
Abstract

Dear Editor,
We report a 50-year-old East Asian male who developed symptomatic severe hepatocellular injury following the initiation of dual therapy with rosuvastatin and ticagrelor post-percutaneous coronary intervention (PCI). 1 The patient was initially admitted for a non-ST-elevation myocardial infarction with a baseline alanine aminotransferase (ALT) of 31 U/L and normal renal function (serum creatinine 0.9 mg/dL; eGFR 98 mL/min/1.73 m²). Ticagrelor (90 mg twice daily) was newly initiated on the day of PCI (day 0, December 5). On the following day (day 1, December 6), rosuvastatin (10 mg daily) was added to the regimen. Both medications were newly initiated for this patient. Thirty days post-PCI (29 days after starting the dual therapy), the patient was readmitted, presenting with fatigue and tea-colored urine. Laboratory results revealed severe acute hepatitis (ALT 2246 U/L, aspartate aminotransferase [AST] 1045 U/L) and a peak R-factor of 57.5, indicating a purely hepatocellular injury. Notably, the AST trend closely mirrored the ALT elevation, further supporting a sustained hepatocellular insult. To rule out other statin-related toxicities, creatine kinase (CK) levels were found to be within the reference range (223 U/L), effectively excluding rhabdomyolysis. Viral hepatitis, biliary obstruction, and autoimmune etiologies (antinuclear antibodies (ANA), anti-smooth muscle antibodies (ASMA), and immunoglobulin G [IgG] levels) were also systematically excluded.
An objective causality assessment using the Roussel Uclaf Causality Assessment Method (RUCAM) scale was performed, 2 yielding a score of 8, which indicates a “Probable” relationship between the combined drug therapy and the hepatic injury. Initially, rosuvastatin was discontinued; however, the ALT level exhibited a “stalled de-challenge” response, plateauing at >300 U/L for approximately 60 days. Given the failure of biochemical normalization, ticagrelor was discontinued on day 93 post-PCI, and the patient was switched to clopidogrel 75 mg daily. Following the cessation of ticagrelor, rapid recovery was observed, with an 85% reduction in ALT within 13 days, normalizing to 38 U/L by day 106 post-PCI (Figure 1). To ensure complete hepatic recovery and avoid further confounding factors, no other statins or antilipidemic agents were initiated during this period.
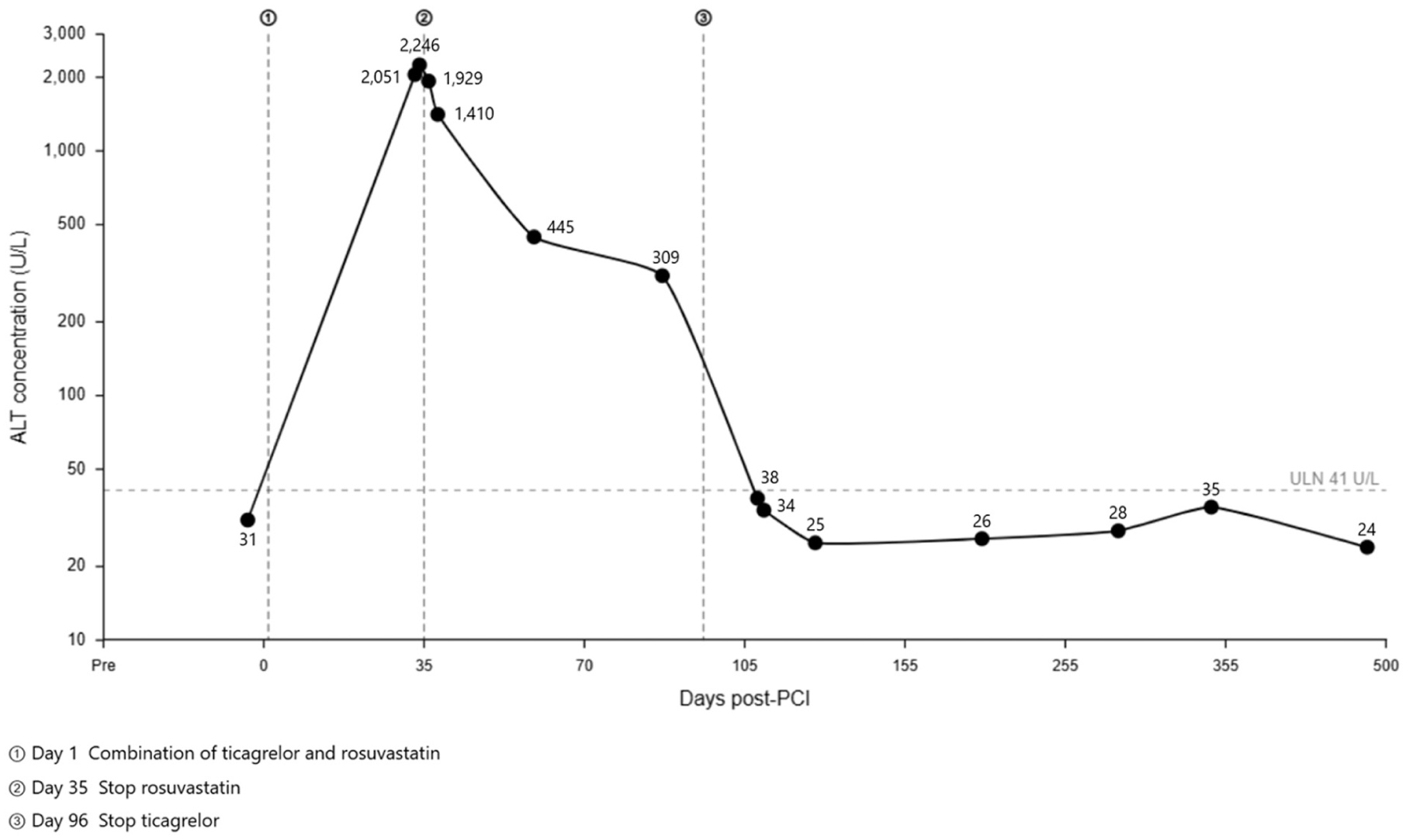
Longitudinal assessment of alanine aminotransferase (ALT) following the discontinuation of rosuvastatin and ticagrelor.
Identifying the specific causative agent in multidrug drug-induced liver injury (DILI) is challenging, particularly when standard de-challenge fails. 