
Abstract
Background:
Only one-fifth of patients meeting the criteria for intravenous (IV) iron therapy received IV iron in the real-world practice. Pharmacists-providers collaborative iron deficiency (ID) clinic was developed to implement guideline-directed IV iron therapy.
Objective:
To evaluate the 4-year performance of the pharmacists-providers collaborative ID treatment clinic in the heart failure (HF) service.
Methods:
A single-center retrospective cohort study was conducted to evaluate the performance of the iron deficiency pharmacists-providers collaborative care clinic during the induction and maintenance phases of IV iron therapy. The study included patients who were seen by HF providers and received the IV iron consultation with HF pharmacists. The study included patients aged 18 years or older who were diagnosed with HF or pulmonary hypertension and received at least 1 dose of IV iron in outpatient settings. It was managed by the pharmacists-providers collaborative IV iron clinic. The primary outcome was adherence to all of the following criteria: the IV iron appropriate use criteria, laboratory requirements, and dosing during the induction course. The use of oral iron therapy was evaluated.
Results:
A total of 187 patients were included in the final cohort. The median follow-up period of the IV iron consulting team was 372 (176, 623) days. One hundred fifty-two patients (81.3%) were adherent to the appropriate criteria. The most common reasons for nonadherence were the absence of maintenance laboratory requirements (15.5%), failure to administer all induction doses (1.6%), inappropriate use (1.1%), and incorrect dose (0.5%). Among 15 patients on oral iron therapy, the consulting team discontinued it in 3 patients (20.0%) during follow-up.
Conclusion and Relevance:
The pharmacists-providers collaborative IV iron clinic was effective to implement IV iron therapy in heart failure care settings. These results highlight the importance of multidisciplinary care management for ID in real-world HF practice.
Introduction
Iron deficiency in heart failure (HF) occurs in more than 50% of patients with HF. 1 Iron deficiency is significantly associated with worse functionality, lower quality of life, and increased mortality. 1 Multiple clinical trials have shown that intravenous (IV) iron therapy improved functionality and quality of life and reduced hospitalizations for HF.2-5 The American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Failure Society of America (HFSA) HF guidelines recommend IV iron therapy for patients with HF with reduced ejection fraction (HFrEF). 6 However, only one-fifth of patients meeting the criteria for IV iron therapy received IV iron in the real-world practice, potentially due to a lack of implementation strategies for IV iron therapy, access to IV iron infusion centers, care coordination issues, and time constraints of HF providers.7,8 Authors previously documented the first reported pharmacists-providers collaborative iron deficiency treatment clinic to overcome these implementation barriers. 9 The initial pilot study showed significant improvements in the quality of iron deficiency care and doubled the number of patients who received IV iron therapy during the induction course. However, the initial report described only the clinic’s short-term performance during the induction course, and the number of patients was small. The clinic also offered IV iron therapy to patients with pulmonary hypertension and HF with preserved ejection fraction (HFpEF) after clinical evidence showed positive results.10-12 The primary objective of the study was to evaluate the 4-year long-term experiences of this pharmacists-providers collaborative iron deficiency clinic during both the induction and maintenance phases in a large-scale cohort.
Methods
Description of the Clinical Service
Authors previously reported details of this multidisciplinary pharmacists-providers collaborative iron deficiency service. 9 Briefly, the HF services offer a pharmacists-providers collaborative iron deficiency care service mainly for outpatients, and it recently initiated a transition-of-care service for IV iron to improve care transitions from inpatient to outpatient settings in patients with HF. Once HF providers (advanced HF cardiologists or advanced practice providers) identify candidates for IV iron therapy after screening for iron deficiency, HF pharmacists received consulting orders from HF providers and lead the entire process, including IV iron therapy eligibility, development of an IV iron therapy plan, referrals to local infusion centers based on the patient’s residential location after insurance authorization approval, and monitoring recipients of IV iron therapy. The referrals were placed both in outpatient and inpatient settings. Once patients receive an IV iron induction course, iron studies and complete blood counts (CBCs) were obtained 3 to 6 months after the induction course ends. Heart failure pharmacists assessed the need for IV iron maintenance therapy and developed it longitudinally. Ferric carboxymaltose was the preferred agent, and iron sucrose was the second-line agent in outpatient settings, depending on the insurance formularies and local infusion center availability. If ferric carboxymaltose was selected, phosphorus aimed to be measured every 6 months. Insurance specialists authorized all IV iron therapy plans through insurance, if required.
