
Abstract
Objective:
To review the pharmacology, efficacy, and safety of zoliflodacin for the treatment of uncomplicated urogenital gonorrhea due to Neisseria gonorrhoeae in adults and pediatric patients 12 years of age and older.
Data sources and extraction:
A literature search was conducted in Scopus, Web of Science, PubMed Central, Gale Academic FileOne, MEDLINE, Journals@Ovid, and Science Direct databases for all articles relevant to zoliflodacin from inception through February 12, 2026.
Data synthesis:
Preclinical, pharmacokinetic, and clinical trial data have demonstrated that zoliflodacin is effective against multidrug-resistant (MDR) N. gonorrhoeae, with high urogenital cure rates and no current evidence of increasing minimum inhibitory concentrations. Evidence from phase II and III trials supports its single-dose use as an alternative to ceftriaxone; however, the reduced efficacy for pharyngeal and rectal lesions requires additional evaluation.
Relevance to patient care and clinical practice in comparison with existing drugs:
Zoliflodacin could serve as an oral alternative to ceftriaxone, particularly for patients with a cephalosporin allergy, and be a viable option for resistance-directed therapy. Continued surveillance will be imperative as zoliflodacin use increases.
Conclusion:
Zoliflodacin is a novel, first-in-class spiropyrimidinetrione antibiotic for the treatment of uncomplicated urogenital gonorrhea that is efficacious and provides a novel option for MDR N. gonorrhoeae.
Introduction
Urogenital gonorrhea, caused by the Gram-negative bacteria Neisseria gonorrhoeae, continues to be an urgent public health threat, with global estimates of 82.4 million new cases of gonorrhea among patients aged 15 to 49 years old.1,2 This common sexually transmitted infection can be spread through vaginal, oral, or anal sex. The variety observed in symptomology, from a lack of symptoms to pain, burning, and discharge, raises challenges in identification and timely treatment. 1 In addition to this challenge, N. gonorrhoeae has developed resistance to all classes of antibiotics utilized for this indication, including tetracyclines, macrolides, and fluoroquinolones, leaving ceftriaxone as the only remaining agent recommended. 3 However, trends of decreasing cephalosporin susceptibility have been observed.2,4 In response, the World Health Organization (WHO) global action plan focused on the development of new antibiotics for the treatment of gonorrhea as a high priority, and the US Centers for Disease Control and Prevention (CDC) listed drug-resistant N. gonorrhoeae as an urgent public health threat.2,5
On December 12, 2025, the US Food and Drug Administration (FDA) approved the use of zoliflodacin for the treatment of uncomplicated urogenital gonorrhea due to N. gonorrhoeae in adults and pediatric patients 12 years of age and older. 6 This review strives to cover the pharmacology, pharmacokinetic (PK), and pharmacodynamic (PD) properties, clinical trial data, safety, and administration recommendations of zoliflodacin.
Data Sources
A literature search was performed to ensure this review was informed by all available and retrievable articles and abstracts relevant to zoliflodacin’s clinical and efficacy profile. The search took place on February 12, 2026, and used Scopus, Web of Science, PubMed Central, Gale Academic FileOne, MEDLINE, Journals@Ovid, and Science Direct databases. The search terms “zoliflodacin OR EXT0914 OR AZD0914 AND gonorrh*” were used with filters for English language and “article” resource type. The date range was from inception through February 12, 2026. Articles were included for safety and efficacy information if they were in vivo human studies evaluating zoliflodacin. Articles were included for PK and PD information if they evaluated zoliflodacin PK or PD characteristics. Some that did not meet the inclusion criteria were used for background information. The exclusion criterion for safety and efficacy information was articles with clinical outcomes other than N. gonorrhoeae infections.
Registered clinical trials were also searched using “gonorrhea” in the “condition/disease” field, “EXT0914” in the “other terms” field, and “zoliflodacin” in the “intervention/treatment” field on the ClinicalTrials.gov website on February 12, 2026. This search found registered clinical trials with the following identifiers: NCT02257918, NCT03404167, NCT03959527, NCT03613649, NCT03718806, and NCT01929629. Finally, references and government websites (ie, FDA website) were used for background information.
