
Abstract
Objective:
To evaluate the efficacy and safety of adding pioglitazone as a third-line agent in patients with type 2 diabetes mellitus (T2DM) inadequately controlled on metformin and sodium-glucose cotransporter-2 inhibitors.
Data Sources:
A systematic search of PubMed, Scopus, the Cochrane Library, and Google Scholar was conducted through February 2026 for randomized controlled trials (RCTs).
Study Selection and Data Extraction:
Eligible RCTs reported outcomes on glycemic control and cardiometabolic parameters. Two reviewers independently screened studies, extracted data, and assessed risk of bias using the Cochrane Risk-of-Bias tool 2, with certainty of evidence evaluated using the Grading of Recommendations Assessment, Development, and Evaluation tool.
Data Synthesis:
Four RCTs (n = 1213) were included. Using a random-effects model, pioglitazone significantly reduced glycated hemoglobin (HbA1c) (mean difference [MD]: −0.56%; 95% confidence interval −0.74 to −0.38; P < 0.00001) and increased the likelihood of achieving HbA1c <7% (risk ratio: 2.37; 95% CI 1.87-3.01). Subgroup analysis demonstrated a dose-dependent effect, with 30 mg providing greater glycemic reduction than 15 mg. Significant improvements were also observed in fasting plasma glucose, homeostasis model assessment of insulin resistance, triglycerides, high-density lipoprotein cholesterol, and diastolic blood pressure. However, pioglitazone was associated with weight gain (MD: 2.38 kg) and a higher risk of adverse drug reactions.
Relevance to Patient Care and Clinical Practice:
These findings suggest that pioglitazone is an effective add-on therapy for patients with T2DM who remain uncontrolled on metformin and SGLT2 inhibitors, particularly in those with significant insulin resistance. However, its use should be individualized, with careful consideration of predictable adverse effects such as weight gain and tolerability, rather than routine escalation for all patients.
Conclusions:
Adding pioglitazone to metformin and SGLT2 inhibitors significantly improves glycemic control and metabolic parameters. While the 30 mg dose offers greater efficacy, clinicians must balance these benefits against predictable side effects like weight gain.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder that poses a significant global public health concern, affecting approximately 11% of adults between 20 and 80 years of age, imposing a substantial health care and socioeconomic burden worldwide. 1 The pathophysiology of T2DM primarily involves the inability of tissues to respond to insulin due to the defective secretion of insulin by pancreatic β-cells, disrupting glucose homeostasis. 2 Despite the widespread use of metformin as the first-line therapy for the clinical management of T2DM, many patients failed to reach clinical endpoints, such as glycemic control (glycated hemoglobin [Hb1Ac] target), and lipid profile, because of the multiple pathophysiological defects, for which combination therapy involving antidiabetic drugs is now being used to treat. 3 However, if the patients still fail to achieve glycemic targets, then a third-line agent is typically added to the regimen to enhance results.
Among all the oral antidiabetic drugs (OADs), sodium-glucose cotransporter-2 (SGLT2) inhibitors are commonly used as combination therapy with metformin, as these are the only novel class of drugs that inhibit renal glucose reabsorption through the blockade of SGLT2 cotransporters in the proximal tubules, thereby lowering the plasma glucose concentration independently of insulin secretion. 4 It has been reported that these drugs have demonstrated significant reductions in HbA1c and body weight when added to the background therapy. A study evaluating empagliflozin (10 and 25 mg) as an add-on to the background metformin treatment for 24 weeks reported that empagliflozin significantly improved glycemic control, HbA1c levels, weight, and blood pressure (BP) in comparison with placebo. 5 Substantial evidence also suggests that SGLT2 inhibitors help in reducing major adverse cardiovascular events (MACEs), hospitalizations for heart failure (HHF), and significantly improve renal outcomes in patients with T2DM. 6 Nonetheless, despite their favorable safety profile, these antidiabetic agents showed certain adverse events, including euglycemic diabetic ketoacidosis (euDKA), constant reduced BP, and genitourinary infections. 7 Despite the therapeutic benefits, patients with pronounced insulin resistance fail to achieve the recommended glycemic targets when treated with the dual therapy of metformin with SGLT2 inhibitors. This highlights the need to use third-line agents for obtaining optimal combination therapies.
Pioglitazone belongs to the thiazolidinedione class of antidiabetic drugs that works by the stimulation of nuclear transcription factor peroxisome proliferator-activated receptor-γ (PPAR-γ), which is involved in lipid and glucose metabolism. 8 It improves insulin responsiveness across peripheral and hepatic tissues, leading to further reductions in HbA1c and reduces the levels of fasting plasma glucose (FPG) and insulin resistance, which ultimately reduces the risk of myocardial infarction and stroke. 9 However, the use of pioglitazone as a monotherapy can cause fluid retention, resulting in plasma volume expansion and weight gain and heart failure. 10
The impact of adding pioglitazone as an added therapy to metformin and SGLT2 inhibitors to control T2DM is shown by recent randomized controlled trial (RCT), demonstrating significant improvements in HbA1c, fasting glucose, achieving recommended glycemic rates, and boost homeostasis model assessment of insulin resistance (HOMA-IR) levels.8,9 This meta-analysis is an updated synthesis of available evidence to determine the effectiveness and safety of this strategy and to support evidence-based clinical practice. GLP-1 receptor agonists are increasingly incorporated into treatment algorithms due to their favorable glycemic and weight-loss benefits. However, GLP-1 receptor agonists are high-cost, the injectable route limits acceptance, gastrointestinal side effects limit adherence, and oral options are still preferred in many real-world settings in low- and middle-income countries. Therefore, pioglitazone is an inexpensive oral insulin-sensitizing agent with a complementary mechanism of action that directly targets one of the central pathophysiological defects in T2DM. This makes the combination of metformin, SGLT2 inhibitors, and pioglitazone highly relevant to real-world clinical practice, particularly in second- and third-world countries where oral combination regimens are used commonly.
Material and Methods
This meta-analysis was reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 11 A PRISMA checklist is given in Supplemental Table 1. The protocol for this meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the reference number CRD420261319950.
Data Sources and Search Strategy
A thorough search was carried out using PubMed/MEDLINE, Scopus, Cochrane Library, and Google Scholar databases. The reference lists of the retrieved publications, as well as previous systematic reviews and meta-analyses, were examined for relevant articles. The search method placed no constraints on publishing status or language. The search words included relevant MeSH terms and associated keywords, such as (“pioglitazone” OR “thiazolidinedione” OR “glitazone”) AND (“metformin”) AND (“dapagliflozin” OR “SGLT2 inhibitor” OR “empagliflozin”) AND (“diabetes mellitus type 2” OR “T2DM”). Although individual SGLT2 inhibitors such as canagliflozin were not explicitly included as separate keywords, the use of the broader term “SGLT2 inhibitor” was intended to capture all agents within this class. Furthermore, all eligible RCTs identified in the final analysis evaluated dapagliflozin or empagliflozin as background therapy, with no relevant studies involving canagliflozin meeting the inclusion criteria. This likely reflects regional prescribing patterns and the availability of SGLT2 inhibitors in the populations studied. The detailed search strategy will be provided in Supplemental Table 2.
Study Selection and Eligibility Criteria
All articles retrieved through the systematic search were imported into the EndNote reference library, version X8.1 (Clarivate Analytics), where duplicates were there after omitted. Primary screening was performed by going through the title and abstract, followed by secondary or full-text screening, performed independently by 2 reviewers using Rayyan.AI. Conflicts were resolved by consensus and adjudication by a third reviewer where necessary. Rayyan.AI is an automated AI that effectively enables the inclusion and exclusion of articles and saves time for reviewers. Two authors independently examined and chose studies, and any differences were handled by a third author. Selected studies were retrieved for full-text review to ensure relevance. The inclusion criteria were defined using the Population, Intervention, Control, and Outcomes (PICO) methodology for systematic reviews, where:
This meta-analysis included RCTs comparing the addition of pioglitazone with placebo or no additional glucose-lowering therapy in adults with T2DM inadequately controlled on background treatment with metformin and an SGLT2 inhibitor. Studies enrolling patients receiving stable doses of metformin plus an SGLT2 inhibitor were eligible. The trials that explicitly specify 2 different doses of pioglitazone added to background therapy with metformin plus an SGLT2 inhibitor were considered for subgroup analysis.
