
Abstract
Background:
Status epilepticus (SE) often requires escalating antiseizure medication (ASM) therapy, increasing risks of hypotension, prolonged ventilation, and metabolic complications. The renin-angiotensin-aldosterone system (RAAS) has been implicated in neuronal excitability and neuroinflammation, yet its role in acute seizure management remains unclear.
Objective:
To evaluate the association between RAAS inhibitor exposure and ASM burden among critically ill adults with SE, and to assess treatment intensity based on total ASM administrations.
Methods:
We conducted a retrospective cohort study of adults with non-structural SE admitted to a tertiary neurocritical care unit between 2019 and 2024. Exposure was defined as administration of a RAAS inhibitor, angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB), during the intensive care unit (ICU) stay. The primary outcome was ASM burden, defined as the number of distinct ASMs administered during the ICU course. Continuous electroencephalogram reports were reviewed for electrographic seizure activity during the first 48 hours of monitoring. Negative binomial regression with log-transformed length of stay as an offset estimated incidence rate ratios (IRRs). Models were adjusted for age, hypertension, diabetes, and SE type, and validated using inverse probability of treatment weighting (IPTW).
Results:
Among 77 patients (17 RAAS inhibitor exposed, 60 non-RAAS inhibitor), RAAS inhibitor exposure was associated with a lower ASM burden (unadjusted IRR = 0.45; 95% confidence interval 0.24-0.83, P = 0.01). The association remained directionally consistent after covariate adjustment (IRR = 0.71 [0.38-1.34], P = 0.31) and after IPTW weighting (IRR = 0.63 [0.35-1.16], P = 0.14). Electrographic seizures were absent in the RAAS inhibitor group during the first 48 hours of EEG monitoring.
Conclusions and Relevance:
RAAS inhibitor exposure was associated with lower ASM utilization in critically ill patients with SE, with consistent direction across adjusted models. These findings support further investigation into RAAS modulation as a potential neuroprotective mechanism in acute epileptic states.
Keywords
Introduction
Seizures and epilepsy are complex processes influenced by multiple neurochemical pathways, among which the renin-angiotensin-aldosterone system (RAAS) has gained increasing attention. Experimental data indicate that RAAS activity contributes to neuronal excitability, neuroinflammation, and blood-brain barrier (BBB) disruption. Inhibition of RAAS through angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II type1 receptor blockers (ARBs) reduces seizure frequency and neuronal injury in animal models of temporal lobe and chemically induced epilepsy.1,2 These effects appear to extend beyond hemodynamic regulation, suggesting direct neuroprotective and anti-excitatory properties.
Pharmacologic modulation of the RAAS has also demonstrated synergistic interactions with antiseizure medications in preclinical models, where ACEIs such as captopril enhanced the anticonvulsant activity of carbamazepine and lamotrigine. These interactions appear to be pharmacodynamic in nature, potentially reflecting modulation of central RAAS pathways involved in seizure susceptibility. 3 Additional work supports a role for RAAS inhibition in reducing oxidative stress and excitotoxicity. 4 Together, these findings position the RAAS as a potential therapeutic target in seizure management.
Complementing these findings, population-based studies in hypertensive adults have reported a lower incidence of new-onset epilepsy among users of ARBs compared with other antihypertensive agents. In large multicenter retrospective analyses, ARB therapy was associated with a 23% to 30% relative reduction in epilepsy risk compared with ACE inhibitors, β-blockers, or calcium channel blockers, with the strongest effect observed for losartan and in patients without prior cerebrovascular disease. 5 These differences may be related to the more direct blockade of angiotensin II type 1 (AT1) receptors by ARBs, which are implicated in neuroinflammatory signaling, BBB dysfunction, and neuronal excitability, whereas ACE inhibitors act upstream and may have less specific central effects. These shared pharmacologic effects, including modulation of neuroinflammation, oxidative stress, and BBB integrity, may contribute to a clinically meaningful reduction in seizure propagation and treatment escalation.
Despite growing interest in the neuroprotective role of RAAS modulation, its relevance to acute seizure management in critically ill patients remains uncertain and poorly characterized. In the intensive care unit (ICU), status epilepticus (SE) often requires escalating antiseizure medication (ASM) therapy, increasing the risks of hypotension, prolonged ventilation, and metabolic complications.6-12 Whether RAAS inhibition during acute hospitalization modulates seizure activity or reduces ASM burden has not been previously characterized.
Increasing evidence indicates that neuroinflammation plays a central role in the initiation and perpetuation of SE. Proinflammatory cytokines such as interleukin (IL)-1β, interleukin-6, tumor necrosis factor-α (TNF-α), and the high mobility group 1 activate the signaling pathways of NFκB (nuclear factor kappa-light-chain-enhancer of activated B cells) and toll receptors, disrupt the integrity of the BBB, and enhance neuronal excitability. 13 Experimental blockade of these mediators and their downstream cascades has reduced seizure recurrence and improved outcomes in both animal and clinical studies, underscoring inflammation as a modifiable component of the pathophysiology of SE. 14 Because activation of the RAAS similarly promotes cytokine release and oxidative stress, pharmacologic inhibition of RAAS may attenuate these inflammatory processes, providing a mechanistic rationale for exploring its role in acute seizure management.