Pharmacology
Zoliflodacin (formerly AZD0914) is a first-in-class spiropyrimidinetrione antibacterial agent that inhibits bacterial type II topoisomerases, including DNA gyrase and topoisomerase IV, enzymes essential for DNA replication. 7 While both zoliflodacin and fluoroquinolones target bacterial type II topoisomerases, their core structural scaffolds differ. 7 Unlike fluoroquinolones, which require a Mg²⁺-mediated water-metal ion bridge with residues in the GyrA and ParC subunits, zoliflodacin binds through alternative interactions mediated by its spiropyrimidinetrione scaffold, which bypasses the water-metal ion bridge completely (Figure 1). 8 This distinct binding mode prevents DNA relegation and preserves activity against many fluoroquinolone-resistant N. gonorrhoeae isolates. 9 Consistent with this mechanism, in vitro studies demonstrate low zoliflodacin minimum inhibitory concentrations (MICs) against ciprofloxacin-resistant N. gonorrhoeae strains harboring GyrA mutations. 9 Finally, the rigidity of the spiropyrimidinetrione ring is theorized to decrease the likelihood of cross-resistance because the key carbonyl and heterocyclic functional groups are in a fixed orientation that is preserved across mutations that otherwise disrupt fluoroquinolones. 9
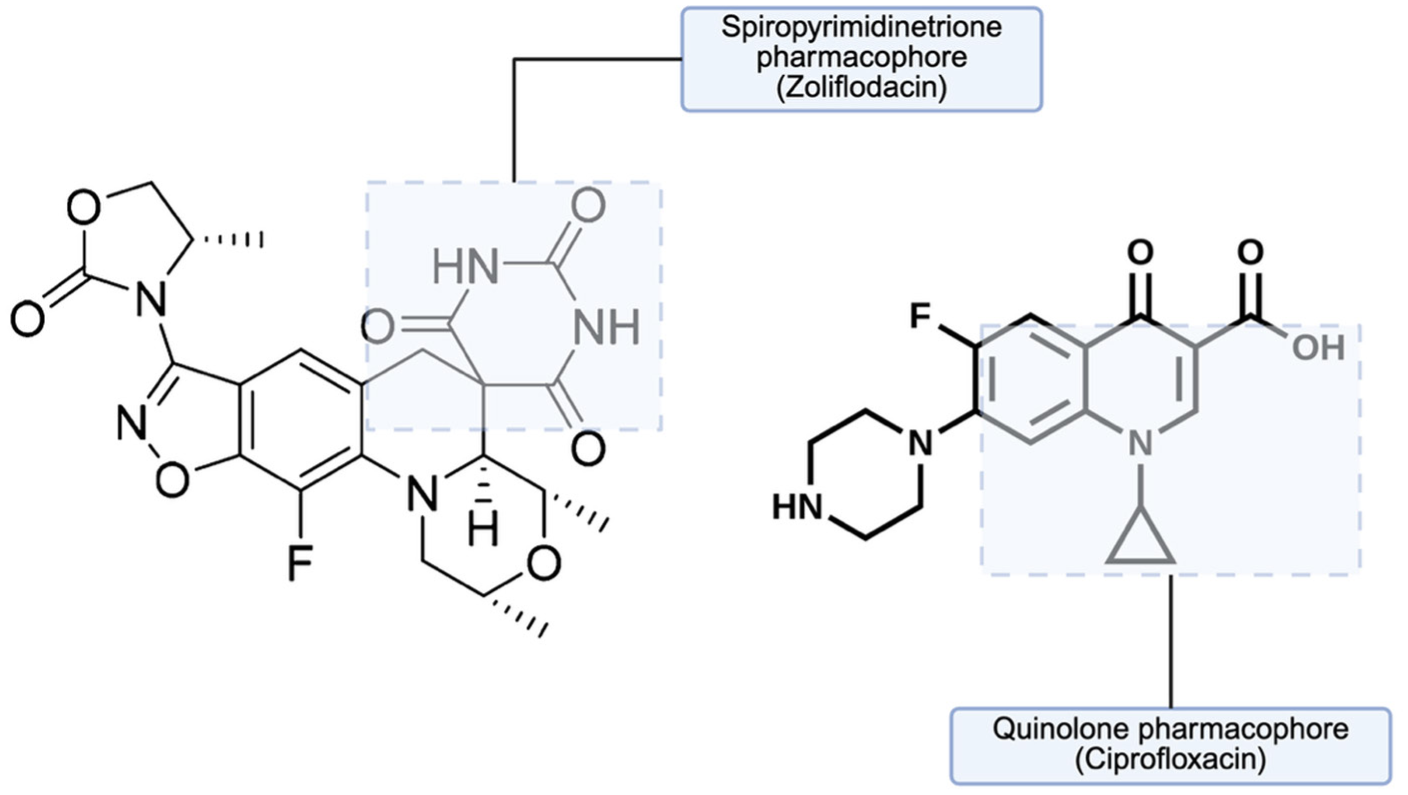
Structural comparison of zoliflodacin and fluoroquinolone cores.
