
Abstract
Objective:
To evaluate the efficacy and safety of oral proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors in patients with hypercholesterolemia and assess their potential as a convenient alternative to injectable therapies.
Data Sources:
PubMed, Embase, Scopus, and CENTRAL were searched from inception to May 10th, 2026, using terms related to oral PCSK9 inhibitors and hypercholesterolemia. The study was registered with PROSPERO (CRD420261329028).
Study Selection and Data Extraction:
Randomized controlled trials (RCTs) comparing oral PCSK9 inhibitors with placebo in adults receiving background lipid-lowering therapy were included. Two reviewers independently screened studies and extracted data on an Excel sheet.
Data Synthesis:
Five RCTs were analyzed. Oral PCSK9 inhibitors significantly reduced LDL cholesterol (mean difference [MD] −52.15 mg/dL; 95% CI −59.42 to −44.87), apolipoprotein B (MD −42.85 mg/dL; 95% CI −49.52 to −36.18), and lipoprotein(a) (MD −35.11 mg/dL; 95% CI −52.86 to −17.36) compared with placebo. Significant reductions were also observed in triglycerides and total cholesterol. Safety outcomes were comparable to placebo, with no increased risk of adverse events (risk ratio [RR] 1.04; 95% CI 0.98-1.09) or serious adverse events. Subgroup analyses indicated enhanced efficacy with enlicitide and specific dosing regimens.
Relevance to Patient Care and Clinical Practice:
Oral PCSK9 inhibitors address major barriers inherent to injectable biologics. By eliminating needle-related anxiety, injection-site reactions, and the logistical burdens of cold-chain storage, these agents may significantly improve patient adherence and satisfaction. This transition to a convenient oral regimen facilitates integration into standard care, potentially expanding access for patients reluctant to maintain long-term injectable therapy.
Conclusions:
Oral PCSK9 inhibitors significantly improve atherogenic lipid profiles and are well tolerated. They represent a promising and convenient alternative to injectable PCSK9 inhibitors for managing hypercholesterolemia.
Keywords
Introduction
Hypercholesterolemia is a significant modifiable risk factor, alongside other contributors, for atherosclerotic cardiovascular disease (ASCVD), which continues to be a leading global cause of morbidity and mortality. Recent American College of Cardiology (ACC)/American Heart Association (AHA) guidelines have identified low-density lipoprotein cholesterol (LDL-C) levels as the primary factor for increased ASCVD risk and a key target for prevention strategies. 1 According to the World Health Organization, an estimate of 17.9 million deaths are reported globally among individuals with cardiovascular diseases (CVDs) each year. 2 Moreover, the Global Burden of Disease Study 2023 also reports 437 million CVD disability-adjusted life years (DALYs) and deaths occurring worldwide. 3 Elevated LDL-C drives atherosclerosis by depositing cholesterol in arteries, increasing the risk of heart attack or stroke, and leaving many patients worldwide with inadequately controlled levels despite advances in lipid-lowering therapies. 4
Statins remain the cornerstone of pharmacotherapy for hypercholesterolemia because of their proven efficacy in reducing LDL-C levels and lowering cardiovascular risk. 5 However, concerns over the potential for serious adverse effects in vulnerable populations limit their efficacy in clinical practice. In a clinical trial by the Cholesterol Treatment Trialists’ Collaboration, patients with diabetes or previous vascular disease undergoing statin therapy reported a 7% increase in muscle pain in the first year. 6 Some patients require additional lipid-lowering therapy to reach LDL-C targets, while others cannot tolerate statins or experience adverse effects that limit dosing. 7
PCSK9 promotes degradation of hepatic LDL receptors, reducing LDL-C clearance. Inhibiting PCSK9 increases receptor recycling, enhancing LDL-C removal and significantly lowering circulating cholesterol. 8 Consequently, PCSK9 inhibitors have emerged as a crucial addition to contemporary lipid-lowering therapy, specifically for high-cardiovascular-risk patients who fail to meet the standard LDL-C levels with conventional treatments. Recent ACC/AHA guideline recommendations emphasize intensive LDL-C lowering, targeting LDL-C levels <55 mg/dL in very high-risk ASCVD patients, and recommend adding ezetimibe and/or PCSK9 inhibitors when treatment goals are not achieved with maximally tolerated statin therapy. 9 Large randomized trials have demonstrated the benefits of PCSK9 inhibitors. The FOURIER trial showed that evolocumab reduced LDL-C by 59% and lowered major cardiovascular events in patients with ASCVD. 10 Similarly, the ODYSSEY OUTCOMES trial found that alirocumab significantly reduced recurrent ischemic cardiovascular events after acute coronary syndrome, with a 15% relative risk reduction in major adverse cardiovascular events (9.5% vs 11.1%; hazard ratio 0.85, 95% CI 0.78-0.93; P < 0.001). 11 PCSK9 inhibitors are currently injectable and highly effective, but administration, cost, storage, and access can limit use. 12 As a result, there is growing interest in the evolution of orally administered PCSK9 inhibitors that might provide considerable convenience and possibly ameliorate treatment utilization and adherence.