Data Extraction
On a pre-piloted Microsoft Excel sheet, 2 authors independently evaluated the data and supplemental resources; disagreements were settled by consulting a third author. From the selected studies, the following information was extracted: study labels, year of publication, study design, number of participants in each arm, baseline patient characteristics (eg, age, sex, body mass index [BMI], systolic blood pressure [SBP], diastolic blood pressure [DBP], total cholesterol, and insulin), and results about the effectiveness and safety profile. Effectiveness endpoints included change in HbA1c and proportion of patients achieving glycemic targets (eg, HbA1c <7%). While safety endpoints included adverse events (edema, hypoglycemia, and serious adverse events), and treatment discontinuation due to adverse events.
Quality Assessment
Two authors independently assessed the quality and risk of bias of the included studies. For RCTs, the Cochrane Risk-of-Bias tool 2.0 (RoB 2.0) was used. 12 This tool assesses the risk of bias associated with the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Judgments were categorized as “Low risk,” “High risk,” or “Some concerns.”
Statistical Analysis
Two authors conducted the integration of study findings using Review Manager (RevMan version 5.4; Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2014). For dichotomous outcomes (eg, achievement of glycemic targets and safety outcomes), we calculated pooled RR with their 95% confidence intervals (CIs). For continuous outcomes (eg, change in HbA1c, FPG, HOMA-IR, and body weight), mean differences (MDs) with 95% CI were computed. We combined the findings from all included research using the Mantel-Haenszel random-effects model, and we displayed them in forest plots. A P-value of less than 0.05 was considered statistically significant. Utilizing the Higgins I² index, statistical heterogeneity was evaluated. High heterogeneity is indicated by I² > 50%, moderate by I² 25% to 50%, and low by <25%. Prespecified subgroup analyses were conducted according to the pioglitazone dose (15 vs 30 mg). Sensitivity analyses were performed by sequential exclusion of individual studies to assess the robustness of the findings.
Certainty of Evidence
We used a GRADE (Grading of Recommendations Assessment, Development, and Evaluation) tool to assess the overall quality and strength of evidence for each primary and secondary outcome. 13
Results
Study Selection
A total of 707 records were identified from PubMed (n = 257), the Cochrane Library (n = 118), Google Scholar (n = 100), and Scopus (n = 232). Of these, 350 duplicates and 13 records removed for other reasons were excluded, as they contained animal population, leaving 344 records for screening. Following title and abstract screening, 331 records were excluded due to irrelevance or ineligible study design. Full-text articles were sought for the remaining 13 records. All 13 full-text articles were assessed for eligibility; 9 were excluded, including ongoing trials (n = 3), conference abstracts (n = 4), and use of a different intervention (n = 1). 14 Finally, 4 studies (RCTs) met all eligibility criteria, including one newly identified record, and were included in the review (Figure 1).15-18
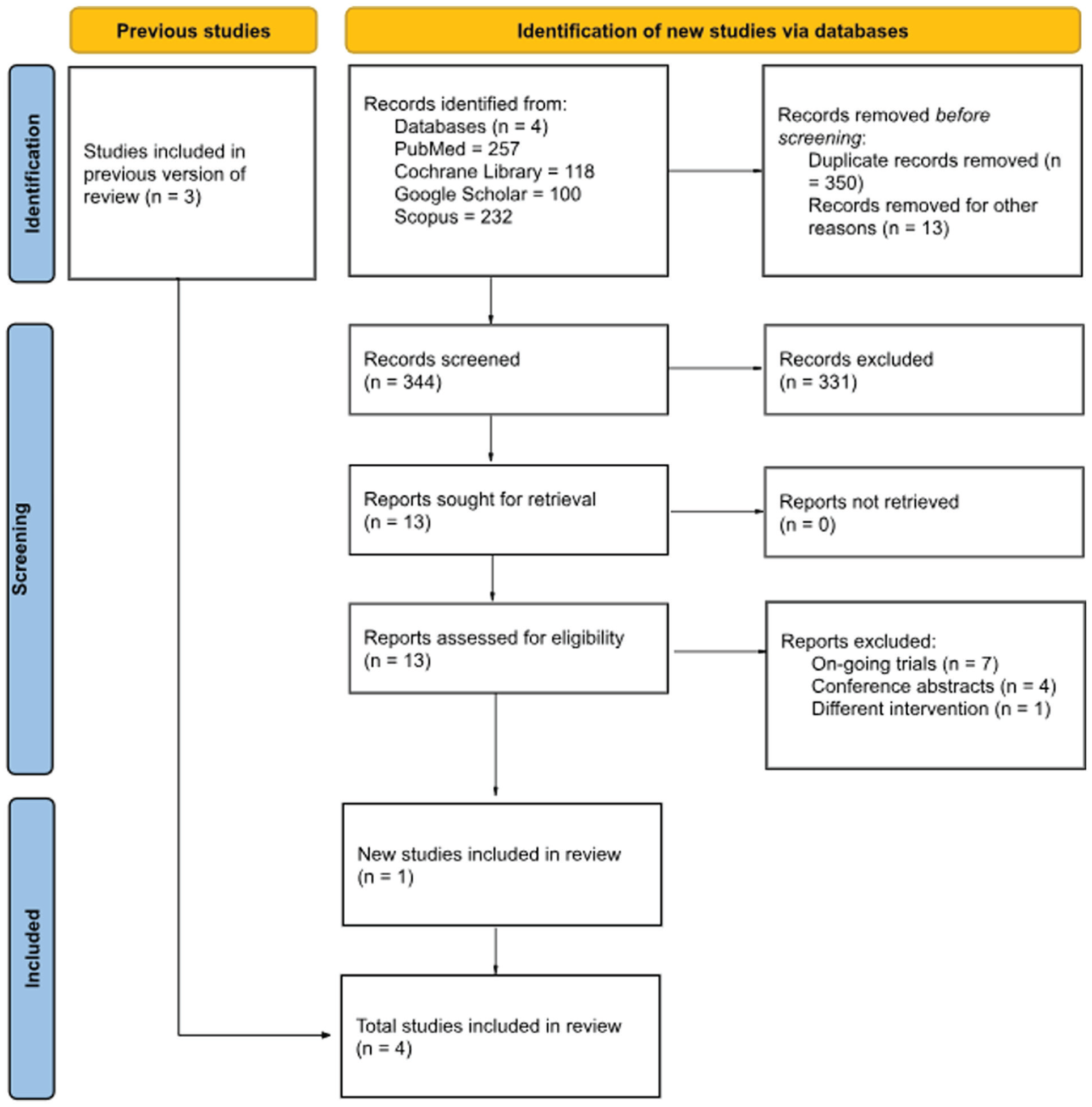
PRISMA flow diagram of study selection.
Baseline Characteristics
Table 1 summarizes the baseline characteristics of participants across 4 RCTs (Cho et al 2024, Heo et al 2024, Lim et al 2024, and Hong et al 2025) evaluating the efficacy of pioglitazone for T2DM. All studies were conducted in South Korea and utilized dapagliflozin as the background SGLT2 inhibitor. A total of 1213 participants were included.
Baseline Characteristics of Included Randomized Controlled Trials.