Zoliflodacin exhibits a broad spectrum of activity against several clinically relevant pathogens, including Gram-positive organisms such as Staphylococcus and Streptococcus species, fastidious Gram-negative organisms such as Haemophilus influenzae and N. gonorrhoeae, atypical pathogens including Legionella pneumophila, and anaerobes such as Clostridioides difficile. 10 Notably, zoliflodacin demonstrates potent in vitro activity against N. gonorrhoeae, including isolates resistant to multiple recommended therapies. In a surveillance study of 873 contemporary clinical isolates collected from 21 European countries, zoliflodacin MIC values ranged from ≤0.002 to 0.25 mg/L, with an MIC₅₀ of 0.064 mg/L and an MIC₉₀ of 0.125 mg/L. 11 These MIC values were substantially lower than those observed for ciprofloxacin and other gonorrhea-active agents. High resistance rates to existing therapies were observed in the same isolate collection, including 55% for ciprofloxacin, 8.4% for azithromycin, 4.1% for cefixime, and 0.2% for ceftriaxone. Despite these resistance patterns, zoliflodacin MIC values remained similar among isolates that were susceptible or resistant to these agents, indicating preserved activity against multidrug-resistant (MDR) N. gonorrhoeae. Notably, no correlation was observed between zoliflodacin MICs and those of ciprofloxacin (r = −0.0006), supporting a lack of cross-resistance. Similar susceptibility patterns have been reported in clinical isolates from Thailand, South Africa, and phase II clinical trial isolates from the United States, supporting a global wild-type MIC distribution for zoliflodacin and a proposed susceptibility breakpoint of 0.5 mg/L.12,13
Resistance to zoliflodacin appears to arise infrequently and is primarily associated with mutations in the drug target, the GyrB subunit of DNA gyrase. In vitro studies using WHO N. gonorrhoeae reference strains, including MDR isolates (WHO O, V, and X), demonstrated a low frequency of resistance selection compared with other gonorrhea-active agents. 14 Resistant mutants contained single amino acid substitutions in GyrB, most commonly D429N and less frequently K450T or K450N, which increased zoliflodacin MICs to 0.5 to 4 mg/L. Importantly, these mutations do not confer cross-resistance to other topoisomerase II inhibitors such as ciprofloxacin or sitafloxacin, which primarily target the GyrA subunit. Large genomic surveillance analysis has also shown that these mutations were rare, with none detected among 12 493 N. gonorrhoeae genomes in the PathogenWatch. 15
Pharmacokinetics and Pharmacodynamics
Zoliflodacin demonstrates dose-proportional PK at lower single doses (<800 mg), with slightly less than proportional increases in exposure at higher doses (800-4000 mg). 16 In adults, zoliflodacin is administered as a single 3 g oral suspension dose. 6 Absorption is affected by food intake. A moderate-to-high-fat meal delays absorption but increases overall exposure by ~ 1.5 to 2 fold.6,16 Following a 3 g oral dose, peak plasma concentrations occur at approximately 2.5 hours in the fasted state (4 hours with food), with a geometric mean Cmax of ~28.5 µg/mL and AUC₀–∞ of ~353 h·µg/mL in patients with uncomplicated urogenital gonorrhea. Zoliflodacin has an elimination half-life of approximately 5 to 6 hours, is about 83% protein bound, and is eliminated primarily via fecal excretion, with metabolism occurring through both CYP-mediated pathways, predominantly CYP3A4/5.6,16
Zoliflodacin exhibits concentration-dependent bactericidal activity and resistance suppression at high single-dose exposures. In a dynamic hollow-fiber infection model inoculated with susceptible and resistant N. gonorrhoeae strains (WHO F and WHO X), single doses of 2 to 8 g produced rapid killing within 6.5 hours and sustained bacterial suppression for up to 7 days. 12 In contrast, lower exposures (0.5-1 g/day) resulted in bacterial regrowth by 72 hours in isolates harboring the GyrB D429N mutation (MIC 0.5-1 µg/mL). Mutant suppression corresponded to a free-drug AUC/MIC target of approximately 70, supporting the clinical strategy of administering zoliflodacin as a large single oral dose.