Recently, several randomized controlled trials (RCTs) have evaluated the efficacy and safety of oral PCSK9 inhibitors in patients with hypercholesterolemia. Early trials by Koren et al, followed by subsequent studies in 2025 and a trial by Ballantyne et al, demonstrated promising reductions in LDL-C and other atherogenic lipid parameters with oral PCSK9 inhibition. Our previous meta-analysis synthesized data from the initial 3 trials and provided preliminary evidence supporting the efficacy and safety of this emerging drug class 13 ; however, it was limited by the small number of available studies and a relatively modest pooled sample size. Since then, 2 additional RCTs have been published, expanding the available evidence base. Therefore, an updated and more comprehensive evaluation is warranted. In this systematic review and meta-analysis, we incorporate these newly published trials to increase the overall sample size and strengthen the robustness of the evidence. We also perform subgroup and sensitivity analyses to explore potential sources of heterogeneity and assess the consistency of treatment effects. Collectively, this updated analysis provides a more comprehensive assessment of the therapeutic potential of oral PCSK9 inhibitors, which may represent a convenient alternative to injectable therapies and improve treatment adherence among patients at high cardiovascular risk.
Methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria, and a PRISMA checklist is provided in Supplemental Table 1. Our study is registered with PROSPERO CRD420261329028. Available from https://www.crd.york.ac.uk/PROSPERO/view/CRD420261329028
Search Strategy and Data Sources
This meta-analysis was conducted according to the PRISMA guidelines. 14 An extensive literature search on PubMed (MEDLINE), Scopus, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) was conducted, from inception till May 10th, 2026. Search Strategies incorporated a combination of MeSH terms and keywords such as (“hypercholesterolemia” OR “hyperlipidemia” OR “dyslipidemia” OR “atherosclerotic cardiovascular disease” OR “ASCVD”) AND (“oral PCSK9 inhibitor” OR “proprotein convertase subtilisin/kexin type 9” OR “NNC0385-0434” OR “MK-0616” OR “AZD0780” OR “enlicitide”). The detailed search strategy is provided in Supplemental Table 2. In addition, we performed manual searches of reference lists from all eligible studies to identify potentially relevant studies.
Selection of Studies and Eligibility Criteria
All retrieved records were imported into Rayyan, and duplicates were removed. 15 Two reviewers independently screened titles and abstracts, followed by full-text assessment of potentially eligible studies. Any disagreement regarding interpretation and individual study inclusion was resolved by discussion before the final analysis. The study-selection process is summarized in the PRISMA flowchart (Figure 1).