3 Initially, rosuvastatin was deemed the most likely causative agent due to the clear temporal relationship following its initiation and its documented association with idiosyncratic liver injury. However, the rapid and severe nature of the enzyme elevation in this case was atypical for standard statin toxicity. This clinical discrepancy, combined with the “stalled de-challenge” response observed after rosuvastatin cessation, strongly suggested that the injury was not an isolated drug effect but rather driven by a potent drug-drug interaction (DDI) that exacerbated the toxic potential of the statin. This case highlights a critical clinical question: do DDIs increase the potential for hepatotoxicity and significantly prolong the time to resolution? Our observations suggest they do. Current evidence indicates that ticagrelor and its active metabolites are potent inhibitors of Breast Cancer Resistance Protein (BCRP), for which rosuvastatin is a major substrate. As highlighted in recent studies by Lehtisalo et al 4 and Dermota et al, 5 ticagrelor can lead to a nearly 2-fold increase in the elimination half-life of rosuvastatin. This prolonged half-life likely explains the sustained hepatic injury observed even after statin cessation, as residual rosuvastatin clearance remained hindered by the ongoing ticagrelor administration, effectively extending the time to resolution. The selection of rosuvastatin 10 mg daily, while a standard moderate-intensity dose in our post-PCI program, warrants critical consideration in the context of the patient’s East Asian ethnicity. While this dose was initiated based on cardiovascular secondary prevention guidelines without pre-existing contraindications, it may not have reflected sufficient individualization for a patient transitioning to complex dual therapy, including ticagrelor. Pharmacogenetic data suggest that East Asian subjects exhibit higher systemic exposure (AUC) to rosuvastatin compared to Western populations, and the addition of a potent BCRP inhibitor like ticagrelor likely acted as a catalyst for the severe hepatocellular injury observed. 4 A more pre-emptive risk mitigation strategy, such as initiating a lower dose (5 mg) or performing baseline genetic screening for solute carrier organic anion transporter family member 1B1 (SLCO1B1) and ATP binding cassette subfamily G member 2 (ABCG2) polymorphisms, might have reduced the severity of the subsequent DILI. 6 Ultimately, this case demonstrates that DDIs can act as a “kinetic trap,” in which the interacting agent (ticagrelor) prevents clearance of a hepatotoxic substrate (rosuvastatin), thereby increasing its toxic potential. 7 When liver enzymes fail to recover after removing a suspected statin, concurrent medications like ticagrelor must be evaluated not only as potential co-offenders but also as factors that prolong the clinical resolution of the injury.
Footnotes
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki. Since this is a retrospective case report of a single patient undergoing standard clinical care, our institution waived formal institutional review board approval, and the patient’s privacy has been strictly protected.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Author Contributions
T-RP and T-WW were both involved in the clinical management of the patient and the conceptualization of the case report. T-RP performed the literature review and drafted the initial manuscript. T-WW provided critical revisions for intellectual content and supervised the work. All authors have read and approved the final version of the manuscript.