Population PK analyses using data from phase I and III studies (n = 261 participants) were used to estimate PK/PD target attainment for a single 3 g oral dose of zoliflodacin. 17 Using the efficacy index of free-drug AUC₀–∞/MIC ≥ 71, the probability of target attainment (PTA) was ≥96.2% for isolates with MIC < 0.5 mg/L, a range that includes approximately 99.6% to 100% of contemporary N. gonorrhoeae isolates (Figure 2). When averaged across observed MIC distributions, simulated PTA exceeded 99.5% under both fed and fasted conditions, supporting the selected 3 g single-dose regimen. Finally, it is worth noting that time-kill analyses indicate that zoliflodacin may exhibit reduced bactericidal activity when combined with certain agents, particularly tetracycline, suggesting a potential antagonistic PD interaction that warrants further evaluation in vivo. 14
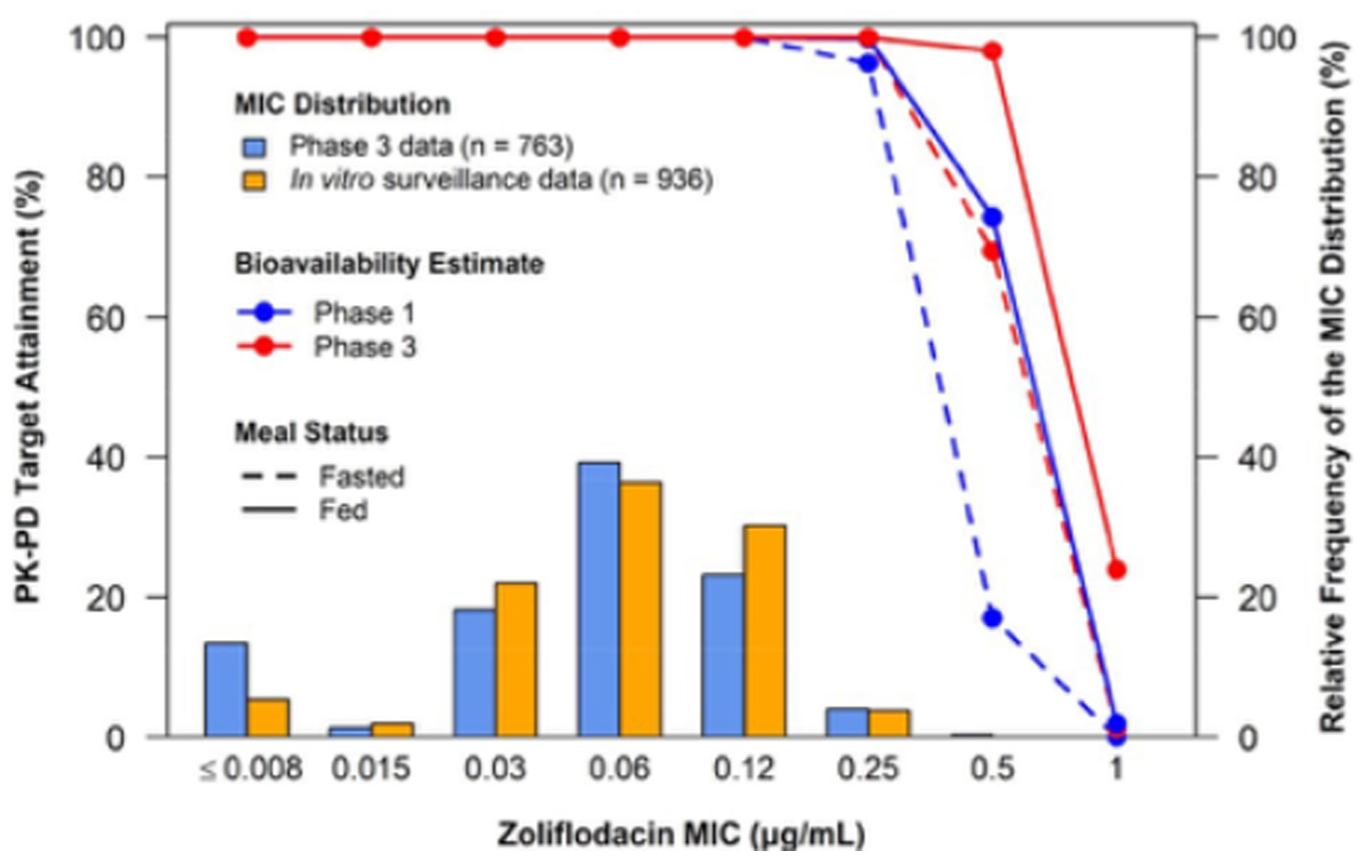
Probability of pharmacokinetic-pharmacodynamic target attainment for zoliflodacin by MIC following a single 3 g oral dose. 16
Clinical Efficacy and Safety
Clinical efficacy was evaluated from phase II and III trials, including a subgroup analysis in a published abstract.
Phase II Trial
Taylor et al 13 conducted a 3-armed randomized controlled clinical trial (NCT02257918) in 2018 with initial results reported at the Infectious Diseases Society of America’s ID Week conference in 2016. 18 The subjects were recruited from sexual health clinics in 5 US cities. Subjects were included if they were nonpregnant, aged 18 to 55, with signs and symptoms of urogenital gonorrhea, untreated urogenital gonorrhea, or reported sexual contact with a partner with gonorrhea in the past 14 days. Subjects were instructed to abstain from intercourse for 7 days after treatment, use contraception for 30 days before treatment, and use a condom with another contraceptive 30 days after treatment.