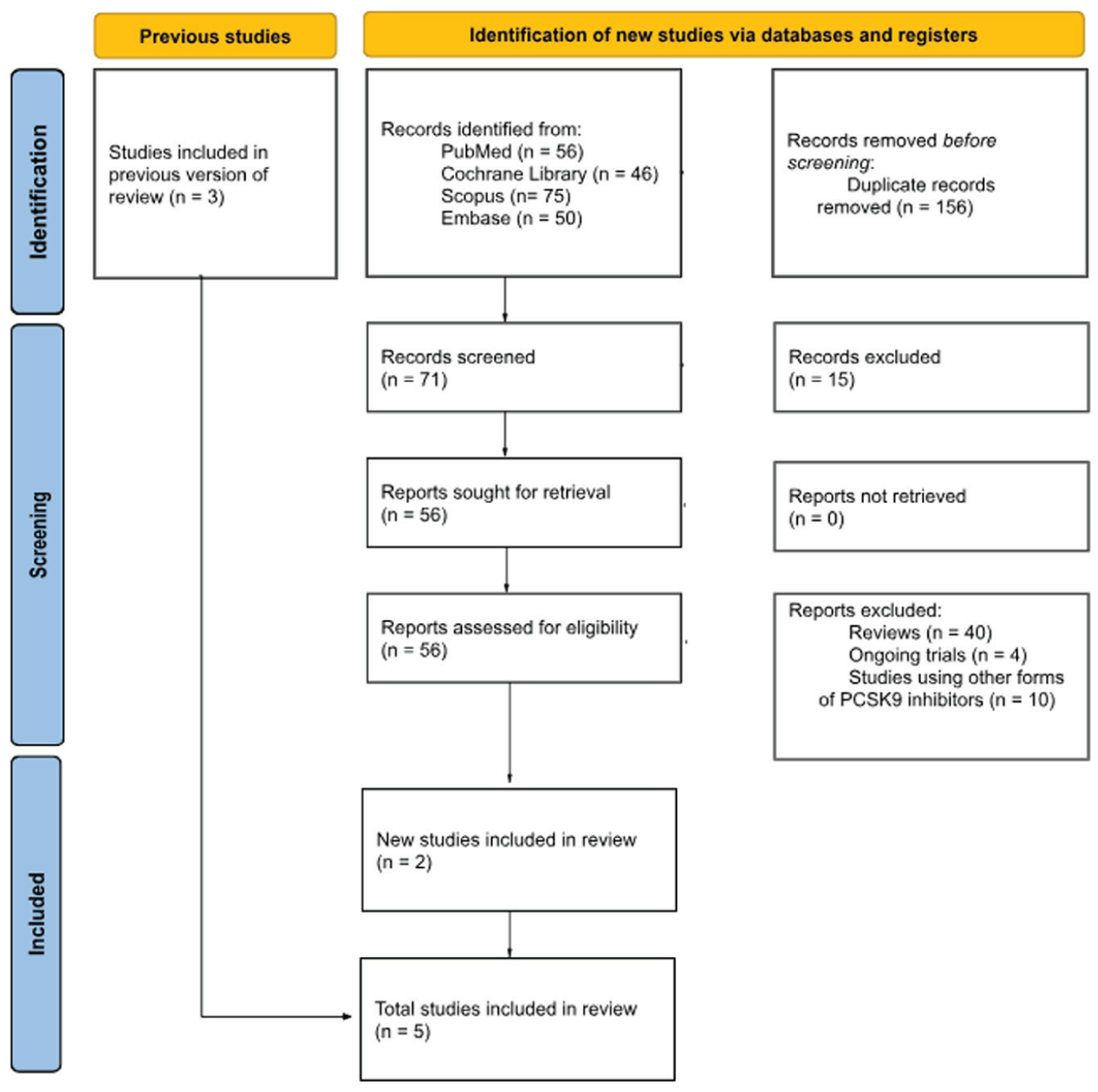
PRISMA flow diagram of study selection.
Studies using a structured Population, Intervention, Comparator, Outcomes, Study type (PICOS) framework were included. Adult patients (18 years of age or older) with dyslipidemia or hypercholesterolemia who were receiving steady background lipid-lowering treatment made up the eligible population. For individuals who are intolerant to statins, this background therapy may consist of nonstatin medication and/or a maximum tolerated statin. Patients having myocardial infarction, stroke, acute coronary syndrome, homozygous familial hypercholesterolemia, significant renal impairment (estimated glomerular filtration rate [eGFR] <30-45 mL/min), or triglyceride levels ≥400 mg/dL were not included in the study. The administration of any dose of an oral PCSK9 inhibitor once daily for 8 to 24 weeks was the intervention of interest. A placebo given once daily in addition to the same background therapy served as the comparator.
Only RCTs that matched all components of this eligibility framework were included. Nonrandomized studies, as well as commentaries, editorials, and case reports, were excluded from the analysis. Language was not a barrier while shortlisting studies.