Consequently, this study aimed to evaluate the association between RAAS inhibitor exposure and ASM utilization among critically ill adults with SE. The primary objective was to evaluate the association between RAAS inhibitor exposure and ASM burden, and the secondary objective was to assess treatment intensity based on total ASM administrations.
Methods
This retrospective cohort study was conducted in a tertiary, high-volume neurocritical care unit at Memorial Hermann – Texas Medical Center, affiliated with the McGovern School of Medicine at UTHealth Houston. The unit is a 32-bed neurocritical care ICU staffed by board-certified neurointensivists with multidisciplinary involvement from neurology, neurosurgery, and critical care teams, including fellows, residents, and advanced practice providers, and manages a broad spectrum of neurologic emergencies such as SE, acute stroke, intracranial hemorrhage, and traumatic brain injury. The patient population included adult individuals diagnosed with SE who were admitted between January 2019 and December 2024. Patient data were extracted using the institutional electronic health record (EHR) system. This study, titled “Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients with Status Epilepticus: A Retrospective Cohort Study” received approval from the UT Health Science Center at Houston Institutional Review Board (IRB) on November 1, 2024; IRB #HSCMH241092. All procedures were conducted in strict accordance with the ethical standards established by the IRB and adhered to the principles outlined in the Helsinki Declaration of 1975.
Eligible patients were those aged 18 years or older who met the diagnostic criteria for SE. The SE was defined as continuous or recurrent clinical or electrographic seizures that lasted for at least 5 minutes without a return to baseline consciousness.6,9,15 To ensure a clinically comparable cohort, patients with acute structural brain injuries (including ischemic stroke, intracerebral hemorrhage, traumatic brain injury, hypoxic-ischemic injury, central nervous system infections, and intracranial mass lesions) were excluded, as these conditions are managed with disease-specific protocols, including guideline-directed blood pressure targets, which directly influence antihypertensive selection independent of seizure-related considerations.
All included patients were required to have received at least one antihypertensive agent during their stay in the ICU to ensure a comparable exposure to blood pressure-modifying therapy. Exposure was defined as the administration of any RAAS inhibitor, either an ACEI or an ARB, during the stay in the ICU. Outpatient medication reconciliation was incomplete; therefore, the analysis reflects acute administration during the ICU stay rather than chronic use. Continuation versus initiation of therapy could not be distinguished. The ACEIs and ARBs were pooled in a single “RAAS inhibitor” category for the primary analysis (Supplemental Table S1).
The specific oral antihypertensive medications administered, and their respective frequencies in each group, are provided in Supplemental Table S8. Detailed dose and strength data for RAAS inhibitors were not systematically abstracted due to the substantial manual effort required to complete capture at all charts and time points. Covariates included age, hypertension, diabetes, and type of SE (generalized, focal, or non-convulsive). Clinical surrogates (comorbidities, admission blood pressure, renal function, and use of vasopressors) were used as proxies for baseline illness severity. The primary outcome was ASM burden, defined as the number of distinct antiseizure medications administered during the ICU stay. The secondary outcome was treatment intensity, defined as the total number of ASM administrations during hospitalization. At our institution, ASM management for SE generally follows guideline-based practice, with initial benzodiazepine administration followed by sequential or combination use of second-line agents. In clinical practice, escalation may involve addition of multiple agents rather than strict maximization of a single medication prior to transition. Detailed data on ASM dose, titration, and daily strength were not systematically abstracted, as these data are not consistently available in a structured format and would require granular chart-level reconstruction across time points. This approach is consistent with prior treatment burden studies that prioritize feasible and reproducible measures of exposure. The specific antiseizure medications administered during the ICU stay, including oral agents, and their respective frequencies in each group are provided in Supplemental Table S7. The most commonly administered antiseizure medications included levetiracetam, lacosamide, and valproate, with less frequent use of other agents as detailed in the table.
A negative binomial regression model was fitted with the logarithmic transform in length of stay (LOS) entered as an offset to account for exposure time. A sensitivity analysis was performed excluding patients older than 75 years and those with chronic hypertension. This analysis was performed because including patients >75 years in the regression model substantially attenuated the observed association between the use of RAAS inhibitors and the burden of ASMs, likely reflecting that older patients in this cohort tended to receive fewer ASMs, thus acting as confounders. Similarly, chronic hypertension was a marker for long-term antihypertensive exposure, and its exclusion helped to focus the analysis on the acute effects of RAAS inhibitors in the ICU. Confounding by indication was addressed using stabilized inverse probability of treatment weighting (IPTW). The propensity model included age, hypertension, diabetes, and SE type. Weights were truncated at the 1st and 99th percentiles, and balance was assessed using standardized mean differences. Weighted negative binomial regression with LOS offset produced the IPTW-adjusted incidence rate ratio (IRR) (Supplemental Tables S2a, S2b, S6).