Study Design
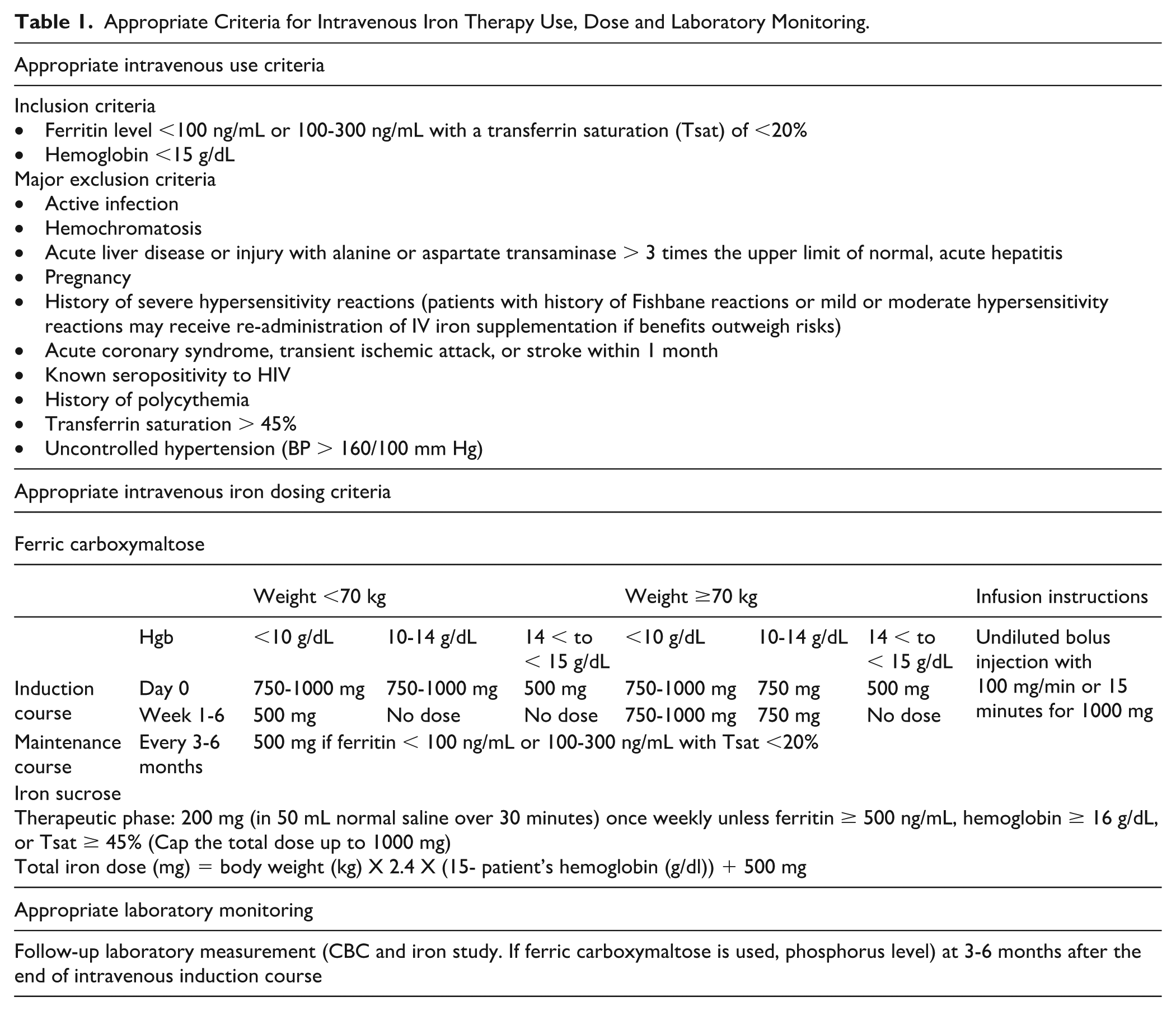
A single-center retrospective cohort study was conducted to evaluate the performance of the iron deficiency pharmacists-providers collaborative care clinic during the induction and maintenance phases. The study included patients who were seen by HF providers and received an IV iron consultation with HF pharmacists from January 1, 2021, to May 30, 2025. The study included patients aged 18 years or older who were diagnosed with HF or pulmonary hypertension, completed the induction course of either ferric carboxymaltose or iron sucrose in an outpatient setting, and were managed by the pharmacist-provider collaborative IV iron clinic. Iron deficiency was defined as either absolute iron deficiency (ferritin < 100 µg/L) or functional iron deficiency (ferritin level 100-299 µg/L and transferrin saturation < 20%). Hemoglobin levels greater than 15 mg/dL were excluded. The primary outcome was adherence to all of the following 3 criteria: IV iron appropriate use criteria, laboratory requirements, and dosing during the induction course (Table 1). The appropriate criteria were developed based on the HFSA statement, HF guidelines, and the published expert consensus.1,6,8 Reasons for nonadherence were selected from the options: no maintenance iron study or hemoglobin levels within 6 months after the induction course, incorrect dose, and inappropriate use. IV iron doses were retrospectively confirmed by calling infusion centers if given at the outside health system network. The secondary outcomes included 1-year hospitalization for HF, all-cause mortality, EF within 1 year after induction course therapy in patients with HFrEF or HF with mildly reduced EF, and discontinuation of oral iron therapy in patients with HFrEF. Longitudinal changes in iron study laboratory results were evaluated over 4 years. Adverse events were also reported.