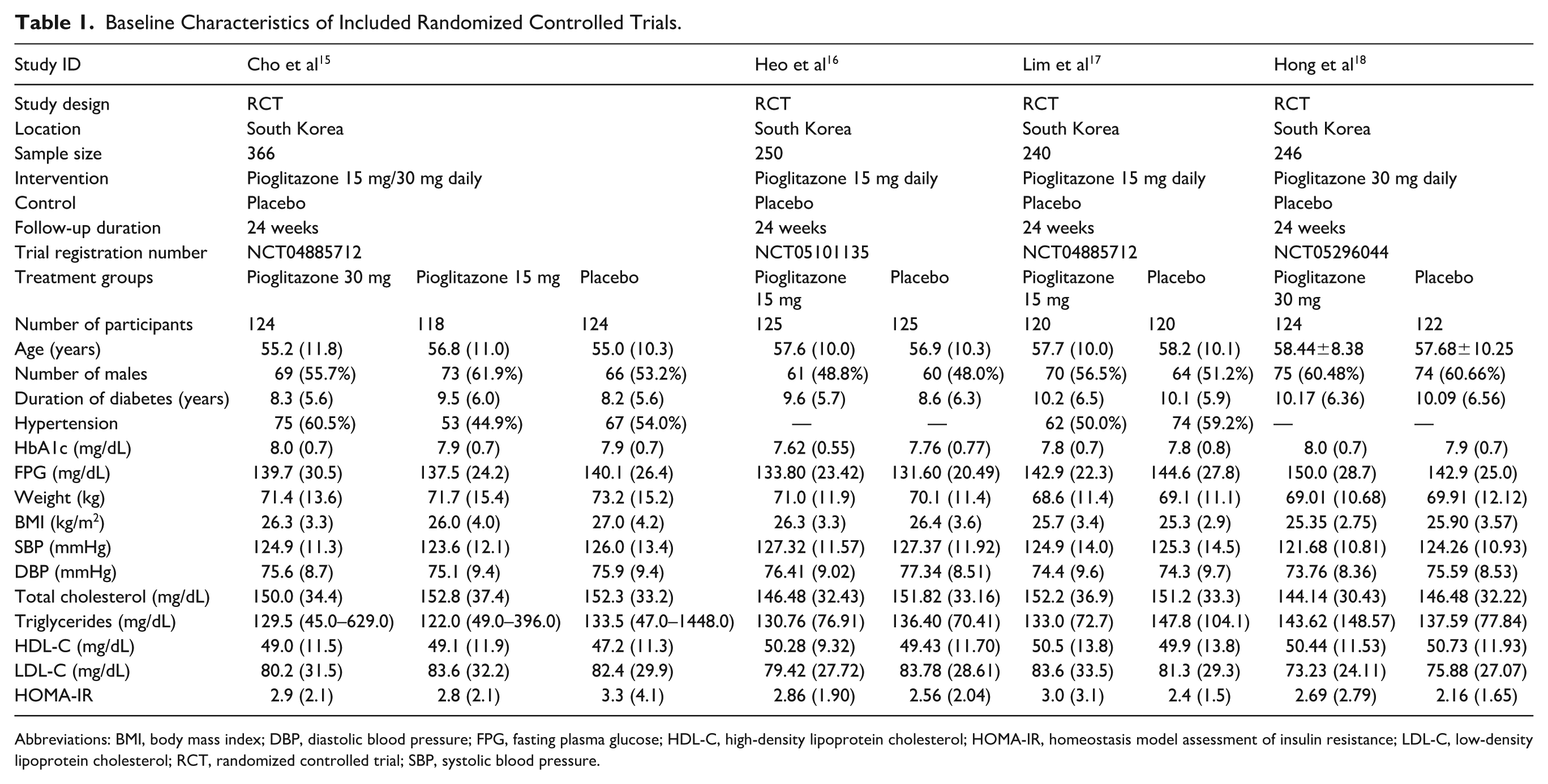
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; RCT, randomized controlled trial; SBP, systolic blood pressure.
Baseline characteristics were compared descriptively across studies to assess clinical comparability. Formal statistical comparisons were not performed, as participants were not randomized between trials, and such analyses may be misleading in the context of cross-study comparisons.
Overall, the study populations were broadly comparable. Mean age ranged approximately from 55 to 58 years, and the proportion of male participants varied between 48% and 62%. Duration of diabetes was similar across trials, ranging approximately from 8 to 10 years. Baseline glycemic parameters were consistent, with HbA1c levels between 7.6% and 8.0%, and FPG values ranging approximately from 131 to 150 mg/dL.
Anthropometric measures were also comparable, with mean BMI values between 25.3 and 27.0 kg/m² and body weight ranging approximately from 68 to 73 kg. Cardiovascular parameters, including SBP and DBP, as well as lipid profiles (total cholesterol, TGL, HDL-C, and low-density lipoprotein cholesterol [LDL-C]), showed minimal variation across studies.
Some heterogeneity was observed in the prevalence of hypertension and HOMA-IR values, as well as minor differences in age distribution and metabolic parameters. In addition, variation in pioglitazone dosing (15 vs 30 mg) and study-specific inclusion criteria may have contributed to these differences. However, these variations were not considered clinically substantial and are unlikely to significantly impact the overall comparability of the study populations.
Risk-of-Bias Assessment
To evaluate the risk of bias in the included studies, we employed the Cochrane RoB 2 tool. Figure 2 illustrates that all 4 included studies had a low RoB across all 5 domains: bias arising from the randomization process (D1), bias due to deviations from intended interventions (D2), bias due to missing outcome data (D3), bias in the measurement of outcomes (D4), and bias in the selection of the reported results (D5).
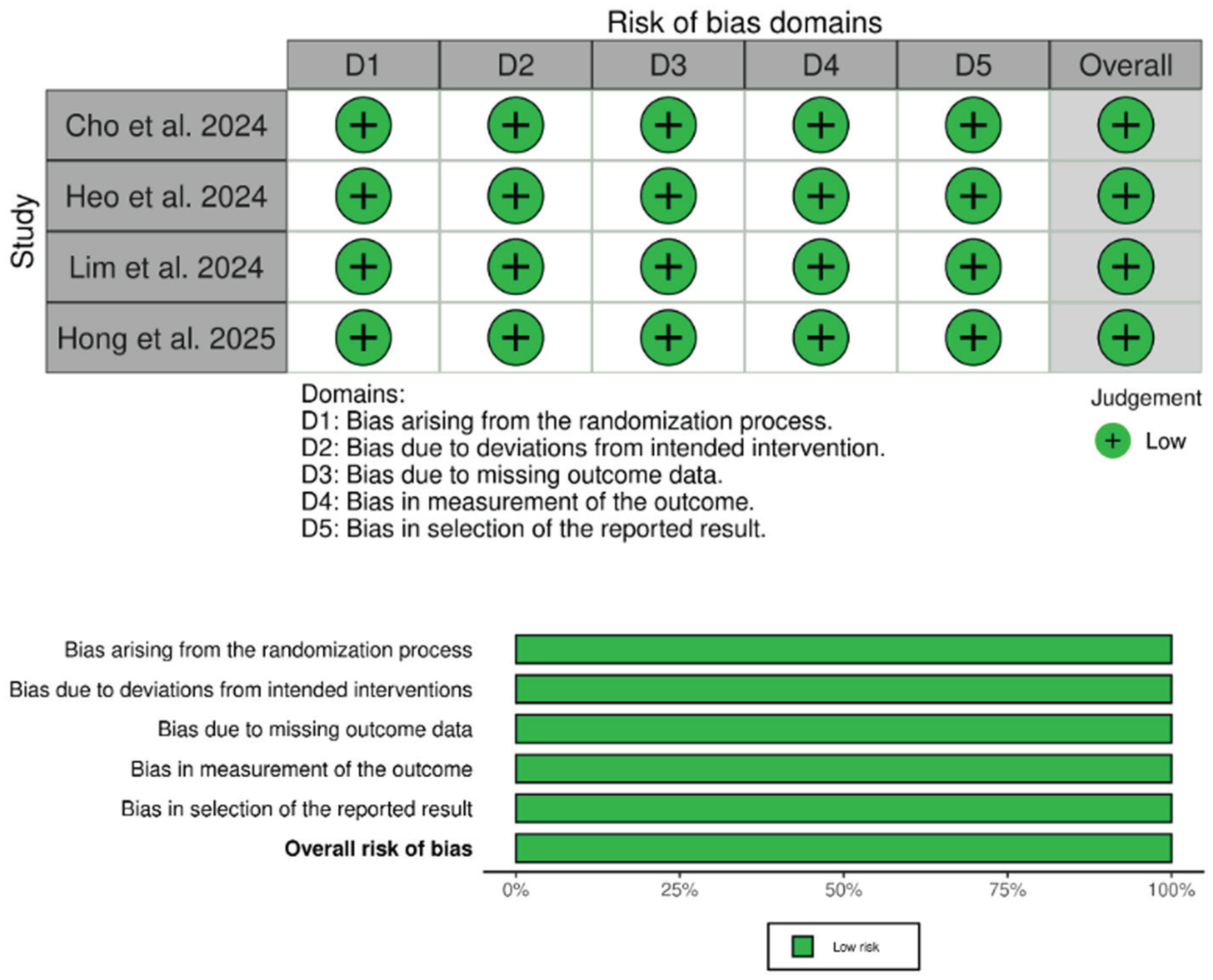
Risk-of-bias assessment using the Cochrane RoB 2 tool.