The diagnosis of SE was established by the treating neurology team based on clinical and/or electrographic criteria consistent with established definitions and was not independently adjudicated for the purposes of this study. Data collection and monitoring was conducted by the Epitome Research Team, a specialized group within the Epilepsy Division at McGovern Medical School, The University of Texas Health Science Center at Houston. The team is trained in systematic clinical data abstraction and verification, following standardized extraction workflows with independent cross-checking and quality assurance procedures to ensure precision, completeness, and consistency across all study variables. Continuous electroencephalogram (cEEG) monitoring data were reviewed for all patients who underwent recording, based on formal clinical interpretations documented in the medical record by the treating epileptology team. No independent EEG interpretation or diagnostic adjudication was performed by the study investigators.
Each 24-hour period was assigned an ordinal EEG score (0 = normal, 1 = encephalopathy, 2 = epileptiform discharges, 3 = electrographic seizure). The proportion of monitored patients exhibiting seizures or discharges was calculated daily for EEG days 1-2 (primary window) and EEG days 3-5 (exploratory). Because EEG duration varied between groups, total monitoring days were compared, and analyses focused on the first 48 hours, where overlap was greatest (Supplemental Table S6).
Mean arterial pressure (MAP), creatinine, and blood urea nitrogen (BUN) from the first 24 hours of ICU admission were extracted to assess hemodynamic and renal comparability. Seven-day medians were summarized in Supplemental Table S3. Exposure to continuous sedative infusions (midazolam, propofol, ketamine, and pentobarbital) was tabulated as any use during the ICU stay (Supplemental Table S4). Analyses were performed in R 4.3 and Python 3.11 using statsmodels. Post hoc calculations indicated 80% power (α = 0.05, two-sided) to detect an IRR ≤ 0.36 or ≥ 2.8 for RAAS exposure effects on ASM burden (Supplementary Statistical Methods and Supplemental Table S10).
Results