Subjects were assigned to receive either a zoliflodacin powder for oral suspension as treatment in a single 2 g or 3 g dose or a single intramuscular 500 mg ceftriaxone dose as a standard of care control in a 70:70:40 ratio. The primary efficacy outcome was microbiologic cure at the test-of-cure visit at 6 ± 2 days. The primary safety outcome was the proportion of subjects with adverse events from the first to the third visit. Secondary outcomes included microbiologic cure at the pharyngeal and rectal sites via a nucleic acid amplification test (NAAT), the proportion of negative results from urethral, cervical, rectal, or pharyngeal sites, and the proportion of subjects with clinical cure, and MICs against zoliflodacin and ceftriaxone at baseline and test of cure.
There were 179 subjects in the micro-intention to treat analysis (141 urogenital, 23 pharyngeal, and 15 rectal). Urogenital cure rates were similar at to the test-of-cure visit, with subjects receiving zoliflodacin 2 g (n = 57) and 3 g (n = 56) each having a 96% cure rate (95% confidence interval CI 88 to 100), and ceftriaxone (n = 28) had a 100% cure rate (95% CI 88 to 100). Subjects with rectal lesions were 100% cured with a 95% CI 48 to 100, 59 to 100, and 29 to 100, respectively. Pharyngeal lesions showed cure rates of 50% (95% CI 16 to 84) for zoliflodacin 2 g, 82% (95% CI 48 to 98) for zoliflodacin 3 g, and 100% for ceftriaxone (95% CI 40 to 100).
Clinical cure rates were 91% (95% CI 80 to 97) for zoliflodacin 2 g, 94% (95% CI 83 to 99) for zoliflodacin 3 g, and 96% (95% CI 81 to 100) for ceftriaxone 500 mg. Test-of-cure negative NAAT rates from the micro-ITT analysis found 84% (95% CI 72 to 93), 81% (95% CI 67 to 90), and 89% (95% CI 71 to 98) clearance rates for zoliflodacin 2 g, zoliflodacin 3 g, and ceftriaxone 500 mg, respectively.
There were 84 adverse events reported. The zoliflodacin 2 and 3 g groups accounted for 61 adverse events, with 21 participants’ events attributed to the drug. Most were gastrointestinal in nature and self-limiting, according to the investigators. None of the isolates at baseline or the test of cure had MICs above the ≥ 0.5 breakpoint for zoliflodacin; however, there were MICs above the breakpoint for azithromycin, penicillin, and ciprofloxacin in the micro-ITT analysis. 13
Overall, the study demonstrated that single-dose oral zoliflodacin was effective for treating uncomplicated urogenital gonorrhea, with cure rates comparable with intramuscular ceftriaxone at both 2 and 3 g doses. Zoliflodacin performed well at rectal sites, but its efficacy at pharyngeal sites was noticeably lower than that of ceftriaxone. However, a direct comparison by site was not made in this study. Clinical cure rates and test-of-cure negative NAAT rates appeared similarly high across all groups. Most adverse events were mild and gastrointestinal. Finally, no zoliflodacin resistance was detected using MIC thresholds, which supports its potential as a treatment option amid the rising N. gonorrhoeae’s antimicrobial resistance landscape.
Phase III Clinical Trial
The phase III trial from Luckey (NCT03959527) was published in January 2026. 19 The study took place at 17 clinical sites in Belgium, the Netherlands, South Africa, Thailand, and the United States. Subjects were included if they were nonpregnant, aged 12 and older, with signs and symptoms of urogenital gonorrhea, lab-confirmed gonorrhea infection in the past 14 days, or reported sexual contact with a partner with gonorrhea in the past 14 days.
The study design was an open-label, randomized controlled trial with participants (total n = 923) stratified by sex assigned at birth. Participants were assigned in a 2:1 ratio to receive a single oral dose of zoliflodacin 3 g (n = 506) powder for oral suspension or ceftriaxone 500 mg intramuscularly with a single oral dose of azithromycin 1 g (n = 238). The primary endpoint was the proportion of participants with microbiological cure at the urogenital site at the test-of-cure visit (6 ± 2 days after treatment) and at follow-up (30 ± 3 days after treatment) to determine noninferiority of zoliflodacin compared with the standard of care. Secondary endpoints included the proportion of participants with microbiological cure at rectal and pharyngeal sites, the proportion of male participants among those with a clinical cure, and the proportion of female and male participants with microbiological cure at the test-of-cure visit.
