
Abstract
Objective:
To evaluate the efficacy and safety of mepolizumab, a humanized monoclonal antibody that targets interleukin-5, a key mediator in eosinophilic inflammation, in reducing moderate-to-severe exacerbations among patients with eosinophilic chronic obstructive pulmonary disease (COPD).
Data Sources:
PubMed, Scopus, Web of Science, and Cochrane databases were systematically searched using the terms: “Mepolizumab,” “COPD,” “Chronic Obstructive Pulmonary Disease,” for randomized controlled trials comparing subcutaneous mepolizumab (100 mg every 4 weeks) with placebo in patients with eosinophilic COPD from inception till July 2025.
Study Selection and Data Extraction:
Randomized controlled trials comparing subcutaneous mepolizumab with placebo in adults with eosinophilic COPD were included. Two independent reviewers screened studies and extracted data. Finally, 4 studies with a total of 1953 patients were included. Of these, 978 (50.0%) received mepolizumab.
Data Synthesis:
Statistical analysis was performed using R software (version 4.5.0). Mepolizumab significantly prolonged the time to first moderate or severe exacerbation (hazard ratio [HR] = 0.80; 95% confidence interval [CI] 0.69-0.92; P = 0.016) and reduced the rate of moderate-to-severe exacerbations (rate ratio 0.80; 95% CI 0.78-0.83; P < 0.001). The risk of adverse events (AEs) (risk ratio [RR] = 1.00; 95% CI 0.95-1.06; P = 0.962) was similar between groups, while the risk of serious adverse events or death (RR = 0.83; 95% CI 0.72-0.96; P = 0.031) was significantly lower in the mepolizumab group.
Relevance to Patient Care and Clinical Practice in Comparison With Existing Drugs:
Mepolizumab provides a targeted, biomarker-guided treatment option, potentially reducing exacerbations without the added safety concerns like infections and metabolic complications as seen with existing therapies.
Conclusion and Relevance:
Mepolizumab reduces the time to first moderate or severe exacerbation and prolongs symptom-free periods in patients with eosinophilic COPD, without increasing the risk of AEs.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms, such as dyspnea, cough, sputum production, and pulmonary exacerbations. 1 Despite significant advances in prevention and management strategies, COPD remains one of the foremost causes of death worldwide. 2 Patients admitted to health care facilities during exacerbations have a high in-hospital mortality rate and significant mortality during subsequent follow-up. 3 Among patients with stable COPD, up to 20% to 40% exhibit an eosinophilic phenotype, historically characterized by 2% or more eosinophils in the peripheral blood smear, a leukocyte count of approximately 150 to 300 eosinophils/μL 4 and sputum eosinophilia. 5 However, for the purpose of treatment, an absolute cut-off value of ≥300 cells/μL is generally used. 6 Eosinophilia has been associated with up to 28% of the exacerbations, ranking third after bacterial and viral clusters. 7 Elevated blood eosinophil counts correspond to increased eosinophil infiltration in the lungs, which is subsequently responsible for increased type 2 inflammatory markers, leading to airway remodeling, mucus plugging, and immune dysregulation. 8
Eosinophilic COPD is a biologically distinct phenotype characterized by heightened type 2 inflammation and airway eosinophilia. The evaluation of COPD longitudionally to identify predictive surrogate endpoints (ECLIPSE) study analyzed the association of blood eosinophil counts with exacerbations in COPD patients and demonstrated that higher blood eosinophil counts were associated with an increased risk of exacerbations. 5 In this context, interleukin (IL)-5 is an important factor responsible for recruitment, differentiation, survival, and degranulation of eosinophils in the airways. 9 It is the central cytokine responsible for the proliferation, activation, recruitment, and maturation of eosinophils in tissues. Along with other tissue factors, such as IL-4, IL-3, and IL-13, IL-5 causes degranulation of eosinophils, which releases major basic proteins, eosinophil cationic protein, eosinophil peroxidase, and eosinophil-derived neurotoxin. 8 These factors, in addition to providing defense against parasitic infections, also cause tissue injury, remodeling, and changes in the biochemical composition of mucus. 10 Mepolizumab, an IL-5 neutralizing monoclonal antibody, has well-established efficacy in eosinophilic asthma, and similar biological mechanisms have been demonstrated in COPD as well.11-14
From a pharmacological point of view, mepolizumab demonstrates a high receptor affinity and has a terminal half-life of 20 days, which helps in sustained suppression of circulating eosinophils. 15 Its selective binding to the soluble IL-5 inhibiting its ligation to IL-5Rα explains the relative lack of substantial side effects with mepolizumab. 16 This selective ligand affinity also probably explains the modulation of eosinophil response rather than complete depletion of eosinophils as observed with receptor targeting therapies, thereby preserving more physiological immune function.17,18
The role of mepolizumab in COPD with an eosinophilic phenotype was first studied in 2 phase-3 trials (METREX and METREO). 19 An analysis of these 2 trials concluded that COPD patients with eosinophilia were likely to benefit from add-on therapy with mepolizumab. 20 However, a previous meta-analysis has been conducted assessing the efficacy of biological treatment in COPD, and they performed a subgroup analysis of mepolizumab by pooling data from those 2 studies, METREX and METREO trials, and it did not demonstrate a reduction in exacerbation risk. 21 But Hu et al 21 did not limit their analysis to the eosinophilic phenotype of COPD and included all participants of the METREX trial, which did not have an eosinophil level cut-off in their inclusion criteria. The differences in the populations analyzed may have led to this conflicting outcome. Additional data have become available since. Two more randomized controlled trials (RCTs) demonstrated benefits when adding mepolizumab to standard background triple-inhaled therapy among patients with eosinophilic COPD.22,23 The 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report mentioned this conflicting evidence of mepolizumab on exacerbation reduction. 1
Therefore, considering emerging evidence, we conducted a systematic review and meta-analysis to assess the efficacy and safety of mepolizumab in the treatment of COPD patients expressing the eosinophilic phenotype.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Cochrane Collaboration Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines (Supplementary Material S1 and S2). 24 The protocol for this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251101907.
Search Strategy and Data Extraction
PubMed, Scopus, Web of Science, and Cochrane databases were systematically searched from inception to July 2025 for RCTs meeting the inclusion criteria. The search strategy included the terms: “Mepolizumab,” “COPD,” “Chronic Obstructive Pulmonary Disease.” The complete search strategy is provided in Supplementary Material S3. In addition, we analyzed abstracts from major pulmonology conferences held between 2021 and 2025, and references of included RCTs for potentially eligible studies. Two authors (R.B. and A.D.) independently assessed titles, abstracts, and full-text articles, while 2 authors (R.B. and E.M.M.C.) independently extracted baseline characteristics and outcomes based upon prespecified criteria. Discrepancies were resolved through consensus among all the authors. Baseline characteristics were reported as mean (± standard deviation) for continuous variables and as absolute numbers for categorical variables.
