
Abstract
Background:
The preferred dosing strategy for phenobarbital in alcohol withdrawal syndrome (AWS) is not well established.
Objective:
We compared the effects of a 10- vs 20-mg/kg dose on the incidence of severe AWS and benzodiazepine use.
Methods:
This retrospective cohort study included patients who received a phenobarbital front-loaded dose with either 10 mg/kg or 20 mg/kg. The primary endpoints were severe AWS (Clinical Institute Withdrawal Assessment [CIWA] score ≥15, use of restraints, or seizures) and total lorazepam equivalents. Secondary endpoints were the frequency of intubation and intensive care unit (ICU) length of stay.
Results:
We included 135 patients (n = 71, 10 mg/kg; n = 64, 20 mg/kg). Demographics were similar except baseline CIWA, cirrhosis history, and benzodiazepine administration pre-phenobarbital were higher in the 10-mg/kg group. The incidence of severe AWS was higher in the 10-mg/kg group (56.3% vs 32.8%; P = .006), as was lorazepam administration 48-hour post-phenobarbital load (7 ± 10.3 vs 2.6 ± 5.9 mg; P < .001). After controlling for differences in baseline CIWA scores, there was no difference in severe AWS (odds ratio [OR] [95% CI] = 0.532 [0.215 to 1.315]), but benzodiazepine usage was lower in the 20-mg/kg group (B = −3.376, P = .046). The frequency of new intubation was 5.9% and 10.2% for the 10- and 20-mg/kg groups, respectively (P = .483). No difference in ICU length of stay was noted (10 mg/kg, 4.5 ± 3.4 vs 20 mg/kg, 3.9 ± 3.6; P = .411).
Conclusion and Relevance:
A 20-mg/kg phenobarbital dose did not reduce severe AWS but may lower benzodiazepine usage in the early withdrawal period. A 20-mg/kg dose was not associated with increased intubations. Clinicians may consider this option when crafting phenobarbital dosing regimens in patients with severe AWS.
Introduction
Alcohol is the most common substance used by adults in the United States and is associated with more than 178 000 deaths per year. 1 Alcohol withdrawal syndrome (AWS) is a potentially deadly complication that can occur following the abrupt cessation or reduction of alcohol. Approximately 50% of patients with alcohol use disorder will experience AWS upon decreasing or discontinuing use. 2 Severe forms of AWS can lead to seizures and/or delirium tremens, which carry a significant morbidity and mortality risk.
Benzodiazepines are used as first-line agents for the management of AWS, but phenobarbital has increasingly been described as an effective alternative. 3 Phenobarbital, like the benzodiazepines, works by enhancing the activity of gamma-aminobutyric acid (GABA) but also inhibits the effects of glutamate. Furthermore, the long half-life provides an important advantage with dosing with continued efficacy for an extended period of time after administration, without the need for additional doses via a taper.
Multiple dosing strategies have been described in the literature, with the most common being a single, large loading dose (ie, front-loading strategy), low-intermittent dosing (eg, 260 mg ×1, then 130 mg every 15 min as needed) or symptom-based dosing according to a validated scoring system. 3 One study compared a front-loaded strategy with low-intermittent doses, and a significant reduction was noted in mechanical ventilation incidence and sedative use with front-loaded dosing. 4 There is wide variance, though, with the specific dose used as part of a front-loaded strategy, as there are few comparative data to guide clinicians. Currently, our institution utilizes either a 10- or 20-mg/kg loading dose of phenobarbital for AWS. This is centered around phenobarbital pharmacokinetics and serum concentrations extrapolated from seizure data. The objective of this study was to determine whether a 10-mg/kg or 20-mg/kg loading dose of phenobarbital results in a lower frequency of severe alcohol withdrawal and lower benzodiazepine use.
Methods
The Institutional Review Board (IRB) approval was obtained prior to initiation of the study. This retrospective cohort study evaluated patients admitted to 2 affiliated hospitals between October 2021 and October 2024. All patients who were prescribed a phenobarbital loading dose were identified from the institution’s electronic medical record. Patients were included if they were at least 18 years of age and had phenobarbital ordered specifically for the indication of AWS with Clinical Institute Withdrawal Assessment for Alcohol–Revised (CIWA-Ar) monitoring. Exclusion criteria were pregnancy, use of antiseizure medication prescribed for a seizure disorder, and current use of phenobarbital in the outpatient setting.