The urogenital microbiological cure rate for zoliflodacin was 90.9% (95% CI 88.1 to 93.3) compared with 96.2% (95% CI 92.9 to 98.3) in the control group. The difference was 5.3% (95% CI 1.4 to 8.6), which was less than the prespecified 12% noninferiority margin. Of note, the FDA recommends a 10% noninferiority margin in its guidance on developing drugs for treating uncomplicated gonorrhea. 20 The per-protocol analysis found a 3.2% difference in microbiological cure rates (95% CI 1.1 to 5.1). Cure rates at the pharyngeal and rectal sites in the micro-ITT population were 79.2% (95% CI 65.9 to 89.2) and 87.3% (95% CI 78.0 to 93.8), respectively. In the per-protocol analysis, the pharyngeal and rectal sites each had over a 90% cure rate. The cure rate difference by site was −0.7% (95% CI −20.8 to16.3) and 1.2% (95% CI −14.3 to 12.6) for pharyngeal and rectal sites, respectively.
The safety outcome analysis found no deaths or serious adverse events reported. The most common adverse events reported were headache (10%), neutropenia (7%), and leukopenia (4%) in the zoliflodacin group. A post hoc analysis found that only black or African American race (odds ratio [OR] 109.70, 90% CI 20.91 to 575.53) and male sex (OR 0.24, 90% CI 0.11 to 0.53) were strongly associated with neutropenia. There were no increases in zoliflodacin MICs from baseline to test of cure. 19
A subanalysis was conducted to determine cure rates by baseline zoliflodacin MIC and susceptibility to ciprofloxacin. 21 The subanalysis found that isolates from patients receiving zoliflodacin with MICs ≤0.12 had cure rates >90%. Isolates with MICs of 0.25 (n = 22) and 0.5 (n = 3) had cure rates of 81.8% and 66.7%, respectively. Microbiological cure rates in zoliflodacin group isolates that were susceptible to ciprofloxacin were 97.4% (95% CI 92.6 to 99.5), 75% (95% CI 42.8 to 94.5), and 90.9% (95% CI 58.7 to 99.8) for urogenital, pharyngeal, and rectal sites, respectively. Cure rates for ciprofloxacin-resistant isolates were 96.6% (95% CI 94.2 to 98.3), 97.1% (95% CI 84.7 to 99.9), and 96.7% (95% CI 88.7 to 99.6), for urogenital, pharyngeal, and rectal sites, respectively. 21
This phase III trial found that single-dose 3 g zoliflodacin was noninferior to ceftriaxone plus azithromycin for treating uncomplicated urogenital gonorrhea. Cure rates at rectal and pharyngeal sites for the micro-ITT analysis were somewhat lower for zoliflodacin but similar to ceftriaxone with azithromycin for urogenital, pharyngeal, and rectal lesions. Cure rates at all sites exceeded 90% in the per-protocol analysis. In addition, differences in cure rate between zoliflodacin and ceftriaxone with azithromycin were similar at the pharyngeal and rectal sites. Adverse events were uncommon, with headache, neutropenia, and leukopenia reported most. While significant differences in adverse event frequencies for black or African American race or male sex were observed, the unbalanced race and sex of the sample may require a follow-up study to conclude that there is a true relationship. Just like in the phase II trial, no increase in zoliflodacin MICs was observed, further supporting its potential as a viable treatment option for drug-resistant N. gonorrhoeae urogenital infections. The subanalysis showed high cure rates at MICs ≤0.25, but the higher MIC isolates were few, which makes interpretation of efficacy difficult. In addition, zoliflodacin microbiological cure rates for ciprofloxacin-resistant isolates were >96% for urogenital, pharyngeal, and rectal lesions. A summary of findings from the phase II and III clinical trial safety and efficacy outcomes is available in Table 1.
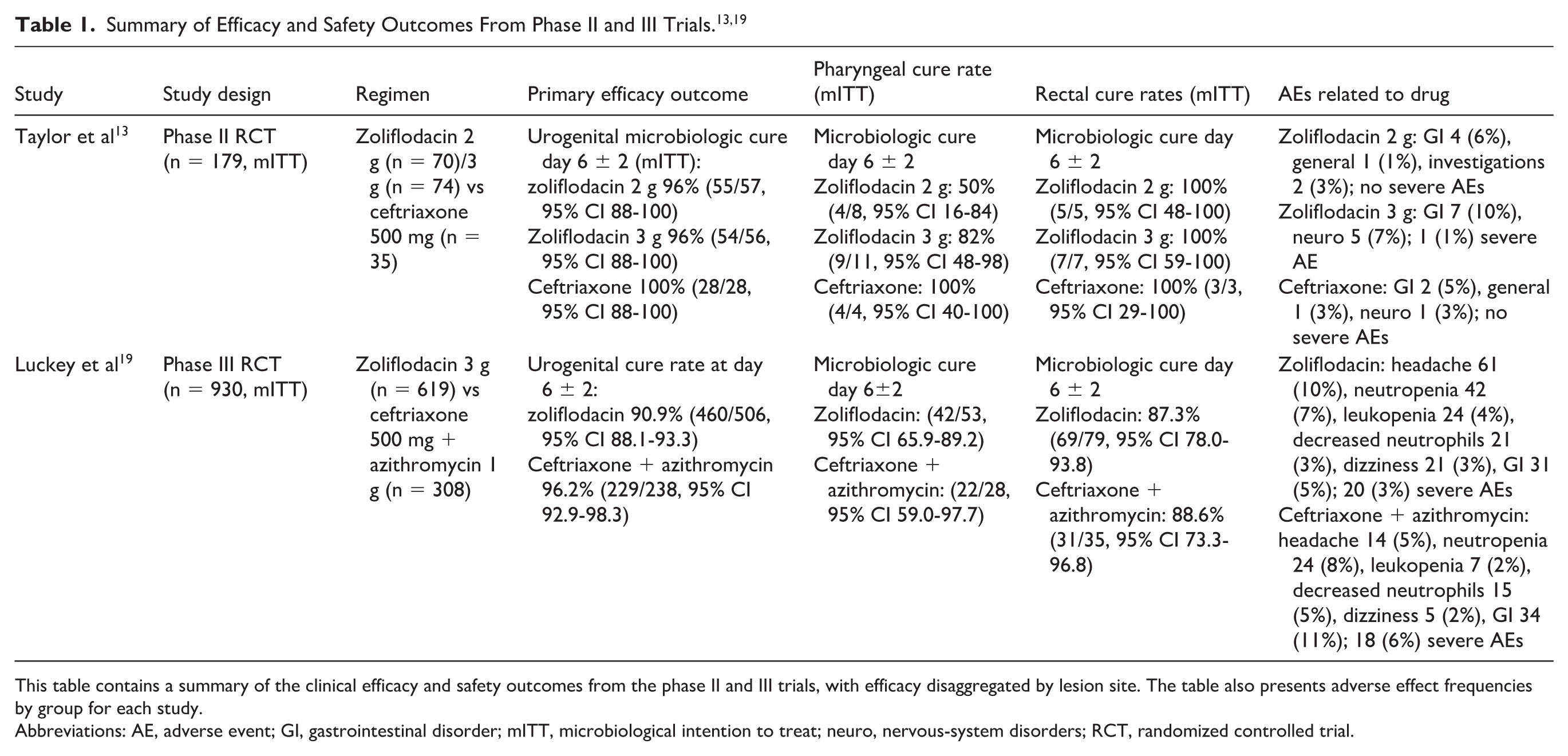
This table contains a summary of the clinical efficacy and safety outcomes from the phase II and III trials, with efficacy disaggregated by lesion site. The table also presents adverse effect frequencies by group for each study.