Appropriate Criteria for Intravenous Iron Therapy Use, Dose and Laboratory Monitoring.
The distribution of IV iron therapy administered throughout the Appalachian region was visually described. The rural area was defined with the Health Resources and Services Administration Rural Health Grants Eligibility Analyzer. 13 Drive times for zip codes were determined by the location of their centroids within a drive-time band. A rural drive-time analysis was performed by creating rural drive-time bands using ESRI ArcOnline Map’s Generate Travel Areas tool in 15-minute intervals up to 75 minutes. 14 A rural drive time was also created for WVU Medicine Ruby Memorial Hospital, where the HF clinic is located, in 15-minute intervals up to 5 hours, where was the main infusion center for IV iron therapy prior to the implementation of this multidisciplinary pharmacists-providers collaborative iron deficiency service. A density heat map was created to show where the raw numbers of patients were distributed throughout the study area.
This present research was approved by the institutional review board.
Statistical Analysis
Continuous variables were displayed as either the mean and standard deviation or the median and interquartile range (IQR). Categorical variables were described as count (percent: %). A paired t test was used to compare EF readings at baseline and follow-up. The Wilcoxon signed-rank test was used to compare 2 related median values, as a normal distribution could not be assumed. The Friedman test was employed to compare means of related groups for continuous variables. Missing values were imputed using a predictive mean matching multiple imputation model. If the Friedman test was significant, a Wilcoxon signed-rank test was used as the post hoc test for all paired comparisons, with the Bonferroni correction applied. All statistical analyses were performed using SPSS Version 29.0.2. GIS analysis and maps were created using ESRI ArcGIS Pro version 3.3.2 (2025).
Results
Baseline Characteristics and Iron Deficiency Consulting Team Performance
A total of 187 patients were included in the final cohort (Table 2). The majority of IV iron doses were for patients with HFrEF (53.5%). Eighty-three percent of iron deficiency was absolute iron deficiency, and more than 90% had transferrin saturation < 20%. Approximately 79% of patients received ferric carboxymaltose, and the remainder received iron sucrose. The median follow-up period of the IV iron consulting team was 372 (176, 623) days. The total IV iron induction dose (median (IQR)) was 1250 (750, 1250) mg.
Baseline Characteristics of an Iron Deficiency Cohort.
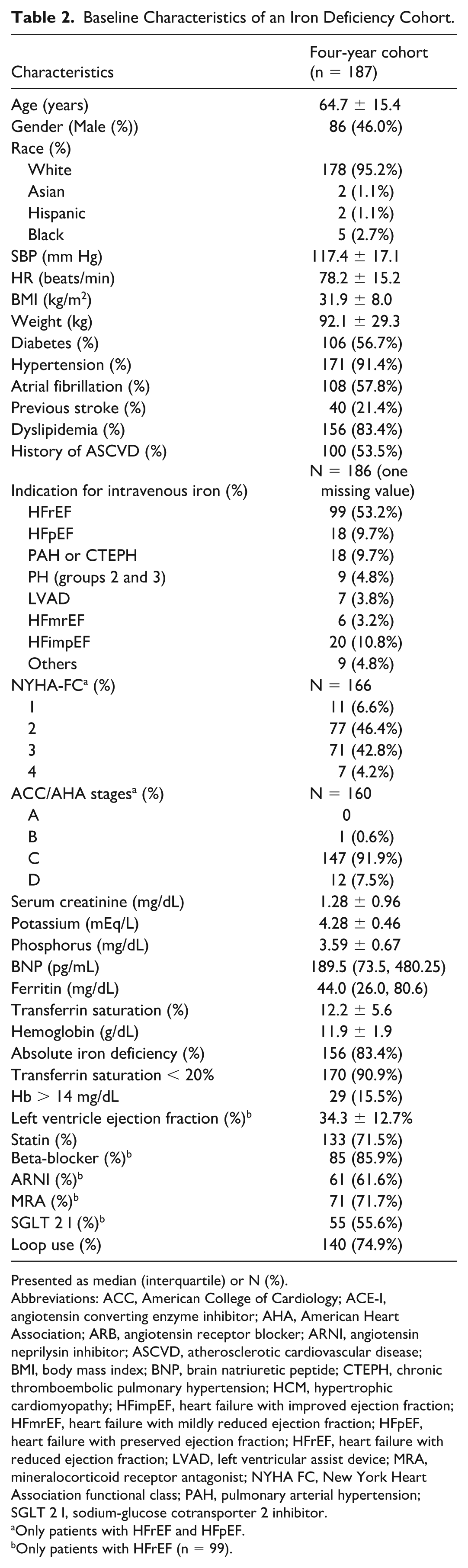
Presented as median (interquartile) or N (%).