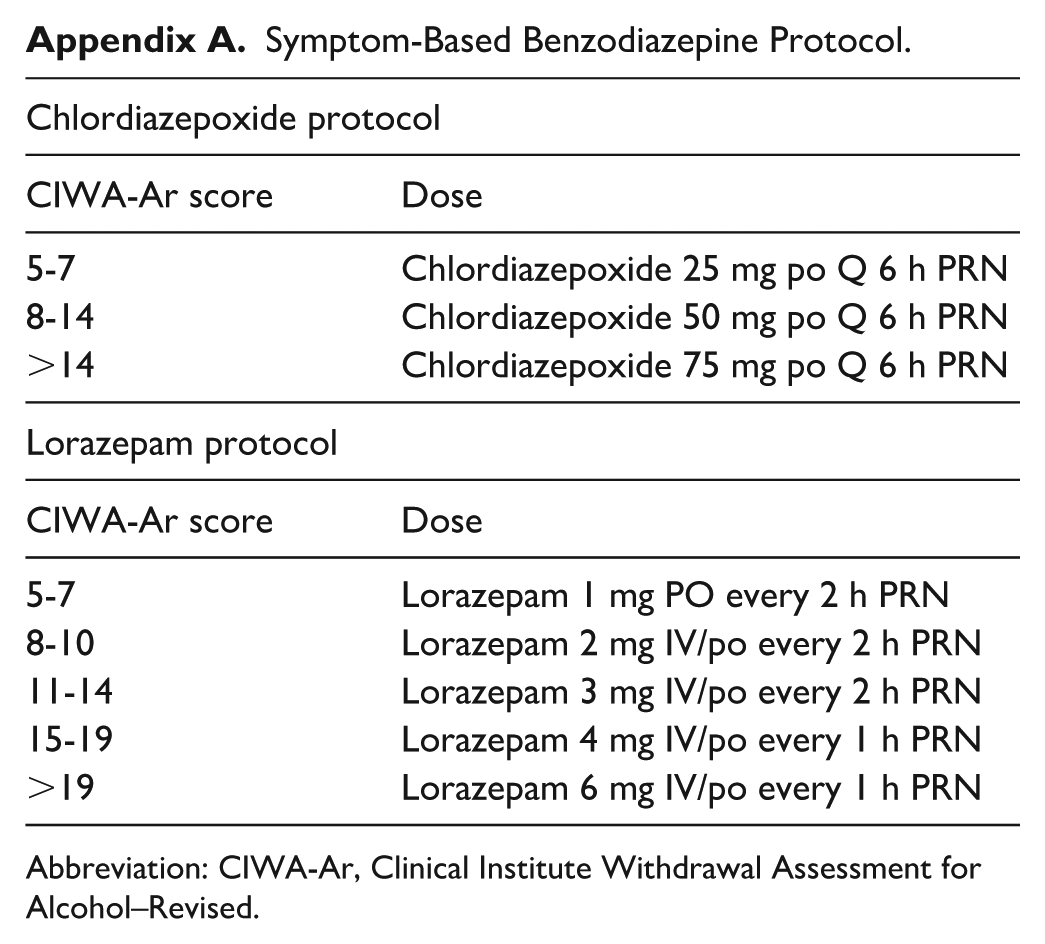
Standard management for alcohol withdrawal at our institution consists of a symptom-based protocol based on CIWA-Ar scores using a benzodiazepine (Appendix A). Phenobarbital is not part of that protocol but is often used in patients considered high-risk for severe AWS (Prediction of Alcohol Withdrawal Severity Scale [PAWSS] > 3) by the treating physician. When phenobarbital is prescribed, a front-loaded strategy is utilized with repeat loading doses given as needed. No taper is utilized. Our practice for weight-based phenobarbital dosing is to use ideal body weight unless this is greater than total body weight. All doses are administered intravenously as a single, 30-minute infusion; loading doses are not split into smaller doses administered sequentially. Phenobarbital loading doses are only permitted in the emergency department or intensive care unit. Symptom-based control is maintained with a benzodiazepine as per the institutional protocol. The management of AWS is primarily overseen by the neurocritical care service, who works in conjunction with the primary team.
Patients meeting the inclusion/exclusion criteria were stratified into 2 groups based on the initial loading dose of phenobarbital prescribed. Data collected included demographics, PAWSS (where documented), CIWA-Ar scores, benzodiazepine and phenobarbital utilization (up to 7 days post-phenobarbital load), phenobarbital serum concentrations, adjunctive AWS medications received following phenobarbital (eg, dexmedetomidine, propofol, gabapentin, clonidine, haloperidol, quetiapine), frequency of mechanical ventilation, occurrence of severe alcohol withdrawal, intensive care unit (ICU), and hospital lengths of stay. Data abstraction was performed using automated computerized reporting systems and manual chart review. Manual chart review was performed by a single author (following training by the senior authors), and quality assurance was performed by 2 senior authors.