In total, 77 patients were identified as meeting the inclusion criteria, consisting of 17 patients (22%) who received a RAAS inhibitor and 60 patients (78%) who were treated with other antihypertensive agents without RAAS blockade. The baseline demographic and clinical characteristics of the study population are summarized in Table 1. Patients in the RAAS group were significantly older, with a median age of 66 years (IQR 62-76) compared to 57 years (IQR 39-66) in the non-RAAS group (P = 0.006). In addition, the prevalence of hypertension was higher in the RAAS group (82% vs 52%, P = 0.028), as was diabetes mellitus (35% vs 12%, P = 0.032). Other comorbidities, SE type, and etiologic categories exhibited no significant differences between the 2 groups. The EEG monitoring was implemented in nearly all patients and demonstrated comparable background and epileptiform activity. However, burst suppression was numerically more frequent in the RAAS group (18% vs 3%, P = 0.07).
Baseline Characteristics by RAAS Inhibitor Use.
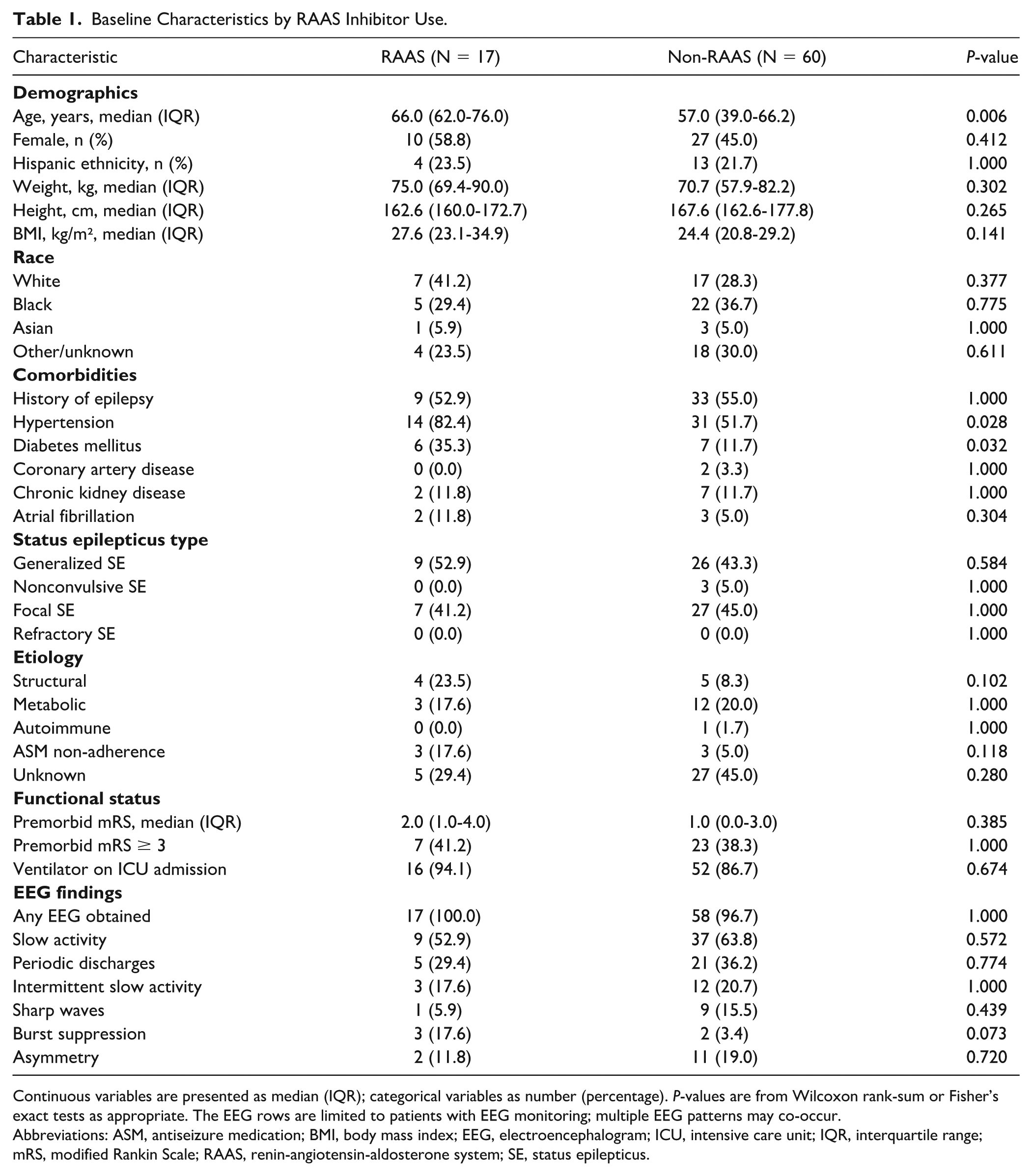
Continuous variables are presented as median (IQR); categorical variables as number (percentage). P-values are from Wilcoxon rank-sum or Fisher’s exact tests as appropriate. The EEG rows are limited to patients with EEG monitoring; multiple EEG patterns may co-occur.
Abbreviations: ASM, antiseizure medication; BMI, body mass index; EEG, electroencephalogram; ICU, intensive care unit; IQR, interquartile range; mRS, modified Rankin Scale; RAAS, renin-angiotensin-aldosterone system; SE, status epilepticus.
The primary endpoint, ASM burden, was measured as the number of distinct antiseizure medications administered during ICU stay. The unadjusted negative binomial model, accounting for LOS, demonstrated that RAAS exposure was associated with a lower ASM burden (IRR = 0.45, 95% confidence interval [CI] 0.24-0.83; P = 0.01). After multivariable adjustment for age, hypertension, diabetes, and SE type, the association was attenuated (IRR = 0.71, 95% CI 0.38-1.34; P = 0.31). Propensity weighting achieved excellent covariate balance (Supplemental Table S2a), with an IPTW-adjusted IRR 0.63 (95% CI 0.35-1.16; P = 0.14) (Table 2 and Supplemental Table S2b). As a secondary analysis, dosing intensity was assessed by the total number of ASM administrations (the sum of all individual doses per patient throughout hospitalization). The ASM count correlated moderately with total administrations (Spearman ρ = 0.49, P < 0.001). The RAAS exposure was associated with a lower total administration rate per LOS day (IRR = 0.55; 95% CI 0.32-0.97; P = 0.04), mirroring the direction of the primary analysis (Table 3).
Negative Binomial Regression for Antiseizure Medication Burden.
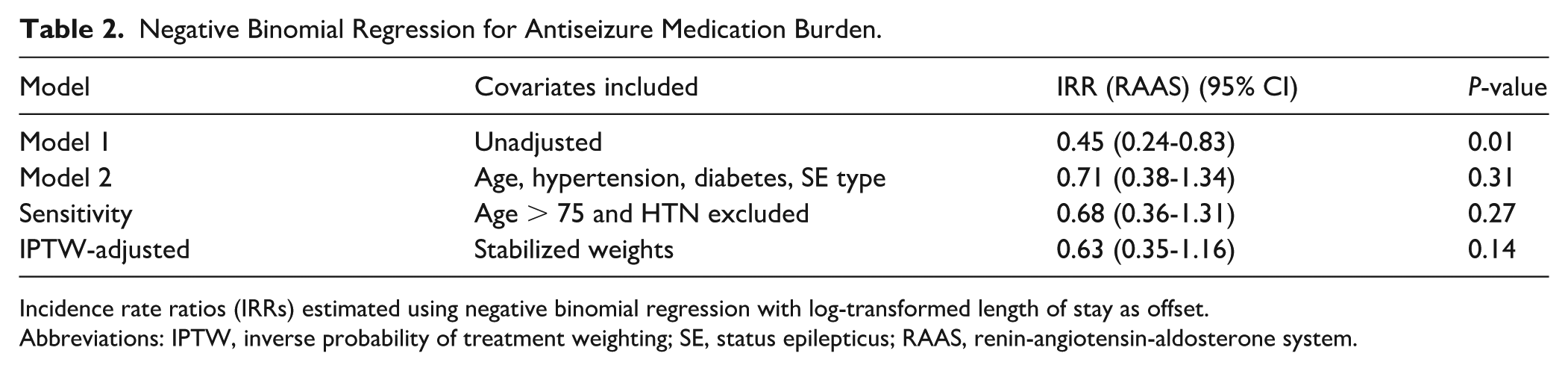
Incidence rate ratios (IRRs) estimated using negative binomial regression with log-transformed length of stay as offset.
