
Abstract
Objectives:
The objectives were to evaluate etripamil, an intranasal L-type nondihydropyridine calcium channel blocker (CCB), for the treatment of acute supraventricular tachycardia.
Data Sources:
We conducted a literature search from PubMed, Embase, Cochrane, and Web of Science using key words etripamil, CARDAMYST, and MSP-2017 until April 2026.
Study Selection and Data Extraction:
We analyzed English-language studies focusing on the pharmacology, efficacy, and safety of etripamil.
Data Synthesis:
Etripamil is a fast-acting intranasal CCB developed for the acute management of paroxysmal supraventricular tachycardia (PSVT). Etripamil significantly increased the rate and shortened the time to conversion of acute symptomatic, atrioventricular node-dependent PSVT to sinus rhythm compared with placebo. Etripamil was generally well tolerated; adverse events were primarily mild to moderate and intranasal-related. Notably, there was no significant increase in serious adverse events compared with placebo, with cardiovascular events being rare.
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs:
Etripamil nasal spray is the first nonparenteral, patient-administered therapy approved for the acute termination of PSVT. Etripamil is the only intranasal agent that significantly increases conversion to sinus rhythm compared with placebo in phase III trials. However, its role in certain higher-risk populations, including patients with atrial fibrillation with rapid ventricular rates, remains to be further defined in post-marketing studies and clinical trials.
Conclusion:
Etripamil is an effective and well-tolerated intranasal medication for the acute treatment of PSVT in adults, providing rapid conversion to sinus rhythm and offering a safe, patient-administered option to reduce symptom burden and potentially decrease emergency department utilization.
Keywords
Introduction
Supraventricular tachycardia (SVT) encompasses a group of arrhythmias, in which the atrial and/or ventricular rates (VRs) exceed 100 beats per minute at rest and originate from the bundle of His or above. Paroxysmal supraventricular tachycardia (PSVT) is a subset of SVT that is atrioventricular (AV) node-dependent and characterized by the presence of a regular and rapid tachycardia with abrupt onset and termination, most commonly representing atrioventricular nodal reentrant tachycardia (AVNRT) or atrioventricular reentrant tachycardia (AVRT). 1 Patients with PSVT may have symptoms of palpitations, chest discomfort, shortness of breath, and/or lightheadedness. 2 In the United States, the incidence of PSVT is estimated to be 36 per 100 000 persons annually when adjusted for age and gender. 1 The estimated prevalence of PSVT is 2.29 per 1000 persons. 1 Older adults and female patients are at greater risk of developing PSVT. However, when compared with patients with cardiovascular disease, patients who develop PSVT without cardiovascular disease tend to be younger. 1 Although it is generally considered a benign arrhythmia, SVT contributed to approximately 250 000 emergency department (ED) visits in 2019, requiring greater health care utilization for termination and administration of intravenous (IV) therapies. 3
Vagal maneuvers remain the first line of therapy for PSVT termination. If noninvasive techniques are ineffective, guidelines recommend inpatient administration of IV adenosine for hemodynamically stable patients. While adenosine is effective at terminating PSVT, administration requires presentation to the ED and can cause patient discomfort. Beyond that, IV nondihydropyridine calcium channel blockers (non-DHP CCBs) and IV beta blockers (BBs) can be considered. Oral BBs, diltiazem, or verapamil (“pill-in-pocket”) are potential options for self-administered abortive therapies for PSVT caused by AVNRT, however, with delayed onset due to oral administration and increased adverse effects.1,2,4 Prior to etripamil, there were limited effective pharmacologic options for self-administration of abortive therapy for PSVT termination.
On December 12, 2025, the Food and Drug Administration (FDA) approved etripamil (CARDAMYST) for the management of acute symptomatic episodes of PSVT. Etripamil is a novel intranasal CCB for self-administration enabling patients to treat PSVT episodes in a nonmedically observed setting. 5 Etripamil is a significant therapeutic advancement as it is the first fast-acting abortive therapy, patient self-administered, to terminate PSVT. This article will describe the pharmacology, pharmacokinetics, dosing and administration, clinical efficacy and safety, and potential role of etripamil in the acute management of PSVT.
Data Selection
Clinical trials were found by searching PubMed, Embase, Cochrane, and Web of Science, using the following terms and phrases: etripamil, CARDAMYST or MSP-2017 (investigational name for etripamil). Searches in each database included dates from inception through April 2026.