Abbreviations: ACC, American College of Cardiology; ACE-I, angiotensin converting enzyme inhibitor; AHA, American Heart Association; ARB, angiotensin receptor blocker; ARNI, angiotensin neprilysin inhibitor; ASCVD, atherosclerotic cardiovascular disease; BMI, body mass index; BNP, brain natriuretic peptide; CTEPH, chronic thromboembolic pulmonary hypertension; HCM, hypertrophic cardiomyopathy; HFimpEF, heart failure with improved ejection fraction; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LVAD, left ventricular assist device; MRA, mineralocorticoid receptor antagonist; NYHA FC, New York Heart Association functional class; PAH, pulmonary arterial hypertension; SGLT 2 I, sodium-glucose cotransporter 2 inhibitor.
Only patients with HFrEF and HFpEF.
Only patients with HFrEF (n = 99).
Outcomes
One hundred fifty-two patients (81.3%) were adherent to the appropriate use criteria, maintenance laboratory requirements, and dosing (Table 3). The most common reasons for nonadherence were the absence of a maintenance laboratory (15.5%), failure to administer all induction doses (1.6%), inappropriate use (1.1%), and incorrect IV iron dose (0.5%).
Outcome Results of the 4-Year Experience Cohort Study.
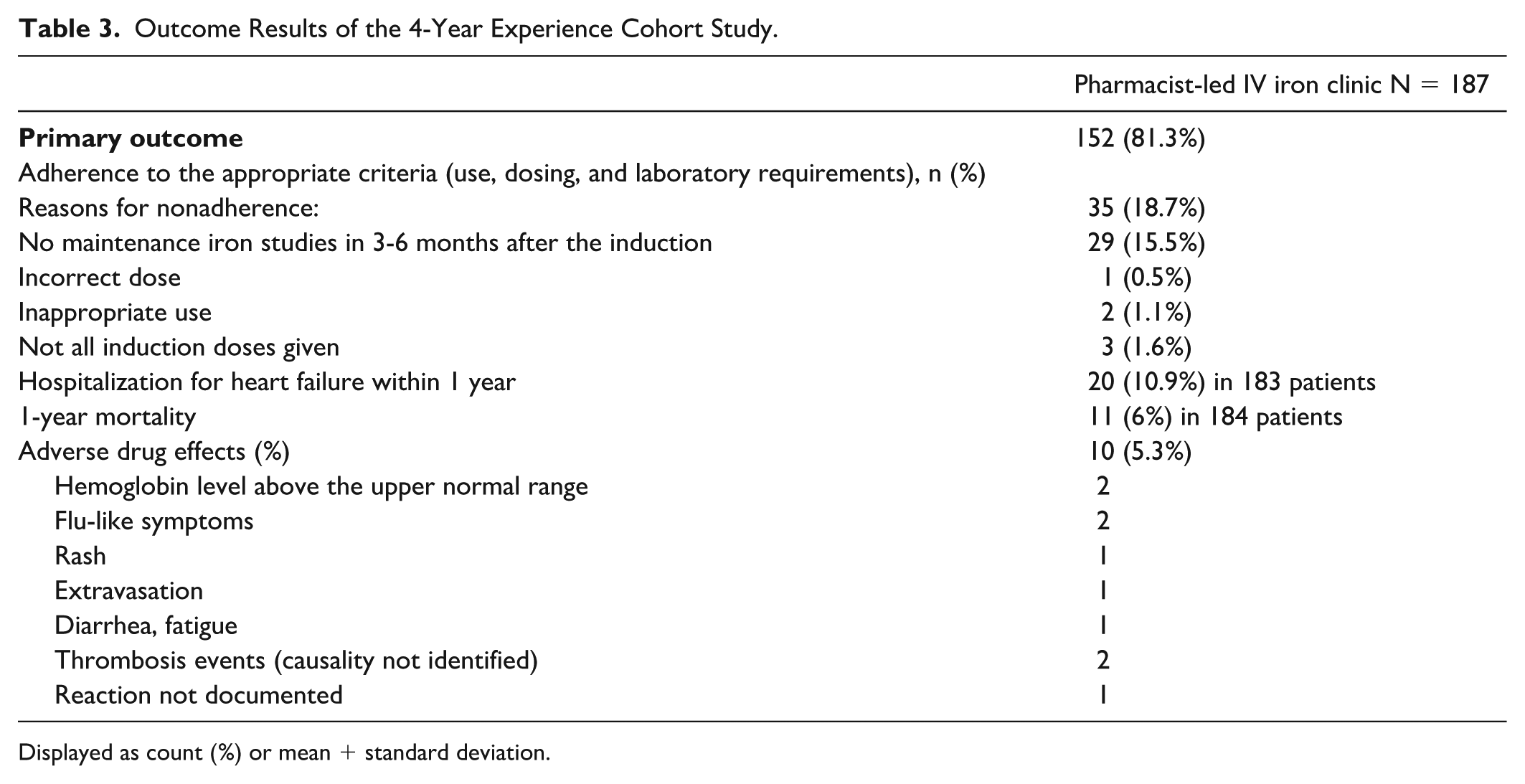
Displayed as count (%) or mean + standard deviation.