Abbreviations: IPTW, inverse probability of treatment weighting; SE, status epilepticus; RAAS, renin-angiotensin-aldosterone system.
Antiseizure Medication Intensity by RAAS Exposure.
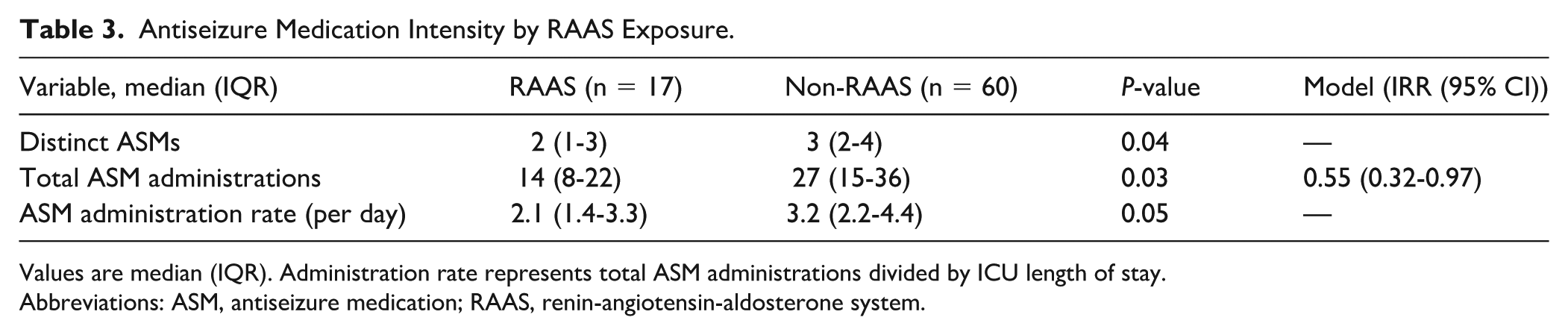
Values are median (IQR). Administration rate represents total ASM administrations divided by ICU length of stay.
Abbreviations: ASM, antiseizure medication; RAAS, renin-angiotensin-aldosterone system.
Additional analyses were conducted to evaluate whether differences in benzodiazepine or sedative exposure influenced the observed association between RAAS inhibitor use and ASM burden. Benzodiazepine exposure, defined as any administration of lorazepam, diazepam, or midazolam during the ICU stay, was not lower in the RAAS group (70.6% vs 52.5%, P = 0.27), and median total benzodiazepine administrations were similar between groups (2 [0-2] vs 1 [0-2], P = 0.15). Sensitivity analyses incorporating benzodiazepine and sedative exposure as covariates demonstrated consistent directionality of the association between RAAS inhibitor use and lower ASM burden. In negative binomial models adjusting for total benzodiazepine administrations, RAAS exposure remained associated with a lower number of distinct ASMs (IRR = 0.49 [0.29-0.83], P = 0.008). Similar results were observed when adjusting for any benzodiazepine exposure (IRR = 0.54 [0.32-0.90], P = 0.019) and for continuous sedative infusion (IRR = 0.47 [0.27-0.80], P = 0.005). These findings are summarized in Supplemental Table S9.
The EEG monitoring duration was shorter among RAAS patients (median 2 [1-4] days) than non-RAAS patients (4 [2-7] days; P = 0.04) (Table 4). During the first 48 hours, electrographic seizures were absent in the RAAS group compared with 5% to 17% in the non-RAAS group, and epileptiform discharges occurred in 18% versus 32% to 42%, respectively (Supplemental Tables S5 and S6). Importantly, all RAAS group patients met established clinical criteria for SE at presentation, as defined by continuous or recurrent clinical seizures lasting at least 5 minutes without return to baseline consciousness, regardless of subsequent EEG findings during hospitalization.
EEG Findings During the First 48 Hours of Monitoring.