Clinical Pharmacology and Pharmacokinetics
Etripamil inhibits L-type calcium channels and is classified as a fast-acting non-DHP CCB. L-type calcium channels play a critical role in cardiomyocyte excitation-contraction coupling by mediating calcium entry that triggers myocardial contraction. 6 Etripamil shares a pharmacological scaffold with verapamil. However, etripamil is structurally modified with a rapidly hydrolyzable ester group, resulting in faster onset and a markedly shorter duration of action. It functions by inhibiting calcium influx into cardiomyocytes and nodal cells. This action slows electrical conduction and prolongs the refractory period within the AV node, effectively interrupting the re-entrant circuits responsible for AV-nodal dependent PSVT and facilitating a swift return to sinus rhythm. 5
Etripamil is formulated for intranasal administration, allowing it to be used in medically unsupervised settings. In MSP-2017-1096, a phase 1 randomized, double-blind, placebo-controlled, dose-escalation studies conducted in healthy adults, etripamil demonstrated rapid absorption. Across a dose range of 3.5 to 140 mg, median peak plasma concentrations (Tmax) were reached within approximately 5 to 7 minutes after administration. 7 The mean terminal elimination half-life (t½) of etripamil is dose-dependent. At lower doses (3.5 and 7 mg), the mean t½ is less than 30 minutes, whereas at higher doses (70, 105, and 140 mg), the mean t½ is approximately 2.5 hours. 7 Etripamil is quickly metabolized by blood esterases and transformed to an inactive metabolite (MSP-2030), thus hepatic metabolism is not a major component in its pharmacokinetic profile. 7 The mean tmax of MSP-2030 is also dose-dependent, ranging from 30 minutes in lower doses and 15 minutes at higher doses. 7
Etripamil exerts a rapid, dose-dependent effect on AV nodal conduction, reflected by prolongation of the PR interval. In clinical studies, etripamil increased the mean PR interval from baseline across all active treatment groups, with peak effects occurring within 10 to 18 minutes after administration. The largest percent increases in mean PR interval range from 3.8% at 18 minutes following the lowest dose of 14 mg to 14.6% at 12 minutes after the highest dose of 140 mg, with intermediate doses producing peak effects between these values. Notably, the 3 highest doses (60-140 mg) produced PR interval prolongation exceeding 10%, consistent with clinically meaningful slowing of AV nodal conduction. 7 This peak effect typically persists for approximately 30 to 45 minutes, consistent with etripamil’s rapid metabolic clearance.
In parallel, heart rate decreases following etripamil administration in patients experiencing PSVT. Importantly, patients in sinus rhythm had minimal changes in the heart rate following administration of single or repeated doses of etripamil 70 mg. 8 Maximum mean changes from baseline heart rate were reached approximately 7 minutes after receiving doses ≥30 mg. This leads to a maximum heart rate reduction of 16 beats per minute (bpm) at 30 mg to 37 bpm at 140 mg. Adjustment of PR interval changes for the accompanying decrease in heart rate did not materially alter the findings, confirming a consistent acute PR prolongation of greater than 10% at the highest doses. 7
In the MSP-2017-1096 study, etripamil administration in healthy participants caused an initial sharp decrease in systolic blood pressure (SBP) shortly after dosing, most pronounced at higher doses. Systolic blood pressure returned toward near-baseline levels within approximately 10 minutes. After this early decline, SBP increased modestly in a dose-dependent manner, with maximal mean increases remaining below 10 mm Hg in all dosing groups except for 140 mg, where a peak increase of 12 mm Hg occurred approximately 25 minutes postdose. 7 In NODE-1, a phase II clinical trial, administration of 35 and 70 mg of etripamil did not cause any significant change in mean SBP in SVT patients. Only higher doses of etripamil (105 and 140 mg) transiently reduced SBP. 9 The minimal effects on blood pressure observed with the single 70 mg dose, together with its demonstrated efficacy, supported selection of this regimen as the clinically relevant dose.
Etripamil shares pharmacologic characteristics with verapamil, the established L-type CCB, but represents a significant advancement in drug delivery strategy. Conventional verapamil, when used for acute termination of PSVT, typically requires IV administration in a monitored ED setting to achieve rapid onset. Oral formulations are reserved for chronic prophylaxis. Peak plasma concentrations of single oral doses of verapamil are achieved within 1 to 2 hours. Oral formulations have extensive first-pass hepatic metabolism and a relatively prolonged elimination half-life of 2 to 7 hours. 10 In contrast, intranasal administration of etripamil bypasses the gastrointestinal tract and hepatic portal circulation, resulting in rapid systemic absorption and peak plasma concentrations within minutes. Its short-acting pharmacokinetic profile produces a transient, AV nodal-targeted calcium channel blockade, providing rapid termination of PSVT while minimizing the risk of sustained hypotension or bradycardia. This rapid onset and offset profile support its development as a patient-administered, out of hospital therapeutic option.
Dosing and Administration
The recommended dose of etripamil is one spray (35 mg) into each nostril, for a total dose of 70 mg. If symptoms persist for 10 minutes after administration, a second dose of 70 mg can be administered. Emergency care should be sought if symptoms do not improve within 20 minutes after a second dose. In a 24-hour period, 140 mg of etripamil should not be exceeded. Each device contains 70 mg of etripamil delivered via 2 nasal sprays. 5 No labeled dose adjustment is provided; the effects of renal and hepatic impairment on etripamil pharmacokinetics are unknown. 11 Etripamil is contraindicated in patients with etripamil hypersensitivity, New York Heart Association (NYHA) Class II to IV heart failure, Wolff-Parkinson-White syndrome, Lown-Ganong-Levine syndrome, or manifest preexcitation (delta wave) on 12-lead electrocardiogram (ECG), sick sinus syndrome, or second-degree AV Mobitz 2 block or higher degree of AV block (except in patients with a permanent pacemaker). 5