Meta-Analysis of Primary Outcomes
Change in HbA1c
Pioglitazone significantly reduced HbA1c levels compared with the control group, with a pooled MD of −0.56% (95% CI −0.74 to −0.38, P < 0.00001, I² = 73%) (Figure 3a).
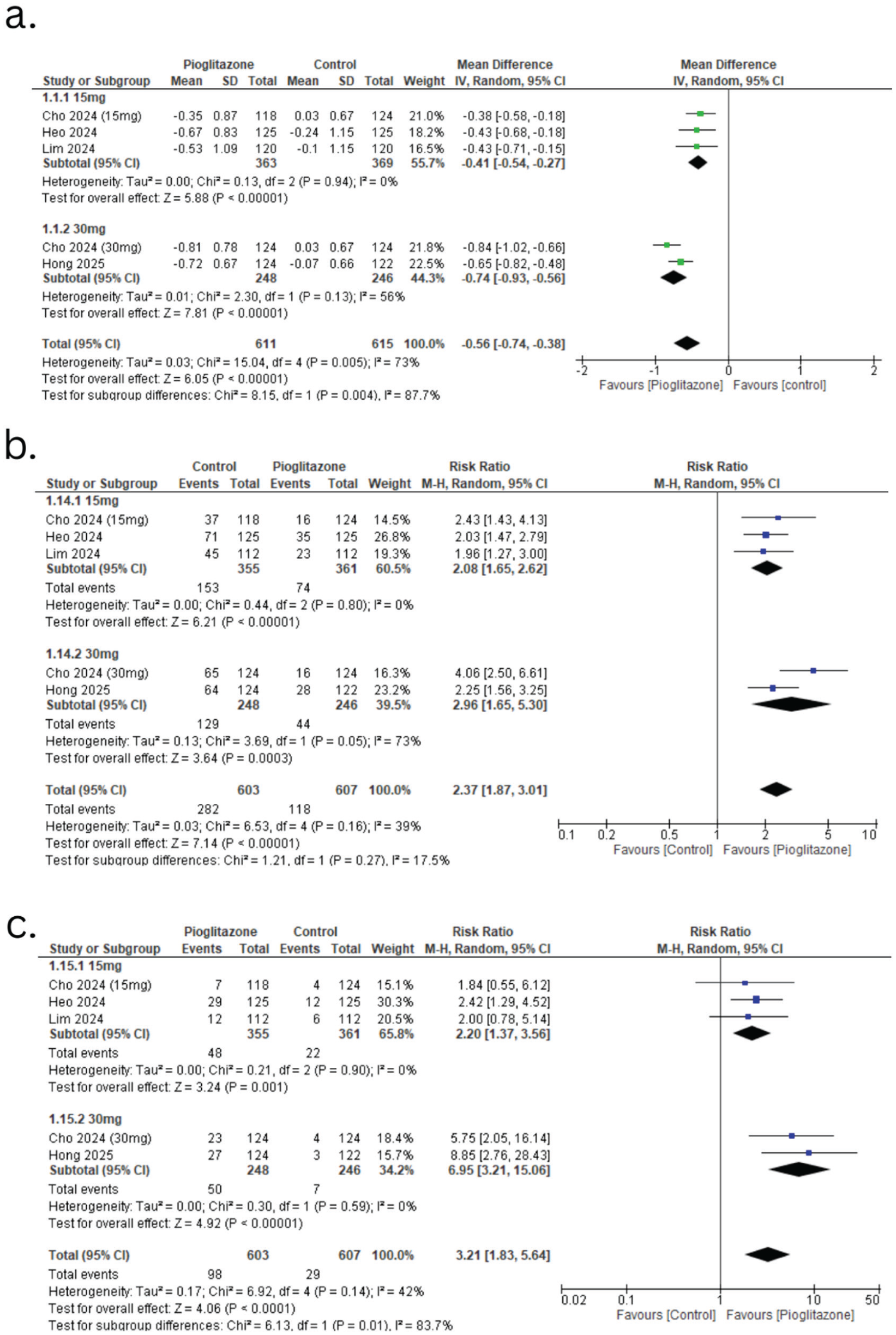
Forest plots of primary glycemic outcomes. (a) Change in HbA1c levels. (b) Achievement of HbA1c <7%. (c) Achievement of HbA1c <6.5%.
Achievement of HbA1c <7% and <6.5%
The proportion of patients achieving HbA1c <7% was significantly higher in the pioglitazone add-on group, with a pooled RR of 2.37 (95% CI 1.87-3.01, P < 0.00001, I² = 39%) (Figure 3b). In addition, pioglitazone increased the likelihood of achieving HbA1c <6.5%, with a pooled RR of 3.21 (95% CI 1.83-5.64, P = 0.001, I² = 42%) (Figure 3c).
Subgroup analysis revealed a dose-dependent effect, with the 30 mg dose of pioglitazone showing a greater reduction in HbA1c and higher rates of achieving both HbA1c <7% and <6.5% compared with the 15 mg dose.
Meta-Analysis of Secondary Outcomes
Endocrine Outcomes
Pioglitazone significantly reduced FPG (mg/dL) levels compared with the control group. The pooled MD was −14.71 (95% CI −18.70 to −10.71, P < 0.00001, I² = 34%), as shown in Figure 4a.
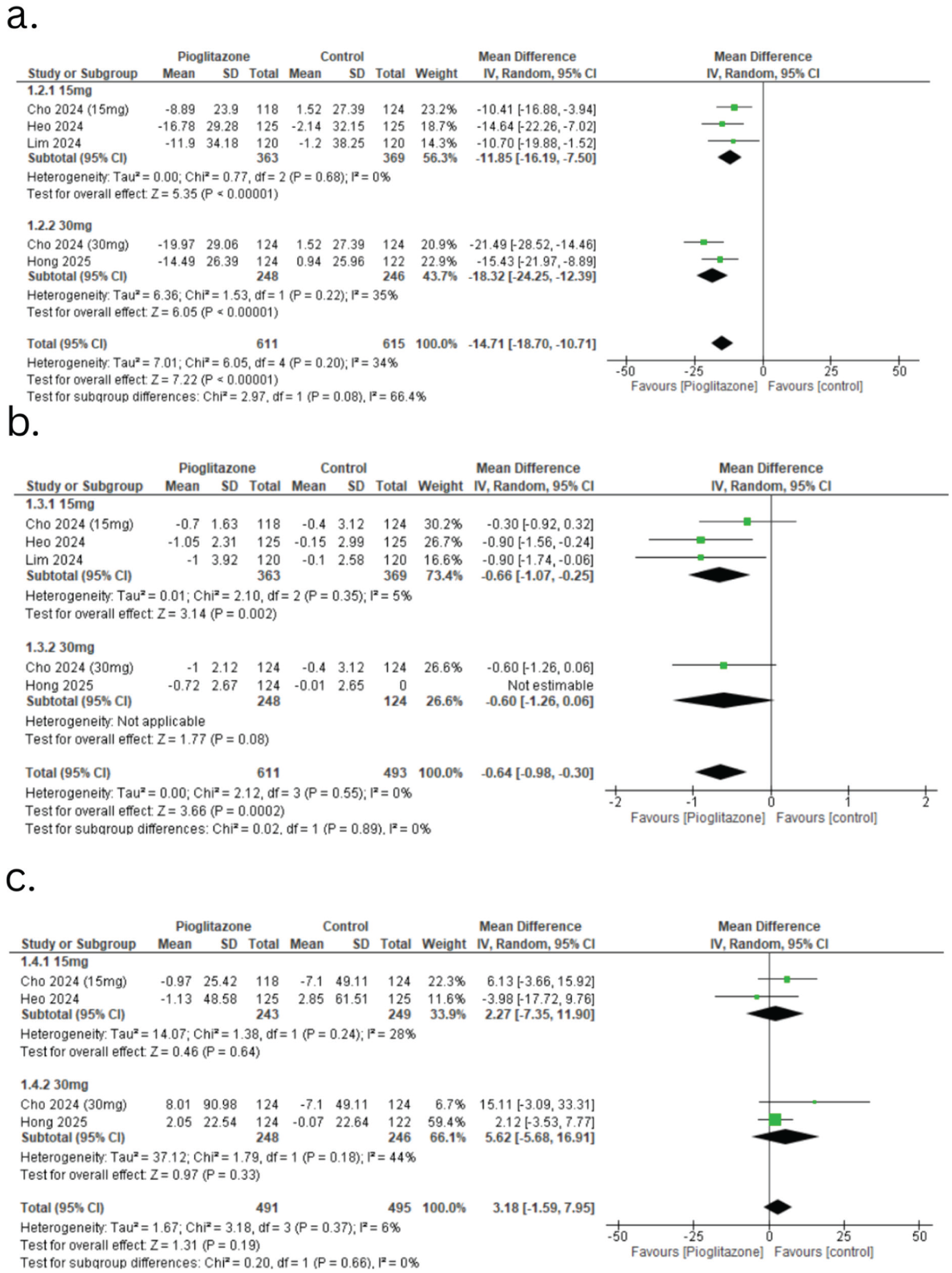
Forest plots of endocrine outcomes. (a) Change in fasting plasma glucose (FPG). (b) Change in insulin resistance (HOMA-IR). (c) Change in β-cell function (HOMA-B).