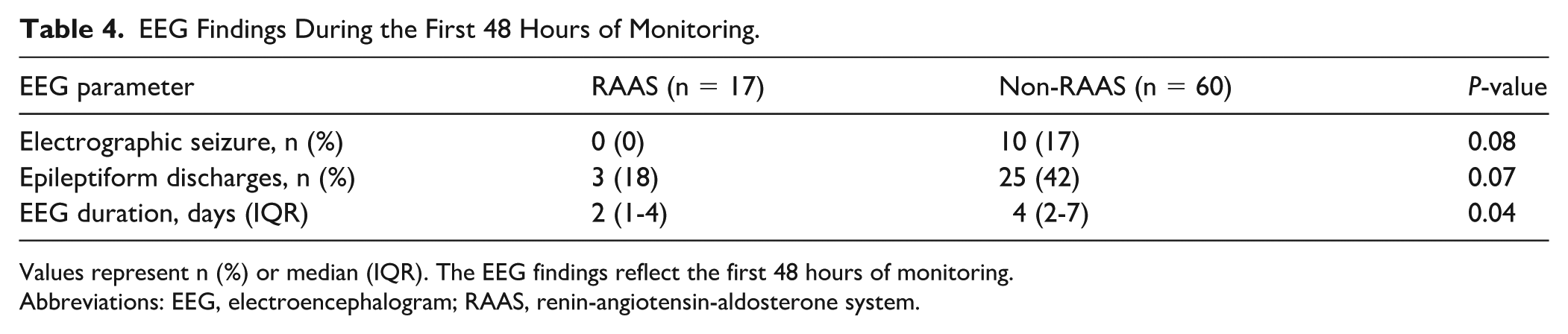
Values represent n (%) or median (IQR). The EEG findings reflect the first 48 hours of monitoring.
Abbreviations: EEG, electroencephalogram; RAAS, renin-angiotensin-aldosterone system.
Admission MAP, creatinine, and BUN were comparable between RAAS and non-RAAS patients. No significant differences were observed in median 7-day MAP or changes in creatinine, suggesting similar hemodynamic stability and renal tolerance. Continuous sedative exposure was infrequent and comparable between groups. Surrogate variables, including comorbidities, vital signs, and vasopressor use, did not differ substantially, indicating similar baseline acuity (Supplemental Tables S3 and S4). Clinical results and medication use are summarized in Table 5. The overall mortality was 5.9% in the RAAS group and 5.0% in the non-RAAS group, with no significant difference (P = 1.00). The median hospital LOS was longer in the RAAS cohort (7.4 days [IQR = 3.9-14.8]) compared with the non-RAAS group (5.0 days [IQR = 2.9-11.2]; P = 0.11). The ICU LOS was shorter in the RAAS group (6 [4-9] days) than in the non-RAAS group (8 [5-12] days; P = 0.09). The median duration of mechanical ventilation was significantly longer for patients receiving RAAS inhibitors (1.5 days [IQR = 0.7-3.7]) compared with non-RAAS patients (0.9 days [IQR = 0.2-1.7], P = 0.046). Utilization of continuous sedative infusions and vasopressor therapy was very low in both groups. There were no meaningful differences observed between groups in these measures. The functional results also did not show significant differences. A modified Rankin Scale (mRS) score at discharge of 3 to 6 was observed in 70.6% of patients in the RAAS group compared with 58.3% of those in the non-RAAS group (P = 0.41). Discharge to inpatient rehabilitation was more prevalent among RAAS patients (41% vs 12%, P = 0.011), while discharge to home was noted in 47% of RAAS patients compared with 67% in the non-RAAS cohort (P = 0.16).
Clinical Outcomes and Medication Utilization (RAAS vs Non-RAAS).
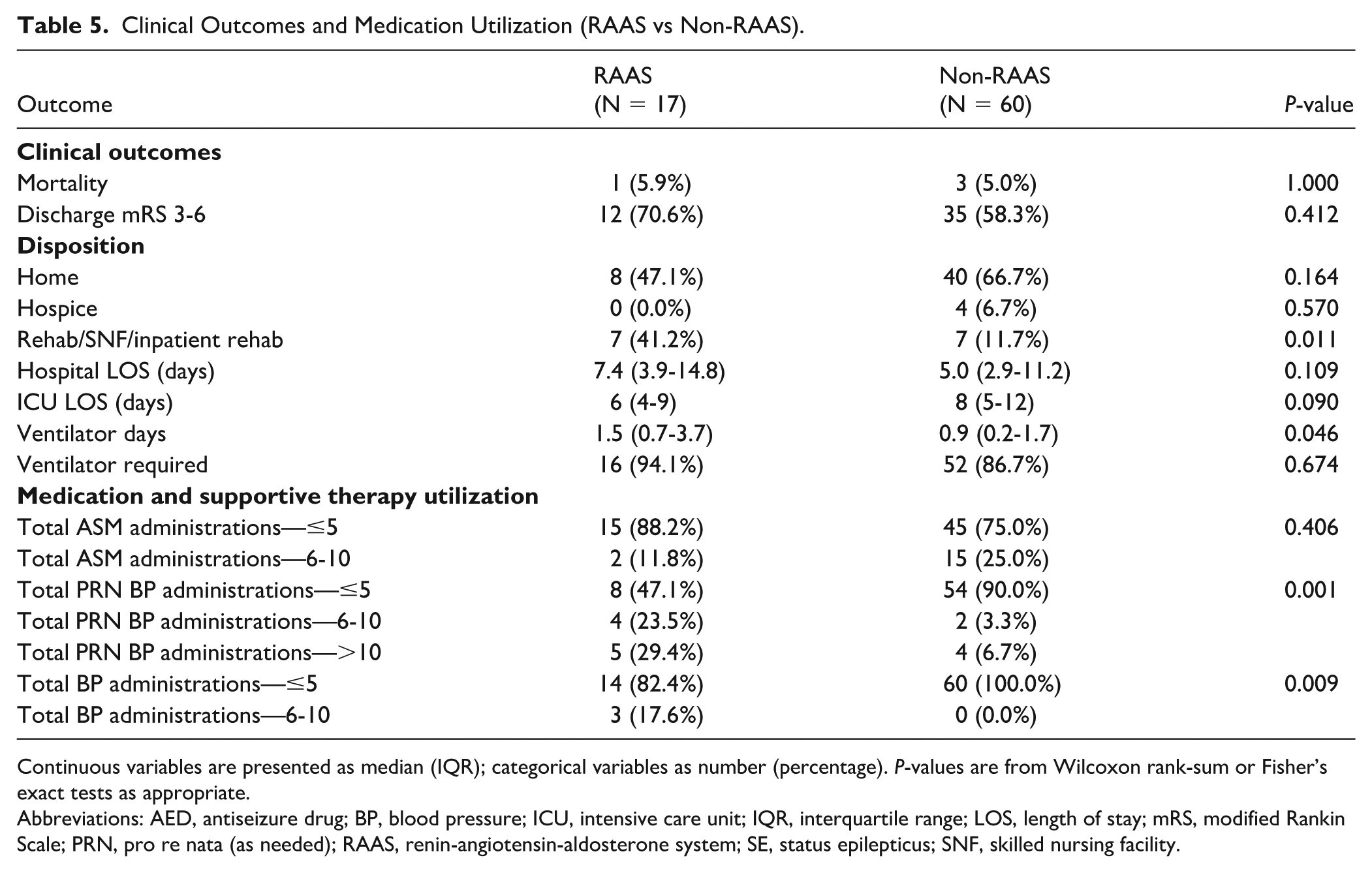
Continuous variables are presented as median (IQR); categorical variables as number (percentage). P-values are from Wilcoxon rank-sum or Fisher’s exact tests as appropriate.
Abbreviations: AED, antiseizure drug; BP, blood pressure; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; mRS, modified Rankin Scale; PRN, pro re nata (as needed); RAAS, renin-angiotensin-aldosterone system; SE, status epilepticus; SNF, skilled nursing facility.
Discussion