Hospitalization for HF at 1 year was 10.9% and 1-year all-cause mortality was 6.0%. The median left ventricular EF at the follow-up was 43.9 (32.5, 55.0) % (P < .001 compared with the median EF 35.0 (25.0, 44.0) % at baseline) (Table 3).
Fifteen patients with HFrEF (15.2%) were receiving oral iron therapy at baseline. Among 15 patients with HFrEF on oral iron therapy, the consulting team discontinued it in 3 patients (20.0%) during follow-up.
Long-Term Iron Therapy Outcomes
Ferritin, transferrin saturation, and hemoglobin values after the IV iron induction phase were significantly increased after an IV iron induction course compared with baseline values (Table 4) and were numerically maintained throughout follow-up (Table 5). Phosphorus levels remained within the normal range throughout the follow-up period.
Clinical Secondary Outcomes Between Baseline and 3- to 6-Month Follow-Up After Induction Course.
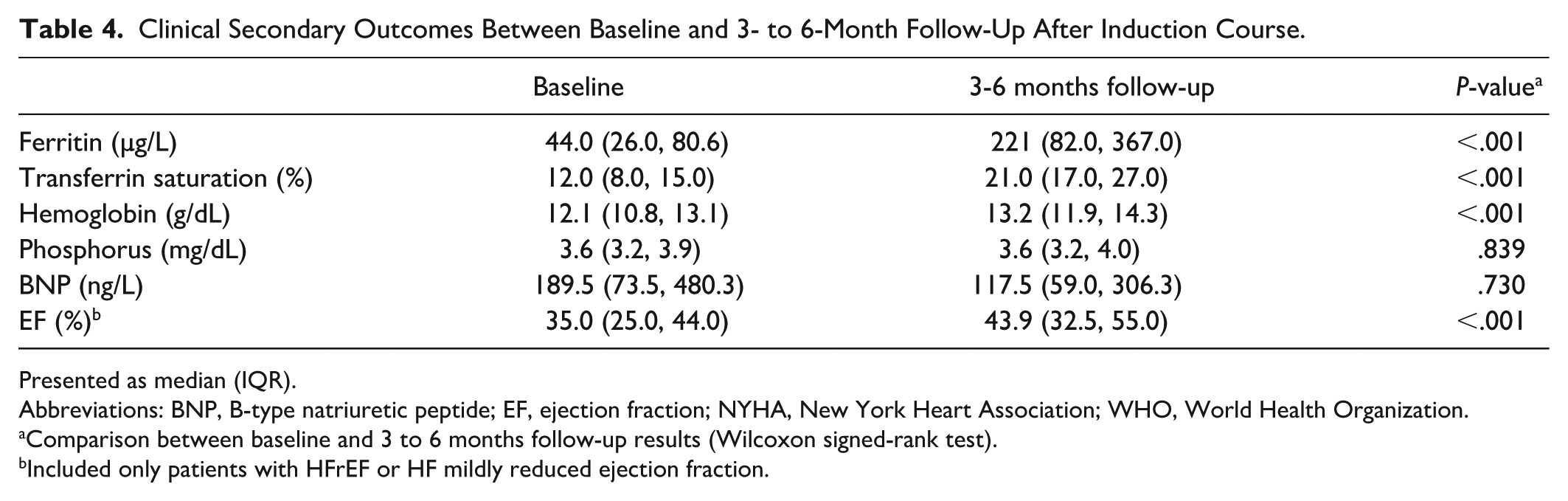
Presented as median (IQR).
Abbreviations: BNP, B-type natriuretic peptide; EF, ejection fraction; NYHA, New York Heart Association; WHO, World Health Organization.
Comparison between baseline and 3 to 6 months follow-up results (Wilcoxon signed-rank test).
Included only patients with HFrEF or HF mildly reduced ejection fraction.
Longitudinal Changes in Laboratory Results, Treatment Achievement Goals, and Oral Iron Therapy Over 4 Years.