The effect of pioglitazone on insulin resistance (HOMA-IR) also showed a significant reduction, with a pooled MD of −0.64 (95% CI −0.98 to −0.30, P = 0.0002, I² = 0%) (Figure 4b). However, no significant difference was noted in HOMA-Beta between the pioglitazone and control groups, with a pooled MD of 3.18 (95% CI −1.59 to 7.95, P = 0.19, I² = 6%) (Figure 4c).
Cardiovascular Outcomes
For SBP (mmHg), no significant effect was observed, with a pooled MD of −0.95 (95% CI −2.45 to 0.55, P = 0.22, I² = 0%) (Figure 5a). However, there was a significant reduction in DBP (mmHg), with a pooled MD of −1.59 (95% CI −2.66 to −0.52, P = 0.004, I² = 0%) (Figure 5b).
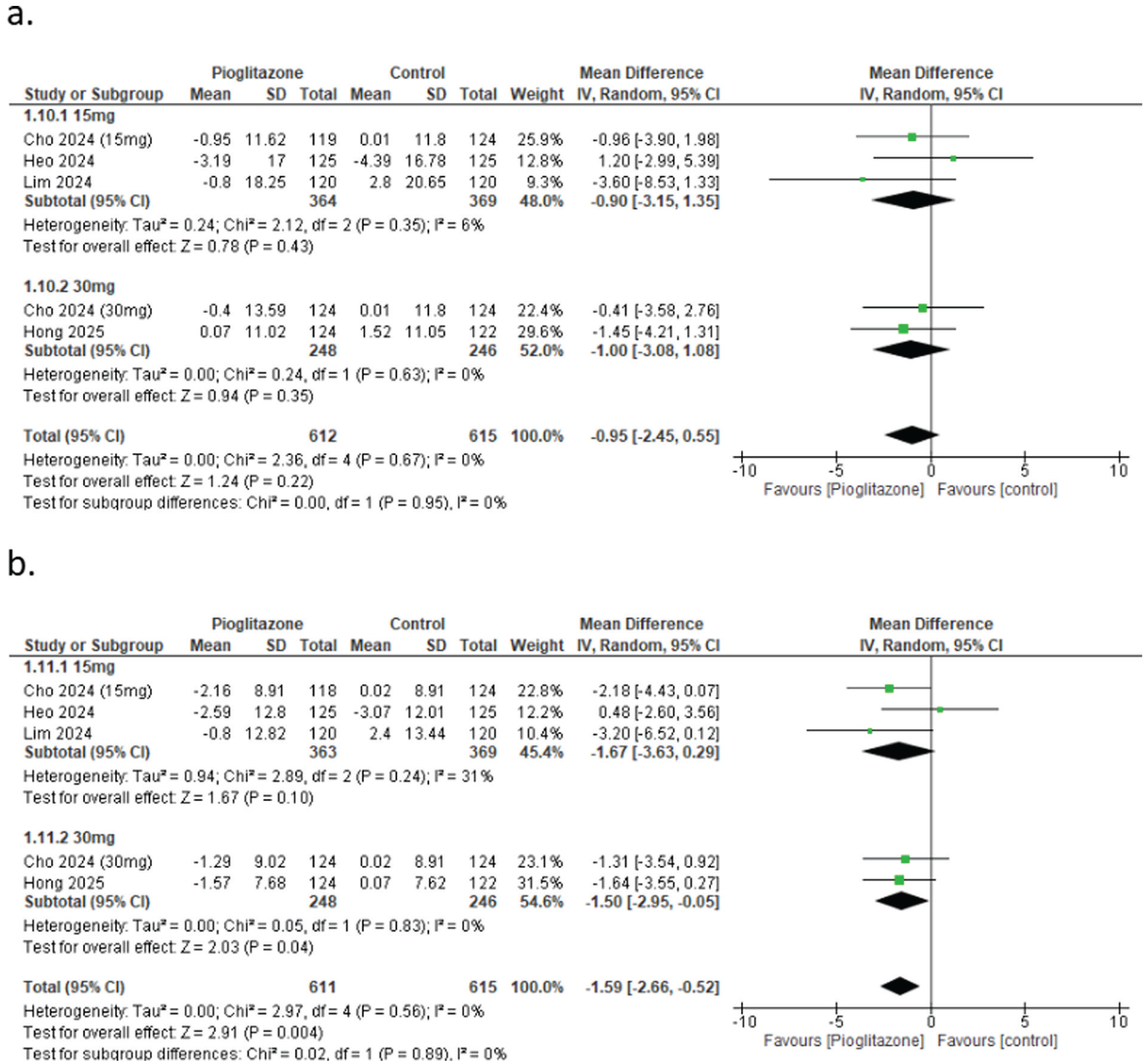
Forest plots of cardiovascular outcomes. (a) Change in systolic blood pressure (SBP). (b) Change in diastolic blood pressure (DBP).
Lipid Profile
Pioglitazone had no significant effect on total cholesterol (mg/dL) (MD = 2.39, 95% CI −1.38 to 6.16, P = 0.21, I² = 0%) (Figure 6a) or LDL-C (mg/dL) (MD = −0.95, 95% CI −4.41 to 2.51, P = 0.59, I² = 0%) (Figure 6b).
