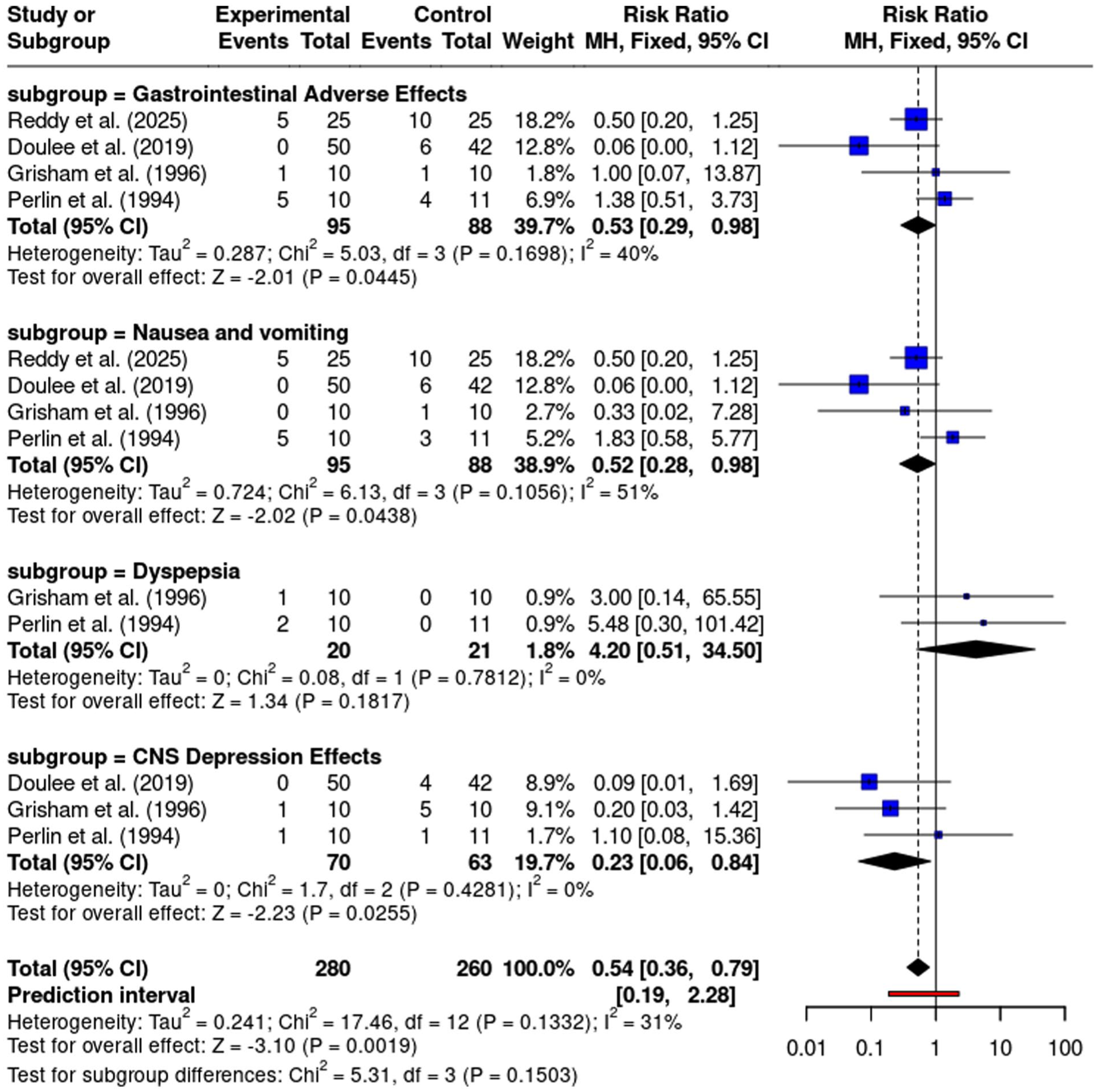
Subgroup analysis of safety outcomes of ketorolac versus comparator.
This subgroup analysis, shown in Figure 5, was conducted to assess the risk of adverse effects of ketamine compared to opioid groups. The overall RR was 9.90 (95% CI: 4.30-22.82, P < 0.0001), showing a statistically significant higher risk of adverse effects with ketamine. The RRs were 12.08 (P = 0.0163) for GI adverse effects, 8.07 (P = 0.0481) for nausea and vomiting, and 9.81 (P < 0.0001) for CNS depression effects. It should be noted that there was significant heterogeneity in the CNS depression effects subgroup.