Abbreviations: AE, adverse event; GI, gastrointestinal disorder; mITT, microbiological intention to treat; neuro, nervous-system disorders; RCT, randomized controlled trial.
QTc Interval Safety Analysis
A study from Newman et al investigated the impact of zoliflodacin on QTc interval. The study was a preclinical in vivo study of 72 healthy subjects in a crossover design to receive zoliflodacin 2 g (n = 68), zoliflodacin 4 g (n = 66), 400 mg moxifloxacin (n = 70), and placebo (n = 69). Patients underwent the Holter electrocardiogram (ECG) analysis, and the primary outcome was time-matched change from baseline QTc (ΔΔQTcF). Secondary outcomes included other time-matched ECG parameters such as PR and QRS intervals, heart rate. Heart rate, T-wave morphology, PK, and PK/PD relationship were also assessed. 22
The primary outcome of change in QTc interval found a maximum least square mean ΔΔQTcF of 1.42 ms (95% CI –∞ to 3.044) at 3 hours after zoliflodacin 2 mg dose and 3.04 ms (95% CI −∞ to 4.674) at 4 hours after zoliflodacin 4 mg dose. The authors interpreted the results as no effect on cardiac repolarization and reported that similar trends were seen with ΔΔQTb and ΔΔQT values. 22 There were no significant changes in heart rate, PR, or QRS interval with either dose of zoliflodacin or placebo. At Cmax plasma concentrations, mean ΔΔQTcF was 1.5 ms (95% CI –∞ to 2.54) and 3.0 ms (95% CI –∞ to 4.41). The ECG showed prolonged QT interval (> 450 ms) in 7% and 4% of subjects in the 2 and 4 g zoliflodacin groups, respectively. Moxifloxacin resulted in 21% of subjects showing a prolonged QT. The authors did note that most new-onset changes in T-wave morphology occurred in the zoliflodacin groups. Changes included biphasic T-wave (n = 1, 4 g), inverted asymmetric T-wave (n = 1, 2 g; n = 2, 4 g). The authors considered these changes to be clinically insignificant, as these changes were in isolated ECGs and resolved. 22
Dosing and Administration
Zoliflodacin is available as a single-dose 3 g granules for oral suspension.6,23 According to prescribing information, the adult dose for an uncomplicated gonococcal infection is 3 g by mouth as a single dose. The dose is the same for pediatric patients ≥12 years old and ≥35 kg for uncomplicated gonococcal infection. There are no recommended dose adjustments for renal or hepatic function. 6
The prescribing information recommends administration on an empty stomach (1 hour before or 2 hours after food) for patients with a body mass of 35 to <50 kg and with food for patients ≥50 kg. The granules for oral suspension must be mixed with 60 mL of water before administration. Once consumed, the monograph recommends using an additional 60 mL of water to rinse the mixing container and consume the mixture to ensure the entire dose was administered. 6
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs
Zoliflodacin has several characteristics that prove relevant to patient care and current clinical practice. First is the availability of a new agent for an MDR organism, which addresses a major driver of treatment failure globally. Given zoliflodacin’s unique mechanism of action, cross-resistance may not be a concern, suggesting it could be efficacious and maintain activity against ciprofloxacin-, ceftriaxone-, and azithromycin-resistant N. gonorrhoeae strains. 2 This provides an option for patients infected with what was previously categorized as pan-resistant strains. Secondly, the oral single-dose administration avoids the requirement of injection-based therapy, allowing for easier treatment in outpatient settings and simplified partner therapy and adherence. In summary, zoliflodacin could serve as an oral alternative to ceftriaxone, especially in patients with a cephalosporin allergy, and be a viable option for resistance-directed therapy strategies. Continued surveillance will be imperative as zoliflodacin use increases.