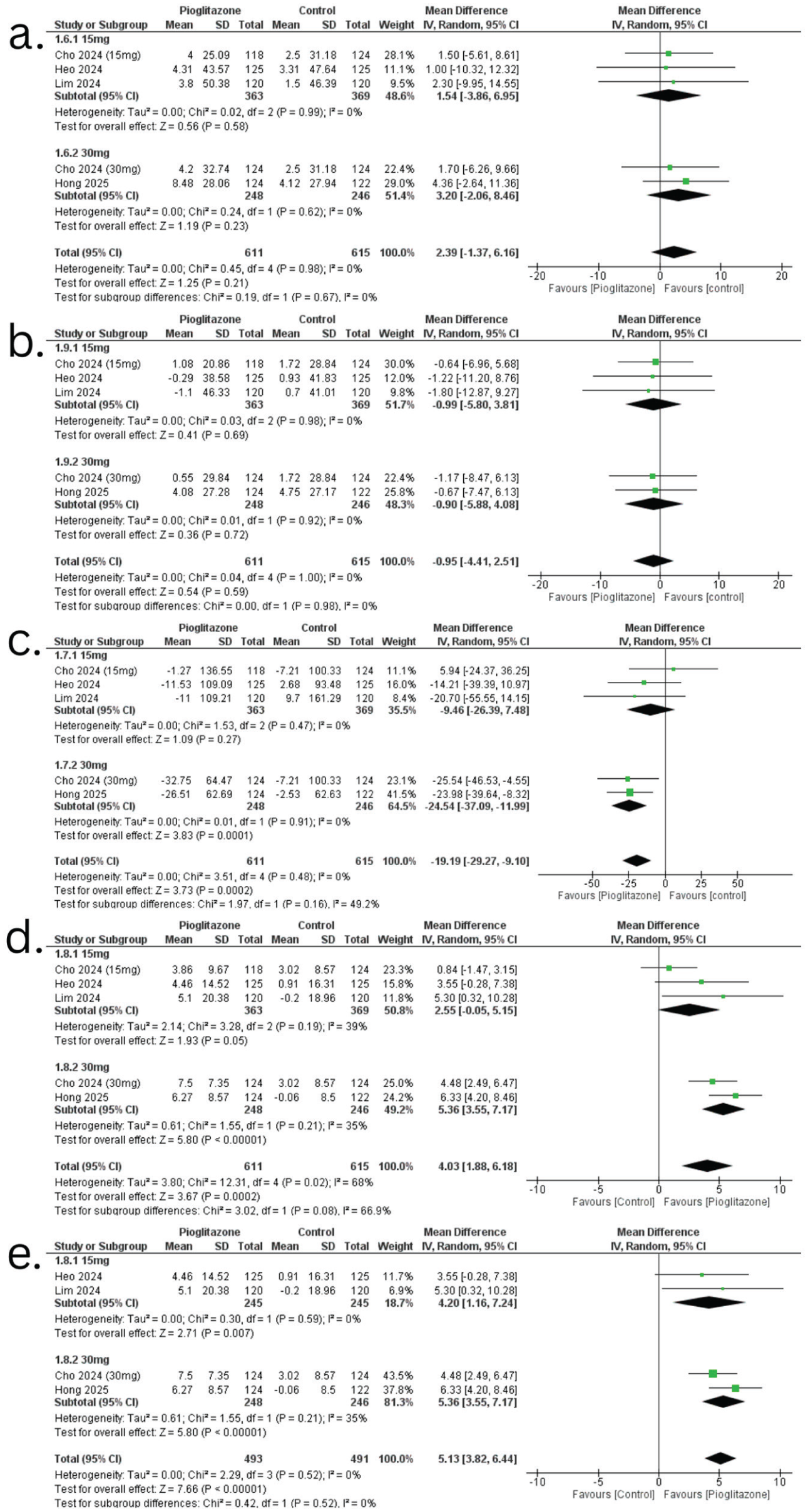
Forest plots of lipid profile outcomes. (a) Change in total cholesterol. (b) Change in low-density lipoprotein cholesterol (LDL-C). (c) Change in triglycerides. (d) Change in high-density lipoprotein cholesterol (HDL-C). (e) Leave-one-out sensitivity analysis for HDL-C stratified by 15 and 30 mg doses.
However, there was a significant reduction in TGL (mg/dL) (MD = −19.19, 95% CI −29.27 to −9.10, P < 0.0002, I² = 0%) (Figure 6c) and a significant increase in HDL-C (mg/dL) levels, with a pooled MD of 4.03 (95% CI 1.88-6.18, P = 0.0002) (Figure 6d).
To address the moderate-to-high heterogeneity observed in Change in HDL-C, we conducted a leave-one-out sensitivity analysis. The analysis revealed a significant effect of pioglitazone compared with the control, with a pooled MD of 4.20 (95% CI 1.16-7.24, P = 0.007) for the 15 mg dose and 5.36 (95% CI 3.55-7.17, P < 0.00001) for the 30 mg dose. The total analysis across all studies demonstrated a pooled MD of 5.13 (95% CI3.82-6.44, P < 0.00001), indicating a robust effect of pioglitazone on HDL-C (Figure 6e).
Safety Outcomes
Pioglitazone caused a significant increase in body weight (kg), with a pooled MD of 2.38 (95% CI 2.05-2.71, P < 0.00001, I² = 0%) (Figure 7a).
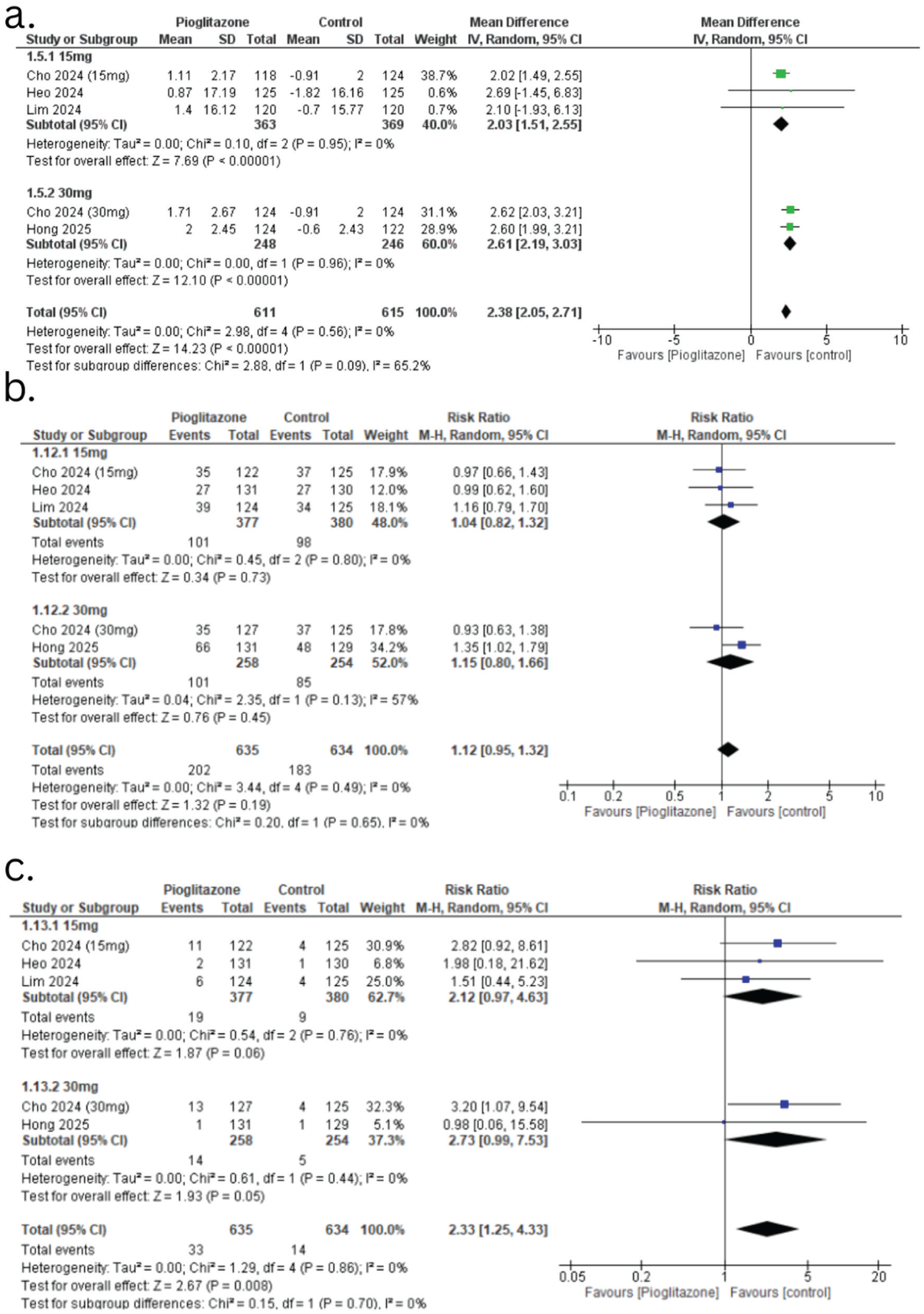
Forest plots of safety outcomes. (a) Change in body weight. (b) Treatment-emergent adverse events (TEAEs). (c) Adverse drug reactions (ADRs).