Eligibility Criteria
We included studies that met the following inclusion criteria: (1) RCTs, (2) evaluating patients diagnosed with eosinophilic phenotype COPD, (3) receiving add-on therapy with IL-5 inhibitor mepolizumab, (4) compared with placebo, and (5) reporting any outcomes of interest. Exclusion criteria were (1) nonrandomized studies, case series, case reports, editorials, reviews, or animal studies, (2) ongoing research or duplicate reports, (3) including asthma or asthma-COPD overlap populations, (4) with therapeutic interventions other than mepolizumab, or (5) studies with insufficient data.
For trials that enrolled both eosinophilic and noneosinophilic COPD populations (METREX), only data from the prespecified eosinophilic COPD subgroup were extracted and included in the meta-analysis. 19 The overall METREX population, which included patients without eosinophilic phenotype COPD, was not analyzed.
Endpoints and Sensitivity Analyses
The outcomes of interest were: time to first moderate or severe exacerbation, rate of moderate-to-severe exacerbations, rate of exacerbations leading to emergency department visit or hospitalization, incidence of adverse events (AEs) and serious adverse events (SAEs) (including death), and patient-reported outcomes using the St George’s Respiratory Questionnaire (SGRQ) and COPD Assessment Test (CAT).
An exacerbation was defined as moderate if it led to treatment with systemic glucocorticoids, antibiotics, or both, and as severe if it led to hospitalization for more than 24 hours or death. The definitions of AEs across studies have been explained in Supplementary Material S4. In patient-reported outcomes, an improvement in symptoms was defined by a minimal clinically important difference (MCID) of 2-point reduction from baseline to week 52 in the CAT scores (scores range from 0 to 40, with higher scores indicating worse health status) 25 and an MCID of 4 points reduction from baseline to week 52 in the SGRQ questionnaire (scores range from 0 to 100, with higher scores indicating worse health status). 26 Severity-specific (eg, GOLD stage) or prior-exacerbation-specific treatment effect estimates were not consistently reported across included trials and therefore could not be formally analyzed.
A prespecified leave-one-out (LOO) sensitivity analysis was also conducted to assess the heterogeneity of pooled estimates. Heterogeneity was assessed using the I² statistic, and a 2-tailed P value of <0.05 was considered statistically significant.
Quality Assessment
The Cochrane Risk of Bias (RoB) 2 27 tool was used to assess the included RCTs. Two authors independently conducted the assessment (R.B. and A.B.). Disagreements were resolved through consensus. Each study was evaluated in 5 domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcomes, and selection of reported results. Individual appraisal included scores of low, some concerns, or high RoB. Publication bias was assessed by funnel-plot analysis of point estimates according to study weights. 28
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was applied to assess the certainty of evidence of each outcome (very low, low, moderate, and high). 29
Statistical Analysis
Effect estimates were pooled using random-effects meta-analysis models. Risk ratios (RRs) were pooled using Mantel-Haenszel random-effects models based on event counts, while odds ratios (ORs), rate ratios, and hazard ratios (HRs) were pooled using inverse-variance random-effects models. Between-study heterogeneity variance (τ²) was estimated using the DerSimonian-Laird method. For inverse-variance models, the Hartung-Knapp adjustment was applied to derive random-effects confidence intervals. Statistical heterogeneity was assessed using Cochran’s Q test and quantified using the I2 statistic. I2 values of 0%, ≤25%, ≤50%, and >50% were interpreted as indicating no, low, moderate, and substantial heterogeneity, respectively. 30 A 2-sided P value <0.05 was considered statistically significant. 31 All statistical analyses were performed using R software (version 4.5.0).
Results
Study Selection and Characteristics
The initial literature search yielded 2575 articles. After the removal of duplicates and noneligible studies by title or abstract review, 19 articles remained. Full texts of these potentially eligible articles were screened for assessment. Sixteen studies were excluded during full-text screening. Finally, 3 studies, with 4 RCTs, were included in this meta-analysis.19,22,23 Pavord et al report 2 parallel, independently conducted randomized phase 3 trials, METREX and METREO, evaluating mepolizumab in eosinophilic COPD. Both trials were conducted under separate protocols with distinct randomization. 19 The PRISMA flow diagram of study screening and selection is detailed in Figure 1. 24
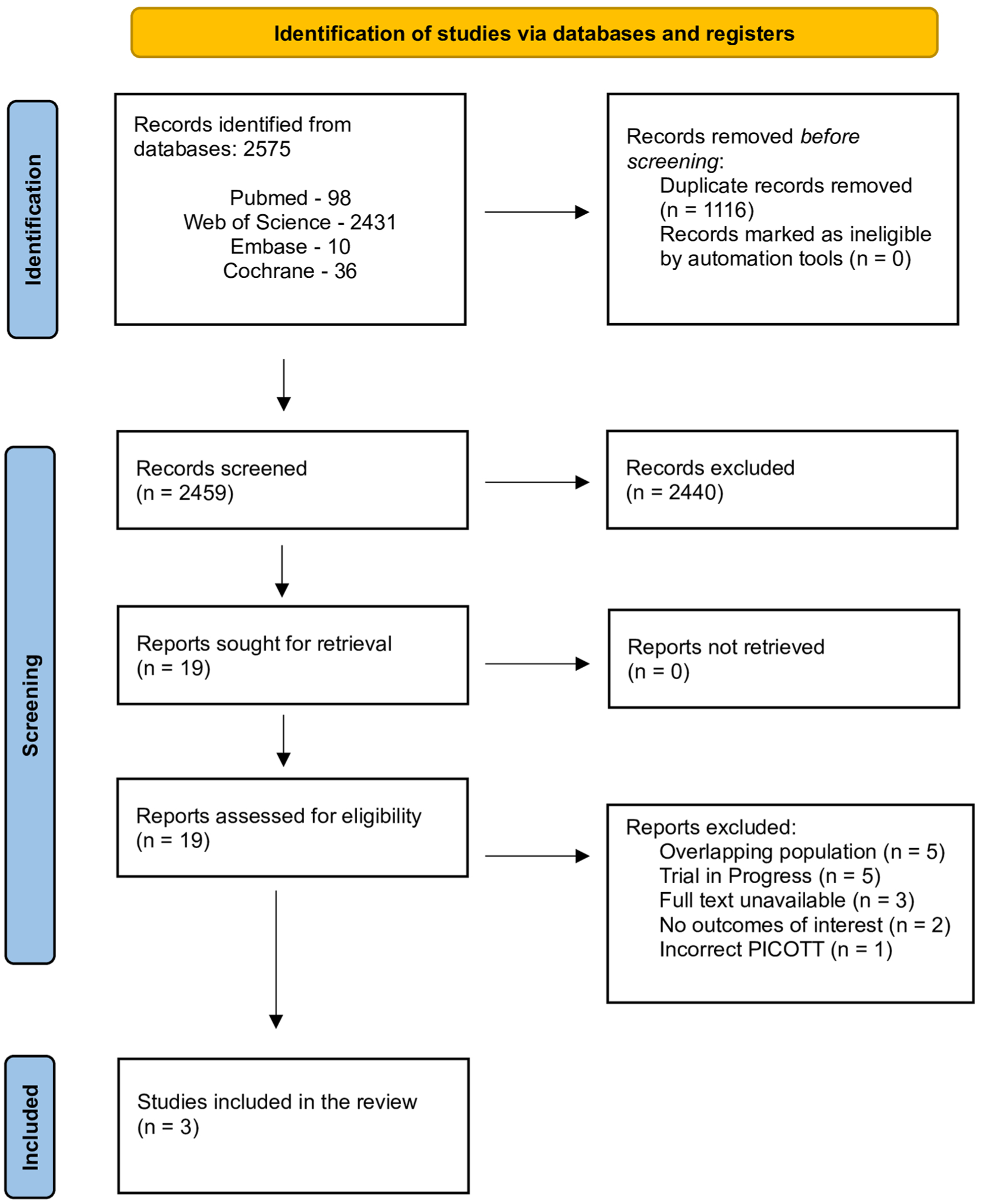
PRISMA flow diagram of study selection.