This retrospective cohort examined the association between RAAS inhibitor exposure and ASM burden among critically ill adults with SE without structural brain injury. The RAAS inhibitor use during the ICU stay was associated with a lower number of distinct ASMs and a reduced rate of total ASM administrations. These exploratory findings were directionally consistent across unadjusted, covariate-adjusted, and propensity-weighted analyses, although CIs were wide because of the modest sample size. The study was powered to detect larger effect sizes than those observed, which may explain the lack of statistical significance despite consistent directionality across models. The direction and internal consistency of these associations may indicate a potential neuroprotective or anti-excitatory role of RAAS modulation in acute epileptic states.
The observed decrease in ASM utilization in patients treated with RAAS inhibitors aligns with a growing body of experimental evidence that underscores the role of RAAS in modulating neuronal excitability and seizure dynamics. Central angiotensin II signaling through type 1 receptors has been established to lead to microglial activation, oxidative stress, and disruption of the BBB, all contributing factors to lowered seizure thresholds.16-19 Furthermore, specifically, blocking angiotensin receptors with agents such as losartan has demonstrated the ability to mitigate astrocytic activation, preserve BBB integrity, and reduce recurrent seizures in rodent models subjected to chemically induced SE. Beyond these neurocentric mechanisms, systemic RAAS activation is also known to drive inflammation via TNF-α, IL-6, intercellular adhesion molecule-1, and NFκB signaling, whereas pharmacologic blockade decreases these inflammatory mediators and oxidative stress, improving endothelial function and vascular homeostasis RAAS and inflammation. 20 Together, these experimental observations provide a substantiated biological basis for the potential of inhibition of RAAS to limit the need for aggressive seizure management in clinical practice.21-25 Population-based studies support the concept of a neuroprotective role for RAAS inhibitors in susceptibility to seizures. Prior research in hypertensive adults has reported a reduced risk of new-onset epilepsy among those treated with ARBs compared with other antihypertensive agents.5,23,26 The observed decrease in the incidence of epilepsy, particularly with the use of losartan, appeared to be independent of the underlying vascular comorbidities, indicating a potential mechanism that transcends the control of blood pressure alone.