The primary endpoints of this study were the incidence of severe AWS and benzodiazepine utilization. Severe alcohol withdrawal was defined as a CIWA-Ar score ≥ 15, the use of restraints post-loading dose, or the occurrence of seizures post-loading dose. Benzodiazepine utilization consisted of the total quantity of benzodiazepines used up to 1 week, converted to milligram lorazepam equivalents. 5 Analysis of benzodiazepine use was performed at 48 hours and total, up to 7 days. Secondary endpoints assessed included frequency of intubation (at any time post-phenobarbital load up to 7 days) and ICU length of stay.
Statistical Analysis
Data were presented as mean (± standard deviation) if normally distributed, median (interquartile range) if skewed, or n (%) if categorical. Continuous data were assessed using the Student’s t-test for normally distributed data and the Mann-Whitney U test for skewed data. Categorical data were assessed using Pearson’s chi-square test or Fisher’s exact test, as appropriate. A univariate analysis was performed to evaluate potential confounders for consideration for a multivariable analysis along with other factors that may be clinically relevant. Multivariable analysis was performed using logistic regression, where all variables were entered simultaneously. Model discrimination and calibration was evaluated using receiver operating characteristic (ROC) area under the curve (AUC) and Hosmer-Lemeshow test. Linear regression was performed to evaluate the relationship between phenobarbital dose and benzodiazepine dosing. Results are reported as B-coefficients with 95% confidence intervals. Statistically significant differences were assessed based on a P-value of < .05. SPSS version 29 (IBM, Armonk, New York) was used for all statistical analyses.