Data Extraction
Data extraction was carried out by 2 independent reviewers (S.I.H. and A.A.J.) from the included articles, and a Microsoft Excel spreadsheet was created to compile baseline characteristics and outcome data extracted from the included RCTs. Important baseline characteristics across studies included age, sex, mean LDL-C, and background statin therapy along with the basic extracted information like study identifiers (author, year, trial name) and study design.
Outcomes
The primary efficacy outcomes included lipid parameters including LDL cholesterol, total cholesterol, triglycerides, apolipoprotein B, lipoprotein(a), very-low-density lipoprotein (VLDL), high-density lipoprotein (HDL), and Apo-CIII. The secondary safety outcomes extracted comprised adverse events and serious adverse events. For this updated meta-analysis, two additional safety outcomes were included: adverse events leading to discontinuation and adverse events leading to death. By capturing both the severity (mortality) and tolerability (discontinuation) of treatment-related adverse events, these endpoints offer a more thorough evaluation of the safety profile of oral PCSK9 inhibitors.
Statistical analysis
All meta-analyses were conducted using the meta package in R (version 4.4.2). Results were presented using forest plots for visual synthesis of findings. For the continuous outcomes, mean differences (MD) with corresponding 95% CIs were calculated. For the dichotomous outcomes, the number of events were used to calculate a pooled effect estimate (risk ratios [RR] with 95% CIs). Random-effects models were employed to estimate the pooled effect size to account for different statistical assumptions and enhance the interpretation. For heterogeneity, a random-effects model based on the Restricted Maximum Likelihood (REML) approach was used. The Chi-square test and Higgins’ I² statistic were used to measure the degree of heterogeneity; values were interpreted as low (<25%), moderate (25%-75%), or high (>75%).
Since the publication of the previous meta-analysis, additional RCTs have become available, allowing for updated quantitative synthesis. The inclusion of these 2 new trials allowed us to conduct prespecified subgroup analyses and sensitivity analyses to more rigorously investigate possible sources of heterogeneity than would otherwise have been possible. When data were available for additional subgroup analyses (for all primary outcomes), we investigated whether or not drug type (NNC0385-0434 vs AZD0780 vs enlicitide [MK-0616]) or dosage (10-15 mg vs 20 mg vs 30-40 mg) influenced effect estimates. We conducted leave-one-out sensitivity analysis of the effect estimates to assess the robustness of the overall results. Data were considered statistically significant if the P-value was ≤0.05 and if publication bias was evaluated by visually examining funnel plots.
Long-term follow-up outcomes were reported in 2 included trials (Navar 2026 and Ballantyne 2025) at 52 weeks. These data were not included in the quantitative meta-analysis because the study populations overlapped with cohorts already included at earlier follow-up time points, which could result in double counting of participants. In accordance with methodological guidance, these long-term outcomes were therefore summarized using a qualitative synthesis. Key efficacy outcomes, including percentage change in LDL-C, were descriptively reported to evaluate the durability of treatment effects with oral PCSK9 inhibitors.
Assessment of Risk of Bias
The risk of bias for each included study was assessed independently by a single author (F.Q.) using the Cochrane Risk of Bias tool (RoB 2) for RCTs. 16 The tool evaluates bias across 5 domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in measurement of the outcome; and (5) bias in selection of the reported result. Each domain was judged as having a “low risk of bias,” “some concerns,” or a “high risk of bias.” An overall risk-of-bias judgment for each study was determined based on the judgments across all domains.
Certainty of Evidence: GRADE Assessment
We used a GRADE (Grading of Recommendations Assessment, Development, and Evaluation) tool to assess the overall quality and strength of evidence for each primary and secondary outcome. 17
Results
Study Identification
A total of 227 articles were identified through various database searches. After removing 156 duplicate records, 71 articles remained for screening. During title and abstract screening, records were excluded if they contained a title or abstract that indicated an obviously ineligible study design type, indicated a population or intervention not relevant to the research question, and if they did not contain original outcome data relevant to the research question. Specifically, of the 15 excluded records at this stage, 9 were excluded because their title referred to either a cohort or a cross-sectional design; the remaining 6 were excluded because their abstract specified a comparator that was not relevant to the research question or did not contain relevant clinical outcome data. The full texts of the remaining 56 articles were assessed for eligibility; 54 were excluded for not meeting the inclusion criteria. Ultimately, 2 new RCTs were included in the final analysis. Combined with the 3 studies from the prior meta-analysis, this resulted in a total of 5 studies.18-22 The PRISMA flowchart is given in Figure 1.