This study evaluated pharmacologic exposure during the ICU stay rather than chronic outpatient therapy, providing a more immediate perspective on the treatment of acute seizures. Because milligram-level dosing data were unavailable, total ASM administrations, normalized to LOS, were used as a pragmatic measure of cumulative treatment intensity and showed moderate correlation with the number of distinct antiseizure medications. Sensitivity analyses incorporating benzodiazepine and sedative exposure as proxies for early treatment intensity yielded consistent findings, suggesting that differences in measured treatment intensity did not account for the observed association between RAAS inhibitor exposure and lower ASM burden.
Admission MAP and renal indices were comparable between groups, and no differences were observed in creatinine trends or vasopressor requirements, indicating similar tolerability of RAAS therapy. Collectively, these findings suggest that RAAS inhibition may reduce pharmacologic escalation in SE, possibly through modulation of neuroinflammatory or neurovascular mechanisms.
This study has several notable strengths. It focuses on a clearly defined population of adults with non-structural SE, without observed refractory cases in this cohort, reducing heterogeneity and isolating systemic pharmacologic effects. Data abstraction and EEG interpretation followed standardized, independently verified workflows, enhancing accuracy and reproducibility. The analysis incorporated both covariate-adjusted and propensity-weighted models to address confounding, and the consistency of results across these approaches supports internal validity. Importantly, this investigation extends previous observations of RAAS modulation from experimental and outpatient settings into a neurocritical care context, providing preliminary clinical evidence that acute inhibitor exposure may influence ASM requirements and support the need for prospective validation.
This analysis was limited by its single-center, retrospective design and modest sample size, which constrain statistical power and generalizability. Detailed medication administration timestamps were unavailable, preventing confirmation of whether RAAS therapy preceded, coincided with, or followed seizure onset. Consequently, causal inference regarding the temporal relationship between RAAS exposure and seizure suppression cannot be established. Outpatient medication reconciliation was incomplete, limiting the ability to distinguish chronic RAAS users from new initiations. To approximate the latter group, we conducted a sensitivity analysis excluding patients with chronic hypertension and those aged >75 years, who were more likely to be on long-term RAAS therapy. Age was significantly different between groups at baseline. However, all primary and secondary analyses were adjusted for age, and a sensitivity analysis confirmed that the observed associations persisted when controlling for this and other key confounders. The findings remained directionally consistent, suggesting that the observed association remained directionally consistent after sensitivity analysis, although the relative contributions of acute versus chronic RAAS exposure could not be determined.
The EEG monitoring duration varied between groups, which may have influenced seizure detection. Formal systemic severity indices (eg, APACHE II, SOFA) were unavailable. In addition, key clinical variables such as electrolyte abnormalities and history of alcohol use disorder were not systematically captured, which may influence seizure risk and treatment requirements. However, clinical and EEG characteristics in Table 1 provided context on acute illness and neurologic severity. Approximately 40% of patients in each group had a premorbid mRS > 3, indicating that many were functionally limited before admission. This baseline dependency could have contributed to the appearance of greater overall illness severity but is unlikely to explain the observed differences in ASM burden between groups. The absence of refractory SE cases may limit applicability to more severe or treatment-resistant forms. Detailed RAAS dosing data and ASM serum concentrations were unavailable; therefore, our analysis reflects exposure status rather than pharmacologic intensity. In addition, milligram-level dosing was not consistently available in a standardized format across medications, and treatment burden was assessed using medication counts and administration frequency, an approach supported in pharmacoepidemiologic literature when dose standardization across heterogeneous agents is not feasible.27,28 Although this may introduce some variability, the use of adjusted models and IPTW helps account for measured confounding and supports the consistency of the observed associations. Finally, as a single-center study, the findings may not generalize to ICUs with different patient characteristics or treatment practices.
Conclusion and Relevance
In this exploratory ICU cohort, RAAS inhibitor exposure was associated with reduced ASM burden and lower cumulative administration intensity in patients with non-structural SE, without evidence of hemodynamic or renal compromise. These findings support further investigation of the renin-angiotensin system as a potential modifiable biological target in SE. Future multicenter studies should integrate timestamped medication data, cEEG analytics, and standardized severity indices to clarify temporal and mechanistic relationships.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-1-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Supplemental Material
sj-docx-2-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-2-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Supplemental Material
sj-docx-3-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-3-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Supplemental Material
sj-docx-4-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-4-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Supplemental Material
sj-docx-5-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-5-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Supplemental Material
sj-docx-6-aop-10.1177_10600280261452558 – Supplemental material for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus
Supplemental material, sj-docx-6-aop-10.1177_10600280261452558 for Association Between Renin-Angiotensin System Inhibitors and Antiseizure Medication Burden in Critically Ill Patients With Status Epilepticus by Sophie Samuel, A. J. Cadena-Tejada, K. Peoples, L. F. Torres and S. O. Smart in Annals of Pharmacotherapy
Footnotes
Acknowledgements
None.
Ethical Considerations
This retrospective study was approved by the UTHealth Houston Institutional Review Board (IRB reference #HSC-MH-24-1092) on November 1, 2024. The requirement for informed consent was waived due to the use of de-identified data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.