Clinical Efficacy
The efficacy of etripamil nasal spray was first established in NODE-1, a phase II trial published by Stambler et al. This was a multicenter, randomized, double-blind, placebo-controlled, dose-ranging study conducted in adult patients with documented history of SVT who were scheduled to undergo electrophysiological studies prior to planned catheter ablation. This study assessed the efficacy and tolerability of etripamil nasal spray at doses ranging from 35 to 140 mg for the rapid termination of PSVT. NODE-1 included 104 patients who were randomized in a 1:1:1:1:1 ratio to receive placebo or etripamil at 35, 70, 105, or 140 mg. The median patient age was 55 years. Most patients were female (56.7%) and white (80.8%). Supraventricular tachycardia was induced using standard pacing and programmed stimulation methods. In cases where these methods were not successful in inducing SVT, an IV isoproterenol infusion was started and attempts to induce SVT were repeated. The study drug was administered after a minimum of 5 minutes in sustained SVT. The primary efficacy endpoint was successful conversion of SVT to sinus rhythm, defined as conversion of SVT to sinus rhythm lasting at least 30 seconds occurring within 15 minutes after administering the study drug. The primary efficacy endpoint was achieved in 35%, 65%, 87%, 75%, and 95% in the placebo and etripamil 35, 70, 105, and 140 mg groups, respectively, with statistically higher conversion rates compared with placebo seen in the 70 mg (conversion rate difference 52%; odds ratio [OR]: 12.38; 95% CI: 2.28-82.26; P = .0006), 105 mg (conversion rate difference 40%; OR: 5.57; 95% CI: 1.19-27.63; P = .0248), and 140 mg (conversion rate difference 60%; OR: 37.14; 95% CI: 3.84-1654.17; P < .0001) groups. For the etripamil doses with statistically significant conversion rates, the time at which 50% of patients converted to sinus rhythm was <3 minutes. There were no differences seen in conversion rates between patients who received isoproterenol to induce SVT and those who did not. Beyond the 70 mg dose, there was no significant gain in conversion rates while there was a significant decrease in SBP. The safety and efficacy data from NODE-1 informed etripamil dosing in future studies. 9
NODE-301 was the first in a series of phase III trials examining the use of etripamil nasal spray for termination of PSVT in real-world settings. This was a multicenter, double-blind, placebo-controlled study designed to evaluate the safety and efficacy of etripamil nasal spray administered in a medically unsupervised setting in patients with symptomatic sustained PSVT. Adults with ECG documentation of PSVT (n = 431) were given 1 or 2 test doses of etripamil 70 mg. The 419 patients (97%) who passed the first or second test dose were randomized 2:1 to receive etripamil 70 mg or placebo, respectively. Randomized patients were given a study kit which contained the blinded treatment, either etripamil or placebo, and a cardiac monitoring system (CMS). The patients were trained on steps to undertake if they were experiencing a suspected episode of PSVT, including placement of the CMS and instructions on how to perform a vagal maneuver. If symptoms persisted after performing the vagal maneuver, they were instructed to take a dose of their assigned treatment. Episodes of PSVT and conversion to sinus rhythm were independently adjudicated by a panel of cardiac electrophysiologists. The study kits, patient training, and adjudication process described here were also used in the subsequent phase III trials discussed later. During the study period, 156 patients had a positively adjudicated episode of AV nodal-dependent PSVT that was not terminated by vagal maneuvers and patients subsequently self-administered the assigned treatment. Of these patients, 107 received etripamil and 49 received placebo. The baseline characteristics between the study groups were well balanced. The primary efficacy endpoint was adjudicated termination of positively adjudicated PSVT episodes and conversion to sinus rhythm for at least 30 seconds. The observation period for the study endpoints was 5 hours. While no statistical difference was seen in conversion to sinus rhythm within 5 hours (hazard ratio [HR] = 1.086; 95% CI: 0.726-1.623; P = .1212), 54% of patients receiving etripamil converted to sinus rhythm within 30 minutes compared with 35% of patients receiving placebo. Patients who took etripamil had a numerically shorter estimated median time to conversion as compared with those receiving placebo (25 vs 50 minutes), with a shorter first quartile conversion time (6.8 vs 20.6 minutes). The primary efficacy endpoint likely did not demonstrate statistical significance because the 5-hour observation window chosen by the study investigators was designed to more fully capture safety endpoints. Paroxysmal supraventricular tachycardia is usually limited by time, and the Kaplan-Meier curves were likely to converge during this extended monitoring window. Capturing the primary efficacy endpoint at 30 minutes aligns more with the pharmacokinetic properties of etripamil. This efficacy window was used to inform the design of future phase III trials. 12