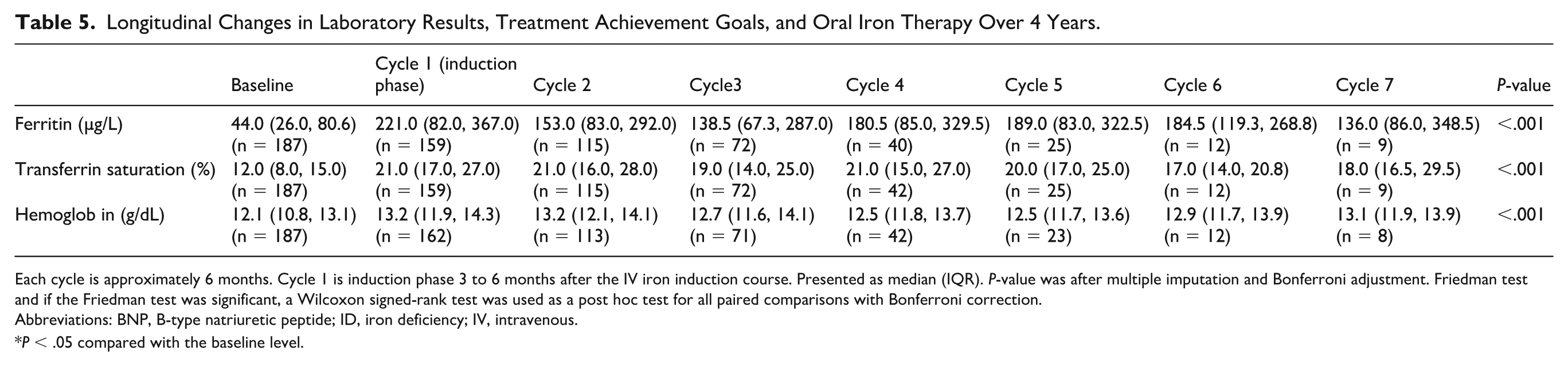
Each cycle is approximately 6 months. Cycle 1 is induction phase 3 to 6 months after the IV iron induction course. Presented as median (IQR). P-value was after multiple imputation and Bonferroni adjustment. Friedman test and if the Friedman test was significant, a Wilcoxon signed-rank test was used as a post hoc test for all paired comparisons with Bonferroni correction.
Abbreviations: BNP, B-type natriuretic peptide; ID, iron deficiency; IV, intravenous.
P < .05 compared with the baseline level.
Geospatial Analysis
Geospatial analysis showed denser patient clusters around infusion centers in the density heat map, represented as yellow-to-red areas (Figure 1). The driving time to the closest infusion centers was significantly shorter than to the Ruby infusion center (26.3 ± 13.4 vs 89.6 ± 53.2 minutes, P < .001). Drive times for all patients were within 75 minutes, with 49% being within 15 minutes of an infusion center.
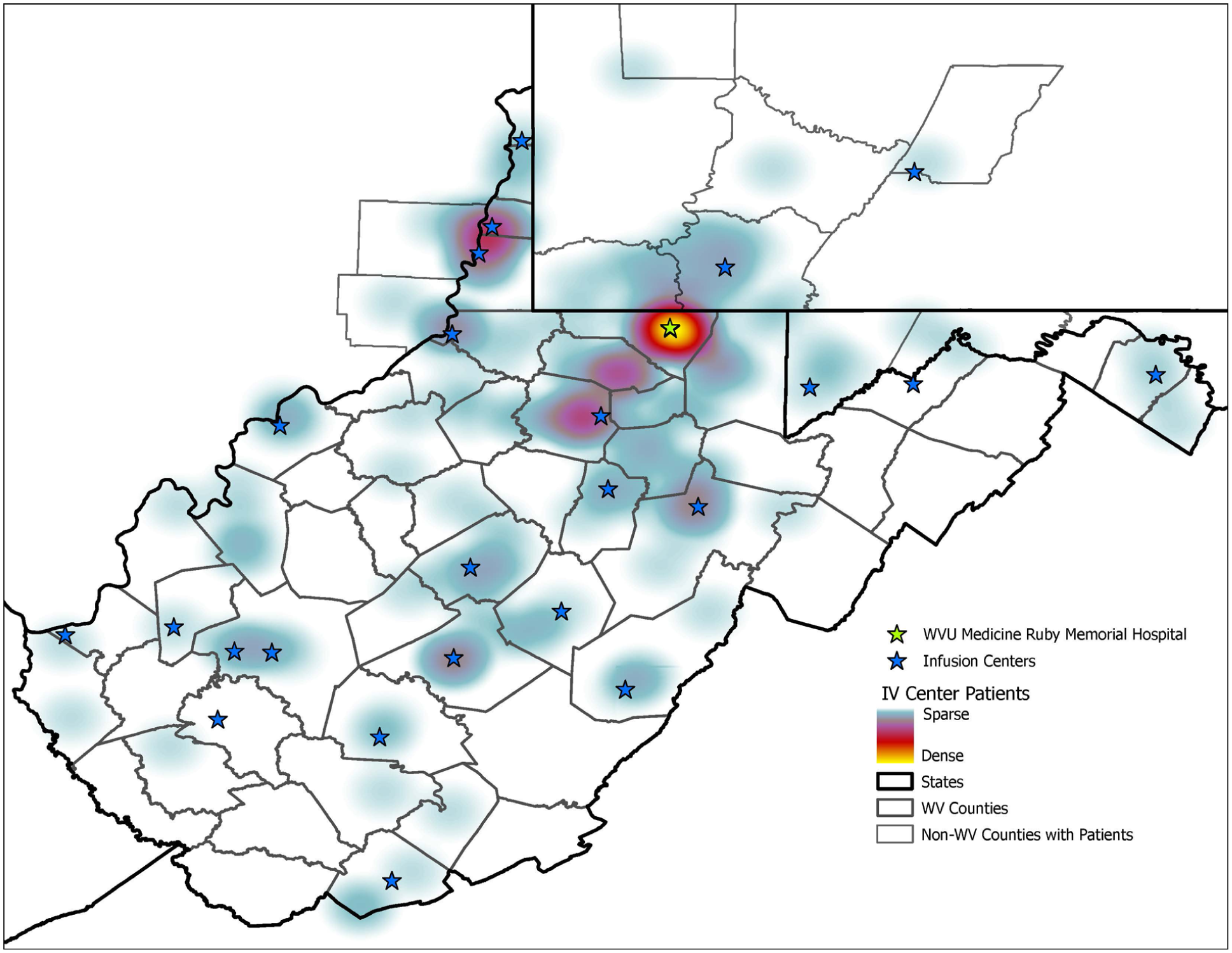
The heat map describing the density of patients around areas in IV iron infusion sites.
Discussion
A pharmacists-providers collaborative iron deficiency clinic coordinated IV iron therapy for 187 patients. More than 80% was adherent to the appropriate use criteria, maintenance laboratory requirements, and dosing. The absence of a maintenance laboratory was the most common reason for nonadherence.
The pharmacists-providers collaborative iron deficiency clinic achieved an adherence rate of approximately 80% to the IV iron guidance (Figure 2). About 82% of nonadherences were due to no follow-up labs within 6 months of induction therapy. These patients either lost follow-ups with the HF service or obtained labs more than 6 months after induction therapy. All nonadherent patients were contacted by the iron deficiency clinic at least 3 times before they were determined to be nonadherent for the follow-up labs. A potential solution to improve this adherence rate is to reinforce the importance of repeating iron studies and hemoglobin labs to promptly assess the needs for IV iron maintenance