The RCTs included in this study comprised 1953 patients, of whom 978 (50.05%) were randomized to the mepolizumab group. The follow-up period ranged from 48 to 104 weeks. Baseline characteristics of included studies, including author name, year of study, demographic characteristics of the patient population, COPD exacerbations, and blood eosinophil count, are listed in Table 1.
Baseline Characteristics of Included Studies.
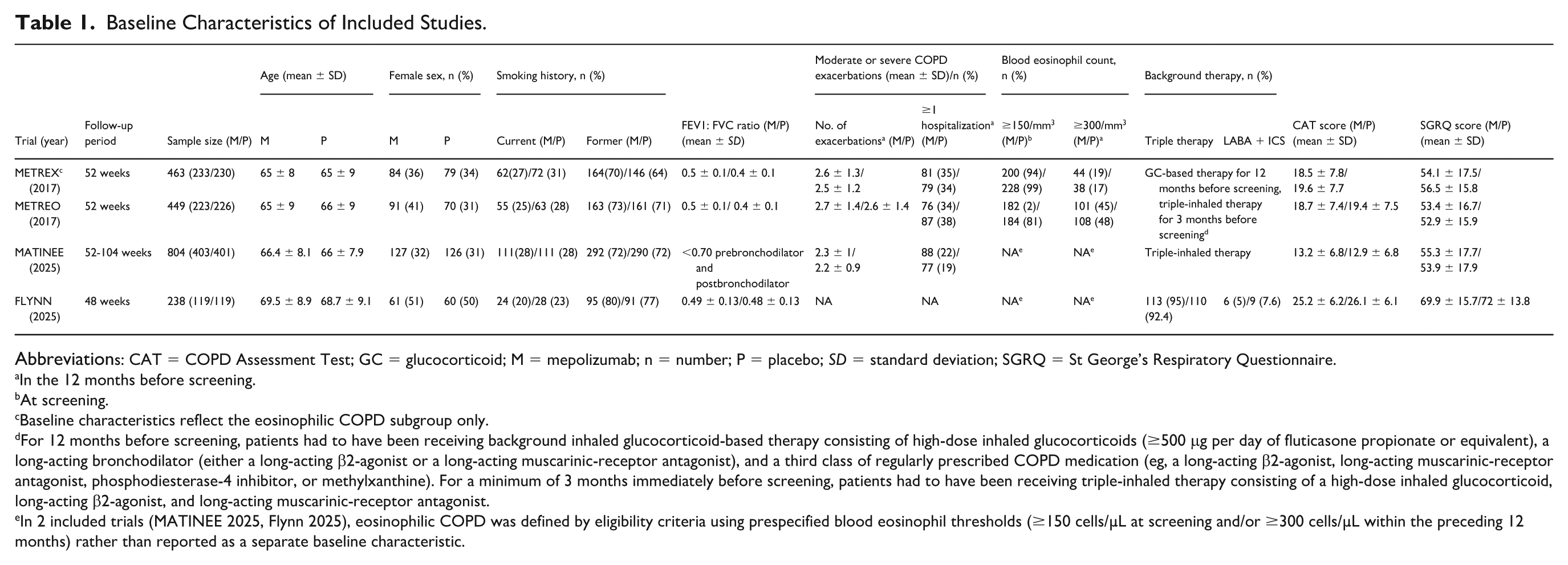
Abbreviations: CAT = COPD Assessment Test; GC = glucocorticoid; M = mepolizumab; n = number; P = placebo; SD = standard deviation; SGRQ = St George’s Respiratory Questionnaire.
In the 12 months before screening.
At screening.
Baseline characteristics reflect the eosinophilic COPD subgroup only.
For 12 months before screening, patients had to have been receiving background inhaled glucocorticoid-based therapy consisting of high-dose inhaled glucocorticoids (≥500 μg per day of fluticasone propionate or equivalent), a long-acting bronchodilator (either a long-acting β2-agonist or a long-acting muscarinic-receptor antagonist), and a third class of regularly prescribed COPD medication (eg, a long-acting β2-agonist, long-acting muscarinic-receptor antagonist, phosphodiesterase-4 inhibitor, or methylxanthine). For a minimum of 3 months immediately before screening, patients had to have been receiving triple-inhaled therapy consisting of a high-dose inhaled glucocorticoid, long-acting β2-agonist, and long-acting muscarinic-receptor antagonist.
In 2 included trials (MATINEE 2025, Flynn 2025), eosinophilic COPD was defined by eligibility criteria using prespecified blood eosinophil thresholds (≥150 cells/µL at screening and/or ≥300 cells/µL within the preceding 12 months) rather than reported as a separate baseline characteristic.
Pooled Analysis
Time to first moderate or severe exacerbation (HR = 0.80; 95% CI 0.69-0.92; P = 0.016; I2 = 0.0%; Figure 2a) was significantly longer in the mepolizumab group. The rate of moderate-to-severe exacerbations (rate ratio = 0.80; 95% CI 0.78-0.83; P < 0.001; I2=0.0%; Figure 2b) was significantly lower in the mepolizumab group. The rate of exacerbations leading to emergency department visit or hospitalization (rate ratio = 0.80; 95% CI 0.51-1.18; P = 0.230; I2 = 63.7%; Figure 3) was similar between the 2 groups.