The RAPID trial was a multicenter, randomized, placebo-controlled, event-driven trial conducted as part 2 of NODE-301. It evaluated the efficacy and safety of a symptom-prompted repeat dose regimen of etripamil 70 mg nasal spray for acute conversion of AV nodal-dependent PSVT to sinus rhythm. Two etripamil 70 mg test doses were administered to 706 adult patients with ECG documentation of PSVT. Of 706 patients, 692 (98%) tolerated the test doses and were randomized 1:1 to receive either etripamil or placebo. RAPID differed from NODE-301 as patients were instructed to self-administer a second dose of the assigned treatment if symptoms persisted 10 minutes after the initial dose. The optional second dose of etripamil for patients allowed for potential increased medication efficacy. Of those who were randomized, 99 patients in the etripamil group and 85 in the placebo group self-administered the study drug in response to an adjudicated episode of PSVT (efficacy population). The efficacy population was well balanced with a mean age of 54 years, 71% were female and 93% were white. The primary efficacy outcome was conversion of AV nodal depended PSVT to sinus rhythm within 30 minutes and lasting at least 30 seconds. The primary outcome occurred in 64% of the etripamil group and 31% of the placebo group (HR = 2.62; 95% CI: 1.66-4.15; P < .0001) with a median time to conversion of 17.2 and 53.5 minutes in the etripamil and placebo groups, respectively. Self-administration of a repeat dose for persistent symptoms occurred in 65 (66%) of patients in the etripamil arm compared with 67 (79%) in the placebo arm. The rate of recurrence of PSVT after conversion to sinus rhythm within 5 hours of study drug administration was low and occurred in 3 patients in each study arm (3% and 4% in the etripamil and placebo group, respectively). The results of the RAPID trial were pivotal in establishing the labeled dosing of etripamil nasal spray for termination of symptomatic PSVT. 13
NODE-302 was an open-label extension of NODE-301. The primary objective was to evaluate the safety of etripamil 70 mg nasal spray for multiple, spontaneous episodes of PSVT over long-term follow-up (median 232 days, range 8-584 days) in multiple episodes of PSVT. Patients who were randomized in NODE-301 and completed a single treatment with etripamil or placebo, either positively or negatively adjudicated, could transition to NODE-302 provided they qualified based on study inclusion and exclusion criteria. From NODE-301, 169 patients transitioned to NODE-302. A total of 188 positively adjudicated PSVT episodes occurred in 92 patients. Seventy-six patients (72.4%) had 1 [52 (49.5%)] or 2 [24 (22.9%)] perceived PSVT events treated with etripamil and 29 (27.6%) had 3 or more episodes. The primary efficacy outcome was conversion from a positively adjudicated episode of PSVT to sinus rhythm within 30 minutes and lasting at least 30 seconds. In the efficacy population, 7 events were censored, owing to conversion to sinus rhythm prior to drug administration. The primary efficacy outcome was achieved in 109 (60.2%) patients with a median time to conversion of 15.5 minutes. In patients’ first positively adjudicated episode of PSVT, 47 (53.4%) converted in 30 minutes with median time to conversion of 21.1 minutes. In patients with a second positively adjudicated PSVT episode, conversion was achieved within 30 minutes in 24 (63.2%) patients with a median time to conversion of 13.7 minutes. Patient response on the first episode of PSVT appeared to be predictive of response to their second episode. A consistent response was observed in 75% of patients (ie, responded for both episodes or did not respond for either). Logistic regression suggested a statistically significant relationship between a patient’s first and second episodes for conversion to sinus rhythm at 30 minutes (x2 = 8.09; P = .0045). The relationship appeared even stronger when the response was defined as conversion at 15 minutes (x2 = 15.1; P = .0001). 14
NODE-303 was an open-label, single-arm study that evaluated etripamil 70 mg nasal spray in a “real-world setting” for multiple, at-home episodes of PSVT without a test dose before first use. Compared with the prior trials (NODE-1, NODE-301, NODE-302, and RAPID), the inclusion criteria were broadened to include patients with comorbid atrial fibrillation or flutter. In addition, prior ECG documentation of PSVT was not required for inclusion, but diagnosis of PSVT by a medical professional and a patient report of at least 1 previous episode of sustained PSVT were required. Assessments were performed for up to 4 episodes of PSVT per patient. The study protocol was amended approximately 21 months after the start of the study to allow a repeat 70 mg dose to be self-administered if symptoms persisted for 10 minutes following the first dose. In the efficacy population (n = 312), 59.9% of patients converted to sinus rhythm for at least 30 seconds within 30 minutes, and 70.5% of patients converted within 60 minutes of etripamil administration. The median time to conversion was 18.3 minutes. Conversion rates at 30 minutes postetripamil administration for episodes 2, 3, and 4 were 61.6%, 54.95%, and 66.7%, respectively. Conversion rates 60 minutes postdrug administration for episodes 2, 3, and 4 were 73.5%, 57.7%, and 77.8%, respectively. The median time to conversion across episodes 1 to 4 was 14 to 19.2 minutes. For all PSVT episodes, the rate of conversion by 60 minutes postdrug administration was 69.9% (386/552) with a median time to conversion of 17 minutes (95% CI 19.9-22.3). In addition, 71.5% (108/151) of patients treated for at least 2 confirmed episodes of PSVT successfully converted within 60 minutes of etripamil administration. Successful conversion of prior episodes was associated with a 71.7% to 80.6% likelihood of converting during subsequent episodes. Of the 43 patients who were not successful in converting to sinus rhythm during their first episode, 55.8% successfully converted on their second episode with etripamil. 15
Phase II and III clinical trials examining the efficacy of etripamil nasal spray demonstrated superiority over placebo for conversion of PSVT to sinus rhythm within 30 minutes of administration. Furthermore, efficacy of patient-administered etripamil 70 mg nasal spray for conversion of perceived PSVT to sinus rhythm with the option of a second dose for symptoms persisting greater than 10 minutes after first dose administration, was also demonstrated in a “real-world” setting. Study design and efficacy data are summarized in Table 1.
Study Design and Efficacy Outcomes of Phase III Clinical Trials of Etripamil.