Characteristics of Studies
The 5 included studies were all RCTs evaluating an oral PCSK9 inhibitor against a placebo in patients with established CVD or those at elevated cardiovascular risk. A detailed overview of the study designs and patient characteristics is presented in Table 1. The clinical and demographic data of both groups were similar prior to any intervention in each of the studies. The majority of participants were male, with mean ages ranging from 61 to 65. The mean body mass index (BMI) for all study groups was also similar at 29 to 30 kg/m², classified as overweight to obese. All groups had statistically similar baseline LDL-C levels, within the inclusion criteria for each study, and there were a high percentage of individuals with a prior diagnosis of type 2 diabetes mellitus. Like the baseline LDL-C levels, baseline triglyceride and total cholesterol levels were similar between the two groups at study initiation. Across the included trials, all participants were receiving stable background lipid-lowering therapy, most commonly statins of varying intensity (low, moderate, or high intensity). A proportion of patients were receiving additional nonstatin therapy, primarily ezetimibe. In addition, some trials included individuals who were statin-intolerant or receiving maximally tolerated statin therapy. While the distribution of these therapies was generally balanced between intervention and control groups within individual trials, the type and intensity of background therapy varied across studies.
Key Baseline and Study Characteristics.
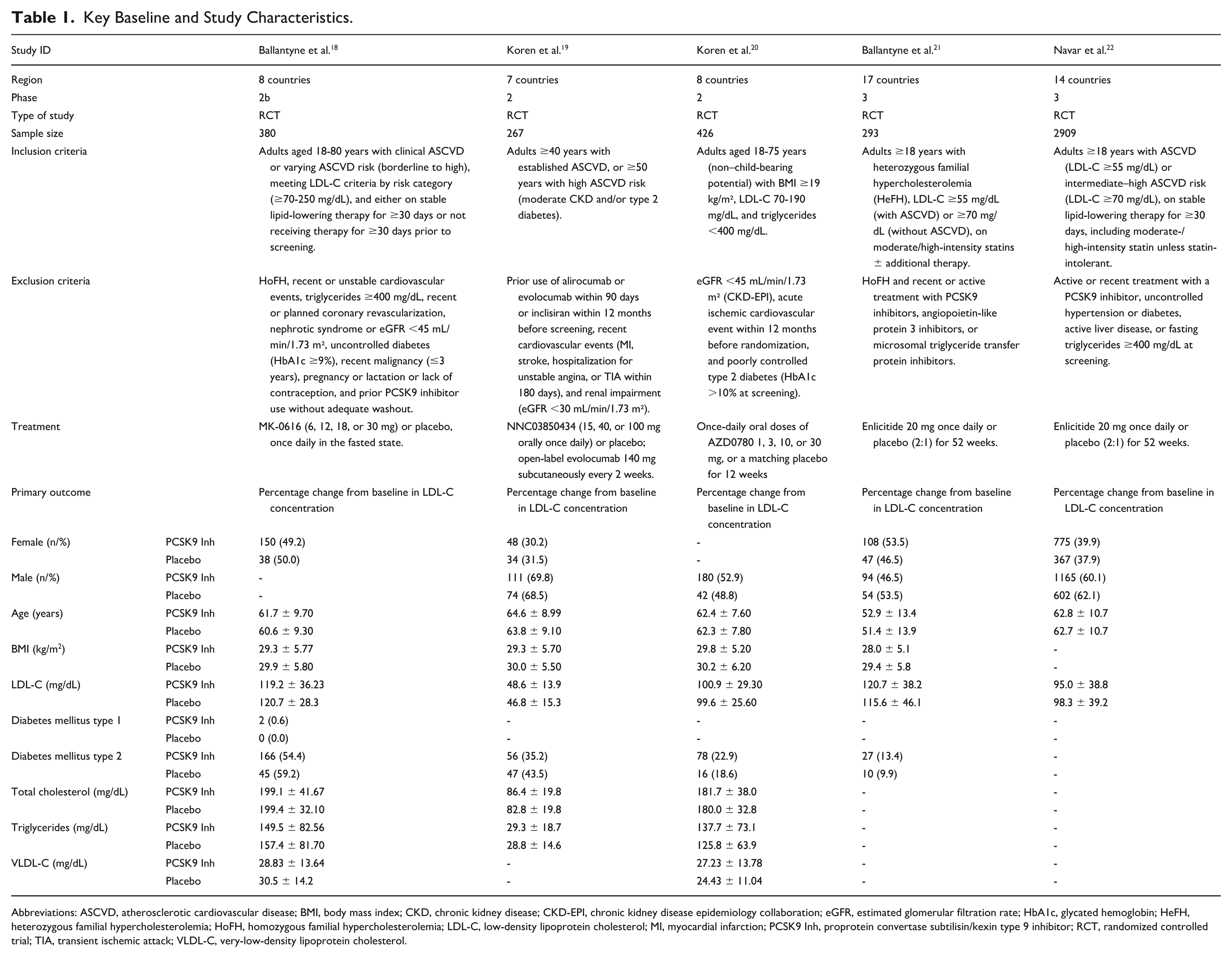
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; BMI, body mass index; CKD, chronic kidney disease; CKD-EPI, chronic kidney disease epidemiology collaboration; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; PCSK9 Inh, proprotein convertase subtilisin/kexin type 9 inhibitor; RCT, randomized controlled trial; TIA, transient ischemic attack; VLDL-C, very-low-density lipoprotein cholesterol.
Risk of Bias Assessment
The risk of bias assessment was conducted using the Cochrane Risk of Bias 2.0 tool for RCTs. Among the 5 included studies, all were judged to have an overall low risk of bias (Koren 2024, Koren 2025, Ballantyne 2023, Ballantyne 2025, and Navar 2026). Across all studies, the randomization process, deviations from intended interventions, outcome measurement, missing outcome data, and selection of reported results were well conducted with no major concerns identified. A summary of the risk of bias assessment is presented in Figure 2.
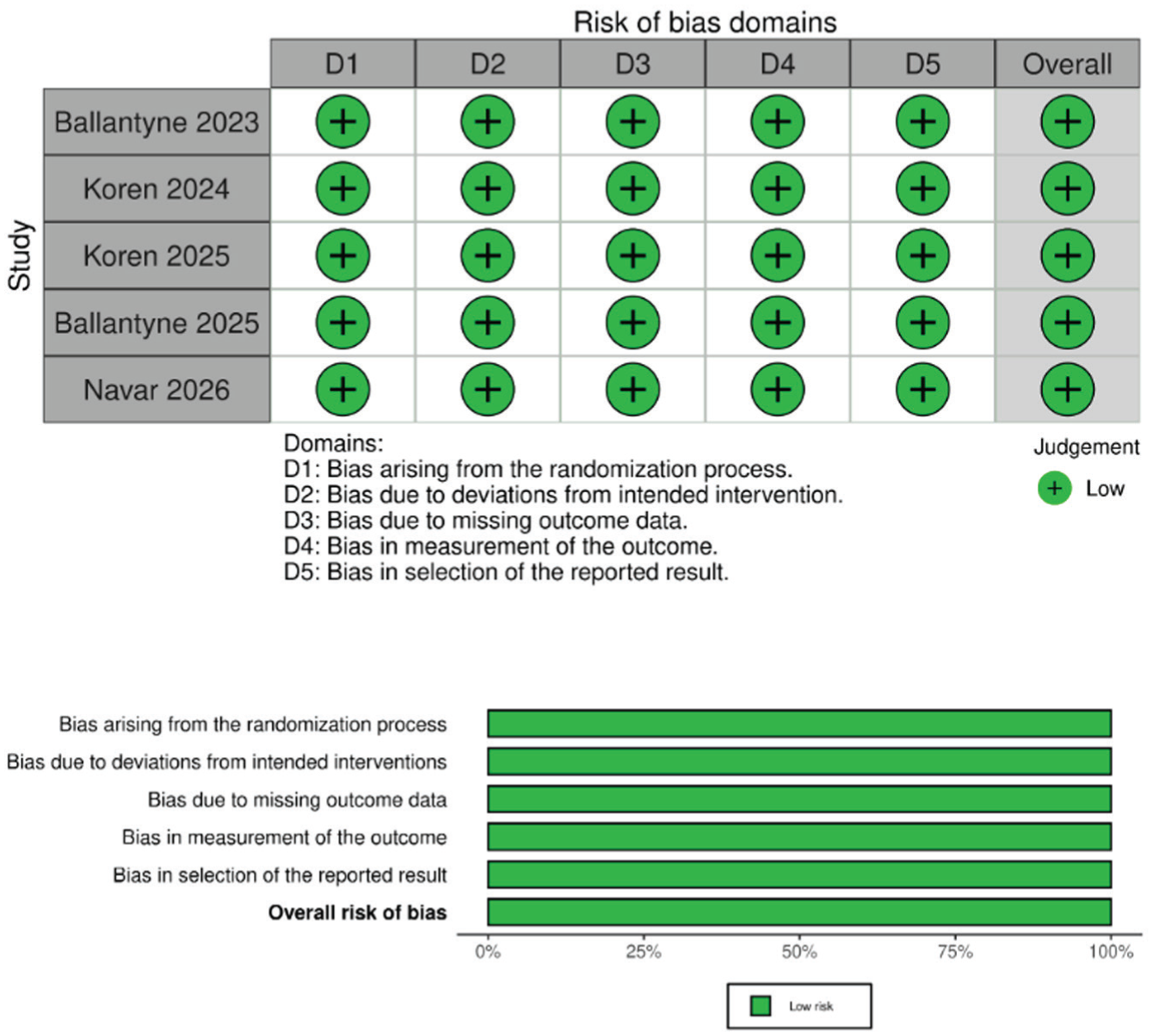
Risk-of-bias assessment of included studies.