Results
A total of 418 patient charts were reviewed with 135 meeting the inclusion/exclusion criteria. The most common admitting diagnosis for the study cohort was ground-level fall (36%), followed by AWS or seizures (18%), motor vehicle collision (10%), and encephalopathy or altered mental status (10%). Seventy-one patients received a 10-mg/kg loading dose, while 64 patients received a 20-mg/kg loading dose. The time to phenobarbital administration was 12 (4.8-24) vs 7.2 (4.8-12) hours, P = .031. Baseline demographics were similar with the exception of cirrhosis, CIWA-Ar score immediately before phenobarbital and benzodiazepine use 24 hours pre-phenobarbital (Table 1). Multivariable analysis revealed patients were more likely to receive a 10-mg/kg dose if they had a history of cirrhosis (odds ratio [OR] [95% CI] = 4.86 [1.41 to 16.78], P = .012) or received a higher dose of benzodiazepine prior to phenobarbital (OR [95% CI] = 1.16 [1.02 to 1.31], P = .026; ROC AUC = 0.686 [0.596 to 0.775]).
Demographics.
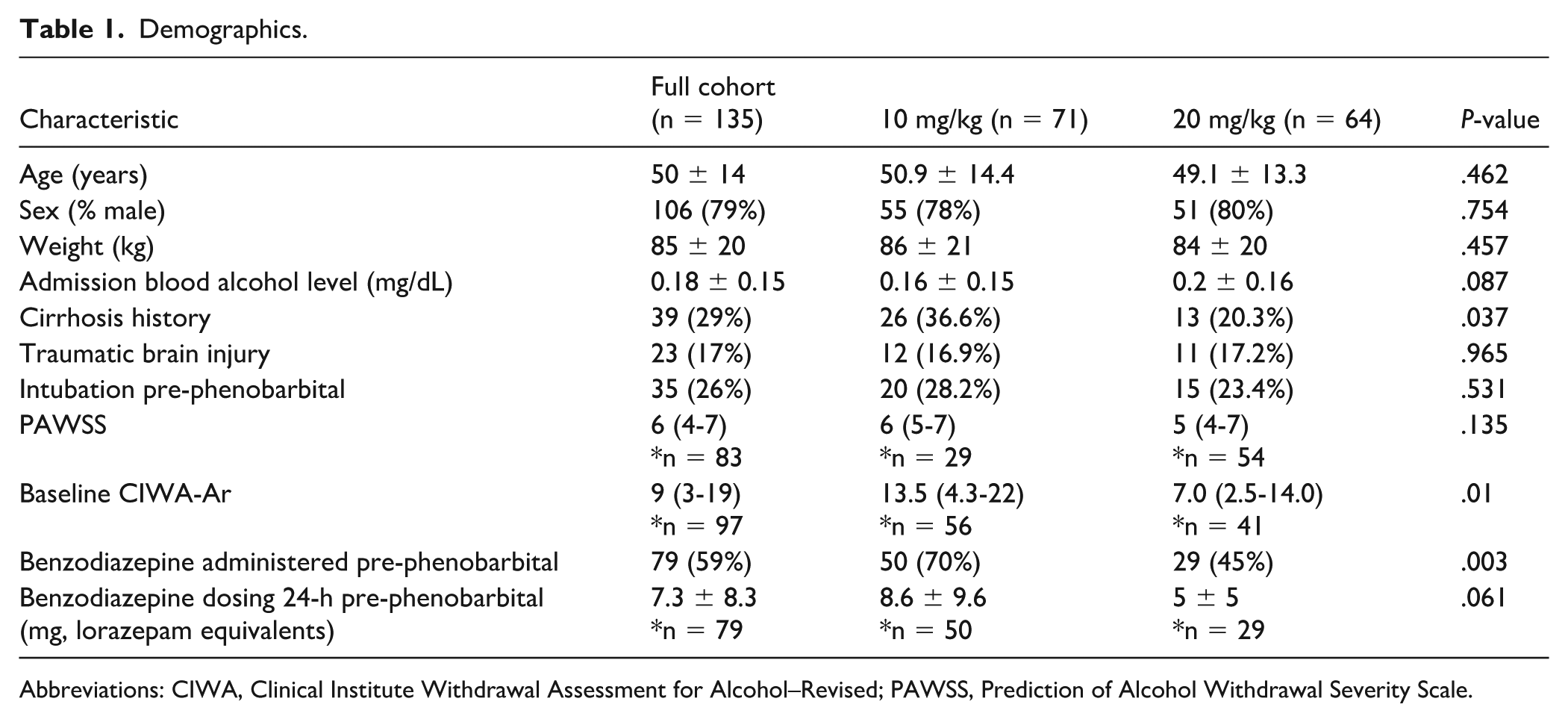
Abbreviations: CIWA, Clinical Institute Withdrawal Assessment for Alcohol–Revised; PAWSS, Prediction of Alcohol Withdrawal Severity Scale.
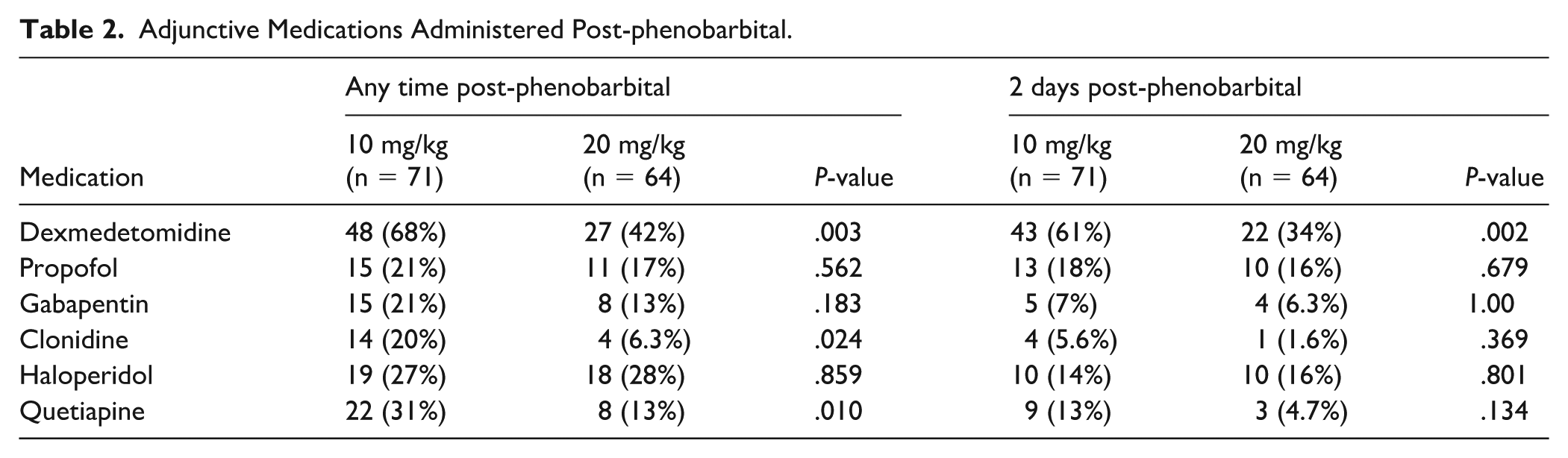
Initial, post-load phenobarbital levels were significantly higher in the 20-mg/kg group (12.1 ± 2.8 vs 22.9 ± 5.5; P < .001). Additional phenobarbital was administered within the next 48 hours in 37% (n = 26) and 33% (n = 21) of patients in the 10-mg/kg and 20-mg/kg groups, respectively. At 48 hours, the cumulative phenobarbital dose received was 13 ± 5.2 mg/kg in the 10-mg/kg group and 23 ± 4.8 mg/kg in the 20-mg/kg group. The use of adjunctive medications (related to AWS) is listed in Table 2.
Adjunctive Medications Administered Post-phenobarbital.