The incidence of treatment-emergent adverse events (TEAEs) was similar between the pioglitazone and control groups, with a pooled RR of 1.12 (95% CI 0.95-1.32, P = 0.19) (Figure 7b). Pioglitazone showed a statistically significant higher risk of adverse drug reactions (ADRs), with a pooled RR of 2.33 (95% CI 1.25-4.33, P = 0.008) (Figure 7c).
GRADE Assessment (Certainty Evidence)
Certainty of evidence ranged from moderate to high across outcomes (Supplemental Table 3). HbA1c and FPG were rated as moderate certainty due to heterogeneity, while most other outcomes were high certainty.
Discussion
This updated systematic review and meta-analysis was conducted to evaluate the efficacy and safety of adding pioglitazone to background therapy with metformin and SGLT2 inhibitors in adults with T2DM inadequately controlled on dual therapy. Although metformin combined with SGLT2 inhibitors is a widely adopted second-line regimen due to its glucose-lowering effects independent of insulin and established cardiovascular and renal benefits, a significant proportion of patients with marked insulin resistance fail to achieve recommended glycemic targets on this combination alone.19-21 A recent meta-analysis specifically examining pioglitazone add-on to metformin and dapagliflozin documented improved glycemic outcomes in this setting. 8 Pioglitazone, a thiazolidinedione and PPAR-γ agonist, provides a complementary mechanism of action by improving peripheral and hepatic insulin sensitivity. 22 Early evidence supports pioglitazone’s insulin-sensitizing effects and favorable changes in lipid metabolism in T2DM more broadly.23,24 Historically, concerns about weight gain and fluid retention associated with thiazolidinediones have tempered use, although these effects are predictable and manageable in many patients. 23 Taken together, these considerations position pioglitazone as a rational third-line option in patients with persistent insulin resistance despite optimized dual therapy. By incorporating more recent RCTs and applying stringent methodological standards, this study aims to provide an updated, comprehensive review of the available evidence, clarifying the balance among glycemic efficacy, metabolic effects, and safety outcomes associated with pioglitazone as a third-line add-on therapy to metformin and SGLT2 inhibitors.
Results were updated from the previous meta-analysis. 8 The primary findings of our study demonstrated a significant reduction in HbA1c with pioglitazone add-on therapy compared with the control group for both HbA1c <7% and <6.5% targets, with substantial heterogeneity. However, in the previous study, negligible heterogeneity was present. Our study then proceeded with a subgroup analysis of 2 dosage groups, which accounted for the heterogeneity in the results. Our study presented a new finding not reported in the previous study: the 30 mg dose had a better effect on HbA1c levels. The magnitude of HbA1c reduction reflects pioglitazone’s complementary mechanism of action: it enhances insulin sensitivity through PPAR-γ activation, modulates gene transcription, and increases glucose uptake in peripheral tissues. However, insulin secretion does not increase; instead, it reduces insulin resistance, thereby lowering HbA1c.22,25,26 It also works synergistically with the glucose excretion effects of SGLT2 inhibitors and with metformin’s reduction of hepatic glucose production, thereby lowering HbA1c levels. 27 From a clinical perspective, this reinforces the role of pioglitazone as an insulin-sensitizing agent, particularly suited for patients in whom insulin resistance is the chief driver of hyperglycemia, rather than insulin deficiency. Secondary outcomes presented with desirable effects in our analysis. Pioglitazone therapy was associated with a significant overall improvement in HOMA-IR, indicating enhanced insulin sensitivity compared with control. In subgroup analyses, the 15 mg dose demonstrated a statistically significant reduction in HOMA-IR, whereas the 30 mg subgroup did not reach statistical significance. However, these findings should be interpreted with caution, as the subgroups were not directly compared and the 30 mg estimate was limited by imprecision, partly due to one study being non-estimable and a smaller effective sample size, resulting in wider CIs. Overall, the pooled results support the insulin-sensitizing effects of pioglitazone. 28 However, HOMA-Beta did not produce any significant change in the studies, as both doses were ineffective for this parameter, suggesting that pioglitazone’s mechanism of action does not depend on beta-cell maintenance. 29 The FPG effect of pioglitazone shows a consistent reduction in this parameter; 15 and 30 mg both showed desirable effects; no superiority was found between the two doses, consistent with the previous meta-analysis.
The significant increase in body weight is a common effect of thiazolidinediones, which act by promoting adipocyte differentiation and fluid retention through the PPAR-γ- mediated pathway. 30 The lipid profile showed an increase in cholesterol levels that was not statistically significant, with no discernible differences between the 15 and 30 mg doses. However, compared with the previous study, the level of TGL did not change. The beneficial effect of pioglitazone on the lipid profile was evidenced by a significant increase in HDL-C levels; our analysis showed a greater change with the 30 mg dose, indicating that 15 mg was superior. 31 LDL-C, total cholesterol, and SBP showed no significant changes with pioglitazone across doses. DBP was modestly reduced, with a more consistent effect at 30 mg, though no clear dose difference was observed. Overall, pioglitazone has a limited impact on BP and is not a primary antihypertensive agent, as small BP reductions occur via improved insulin sensitivity and endothelial function. 32 Clinically, these findings suggest that while pioglitazone offers modest cardiometabolic benefits beyond glycemic control, these should be weighed against predictable adverse effects such as weight gain when individualizing therapy.
In terms of safety, no significant difference is observed for TEAEs, but pioglitazone is associated with a statistically significant increase in ADRs due to its distinct mechanism of action. Pioglitazone can cause heart failure due to fluid retention, so it is to be used carefully in patients with preexisting heart failure. The mechanism of pioglitazone PPAR-γ activation in the collecting ducts of the kidney upregulates epithelial sodium channels, which increases sodium and water reabsorption, leading to expanded plasma volume. 33 This highlights the importance of careful patient selection, with avoidance or cautious use in individuals at high risk of heart failure, while potentially favoring its use in metabolically appropriate patients without significant volume-related comorbidities.
Pioglitazone remains an effective yet often underutilized therapy in the management of T2DM, largely due to concerns regarding adverse effects such as weight gain and fluid retention. However, the findings of this meta-analysis reinforce its clinical value, demonstrating consistent improvements in glycemic control and insulin sensitivity when used as add-on therapy to metformin and SGLT2 inhibitors. These results help contextualize its risk-benefit profile and may support greater clinician confidence in appropriately selected patients, particularly those with prominent insulin resistance and without significant risk of heart failure.
Our analysis has strengths worth noting. First, our findings further elaborate on differences among pioglitazone dose levels and reinforce the previous meta-analysis. By performing prespecified subgroup analyses by pioglitazone dose (15 vs 30 mg), we explored clinically relevant heterogeneity and better characterized potential dose-response relationships, thereby enhancing the clinical applicability of our findings and allowing for clearer interpretation of efficacy and safety signals across dosing strategies. To facilitate clinical interpretation of these findings, a structured comparison of efficacy and safety outcomes between the 15 and 30 mg doses is presented in Table 2. In addition, our study incorporates a larger pooled population than prior syntheses, increasing statistical power, improving precision of effect estimates, and enhancing generalizability across patients with T2DM receiving combination therapy. Importantly, we conducted a formal GRADE assessment, which demonstrated moderate to high certainty of evidence across most outcomes. High-certainty evidence supported improvements in insulin resistance (HOMA-IR), TGL, HDL-C, DBP, and achievement of glycemic targets (<7% and <6.5%). These findings reinforce the consistent metabolic benefits observed with pioglitazone add-on therapy, including clinically meaningful glycemic reductions and favorable effects on insulin sensitivity and lipid profile. In contrast, total cholesterol, LDL-C, and SBP showed no significant changes despite high-certainty evidence, indicating a more selective cardiometabolic effect. Notably, safety outcomes were also supported by high-certainty evidence, confirming increased risks of weight gain and ADRs, highlighting an important trade-off between efficacy and tolerability. This structured evaluation strengthens the credibility of our findings by contextualizing effect estimates within the certainty of evidence rather than statistical significance alone. Collectively, the consistency of benefits across multiple metabolic domains, coupled with well-defined safety considerations, enhances the robustness and clinical applicability of this meta-analysis, supporting the role of pioglitazone as an effective third-line option in appropriately selected patients inadequately controlled on metformin and SGLT2 inhibitors.