doses. Another potential strategy is to increase the number of laboratories or to identify the most accessible laboratory locations within each community. Similarly, the expansion of IV iron infusion centers may have improved access to IV iron therapy by shortening drive times to medical facilities that can offer IV iron infusions. A more comprehensive approach in identifying conveniently located laboratories may help reduce missed or delayed repeated iron studies and hemoglobin labs.
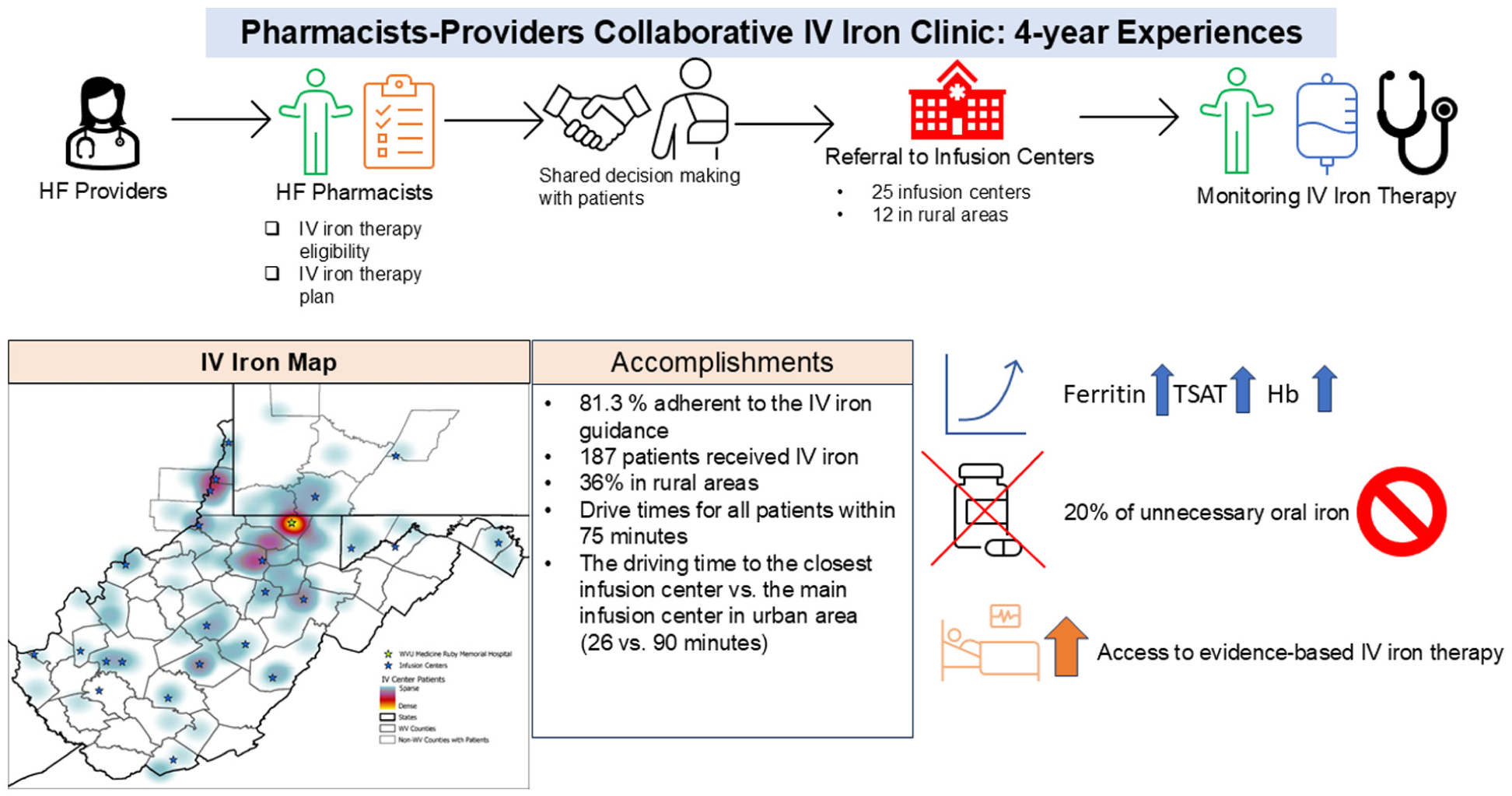
Central illustration. Four-year performance of the pharmacists-providers collaborative iron deficiency clinic.
Limited guidance is available on the duration and monitoring plan for long-term IV iron therapy in practice. HF pharmacists follow up on the labs every 6 months, and approximately 400 to 600 mg of IV iron therapy is administered whenever patients meet the criteria for iron deficiency. The median follow-up period was approximately 1 year, and only a limited number of patients had follow-up longer than 2 years. Further investigations are needed to evaluate the frequency of labs and maintenance labs (every 3 vs every 6 months) and the appropriate criteria for maintenance doses (HF guideline-based criteria vs other criteria, such as transferrin saturation-based criteria).
The present study showed that 15.0% of patients with HFrEF in the study were taking oral iron therapy. The IRON-OUT trial failed to show the benefits of oral iron therapy in patients with HF. 15 Since it is known that polypharmacy and pill burdens affect adherence to pharmacotherapy, ideally, all oral iron therapy can be discontinued once IV iron therapy is initiated. 16 Our study showed that oral iron therapy was discontinued in approximately one-fifth of patients over a median follow-up of 1 year, while the remaining was continued on oral iron therapy. This persistence more likely attributes to clinical inertia and the fact that stopping oral iron therapy was not incorporated with the formal workflow of intravenous iron therapy service. Deprescribing oral iron therapy and reducing pill burdens are the advantages of IV iron therapy. We, therefore, propose that deprescribing oral iron therapy should be an explicit criterion for initiating IV iron therapy in patients with HFrEF.