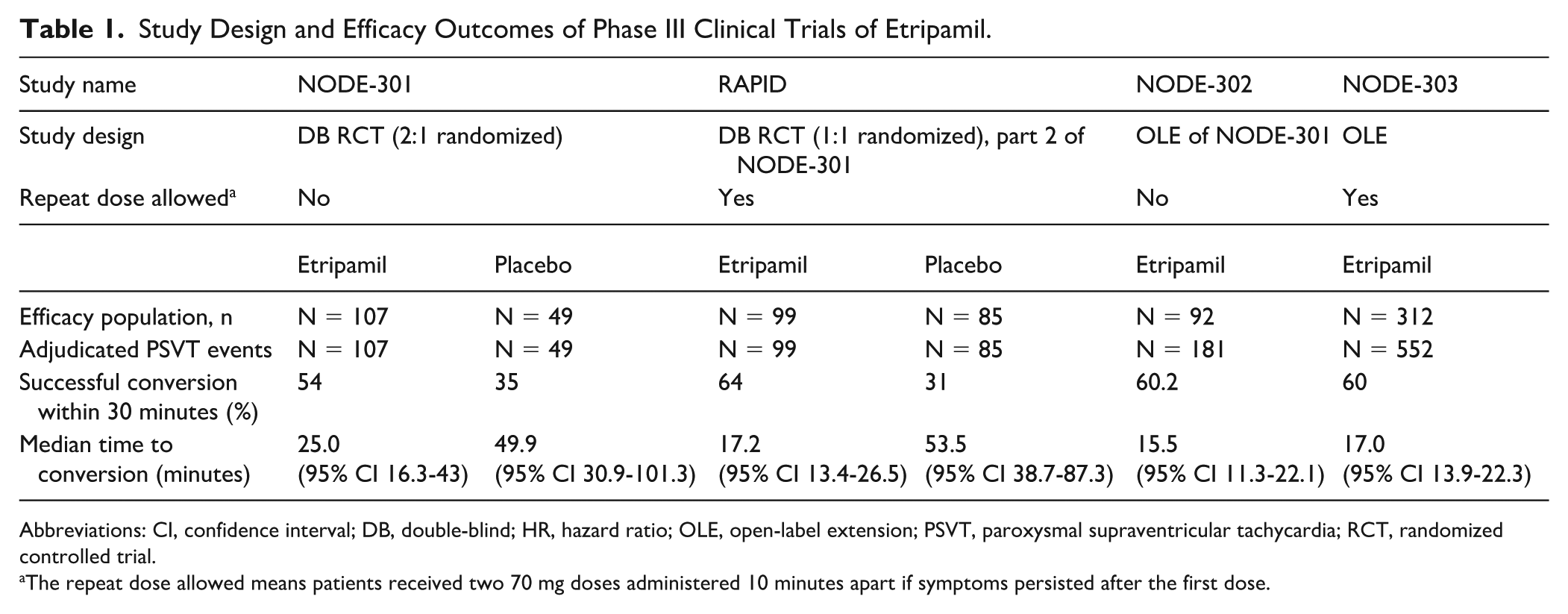
Abbreviations: CI, confidence interval; DB, double-blind; HR, hazard ratio; OLE, open-label extension; PSVT, paroxysmal supraventricular tachycardia; RCT, randomized controlled trial.
The repeat dose allowed means patients received two 70 mg doses administered 10 minutes apart if symptoms persisted after the first dose.
Safety
Etripamil safety was evaluated in 104 patients in NODE-1. Patient vitals and telemetry were monitored for the first 30 minutes after etripamil administration. Adverse events (AEs) were monitored for 12 hours to 5 days after the procedure. At least 1 AE was attributed to the study drug in 70 patients (83.3%) receiving etripamil and 4 (20%) receiving placebo. The incidence of AEs was not related to the etripamil dose used. In general, AEs were mild (44.2%) or moderate (24.0%) in severity across treatment groups. Three patients experienced severe AEs likely related to etripamil: facial flushing, shortness of breath, and chest discomfort in 1 patient; nausea and vomiting in another; cough in the third patient. One patient also had an episode of second-degree AV block and hypotension after conversion to sinus rhythm, which resolved 43 minutes later. Nasal discomfort, nasal congestion, oropharyngeal pain, rhinorrhea, cough, dysgeusia, increased lacrimation, vomiting and nausea occurred most frequently in both the placebo and treatment arms, at rates >10% for etripamil and ≥10% for placebo. It was noted that cough was possibly related to drug presence in the throat, which could be improved by elevating the patients’ head to at least 30 degrees, keeping the chin close to the chest, and avoiding inhaling or swallowing the drug. Patients who received higher doses of etripamil (105 and 140 mg) did have a significant decrease in SBP (–17 and –20 mm Hg) 6 minutes postdose when 65% and 80% of patients were in sinus rhythm, respectively. Sixteen to thirty minutes after receipt of etripamil, there was no difference in mean decrease in SBP from baseline. The lowest patient heart rates within 30 minutes of etripamil or placebo were 58 bpm in the placebo arm, and 70, 55, 71, and 47 bpm in the etripamil 35, 70, 105, and 140 mg arms, respectively. All patients received sedation in this study, which may have impacted rates of bradycardia and hypotension. 9
In NODE-301, the safety population included patients who passed the etripamil test dose and administered study drug during perceived PSVT (n = 198) and patients who only administered the test dose (n = 233). The most common treatment-emergent adverse events (TEAEs), defined as AEs occurring within 24 hours of receipt of the test dose or randomized study drug, were related to nasal administration of the medication. The most common TEAEs are listed in Table 2. Cardiac monitoring system monitoring showed new first-degree AV block lasting >30 seconds in zero patients who received the test dose, 8 (5.8%) patients in the treatment group and 1 (1.7%) patient in the placebo group. Two etripamil treatment arm patients receiving concomitant non-DHP CCB, 4 etripamil treatment patients receiving concomitant BB, and 1 placebo arm patient receiving concomitant BB experienced first-degree AV block. Nonsustained ventricular tachycardia (NSVT) was observed in 15 (11.2%) patients in the etripamil group and 7 (11.7%) patients in the placebo group, not requiring medical treatment. Recurrence of PSVT occurred in 3 (2.2%) etripamil-treated patients and 4 (6.7%) in the placebo group. Second- or third-degree AV block, syncope, and sustained VT were not observed. Ten patients failed the test dose for the following reasons; premature ventricular contractions (PVCs) (n = 3, 2 patients had a history of PVCs), hypotension (n = 2), burning nose (n = 1) lacrimation and sneezing (n = 1), dizziness (n = 1), and for reasons that were not treatment-related AEs (n = 2). No severe events related to etripamil were observed. 12
Common TEAE 24 Hours From Etripamil Phase III Trials.