The incidence of severe alcohol withdrawal was 56% (40/71) and 33% (21/64) for the 10-mg/kg and 20-mg/kg groups, respectively (P = .006) (Table 3). Variables associated with severe AWS via univariate analysis are displayed in Table 4. After controlling for baseline CIWA-Ar, via multivariable analysis, there was no difference in the frequency of severe AWS with a 20-mg/kg phenobarbital dose (OR [95% CI] = 0.532 [0.215 to 1.315]; P = .172; ROC AUC = 0.734 [0.634 to 0.833]).
Severe Alcohol Withdrawal Syndrome Symptoms. a
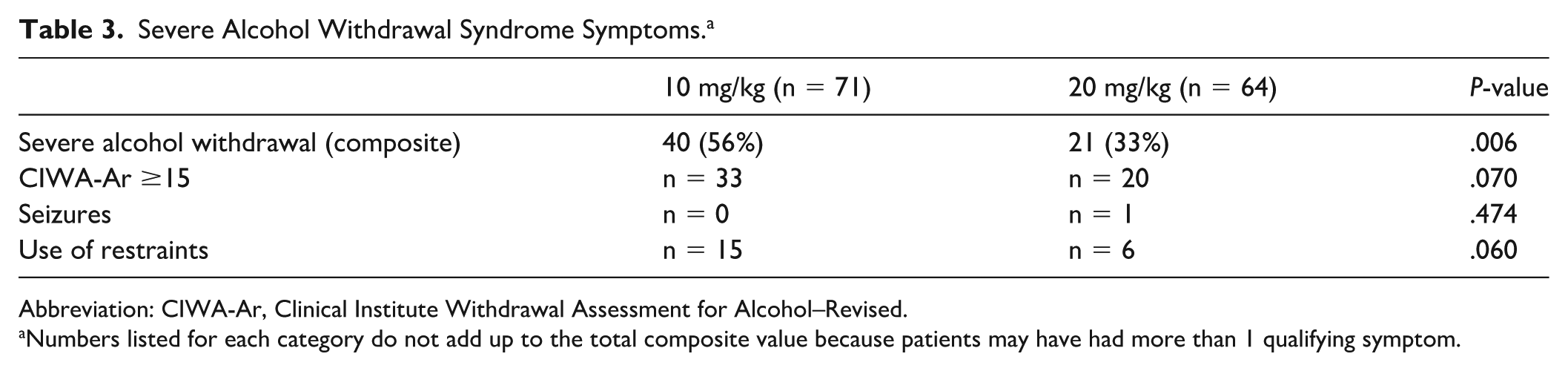
Abbreviation: CIWA-Ar, Clinical Institute Withdrawal Assessment for Alcohol–Revised.
Numbers listed for each category do not add up to the total composite value because patients may have had more than 1 qualifying symptom.
Univariate Analysis for Severe Alcohol Withdrawal.