Zoliflodacin’s place in therapy has not yet been defined by the CDC or WHO clinical practice guidelines, both of which were last updated in 2021.3,24 Due to the lack of evidence of resistance during the clinical trials, it may be expected that zoliflodacin will become a first-line agent. But because of the activity zoliflodacin has demonstrated against ceftriaxone-resistant strains and the limited samples from the clinical trials, it may be prudent to take a more cautious approach and reserve zoliflodacin for gonorrhea infections with resistance to the standard of care. This approach allows for a postmarketing trial and aggressive resistance tracking using the STI Surveillance Network. 25 This approach allows for a more comprehensive understanding of N. gonorrhoeae’s resistance response to zoliflodacin with use on a larger scale. In addition, the ceftriaxone resistance profile in the United States remains relatively controlled for the time being, which may influence the CDC to reserve zoliflodacin for resistant infections.
Zoliflodacin’s limited relative efficacy at extragenital sites has complicated clinical implications. 13 The 2021 CDC clinical practice guideline explains that pharyngeal lesions experience more treatment failure, which it states may be due to lower antibiotic concentrations in the pharynx, diversity in commensal Neisseria population causing horizontal gene transfer, biofilm or colonization dynamics, and that pharyngeal infections are more frequently asymptomatic. 3 This further supports that pharyngeal gonorrhea infections remain difficult to treat and ceftriaxone remains a more effective treatment option with the current evidence. Decreased rectal lesion efficacy is less concerning, since cure rates were still acceptable, just not as high as urogenital lesions. 13 The rationale for the decreased rectal cure rates isn’t explicit and may be a worthwhile topic of future study. We recommend site-specific PK studies and PD modeling incorporating MIC distributions to better understand the difference in efficacy by site. Regarding resistance, we recommend postmarketing resistance monitoring since resistance data have been based on relatively small samples in highly controlled environments. Finally, we also recommend efficacy and safety monitoring and more diverse populations, including populations beyond the inclusion criteria of the phase II and III trials (eg, pediatric adolescent population), for cure rates, drug-drug interactions, and investigating the neutropenia phenomenon seen in the phase III trial.
Conclusion
Zoliflodacin has demonstrated that its efficacy for treatment of uncomplicated urogenital N. gonorrhoeae infections is comparable to the standard of care. Pharyngeal and rectal lesion cure rates were lower than urogenital cure rates but were similar to the standard of care. Adverse events were generally mild and uncommon, with headache, neutropenia, and leukopenia accounting for most of the events. Zoliflodacin does not show evidence of increased MICs in response to treatment. Zoliflodacin offers a practical alternative to ceftriaxone—especially for patients with cephalosporin allergies—though ongoing resistance surveillance is important as its use increases. Additional evidence of zoliflodacin’s efficacy in treating pharyngeal and rectal lesions, further PK/PD studies, and expanded postmarketing safety and efficacy for urogenital infections can help determine its place in therapy.
Footnotes
Acknowledgements
The authors would like to thank Dr Kevin Garey for his guidance and support during the writing of this text.
Author Contributions
All authors contributed equally to this manuscript, including conceptualization, data curation, methodology, visualization, and writing the original draft. All authors have seen and approved the final draft of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI Use
No AI was used in the development of this manuscript.