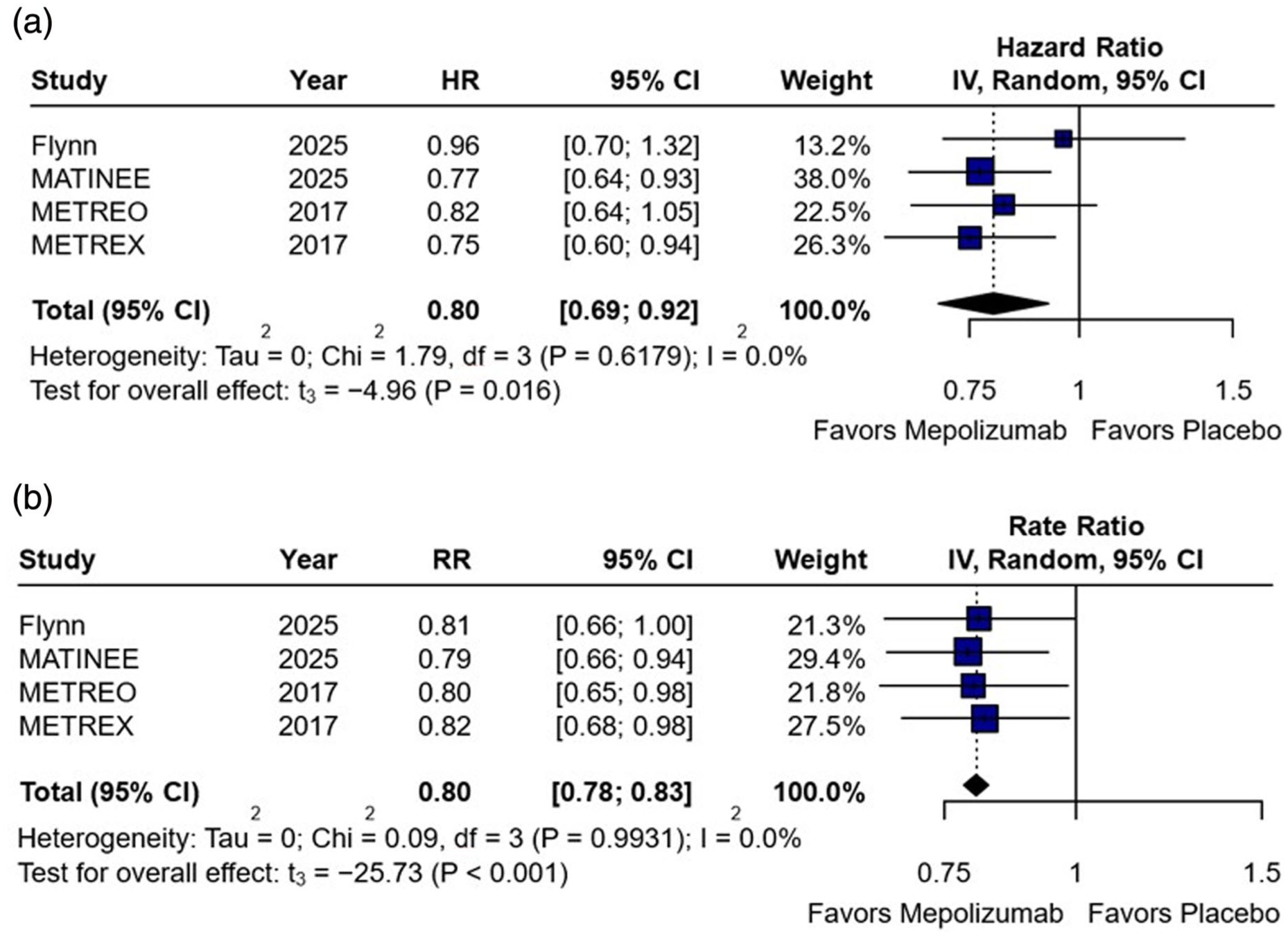
(a) Time to first moderate or severe exacerbation was significantly longer in the mepolizumab group. (b) Rate of moderate-to-severe exacerbation was significantly lower in the mepolizumab group.
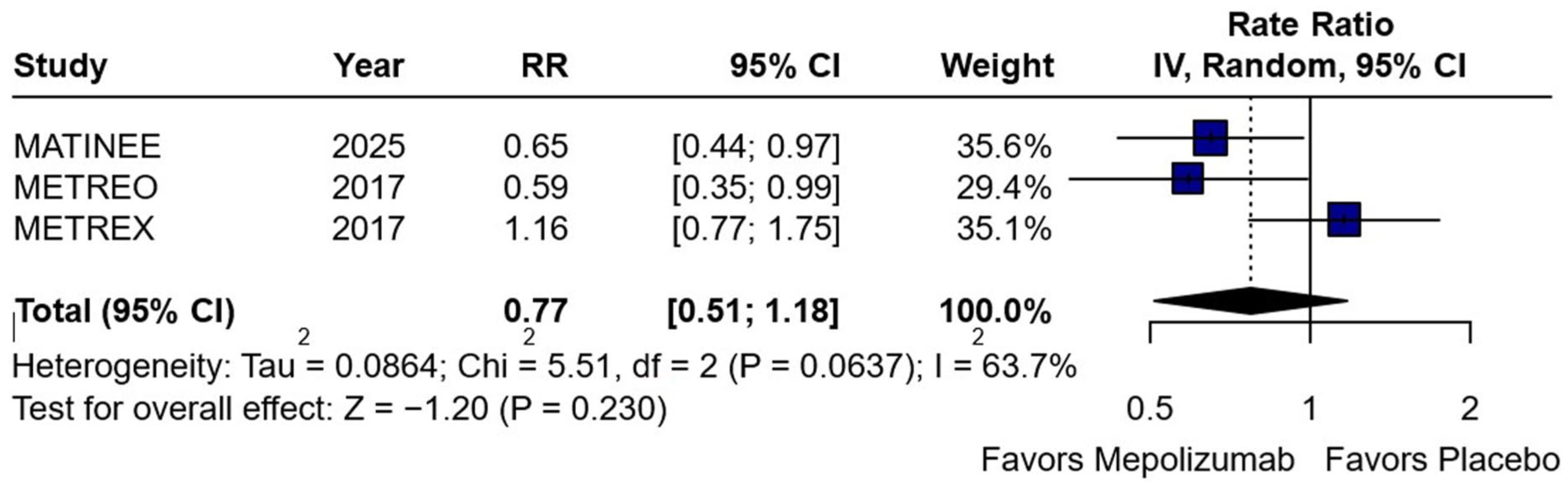
Rate of exacerbation leading to emergency department visit or hospitalization was similar between groups.
Regarding safety endpoints, the risk of AEs (RR = 1.00; 95% CI 0.95-1.06; P = 0.962; I2 = 0.0%; Figure 4a) was similar between the 2 groups. The risk of serious adverse events (SAEs) or death (RR = 0.83; 95% CI 0.72-0.96; P = 0.031; I2 = 0.0%; Figure 4b) was significantly lower in the mepolizumab group.