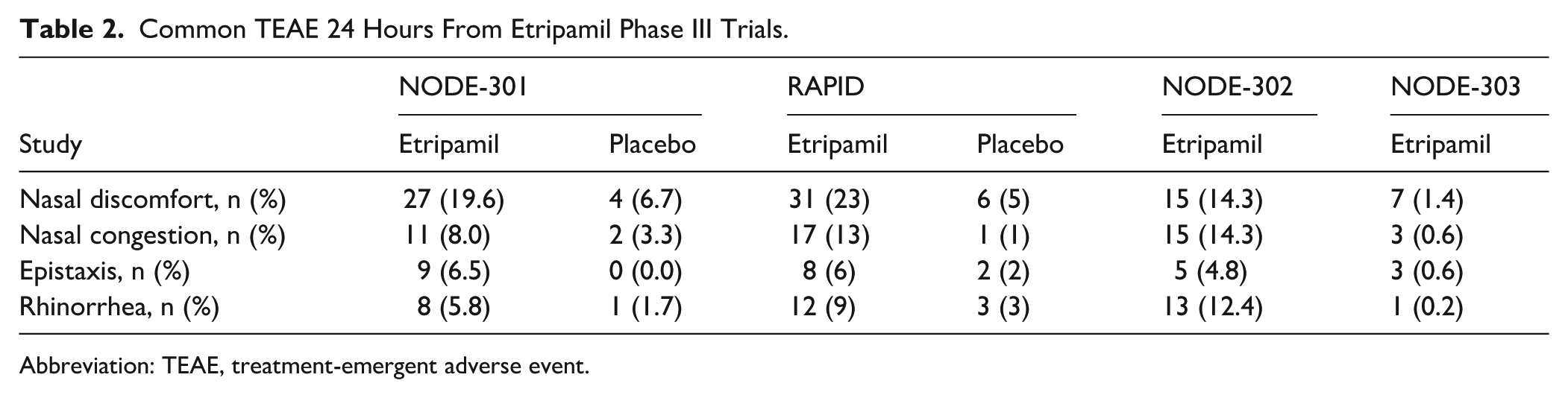
Abbreviation: TEAE, treatment-emergent adverse event.
The safety analysis in RAPID evaluated patients for TEAE within 24 hours of etripamil administration. Of 706 patients enrolled, 692 (98%) tolerated the 140 mg test dose and were randomized. Patients were not randomized after receipt of the test dose for reasons of nasal site discomfort (n = 4), hypotension (n = 1), not meeting blood pressure criteria (n = 2), ventricular arrhythmias (though later determined to be premature atrial contractions with aberrancy) (n = 1), atrial tachycardia (n = 1), or refusal of second test dose (n = 2). The safety population was defined as any patient who received a dose of etripamil or placebo after randomization, for perceived PSVT. Rates of patients with placebo and etripamil TEAEs within 24 hours were 11% (n = 12) and 50% (n = 68), respectively, with rates of common TEAE 24 hours reported in Table 2. In terms of arrhythmias, there were no episodes of syncope, or second- or third-degree heart block associated with etripamil. Rates of reported NSVT were higher in patients who received 2 doses of study drug (etripamil 18%, placebo 20%) compared with 1 dose (10% in both arms) but were not likely related to etripamil use, due to higher placebo rates. Adverse events were similar after repeat etripamil doses, and for patients who administered etripamil for adjudicated arrhythmias other than PSVT. 13
NODE-302 evaluated AEs of etripamil over long-term follow-up for multiple episodes of perceived PSVT. Safety outcomes assessed frequencies of AEs, serious AEs, TEAEs within 24 hours (TEAE 24 h) of receipt of study dose, and etripamil-related TEAEs. Of patients who received etripamil (n = 105), 67 (63.8%) patients reported one or more AEs, and 45 (42.9%) reported one or more TEAE, although only 34 (32.4%) were related to etripamil. Of 235 treated episodes of PSVT, 33 (14%) episodes were for negatively adjudicated episodes of PSVT, hinting at its potential safety for non-PSVT tachyarrhythmias perceived by patients. Similarly, the most common TEAEs were due to intranasal administration; however, this significantly decreased with repeated administration of etripamil. Two severe TEAEs were reported; one patient experienced rhinorrhea and another experienced rhinorrhea and epistaxis. No patients withdrew from the study due to etripamil-related AEs, and no serious AEs were deemed related to etripamil. Cardiac monitoring system did not record any bradyarrhythmias or pauses, nor were there patient-reported episodes of syncope. 14
In NODE-303, patients were able to administer 1 or 2 70 mg doses of etripamil for up to 4 episodes of perceived PSVT, to further evaluate safety with repeat administration. Inclusion criteria were also broadened to include patients with comorbid atrial fibrillation or flutter. Patients were evaluated until study completion or withdrawal for either reaching the maximum of 4 treated episodes or ablation. In total, there were 1054 etripamil-treated perceived PSVT events in this study; approximately 50% (n = 503) of these administrations were first episodes, and others were subsequent, which comprised the safety population. Of the 1054 events, 727 had interpretable ECG CMS data for arrhythmia confirmation. Of these confirmed cases, most (n = 552, 75.9%) were AV-nodal-dependent PSVT, while a few were sinus rhythm/sinus tachycardia (n = 134, 12.7%), atrial fibrillation (n = 25, 2.4%), atrial flutter (n = 4, 0.4%), and atrial tachycardia (n = 4, 0.4%). In the safety population, 428 (85.2%) patients administered a single dose (70 mg) of etripamil for an episode and 75 (14.9%) administered 2 doses (2 × 70 mg). Within the first 24 hours of receiving etripamil, 706 TEAEs were reported in 249 (49.5%) patients that were related to study drug. There were 19 severe drug-related TEAE24h reported in 14 (2.8%) patients. Thirty-three serious TEAEs were reported, but none were related to etripamil. Twenty-four TEAEs were drug-related and