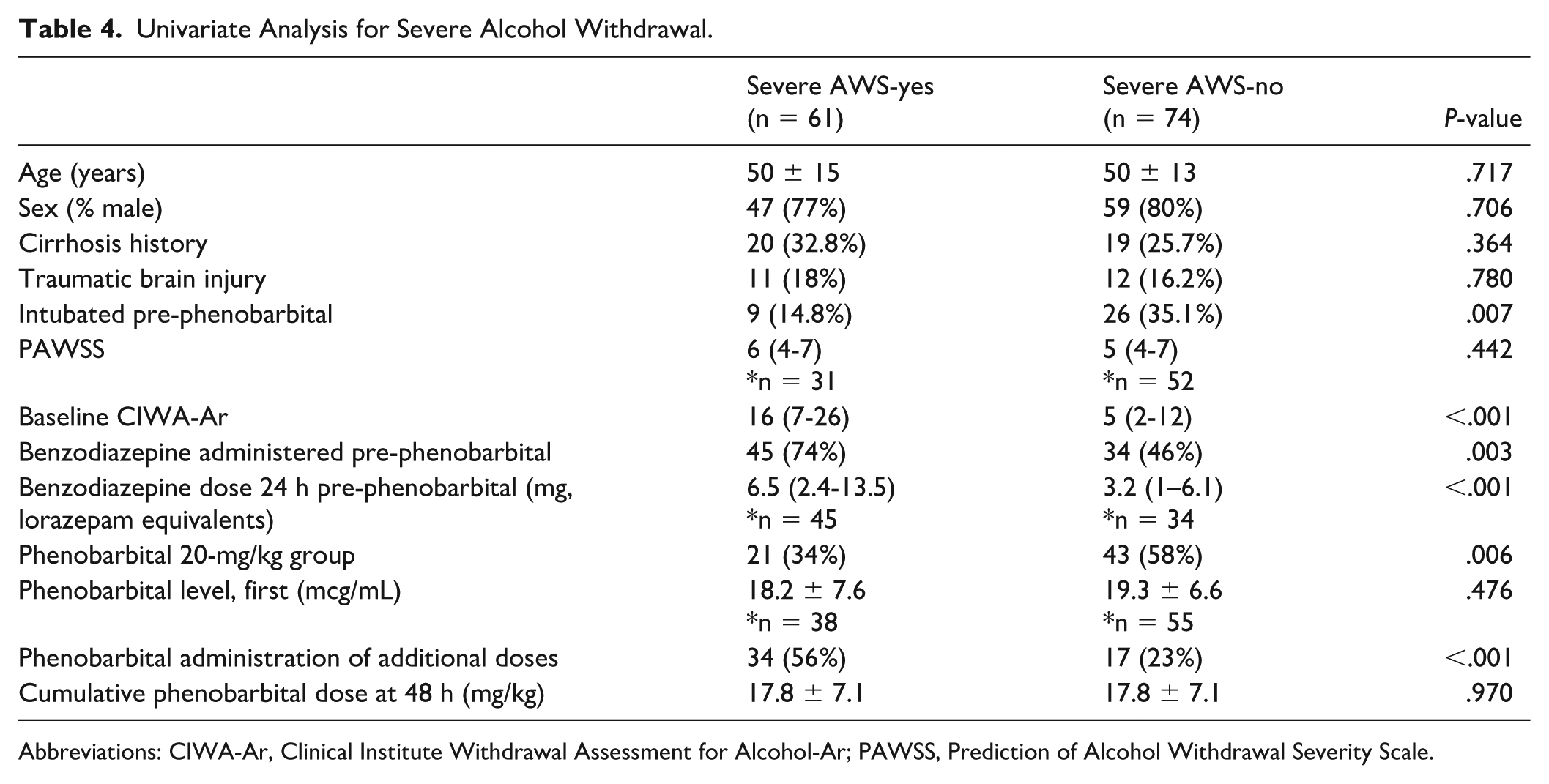
Abbreviations: CIWA-Ar, Clinical Institute Withdrawal Assessment for Alcohol-Ar; PAWSS, Prediction of Alcohol Withdrawal Severity Scale.
Benzodiazepine use was higher in the 10-mg/kg group for both the 48-hour assessment (7 ± 10.3 vs 2.6 ± 5.9, P < .001) and the 7-day study duration (15.4 ± 19 vs 8.4 ± 18.8, P = .033). Daily lorazepam equivalent usage is displayed in Figure 1. After adjusting for differences in baseline CIWA-Ar, these differences remained statistically significant at 48 hours (B [95% CI] = −3.376 [−6.684 to −0.068], P = .046) but not for the 7-day total (B [95% CI] = −3.241 [−11.134 to 4.652], P = .417).
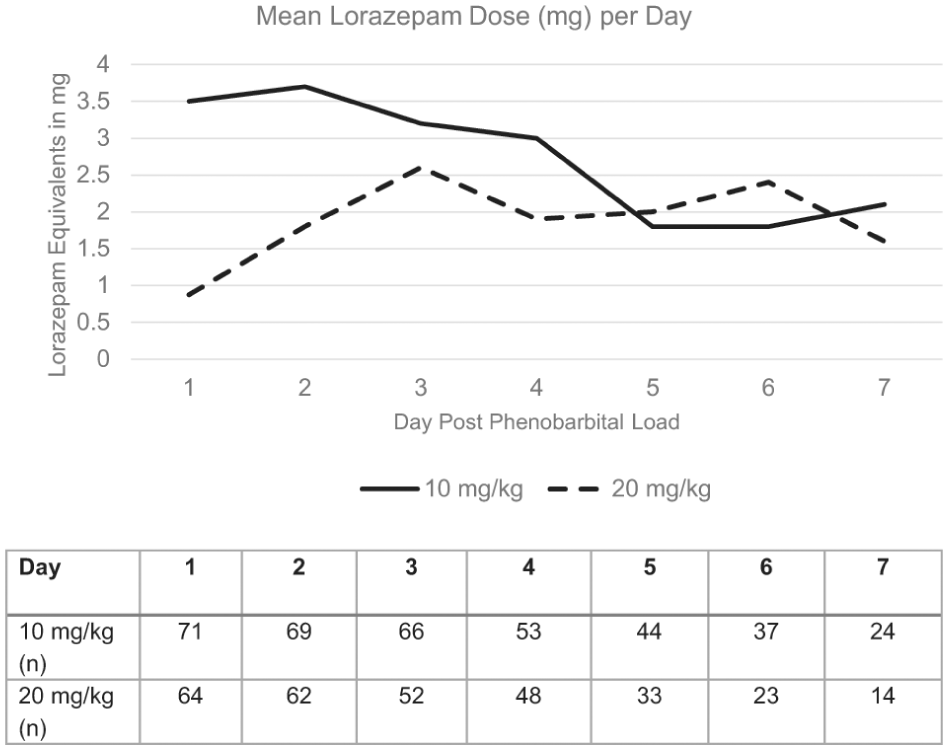
Mean lorazepam equivalents in mg used per day up to 7 days after the phenobarbital loading dose was given.