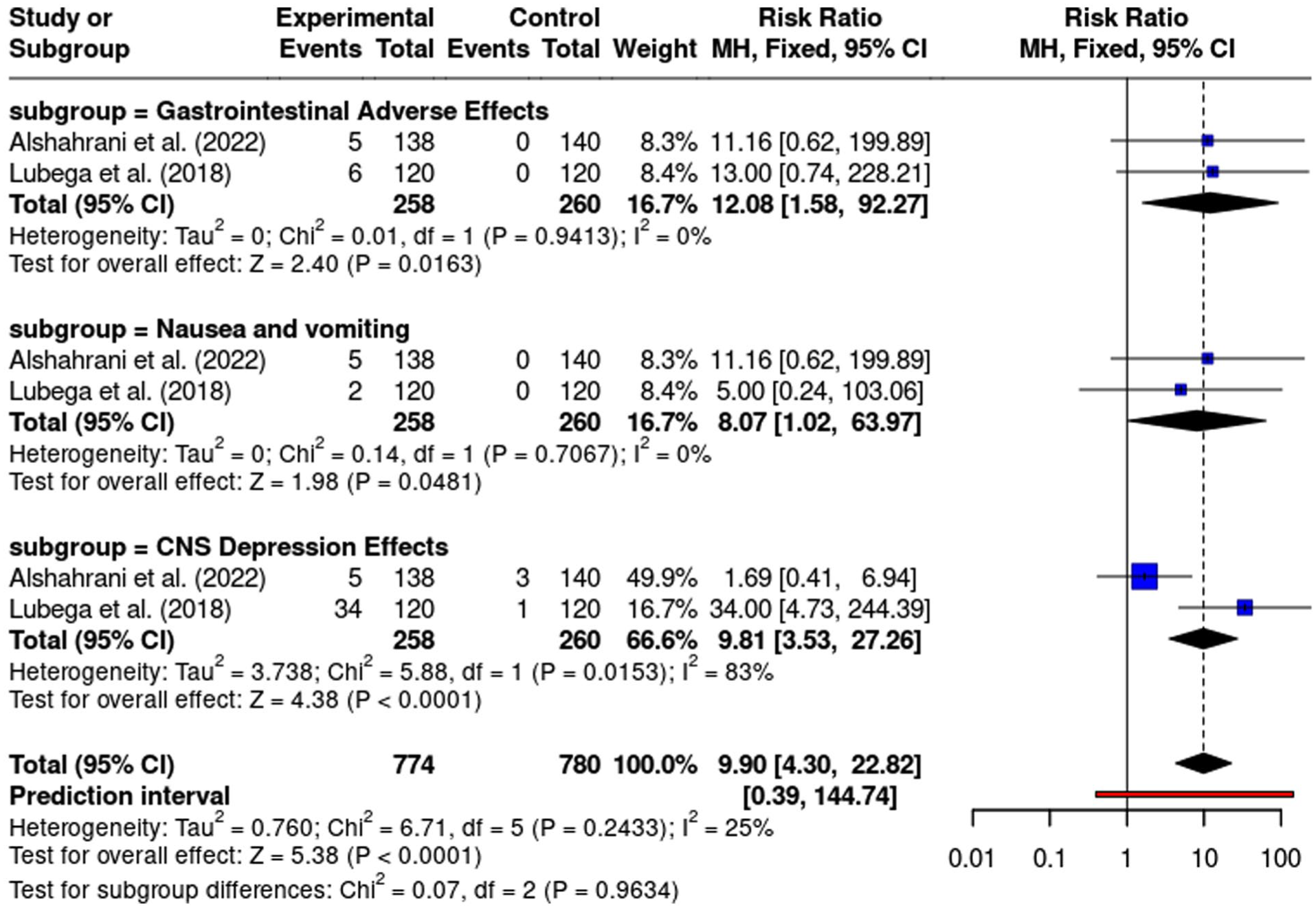
Subgroup analysis of safety outcomes of ketamine versus comparator.