Grade Assessment (Evidence of Certainty)
Supplemental Table 3 shows that the certainty of evidence was moderate for LDL cholesterol, total cholesterol, apolipoprotein B, lipoprotein(a), and serious adverse events, mainly due to heterogeneity or imprecision. Evidence was high for triglycerides and overall adverse events. PCSK9 inhibitors significantly reduced LDL-C (MD −52.15 mg/dL), total cholesterol (MD −25.22 mg/dL), triglycerides (MD −6.56 mg/dL), apolipoprotein B (MD −42.85 mg/dL), and lipoprotein(a) (MD −35.11 mg/dL) compared with control. There was no significant difference in adverse events (RR 1.04, 95% CI: 0.98-1.09) or serious adverse events (RR 0.84, 95% CI: 0.69-1.04) between groups.
Analytical Evaluation of Efficacy Outcomes
Change in LDL-C
Eight comparisons from 5 studies (PCSK9 inhibitors: n = 2457; control: n = 1451) were included for the outcome of change in LDL-C. The 8 comparisons reflect multiple intervention arms (different dosing regimens) evaluated within individual trials against a shared control group. Pooled random-effects analysis showed that PCSK9 inhibitors significantly reduced LDL-C compared with control (MD −52.15 mg/dL; 95% CI: −59.42 to −44.87; P < 0.01) (Figure 3a). Across individual comparisons, LDL-C reductions ranged from −31.90 to −68.40 mg/dL across included trials.