No significant differences were noted in new intubation rates (post-phenobarbital), between the 10-mg/kg and 20-mg/kg groups, respectively (5.9% [3/51] vs 10.2% [5/49], P = .483). Only 4 intubations occurred within 24 hours of phenobarbital administration. All 4 received a single phenobarbital dose, of which 2 (50%) were administered 20 mg/kg; 1 received benzodiazepines in the 24-hour period preceding intubation (15.8 mg lorazepam equivalents). Similarly, there were no significant differences in ICU length of stay, 4.5 ± 3.4 vs 3.9 ± 3.6 days (P = .411), or in total hospital length of stay, 8.3 ± 5.8 vs 6.6 ± 4.7 days (P = .075), between the 10-mg/kg and 20-mg/kg groups, respectively.
Discussion
Phenobarbital is an attractive option for the treatment of AWS because of its long half-life and effects on both GABA and glutamate. While several studies have demonstrated the effectiveness of phenobarbital using a front-loaded dosing strategy, the specific dose for these regimens is not well established.6,7 We evaluated a 10-mg/kg and a 20-mg/kg dosing regimen on the incidence of severe alcohol withdrawal and subsequent benzodiazepine therapy. After controlling for baseline differences between groups, there was no difference in the incidence of severe AWS. Benzodiazepine use, however, was significantly lower following a 20-mg/kg dose, particularly during the 48-hour period, post-dose. This corresponds to the long half-life of phenobarbital (ie, 79 h) and the possibility that serum concentrations were subtherapeutic at that timepoint for the 10-mg/kg group. 8
The relationship between serum concentrations and effectiveness for treating severe alcohol withdrawal are not well known. The therapeutic range for phenobarbital is 10 to 40 mcg/mL, but these are typically extrapolated from literature evaluating status epilepticus and seizures. 8 As expected, serum concentrations in our study were higher in the 20-mg/kg group, but there was no difference in serum concentrations in patients who did and did not exhibit withdrawal. This could be because the serum concentrations achieved in these groups (approximately 19 mcg/mL) were within the therapeutic range. Further research is necessary to determine the role of therapeutic drug monitoring, the correlation between serum concentrations and outcomes, and the most appropriate therapeutic range for alcohol withdrawal.
There are limited data comparing weight-based doses used as part of a front-loaded dosing strategy. One retrospective study explored a 6-mg/kg vs a 10-mg/kg loading dose of phenobarbital followed by a standardized oral taper. 9 Phenobarbital as needed for breakthrough symptoms could be provided. The primary endpoint was the incidence of AWS resistant to the initial protocolized phenobarbital load defined as the administration of additional phenobarbital outside the protocol-described dose (ie, load, taper, and as-needed dosages). There were 176 patients evaluated, and there was no difference in the incidence of withdrawal resistant to the initial phenobarbital protocolized dose (6 mg/kg group, 18.3% vs 10 mg/kg group, 19.7%, P = .82). Cumulative phenobarbital administration during the hospital admission was 10.3 (8.8-13.3) and 14 (12-16.7) mg for the 6- and 10-mg/kg groups, respectively (P < .001). Similar to our study, benzodiazepine use was lower in the higher phenobarbital dosing group, albeit not statistically significant (8.7% of patients vs 1.6%, P = .10).
Other studies have evaluated front-loaded strategies with phenobarbital for AWS. Rosenson et al 10 performed a randomized controlled trial comparing phenobarbital 10 mg/kg with placebo in the emergency department. In this trial, phenobarbital was associated with fewer ICU admissions and decreased total lorazepam required. There were no differences in adverse effects including the frequency of intubation, which was 2% with phenobarbital. Nisavic et al 11 reported the effectiveness of phenobarbital vs benzodiazepines in a retrospective study where dosing was categorized according to the balanced risk for AWS and respiratory compromise. With this protocol, patients could receive initial doses between 6 and 15 mg/kg administered as 3 separate doses, intramuscular, followed by an oral taper. No difference in efficacy or safety outcomes was noted. Nejad et al 12 reported their experiences with this protocol in a second retrospective study comparing phenobarbital with benzodiazepines. In this study, phenobarbital was associated with a reduction in AWS, adverse effects, and other adjunctive medication use. In our study, adjunctive medication use, particularly early administration of dexmedetomidine, was higher in the 10-mg/kg phenobarbital dosing group, which likely reflects worse AWS symptoms at baseline in this group. Last, Ammar et al 13 evaluated phenobarbital monotherapy in a cohort of surgical-trauma patients. Similar to the previous studies, the phenobarbital dose was categorized according to the balanced risk for AWS and respiratory compromise. The dosing range in this protocol was 10 to 15 mg/kg administered over 3 doses, either intravenously or intramuscular, followed by a taper. None of the patients developed severe AWS-related complications (ie, seizures, hallucinations, delirium); the frequency of intubation was 10%.