Discussion
This systematic review and meta-analysis evaluated the efficacy and safety of ketamine or ketorolac as potential nonopioid treatment options in patients with acute painful VOC. There is a growing interest in effective and safe nonopioid analgesics given the risks associated with opioids including risk of tolerance, dependence, and adverse effects such as acute chest syndrome in patients with SCD.11,12,30 The findings in this systematic review and meta-analysis provide valuable insights into the role of ketorolac or ketamine in acute painful VOC management and lowering the risks associated with chronic opioid use. The results show that both agents have potential benefits in pain relief and opioid use reduction, but they have different safety profiles that need to be carefully considered in a clinical setting.
With regard to safety analyses, it is important to emphasize that GI adverse effects that were reported across the studies included nausea and vomiting, liver function tests abnormality, salivation, dyspepsia, dysphagia, diarrhea, and constipation. Subgroup analysis of GI adverse effects was conducted focusing on nausea and vomiting and dyspepsia as these adverse effects were consistently reported in at least two studies. Nausea and vomiting adverse effects were reported across all the studies included in the safety analyses, while dyspepsia was reported in two ketorolac studies. Central nervous system (CNS) adverse effects including nystagmus, dizziness, drowsiness, dysphoria, oversedation, and headache were grouped under CNS depression effects in the analysis.
Ketamine showed comparable success in pain reduction to morphine in acute painful VOC management in both RCTs included in this analysis.16,18 In addition, it demonstrated a significant reduction in opioid requirements supported by Alshahrani et al. 16 The study showed that low-dose ketamine (0.3 mg/kg) significantly reduced total opioid requirements in adults, despite that the differences in pain reduction between both groups were not statistically significant. Lubega et al 18 demonstrated comparable pain reduction between ketamine (1mg/kg) and morphine in pediatrics with severe VOC. In a 2024 retrospective study from 22 pediatric patients admitted with painful episodes of SCD and were administered subanesthetic ketamine infusion, Onyebuchi et al 31 reported that ketamine significantly reduced pain scores and opioids requirements, with most patients experiencing pain relief within 24 hours, and it was tolerated well with no discontinuation due to adverse effects. Onyebuchi et al 31 also reported that ketamine infusion was started at 0.05 to 0.15 mg/kg/hr with a maximum dose of 0.5 mg/kg/hr or 1 mg/kg/hr with the approval of acute pain treatment service. An additional retrospective study by Nobrega et al 32 investigated subanesthetic ketamine infusions, started at 0.05 to 0.4 mg/kg/hr up to 1 mg/kg/hr, combined with opioids in patient with painful VOC. Findings showed that ketamine combined with opioids led to significant decrease in pain scores and opioid consumption. 32 Neri et al 33 suggested that low-dose ketamine could be a useful adjuvant to opioid in patients with refractory SCD-related pain which aligns with ASH recommendation of using subanesthetic ketamine in refractory VOC pain to opioids. 5 A 2022 retrospective study that evaluated the use of low-dose ketamine infusion in 7 pediatric patients with refractory SCD-related pain by Yu et al 34 reported that ketamine had a median of 32% reduction in overall pain scores. In summary, the findings of these retrospective studies support the efficacy outcomes, reductions in pain and opioid requirements, of ketamine reported in this analysis. It is important to note that the two RCTs included in this analysis assessed ketamine at doses ranging from 0.3 to 1 mg/kg and the retrospective studies reported similar dosing ranges (0.05-1 mg/kg), which align with the efficacy findings from the RCTs.
Although ketamine poses effective analgesic benefits in patients with acute painful VOC, there are concerns regarding its safety. The subgroup analysis of safety outcomes of ketamine compared to morphine showed a significantly increased risk of adverse effects, especially GI adverse effects and CNS depression effects including dizziness, drowsiness, dysphoria, and nystagmus. Ketamine had a higher incidence of CNS adverse effects in Lubega et al 18 study. In Alshahrani et al 16 study, ketamine was associated with mild, transient adverse effects including dizziness and nausea and vomiting. Onyebuchi et al 31 reported that patients who received ketamine experienced hallucinations in 11 admissions. On the other hand, Yu et al 34 reported that subanesthetic ketamine infusion was not associated with significant psychotropic effects or hemodynamic adverse effects. Ketamine’s onset of action is rapid and often occurs within a few minutes following drug administration. 35 The effects of ketamine are dose dependent and may include dizziness, nausea, vomiting, confusion, or disorientation. 36 Despite that most adverse effects were transient across the studies, their occurrence may limit ketamine’s use in select patient populations, especially those with underlying neurological or psychiatric conditions.