led to etripamil discontinuation in 12 patients (2.4%). Adverse event rates and severities were similar between patients who received 1 or 2 doses of etripamil. The rate of drug discontinuation was lower in patients who received 2 doses. Etripamil-related TEAEs were mostly related to nasal drug administration; however, new events were reported leading to study drug discontinuation such as oral discomfort (n = 1, 0.2%), syncope (n = 1, 0.2%), hypoaesthesia (n = 1, 0.2%), and hypotension (n = 1, 0.2%). Treatment-emergent adverse events of special interest (AESI) in safety population, were also reported. These were investigator-identified events not identified by the ECG CMS and occurred within 24 hours of etripamil administration. Twenty-three AESIs were reported in 18 patients. Adverse events of special interest included sinus arrest (n = 2, 0.4%), first-degree AV block (n = 2, 0.4%), second-degree AV block (n = 1, 0.2%), atrial flutter (n = 1, 0.2%), atrial fibrillation (n = 1, 0.2%), dizziness (n = 9, 1.8%), syncope (n = 1, 0.2%), and hypotension (n = 2, 0.4%). Two events were considered severe but not related to study drug. Only sinus arrest and first-degree AV block occurred with repeat dose (2 × 70 mg). Overall, there was a decreasing trend in the percentage of patients with any TEAE24h with multiple treated episodes from 46.9%, 40.3%, 37.8%, and 32.0% in episodes 1 through 4, respectively. This trend suggests the potential for increased tolerance of nasal-related AEs with repeat use. Centrally reviewed ECG data from monitoring devices did not show significant concerns of either bradyarrhythmias or tachyarrhythmias after etripamil. Authors also report that TEAE24h were similar in various age groups (≥60 to <70 years and patients aged ≥70 years) and in those taking concomitant cardiovascular medications. NODE-303 demonstrated that etripamil can be safely administered without a test dose and was the first to evaluate etripamil in patients with comorbid atrial fibrillation and flutter. 15
A summary of common TEAEs within 24 hours of etripamil are reported in Table 2. In general, etripamil was consistently well tolerated when administered in a nonhealth care setting and TEAEs were largely due to nasal administration and decreased in frequency with repeat doses. In each study, a portion of patients concomitantly received oral BBs or CCBs, demonstrating safety of etripamil coadministration with these agents. No severe AEs reported were related to etripamil. Etripamil can be safely self-administered by patients experiencing perceived episodes of PSVT.
Relevance to Patient Care and Clinical Practice in Comparison With Existing Drugs
Etripamil for PSVT Termination
Etripamil nasal spray is the first FDA-approved, nonparenteral, patient-administered treatment option for conversion of PSVT to sinus rhythm. While other “pill in pocket” strategies, including oral non-DHP CCBs and oral BBs are recommended, the strength of this recommendation was reduced from class I to class IIb in the ACC/AHA/HRS SVT guidelines. 1 The “pill in pocket” recommendation was removed from the 2019 ESC guidelines. 16 The downgrade and removal of symptom triggered oral therapy for self-treatment of PSVT is likely due to the limited data supporting its use and the possibility of serious adverse reactions.4,17 Although they have not been directly compared, etripamil may be preferred initially to other patient self-administered abortive therapies or IV therapies for PSVT, due to its favorable tolerability and efficacy profile. Etripamil nasal spray also has a more rapid onset of action than the described oral therapies. Nasal sprays have proven to be an effective and easy to administer dosage form for use by nonhealth care professionals as evidenced by medications such as naloxone and midazolam nasal sprays, which are intended for use by the public in the treatment of medical emergencies.18,19 Providers should adhere to etripamil contraindications to ensure safe use in clinical practice.