Adverse effects and particularly respiratory depression are a major concern with initiating phenobarbital, especially in patients who receive significant doses of benzodiazepines. We noted no difference in the frequency of mechanical ventilation between the 2 dosing groups with intubation rates that are consistent with other research reports. 7 Selection bias, though, did exist, as patients with cirrhosis or those with higher pre-phenobarbital benzodiazepine dosing requirements were more likely to receive a 10-mg/kg dose. This is important to consider when generalizing these results to other settings. Unfortunately, we were unable to evaluate other adverse effects such as hypotension or sedation (not requiring intubation). Further research is necessary.
There were several limitations that may have affected this study. First is the retrospective design, so confounding by indication and other limitations inherent to this design exist. There was no established protocol for the use of phenobarbital, nor for the dosing regimen, leaving the decision up to the individual clinician. It is possible that variability in practice existed. We noted a lower use of the 20-mg/kg dose in patients with cirrhosis or higher benzodiazepine exposure, so caution is warranted when generalizing these results. Next was the imbalance in baseline variables between the groups and the selection bias that existed with dose selection. While we attempted to control for these differences through regression analyses, only a randomized controlled trial can completely reconcile these concerns. Third, it is possible that other causes of agitation may have been present other than alcohol withdrawal. These would not be treated with phenobarbital. Fourth is the sample size and the possibility for type II error. Fifth is our patient population may not be generalizable to all hospital settings. Last is the use of CIWA-Ar scores (vs an alternative scoring system) as an indicator for benzodiazepine therapy. The CIWA-Ar scoring system has limitations, especially in the ICU, because of its subjective nature, poor symptom specificity, and need for a communicating patient in order to facilitate scoring. 14 The modified Minnesota Detoxification Scale (mMINDS), which has been validated in the ICU, may be a preferable scoring system.14,15
Conclusion and Relevance
There was no difference in the incidence of severe AWS between a 10-mg/kg and 20-mg/kg phenobarbital loading dose, but a 20-mg/kg dose was associated with less benzodiazepine use during the early withdrawal period. A front-loaded dosing strategy using 20 mg/kg of phenobarbital was not associated with an increased frequency of intubations. Further research is required in this area. Clinicians can consider this dosing approach upon weighing patient-specific risks and benefits with phenobarbital use for the treatment of AWS.
Footnotes
Appendix
Symptom-Based Benzodiazepine Protocol.
| Chlordiazepoxide protocol | |
|---|---|
| CIWA-Ar score | Dose |
| 5-7 | Chlordiazepoxide 25 mg po Q 6 h PRN |
| 8-14 | Chlordiazepoxide 50 mg po Q 6 h PRN |
| >14 | Chlordiazepoxide 75 mg po Q 6 h PRN |
| Lorazepam protocol | |
| CIWA-Ar score | Dose |
| 5-7 | Lorazepam 1 mg PO every 2 h PRN |
| 8-10 | Lorazepam 2 mg IV/po every 2 h PRN |
| 11-14 | Lorazepam 3 mg IV/po every 2 h PRN |
| 15-19 | Lorazepam 4 mg IV/po every 1 h PRN |
| >19 | Lorazepam 6 mg IV/po every 1 h PRN |
Abbreviation: CIWA-Ar, Clinical Institute Withdrawal Assessment for Alcohol–Revised.
Ethical Considerations
This study was approved by the HonorHealth Institutional Review Board (IRB-24-0102) on October 31, 2024.
Author Contributions
Pavan Sastry, PharmD, BS: Study design; Data collection; Interpretation of data; Manuscript creation; Approval of final version.
Jessica Hasty, PharmD, BCCCP, BCEMP: Study design; Interpretation of data; Critical revisions to manuscript; Approval of final version.
Jane Litwak, PharmD, BCCCP: Study design; Interpretation of data; Critical revisions to manuscript; Approval of final version.
Victor Zach, MD: Study conception; Interpretation of data; Critical revisions to manuscript; Approval of final version.
Joseph F. Sucher, MD, FACS: Study conception; Interpretation of data; Critical revisions to manuscript; Approval of final version.
Jeffrey F. Barletta, PharmD, FCCM, FCCP: Study conception; Study design; Data analysis; Interpretation of data; Manuscript creation; Approval of final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jeffrey F. Barletta is a consultant for Wolters Kluwer. The remaining authors have no conflicting interests to report.
Data Availability Statement
Research data are not shared.
Use of Artificial Intelligence
No AI tools were used in the drafting of this manuscript, tables, or figures.