Overall, the evidence supports the efficacy of ketamine in the management of painful VOC, showing comparable analgesic benefits to opioids with the added benefit of reducing opioid requirements. Given ketamine’s safety profile, it may be considered either as a second-line alternative when used as monotherapy or as an adjunct in patients already receiving opioids. It should be administered with careful dose selection due to its dose-dependent safety profile. Based on personalized risk assessment and clinical judgment, there are likely situations where the benefit of ketamine outweighs the risks, making it a viable treatment option.
Ketorolac showed statistically significant efficacy in reducing both pain on pain scales and opioid requirements in acute painful VOC episodes. Of the 6 ketorolac studies included, 3 were conducted in pediatric patients including those by Reddy et al, 15 Hardwick et al, 19 and Grisham and Vichinsky. 20 Reddy et al 15 investigated IV ketorolac infusion at a rate of 0.08 mg/kg/hr. Hardwick et al 19 evaluated IV ketorolac given as a single injection at 0.9 mg/kg. On the other hand, Grisham and Vichinsky 20 evaluated both IM and IV routes, each given as a single injection at 1.0 mg/kg, in pediatric patients. In the study by Grisham et al, it is important to note that the first eight patients received ketorolac or meperidine intramuscularly, and all subsequent patients received the drugs intravenously. The remaining three studies were conducted in adult patients including those by Doluee and Kakhki, 17 Perlin et al, 21 and Wright et al. 22 Doluee and Kakhki 17 evaluated IV ketorolac at a dose of 30 mg injection, while Wright et al 22 investigated IM ketorolac at a dose of 60 mg injection. In the study by Perlin et al, 21 patients allocated to ketorolac received an IV loading dose of 30mg followed by an infusion of 120 mg at 5 mg/hr, for a total dose of 150 mg on the first day; for the remainder of the study, patients received 120 mg/day. When analyzing the studies involving ketorolac, it demonstrated similar efficacy to comparators (morphine or meperidine) in meaningful pain reduction in Reddy et al, 15 Doluee and Kakhki, 17 Hardwick et al, 19 and Wright et al 22 studies. However, it showed greater pain reduction compared to meperidine in Grisham et al and Perlin et al studies. In Wright et al, 22 ketorolac did not reduce the total dose of meperidine received compared to Perlin et al 21 that showed significant reduction in total meperidine received. In the study by Hardwick et al, 19 the mean total dose of morphine received was similar between both ketorolac and comparator groups. Additional observational studies support these findings. A descriptive study by Mach et al 37 that evaluated the use of a single-dose IV ketorolac 0.5 mg/kg injection in 25 children admitted to the emergency department with acute SCD-related pain showed improvement in pain scores following ketorolac administration. A prospective case series by Beiter et al 38 included 51 children presenting with 70 painful VOC episodes that were given either IV ketorolac or IV ketorolac with opioids as needed. All patients received 0.5 to 1.0 mg/kg IV ketorolac and IV fluids. Ketorolac resulted in adequate resolution of pain in 53% of episodes. 38 The consistent reduction in pain scores and opioid requirements demonstrated with ketorolac use in acute painful VOC is clinically significant. These findings are further supported by retrospective studies, showing similar reductions in pain and opioid requirements. Therefore, ketorolac appears to be an effective nonopioid treatment option in acute painful VOC management, potentially reducing the risk of opioid-related complications. It should be emphasized that across the included studies, IV ketorolac dosing varied, with pediatric studies evaluating infusion regimen at 0.08 mg/kg/hr and single IV ketorolac injections ranging from 0.5 to 1.0 mg/kg, while adult studies investigated fixed IV or IM doses of 30 mg or 60 mg or infusion regimen totaling up to 120 mg/day.