Dose-Response Comparison of Pioglitazone 15 Versus 30 mg as Add-On Therapy to Metformin and SGLT2 Inhibitors in Type 2 Diabetes Mellitus.
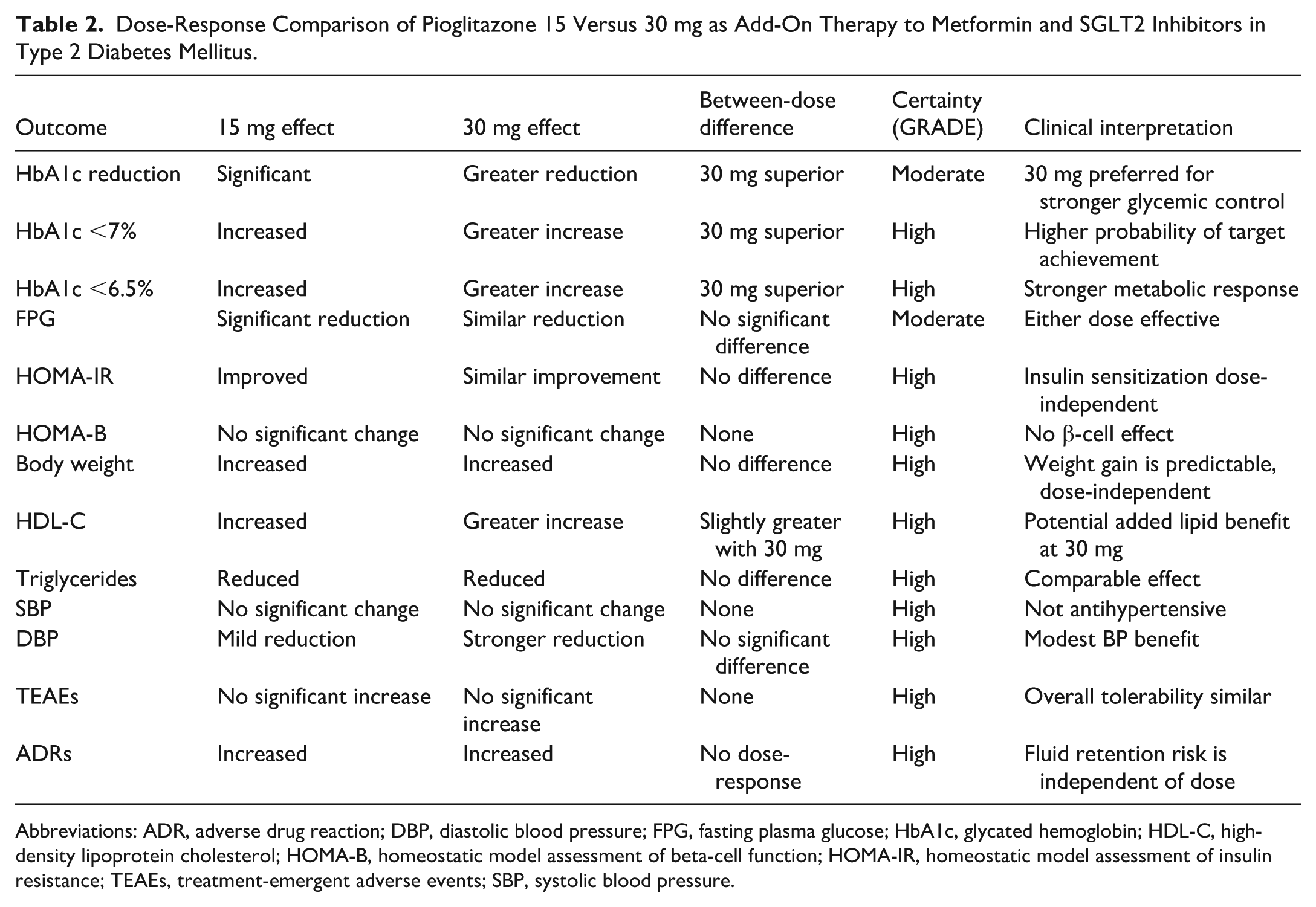
Abbreviations: ADR, adverse drug reaction; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HOMA-B, homeostatic model assessment of beta-cell function; HOMA-IR, homeostatic model assessment of insulin resistance; TEAEs, treatment-emergent adverse events; SBP, systolic blood pressure.
Certain limitations should be considered when interpreting these findings. First, although recent RCTs provide promising evidence, the number of high-quality double-blind phase 3 studies remains limited, which can affect statistical power and contribute to heterogeneity. Disparities in study duration, baseline glycemic control, and pioglitazone dosage regimens likely contributed to variability. In addition, although pioglitazone demonstrated efficacy, its effects on long-term outcomes, such as cardiovascular events or fracture risk, were not assessed in the included RCTs. Finally, most data on metabolic outcomes derive from broader pioglitazone research rather than from studies that combine metformin and SGLT2 inhibitors, indicating areas for future investigation.
Relevance to Patient Care and Clinical Practice
The findings of this meta-analysis have direct implications for the management of patients with T2DM who remain inadequately controlled on metformin and SGLT2 inhibitors. In such patients, particularly those with marked insulin resistance, pioglitazone is a rational third-line option due to its complementary insulin-sensitizing mechanism, which leads to meaningful improvements in HbA1c, fasting glucose, and other metabolic parameters. The observed dose-dependent efficacy suggests that escalation to 30 mg may be considered when greater glycemic reduction is required; however, this must be balanced against the predictable risks of weight gain and fluid retention. Clinically, these results support a more individualized treatment approach, in which pioglitazone may be preferentially used in patients without contraindications, such as heart failure, and in whom avoidance of hypoglycemia is a priority. Importantly, the lack of significant effects on beta-cell function and modest impact on BP indicate that pioglitazone should be viewed as a targeted metabolic adjunct rather than a comprehensive cardiometabolic solution. Overall, this analysis helps refine therapeutic decision-making by identifying a specific patient subgroup for whom adding pioglitazone to metformin and SGLT2 inhibitors may offer the greatest net clinical benefit, while emphasizing the need for careful monitoring and risk-benefit assessment in routine practice.
Conclusion
Overall, this updated meta-analysis demonstrates that adding pioglitazone to metformin and SGLT2 inhibitor therapy improves glycemic control and selected metabolic outcomes in patients with T2DM inadequately controlled on dual therapy. Benefits were observed in both HbA1c reduction and achievement of glycemic targets, with a dose-dependent advantage for the 30 mg regimen, whereas minimal weight gain and predictable physiological effects were the main tolerability considerations. Despite limitations in the number of trials, follow-up duration, and generalizability, the consistent efficacy across studies supports pioglitazone as a viable third-line option.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261452484 – Supplemental material for Efficacy and Safety of Pioglitazone Added to Metformin and SGLT2 Inhibitors in Type 2 Diabetes: An Updated Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-aop-10.1177_10600280261452484 for Efficacy and Safety of Pioglitazone Added to Metformin and SGLT2 Inhibitors in Type 2 Diabetes: An Updated Systematic Review and Meta-analysis by Syed Ibad Hussain, Amna Amir Jalal, Zahabia Adnan, Shanza Shakir, Devya Khaim Chandani and Muhammad Ali Makhdoom in Annals of Pharmacotherapy
Footnotes
Ethical Considerations
The study used publicly available data. Therefore, ethical approval was not required for this study.
Consent for Publication
Patient consent is not required for the publication of this study.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.