Limitations
This is a retrospective cohort study, and no causal inference can be made. The most common reason for nonadherence was the absence of follow-up labs within 6 months of the induction course. However, the study lacked sufficient information about the actual timing of all follow-up labs after the induction course. Next, the main results of the present study are only applicable to patients receiving ferric carboxymaltose, as approximately 80% of the patients in the study received it. Further investigation is needed to compare outcomes between ferric carboxymaltose and iron sucrose to apply this data to patients receiving iron sucrose. Third, our study used the adherence to the appropriate IV iron use, dosing, and monitoring as a primary outcome. Clinical outcomes such as hospitalization for HF were evaluated as secondary outcomes. Clinical outcomes as primary outcomes can be considered in future large-scale prospective studies. Fourth, information on changes in guideline-directed medical therapy (GDMT) during follow-up was not available. Consequently, the observed EF improvements from baseline to follow-up may be confounded by the initiation or optimization of GDMT during follow-up.
Conclusion and Relevance
Our retrospective study showed that the pharmacists-providers collaborative IV iron clinic was effective in implementing the guideline-directed IV iron therapy in heart failure care settings. Prospective studies are needed to investigate the clinical effectiveness of the pharmacists-providers collaborative IV iron clinic.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 5U54GM104942-08. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kazuhiko Kido is an independent contractor as a topic editor for DynaMed, LLC. During the preparation of this work, the authors used Grammarly in order to proofread and check grammar errors. The authors reviewed the contents in this manuscript.