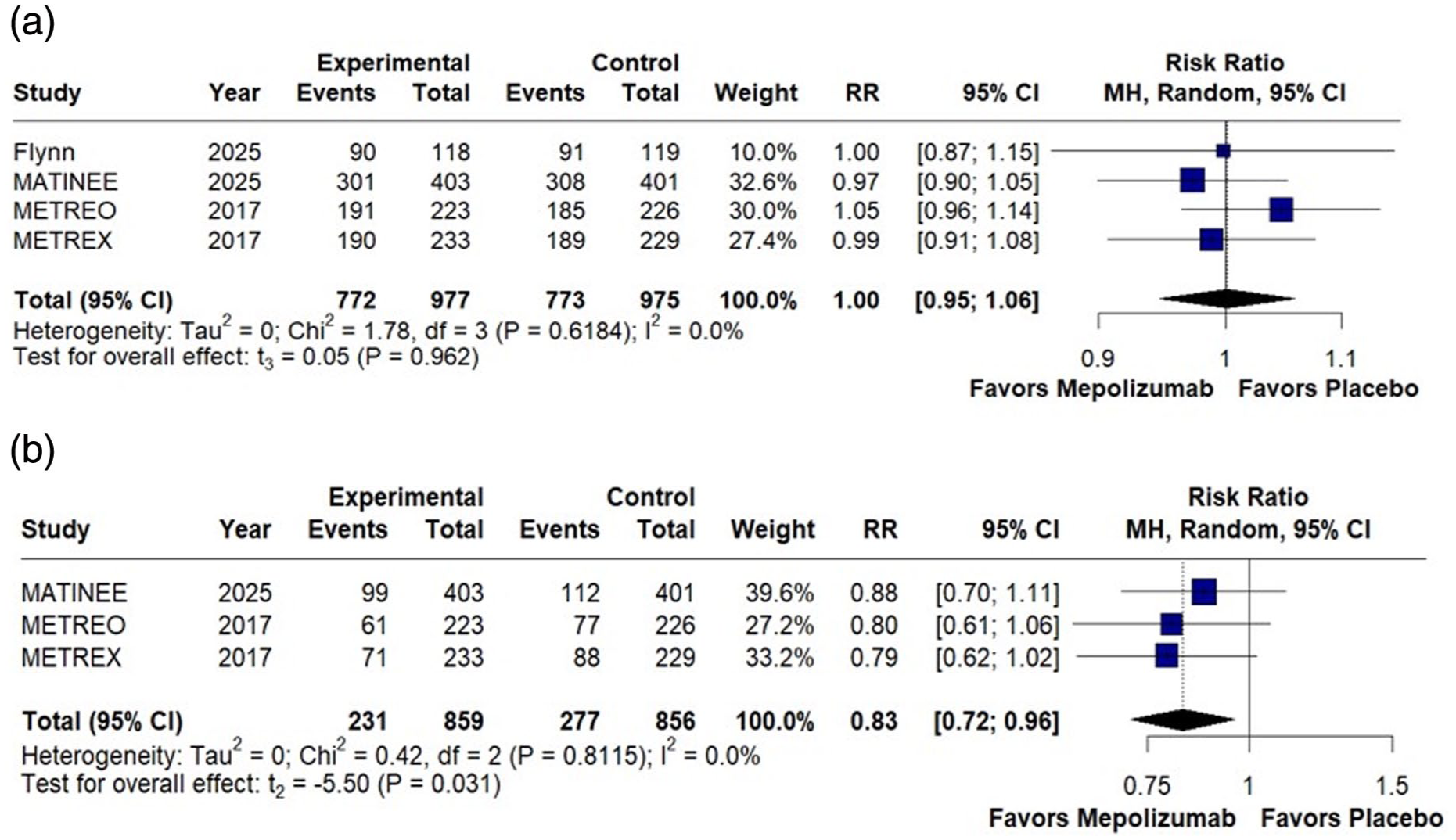
(a) Rate of AE was similar between the 2 groups. (b) Rate of SAE, including death, was significantly lower in the mepolizumab group.
Patient-reported outcomes were assessed using the CAT and SGRQ scores. Although the CAT and SGRQ scores are continuous measures, the included RCTs reported these outcomes as binary responder analyses based on prespecified clinically meaningful improvement thresholds (eg, CAT ≥2-point and SGRQ ≥4-point improvement). Accordingly, ORs were extracted directly from the published trial reports, and no transformation from continuous data to ORs was performed. No significant difference was noted in patient-related outcomes measured by the SGRQ score (OR = 1.20; 95% CI 0.88-1.63; P = 0.123; I2 = 0.0%; Figure 5a) between mepolizumab and placebo groups. The COPD symptom burden measured using the CAT score (OR = 1.15; 95% CI 0.47-2.85; P = 0.565; I2= 75.2%; Figure 5b) also reported no significant difference between the 2 groups.