Paroxysmal supraventricular tachycardia rarely results in mortality; however, symptoms can be distressing and may lead patients to seek medical attention. Enabling patients to self-terminate an episode of PSVT effectively and safely may result in fewer ED visits and reduced utilization of health care services. A prespecified secondary analysis of NODE-301 and RAPID examined the number of patients in each study arm (etripamil vs placebo) who visited the ED within 24 hours of self-administering their assigned treatment. Although neither NODE-301 or RAPID were sufficiently powered to detect a difference in this outcome, a pooled analysis of both studies including 206 patients in the etripamil arm and 134 patients in the placebo arm indicated a statistically smaller percentage of patients in the etripamil arm visited the ED (P = .04). The analysis found an absolute risk reduction of 8.8% and a number needed to treat of 12. 20
When prescribing etripamil, medication cost and insurance coverage need to be considered. Patient access and copay savings programs exist that may make the medication more affordable to certain commercially insured patients. 21 The wholesale acquisition cost for CARDAMYST is $1649 for two 70 mg nasal spray devices. 22
Etripamil for Atrial Fibrillation
Guideline recommended treatment of atrial fibrillation with rapid ventricular rate (AF-RVR) is similar to recommended treatments for PSVT, with non-DHP CCBs and BBs recommended as first line for acute rate control. 23 Currently, etripamil is being examined for the treatment of AF-RVR with phase II results published and phase III trials planned. It is not yet FDA approved for this indication. 24 ReVeRA-201 was a multicenter, randomized, double-blind, placebo-controlled trial evaluating the safety and efficacy of etripamil in reduction of VR in patients experiencing AF-RVR as compared with placebo. Adult patients presenting urgently to the ED with paroxysmal, persistent, or permanent atrial fibrillation with VR > 110 bpm were included. Patients were required to receive anticoagulation for stroke prevention with atrial fibrillation according to guideline recommendations.25,26 Of the 87 patients screened, 69 were randomized 1:1 to receive etripamil 70 mg nasal spray or placebo. After randomization, 56 patients received the study drug (27 etripamil and 29 placebo) and 49 were included in the efficacy population. Of the 7 patients excluded from the efficacy population, 3 converted to sinus rhythm within 1 hour of receiving a dose of the study drug (2 placebo, 1 etripamil), 3 did not meet the AF-RVR efficacy criteria (1 atrial tachycardia, 2 AF with predrug VR < 100 bpm), and 1 patient had a loss of ECG signal. The primary efficacy endpoint showed the adjusted means of maximum reduction in baseline VR of −34.97 bpm (95% CI –45.13 to –24.8) in the etripamil arm and –5.06 bpm (95% CI –7.44 to –2.67) in the placebo arm, for a difference of –29.9 (95% CI –40.31 to –19.52; P < .0001). A prespecified sensitivity analysis showed consistency with a difference in adjusted means of maximum reduction of VR of –30.26 bpm (95% CI –39.47 to –21.04; P < .0001). 27
A post hoc analysis of NODE-303 examined the effect of etripamil on VR in patients with atrial fibrillation identified at the time of monitor application. There were 18 patients in the post hoc efficacy analysis with 21 ECG adjudicated episodes of atrial fibrillation, including 17 episodes of AF-RVR. VR was recorded for 60 minutes following study drug administration. The baseline VR was 129.7 ± 5.4 bpm and in the AF-RVR subset, baseline VR was 138.3 ± 4.3 bpm. The average maximum reduction in VR was 27.4 ± 6.1 bpm at 22 minutes. In addition, 6 (28.6%) AF episodes converted to sinus rhythm within 1 hour of etripamil administration with a mean reduction of VR from baseline up to 1 minute prior to conversion of 37.5 ± 12.3 bpm. 28 No serious AEs or AESIs were reported in this patient population. In general, AEs were similar in patients with adjudicated atrial fibrillation and PSVT, supporting the safe self-administration of etripamil for inadvertent treatment of non-AV nodal dependent arrhythmias. Rates of anticoagulation for stroke prevention in atrial fibrillation were not reported in this study.
Although patients taking class IC and class III antiarrhythmics were excluded in the NODE trials, 8 patients receiving etripamil (29.6%) in ReVeRA-201 were concomitantly prescribed these agents with serious TEAEs occurring in 1 patient in the etripamil arm and 2 occurring in the placebo arm. 27 Phase III trial results may better elucidate the safety of etripamil coadministration with these agents. 24 No significant drug-drug interactions are known. 11
Currently, etripamil is not approved for the treatment of AF-RVR and remains under investigation for this indication with a phase 3 trial (ReVeRA-301) planned to initiate in 2026. 24
Future Directions
Etripamil safety and efficacy for PSVT termination was demonstrated in the NODE trials, however, limited data examined clinical outcomes associated with etripamil use. Future studies should focus on reduction in ED visits, hospitalizations, health care costs, and other interventions used for PSVT termination, to demonstrate clinical impact of etripamil use. Of note, a phase 4, multicenter, observational registry, “Registry of Etripamil (CARDAMYST) Studies Evaluating Treatment in Paroxysmal Supraventricular Tachycardia (RESET-PSVT) is planned to begin enrollment at the end of 2026 and is aimed at generating real-world evidence on the use of etripamil. The study’s primary endpoint is to characterize patterns of use of etripamil in the management of PSVT, including frequency of PSVT episodes, frequency of etripamil use, number to doses used per episode, and triggers for use. Secondary endpoints include comparisons of patient-reported quality of life, health care utilization, and characteristics of PSVT episode between patients using etripamil versus those not using etripamil. An exploratory analysis of prescribing and use patterns across patient subgroups is planned as well as a qualitative analysis of participant experience. 29
Due to etripamil being administered in nonmedically supervised settings in the NODE trials, the clinical utility of etripamil for ED or in hospital administration is unknown. Future prospective trials should focus on comparing etripamil to other abortive therapies for PSVT requiring inpatient administration. A noninvasive approach to PSVT termination inpatient may be preferred in some patients initially with limited IV access, delays in IV access, or to avoid patient-related discomfort from adenosine or cardioversion. In addition, efficacy and tolerability of inpatient administration of etripamil could further justify prescribing etripamil at hospital or ED discharge. Future studies should also examine the use of consumer-facing digital-health technologies such wearable devices to assist patients in identifying episodes of PSVT and direct treatment with etripamil. 23
Conclusions
Etripamil is the first FDA-approved, intranasal L-type CCB for patient self-administration for PSVT termination. Compared with placebo, etripamil had increased rates of PSVT termination after 30 minutes from administration. Adverse events with etripamil were generally mild or moderate in severity and often related to nasal administration. The approval of etripamil is significant because it provides an option for patient self-administration outside of a medically observed setting. Future studies should focus on clinical outcomes associated with etripamil use in special populations. Etripamil for patient self-administration of abortive treatment of PSVT has been suggested for use by the 2019 ESC SVT guidelines and should be incorporated to future iterations of the SVT guidelines. 16
Footnotes
Acknowledgements
The authors wish to thank Neyda Gilman from Binghamton University Libraries for assistance with the literature search.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.