In terms of safety, ketorolac showed a significantly lower risk of adverse effects compared to comparators. Specifically, it demonstrated a lower risk of GI adverse effects, except for dyspepsia, and CNS depression effects as discussed and illustrated in results section and Figure 4. GI symptoms such as nausea and vomiting and dyspepsia were reported but did not lead to discontinuation of ketorolac. It should be emphasized that two studies, Hardwick et al and Wright et al, were not included in the safety analysis. Hardwick et al 19 reported one local histamine response in comparator group, but no other adverse effects were identified. In addition, Wright et al 22 had not identified adverse effects in both intervention and comparator groups. Ketorolac is a safer option for patients with pulmonary comorbidities or at risk of CNS depression compared to opioids and ketamine. SCD changes renal structure and function and causes different renal diseases. 39 NSAIDs are associated with nephrotoxicity, especially when used chronically. 40 A retrospective study assessed the risk of AKI among 253 pediatric patients admitted for painful VOC between 2014 and 2022 and showed that the incidence of AKI was 1.1% in patients who received ketorolac and was not associated with ketorolac dose. 41 Ketorolac showed a favorable short-term safety profile and minimal risk of AKI in patients with SCD when used appropriately. The safety data supports the use of ketorolac as a safe nonopioid analgesic option in acute painful VOC management with consideration of renal function. Despite the FDA’s black box warning against its use in pediatrics, the safety outcomes from this analysis and the retrospective study support the clinical use of ketorolac.
Collectively, the evidence supports the efficacy of ketorolac in the management of painful VOC, demonstrating comparable analgesic benefits to opioids, and in some cases greater benefits. The evidence also supports the additional benefit of ketorolac in reducing opioid requirements. Given ketorolac’s favorable safety profile, it may be used as a nonopioid treatment option in acute painful VOC or as an adjunct in patients already receiving opioids with careful monitoring of renal function.
Several limitations were recognized in this study. All systematic reviews and meta-analyses have limitations due to potentially excluding or not identifying all relevant topics. Some studies had moderate to high heterogeneity due to differences in dosage and patient populations. Moreover, most studies had short durations and small sample sizes, limiting the generalizability and strength of the conclusions. Variations in pain scale measurements across the studies led to complications in drawing conclusions and it required careful interpretation of the results. Furthermore, reduction in opioid requirements endpoint had a single ketamine study, limiting the strength of the evidence regarding this outcome.
Relevance to Patient Care and Clinical Practice
This systematic review and meta-analysis highlights the evidence regarding the efficacy and safety of ketamine or ketorolac in acute pain VOC management. Ketamine demonstrated comparable analgesic effects to opioids along with additional benefits as opioid-sparing agent. However, clinicians must weigh the analgesic benefits versus CNS-related adverse effects, especially in patients with underlying psychiatric or neurological conditions. Thus, ketamine can be utilized as an adjunct to opioids in opioid-tolerant patients or as a second-line therapy in patients experiencing recurrent, severe painful VOC episodes despite opioid management.
Similarly, ketorolac demonstrated comparable analgesic benefits to opioids or even greater to opioids in some cases. It also demonstrated efficacy as an opioid-sparing agent. Despite the black box warning against its use in pediatric population, the evidence from RCTs and retrospective studies supports its safe clinical use in this population with appropriate patient monitoring. Ketorolac appears to be an appropriate option for patients with recurrent acute pain VOC despite chronic opioid therapy, as well as patients at high risk of acute chest syndrome or with existing or worsening neurological, psychiatric, or pulmonary conditions. Practitioners should weigh the analgesic benefits of ketorolac versus the renal and GI risks associated with it to optimize patient outcomes and reduce the incidence of adverse effects.
Conclusion
This systematic review and meta-analysis underlines the potential benefits of ketorolac or ketamine as efficacious analgesic treatment options and opioid-sparing agents in the management of acute painful VOC. Ketorolac or ketamine demonstrated improvement in pain relief and reduction in opioid requirements with ketorolac showing a more favorable safety profile than ketamine. Overall, the evidence supports ketamine or ketorolac as effective analgesics in acute painful VOC management, highlighting their role in current clinical practice as agents that may not only reduce opioids requirements but may also serve as nonopioid treatment options, supporting individualized pain management strategies while reducing opioid-related complications in patients with SCD.
Supplemental Material
sj-docx-1-aop-10.1177_10600280251380939 – Supplemental material for The Efficacy and Safety of Ketamine or Ketorolac Compared to Opioids in Painful Vaso-Occlusive Crisis: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-aop-10.1177_10600280251380939 for The Efficacy and Safety of Ketamine or Ketorolac Compared to Opioids in Painful Vaso-Occlusive Crisis: A Systematic Review and Meta-Analysis by May M. Shehata and Justin P. Reinert in Annals of Pharmacotherapy
Footnotes
Acknowledgements
The authors would like to recognize Wade Lee-Smith, BS, MLS, for his efforts in assisting with the systematic search strategy development and execution.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.