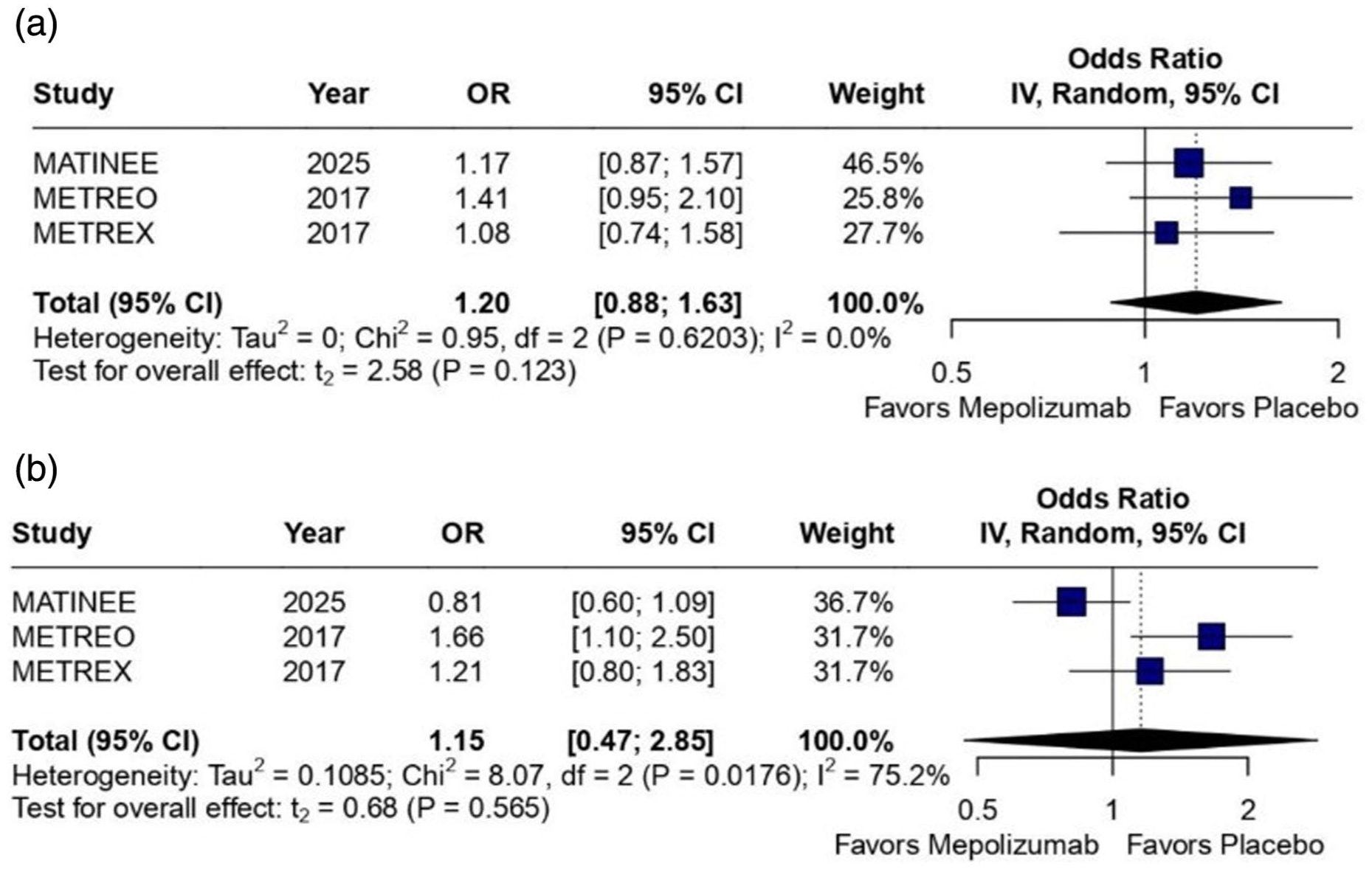
(a) No significant difference in patient-related outcomes (SGRQ score) between mepolizumab and placebo groups. (b) No significant difference in COPD symptom burden (CAT score) between mepolizumab and placebo.
Leave-One-Out Analyses
The robustness of findings was assessed using LOO sensitivity analysis to explore potential contributors to heterogeneity in the outcomes of rate of exacerbations leading to emergency department visit or hospitalization (Supplementary Material Figure S1a) and symptom burden assessed using the CAT questionnaire (Supplementary Material Figure S1b). The direction of effect of mepolizumab on COPD outcomes remained consistent across sensitivity analyses. For exacerbation-related outcomes, heterogeneity was primarily driven by the METREX trial; omission of METREX reduced heterogeneity from 63.7% to 0%. Similarly, for CAT-assessed symptom burden, exclusion of METREX substantially reduced heterogeneity to 11.6% (τ² = 0.0058). Importantly, pooled effect estimates remained statistically nonsignificant across all LOO scenarios.
Quality Assessment
Individual appraisal of each RCT included in this meta-analysis is outlined in Figure 6. The RoB was evaluated using the Cochrane RoB tool. All 4 RCTs reported the endpoints of interest with adequate matching of intervention and control subjects and were assessed as having a “Low” risk.
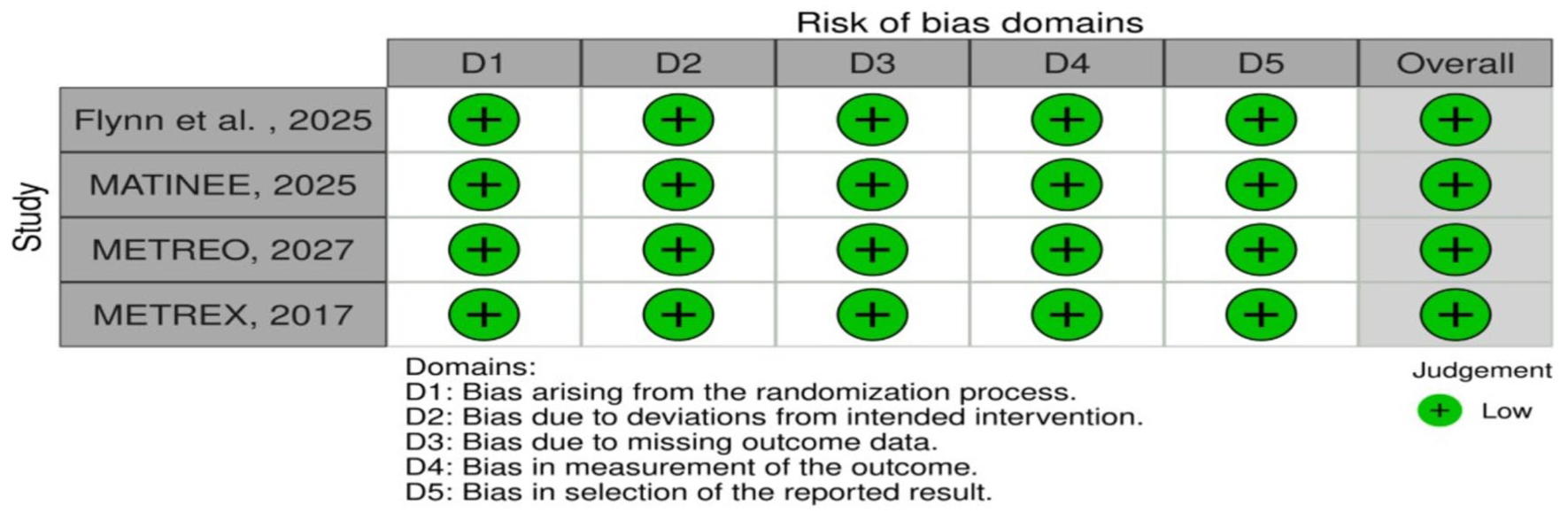
RoB2—traffic light plot.
As shown in Supplementary Material Figure S2, visual inspection of funnel plots suggested no marked asymmetry for most outcomes. Formal statistical testing using Egger’s regression (Supplementary Material Table S1) did not demonstrate statistically significant asymmetry for most outcomes. However, for the outcome of SAEs including death, Egger’s test suggested possible funnel-plot asymmetry (P = 0.02). However, these findings should be interpreted with caution, given the limited number of included studies.
The overall certainty of evidence was rated as high for most outcomes, including time to first moderate or severe exacerbation, rate of moderate-to-severe exacerbations, and AE. These outcomes demonstrated consistent effect estimates across studies, narrow confidence intervals, and a low RoB. For the outcome of SAE or death, the certainty was rated as moderate due to borderline imprecision. Exacerbation leading to emergency department visit or hospitalization was rated as low certainty. A summary of the GRADE assessments for all outcomes is provided in Supplementary Material Table S2.
Discussion
This systematic review and meta-analysis of 4 RCTs comprising 1953 patients evaluated the benefits and safety of mepolizumab 100 mg administered subcutaneously every 4 weeks in addition to background therapy in patients with eosinophilic COPD. The background treatment in all the studies was predominantly inhaled triple therapy according to the standard of care as defined by GOLD guidelines. Main findings were as follows: (1) mepolizumab significantly delayed the time to first moderate or severe exacerbation when compared with placebo (HR = 0.80; 95% CI 0.69-0.92; P = 0.016); (2) reduced the rate of moderate-to-severe exacerbation (RR = 0.80; 95% CI 0.78-0.83; P < 0.001); and (3) without increasing the risk of AE (RR = 1.00; 95% CI 0.95-1.06; P = 0.962). The rate of exacerbations that led to emergency department visits or hospitalization was not significantly different between groups.
The role of eosinophils in the pathogenesis and treatment of COPD has been investigated extensively. A high blood eosinophil count is a reliable marker for selecting patients with COPD who were most likely to benefit from inhaled corticosteroids (ICS). A blood eosinophil count of >300 cells/μL favors strong use of ICS, while a count of <100 cells/μL suggests against its use. 32 Moreover, exacerbations in patients with eosinophilia also show better response to oral corticosteroids. 33 It has also been demonstrated that although eosinophils lead the inflammatory process in COPD, eosinopenia is not associated with better outcomes. On the contrary, eosinopenia (<50 cells/μL) was associated with more severe infections and a higher mortality rate among patients with acute exacerbations. 34 Therefore, a complex relationship exists between eosinophil levels and degree of severity of COPD and the use of eosinophil counts to drive treatment should be done carefully taking patient profile into consideration.
The METREX and METREO trials aimed to demonstrate the possible benefits of mepolizumab in COPD patients with eosinophilia. 19 They reported improvement in the rate of moderate-to-severe exacerbations. While the METREO trial demonstrated a significant increase in time to first moderate or severe exacerbation, the results of the METREX trial were not substantial. This difference was because the METREX trial in its primary analysis did not screen patients based on eosinophilia. However, in a subgroup analysis of only eosinophilic phenotype, the results turned out to be significant. A prespecified analysis of these trials showed that while the most pronounced benefit was observed among patients with ≥300 cells/µL, reductions in exacerbation rates were also observed among those with counts ≥150 cells/µL.19,20 The recently reported MATINEE trial further supports the role of mepolizumab in eosinophilic COPD, demonstrating a reduction in exacerbation rates among patients with elevated eosinophil counts despite optimal inhaled therapy. 22 The COPD-HELP trial conducted by Flynn et al also did not demonstrate significant benefits in time to first moderate or severe exacerbation. 23 However, this study enrolled a smaller cohort of patients with more severe disease, including individuals with frequent prior exacerbations and recent hospitalization for acute exacerbation of chronic obstructive pulmonary disease, which may partially explain the absence of statistically significant benefit. Previous meta-analyses analyzing biologics and anti-IL-5 therapies have shown no benefit in the rate of moderate-to-severe exacerbations with the addition of mepolizumab21,35 in the treatment course. This contrasts with our meta-analysis, which has demonstrated significant benefits for time to moderate or severe exacerbation and rate of moderate-to-severe exacerbations, demonstrating more consistent and clinically meaningful benefits. Again, the reason for this contrast may be because these studies did not specifically focus on the eosinophilic population of the METREX trial and included all the participants. The rate of exacerbations leading to emergency department visits, hospitalization, or both was lower in the mepolizumab group, but the results were not statistically significant. This was primarily due to imprecision, as reflected by wide confidence intervals and substantial heterogeneity among included studies, leading to reduced confidence in the pooled effect estimate.
Several other biologics, such as dupilumab, which targets IL-4Rα; benralizumab, which targets IL-5; itepekimab and tozorakimab, which target IL-33; and astegolimab, which targets suppressor of tumorigenicity 2 (ST2), have shown potential for COPD treatment. 36 A network meta-analysis evaluating these biologics did not find any substantial improvement in exacerbation risks with biologics other than dupilumab. 6 However, this meta-analysis did not include the COPD-HELP and MATINEE trials; therefore, the results should be interpreted with caution. Despite the advent of newer biologics, only dupilumab and mepolizumab remain Food and Drug Administration-approved for use as an add-on maintenance therapy for inadequately controlled eosinophilic COPD.37,38 In patients with COPD who continue to experience exacerbations despite triple-inhaled therapy, macrolide prophylaxis has historically been considered. They have been used in the treatment of COPD because of their antiinflammatory and immune-modulating effects. Long-term (>12 months) use of azithromycin and erythromycin have shown considerable efficacy in suppressing COPD exacerbations when compared with placebo, 39 however, we could not identify any major study, which directly compares macrolides with biologics. Unlike macrolides, which provide broad anti-inflammatory and antimicrobial effects, biologics directly modulate the eosinophilic inflammatory pathway and may therefore be particularly beneficial in selected patients with elevated blood eosinophil counts. Moreover, their role in specifically reducing exacerbations in eosinophilic COPD population warrants further research.
In addition to the existing therapies, there are a number of potential targets that are being developed for treating COPD. These include immunomodulatory drugs, such as chemoattractant receptor-homologous molecule on T helper type 2 cells (CRTH2) antagonists, matrix metalloproteinase (MMP) inhibitors, and tumor necrosis factor inhibitors; monoclonal antibodies, such as thymic stromal lymphopoietin monoclonal antibody, IL-25 monoclonal antibody, and IL-33 monoclonal antibody, and regulators of oxidative stress, such as nicotinamide adenine dinucleotide phosphate oxidase (NOX) inhibitors and peroxidase inhibitors. 40 All these therapies are at various stages of clinical trials and have the potential to expand the treatment paradigm for COPD.
The safety endpoints that were analyzed included the rate of AE and SAE. Previous trials and meta-analyses have reported no significant differences between the risk of AE or SAE, including death, when comparing mepolizumab and placebo.19-23,35 Our study also demonstrated nonsignificant differences regarding the risk of AE. However, the risk of SAE, including death, was significantly lower in the mepolizumab group (RR = 0.83; 95% CI 0.72-0.96; P = 0.031). This finding is likely explained by the fact that most of the SAE consisted of COPD exacerbation, worsening, or pneumonia, which may be positively influenced by mepolizumab.
Data from multiple RCTs have shown mepolizumab to have an acceptable safety profile that is similar to that of placebo. A long-term 10-year extension of multiple prior studies also demonstrated no significant safety concerns with mepolizumab. 41 The most common non-SAEs included influenza-like illness, injection-site reaction, and nasal congestion and sneezing. In the pediatric population, headache was the most common non-SAE. SAEs that were considered treatment-related included colitis, gastritis, and colorectal adenoma in 1 patient and a single resolved episode of spontaneous abortion, which was >28 days after termination of treatment with mepolizumab. 41 However, most of these data are from studies evaluating the role of mepolizumab in asthma and further studies focusing on AE of mepolizumab in COPD patients are required.
Chronic obstructive pulmonary disease exacerbations are major contributors to the significant deterioration of quality of life among patients. Although the METREX and METREO trials reported significant improvement in the CAT scores 25 with the addition of mepolizumab, similar results were not replicated in the subsequent MATINEE and COPD-HELP trials.22,23 Previous RCTs have reported no significant change in the SGRQ scores 26 when comparing the treatment with a placebo.19,22,23 No significant differences in the evaluation of scores were observed between groups. These findings are still under investigation, and further studies are required to evaluate this outcome. 22 The lack of benefit in patient-related outcomes is in line with the fact that biologics may reduce exacerbations without modifying fixed airflow limitation, which continues to be a prime determinant of daily symptoms of COPD. 42
The pharmacoeconomics of mepolizumab have been explored in various studies but these analyses have been limited to patients with asthma. While most of the studies demonstrate substantial fiscal constraints with limited affordability in countries, such as Singapore, Chile, and Colombia,43-45 when compared with other biologics like benralizumab and reslizumab, it provided greater cost-effectiveness. 46 Another study conducted in the Dubai health authority showed direct cost saving with mepolizumab considering the cost of care incurred during exacerbations. 47 All these analyses were country-specific and in the context of the country’s economic thresholds specifically for asthma patients. Therefore, further cost-effective analyses of mepolizumab are required focusing on patients with COPD and also in respect to different economic settings to fully understand the financial burden of this therapy.
Although our study demonstrated favorable outcomes with the addition of mepolizumab to background triple-inhaled therapy in patients with eosinophilic COPD, it has certain limitations. There is a limited number of RCTs available on the subject. Moreover, differences in background inhaled therapy, and eosinophil thresholds likely contributed to heterogeneity across studies. In addition, the absence of stratified outcome reporting by GOLD stage or prior exacerbation history across trials precluded assessment of differential treatment effects by disease severity. Also, lung function indices were reported descriptively at baseline were available but could not be pooled quantitatively because of inconsistent reporting across included trials. Systemic comorbidities, such as cardiac or renal diseases, which may have a role in determining patient response to mepolizumab, were not consistently characterized across studies. Though we were able to analyze overall risk of AE, organ-system-specific (allergies, immune abnormalities, hematological, renal, and hepatic) AEs were not analyzed, as such data were not reported in the included RCTs. Also, blood eosinophil levels exhibit biological variability, and single measurements may not accurately reflect a patient’s inflammatory phenotype. Another limitation is the absence of individual patient-level data, preventing deeper phenotype stratification, such as eosinophil trajectories, comorbidity clusters, and ICS responsiveness. Furthermore, formal subgroup analysis or meta-regression to explore sources of heterogeneity was not feasible due to the limited number of included studies.
Despite these limitations, the evidence suggests mepolizumab offers a targeted biologic option in patients with an eosinophilic phenotype, particularly those with blood eosinophil counts ≥300 cells/µL, who continue to experience exacerbations despite optimal inhaled therapy. These results underscore the importance of integrating biomarkers into treatment algorithms and provide a rationale for precision-based immunomodulatory therapy in COPD.
Relevance to Patient Care and Clinical Practice in Comparison With Existing Drugs
A substantial number of patients with COPD continue to experience frequent exacerbations despite maximum triple-inhaled therapy and conventional dose escalation of inhaled therapy or addition of systemic corticosteroids is limited by modest incremental efficacy and higher risk of complications, such as pneumonia, metabolic complications, and other infections. In this regard, mepolizumab offers a targeted alternative by selectively inhibiting IL-5-driven pathways demonstrating not only superior efficiency in reducing both severity and frequency of exacerbations but also a tolerable safety profile. When compared with other biologics under consideration, only dupilumab has received regulatory approval other than mepolizumab and both the drugs have shown good efficacy with tolerable safety profile; however, the broader immune blockade of dupilumab can lead to increased side effects, which need to be studied further and through long-term follow-up. Mepolizumab benefits from the decade-long safety data in asthma populations. Unlike eosinophil-depleting receptor-directed agents, such as benralizumab, mepolizumab modulates eosinophilic activity while preserving physiological immune function, a clinically relevant consideration in infection-prone COPD patients.
The integration of mepolizumab into clinical practice is facilitated by the routine and already recommended use of blood eosinophil counts to supplement clinical decision-making. This approach enables practice of precision medicine, potentially reducing hospitalizations, systemic corticosteroid exposure and probably health care utilization in long term.
Conclusion
This meta-analysis, synthesizing data from 4 RCTs, including 1953 patients, evaluated the efficacy and safety of mepolizumab in patients with eosinophilic COPD. Mepolizumab significantly prolongs the time to first moderate-to-severe exacerbations and reduces the overall exacerbation rate in the specific population without increasing the risk of AE. Exacerbations drive disease progression, mortality and health care costs in patients with COPD. Mepolizumab offers a targeted biologic option in patients with an eosinophilic phenotype who continue to experience exacerbations despite optimal therapy. Incorporating blood eosinophil counts into treatment decision-making may help identify patients most likely to benefit, thereby improving clinical outcomes.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261437728 – Supplemental material for Efficacy and Safety of Mepolizumab in Eosinophilic COPD: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-aop-10.1177_10600280261437728 for Efficacy and Safety of Mepolizumab in Eosinophilic COPD: A Systematic Review and Meta-Analysis of Randomized Controlled Trials by Rahul Bisht, Arusha Desai, Esteban Marcelo Mogrovejo Carrión, Anjali Bhardwaj, Sidharth Misra, Tejesh Bangalore Shivashankar and Ramita Gupta in Annals of Pharmacotherapy
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval was not needed.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
A.D. and R.B. contributed to the study conception and design. Data collection and analysis were undertaken by A.D., R.B., and E.M.M.C. The initial manuscript was drafted by A.D., R.B., E.M.M.C., A.B., S.M., T.B.S., and R.G. All authors contributed to the review, editing, and refinement of earlier and final versions. All authors approved the manuscript for publication and are accountable for the integrity and accuracy of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are derived from previously published randomized controlled trials and are publicly available within the cited articles. No new individual patient data were generated by the authors for this meta-analysis; therefore, data cannot be publicly shared. All extracted outcome data used in this study are available from the corresponding published sources as referenced throughout the manuscript.
Registration
The protocol for this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251101907.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.