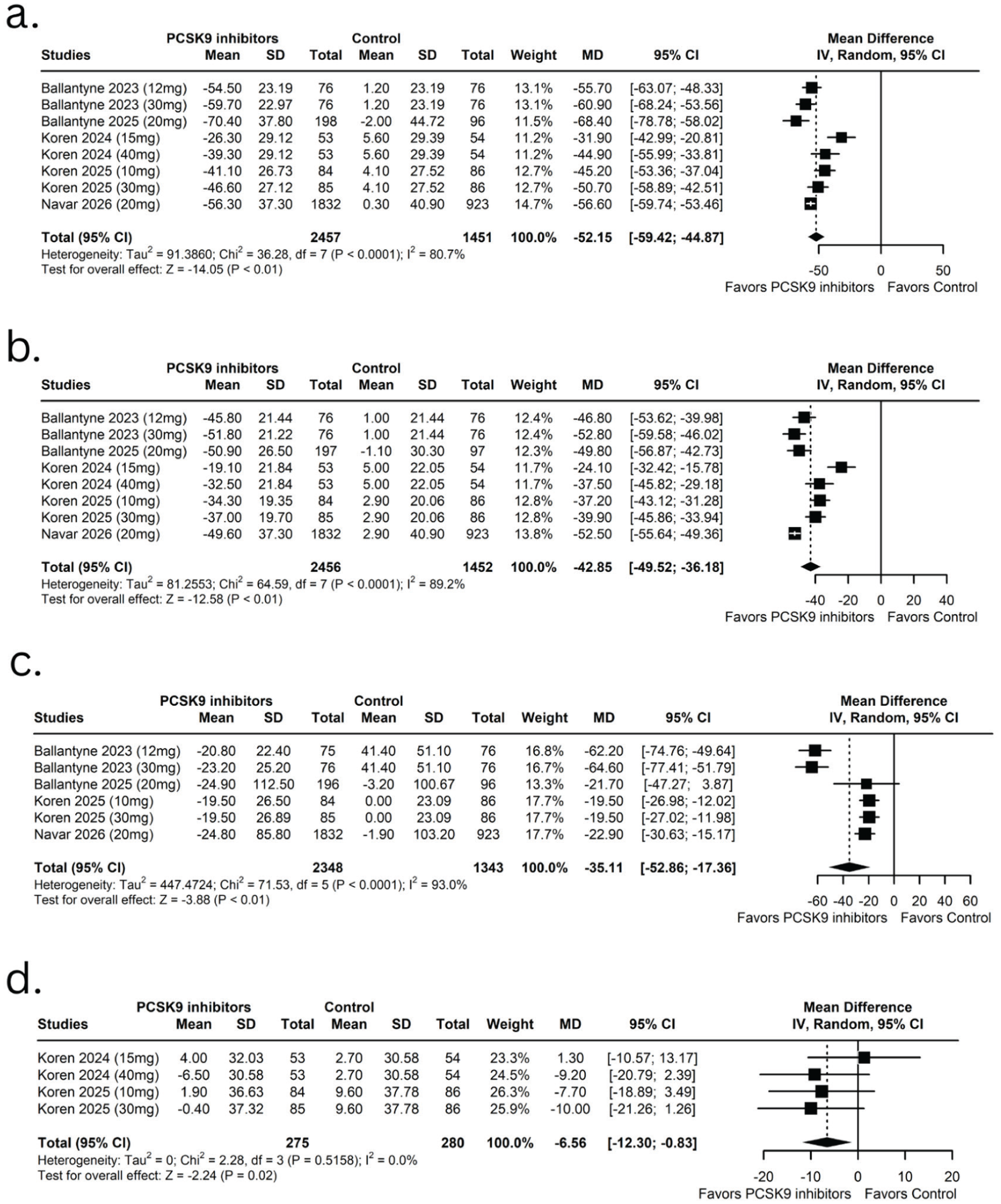
Forest plots of lipid-related efficacy outcomes with oral PCSK9 inhibitors vs control. (A) Change in LDL cholesterol; (B) change in apolipoprotein B; (C) change in lipoprotein(a); and (D) change in triglycerides.
Change in Apolipoprotein B
A total of 3908 adults from 5 RCTs (8 treatment arms) were included in the analysis (Figure 3b). Oral PCSK9 inhibitors significantly reduced ApoB levels compared with control (MD −42.85, 95% CI: −49.52 to −36.18; P < 0.01). However, substantial heterogeneity was observed across studies (I² = 89.2%). A subgroup analysis by type of oral PCSK9 inhibitor largely accounted for this heterogeneity (Supplemental Figure 18).
Change in Lipoprotein(a)
For lipoprotein(a), 6 comparisons from 4 studies (Ballantyne et al, Ballantyne et al, Koren et al, Navar et al) were included (PCSK9 inhibitors: n = 2348; control: n = 1343) (Figure 3c). Random-effects analysis showed a significant reduction in lipoprotein(a) with the use of PCSK9 inhibitors compared with control (MD −35.11; 95% CI: −52.86 to −17.36; P < 0.01), with substantial heterogeneity (I² = 93.0%). To explore this heterogeneity, a subgroup analysis based on the type of oral PCSK9 inhibitor was performed (Supplemental Figure 19).
Change in Triglycerides
The effect of oral PCSK9 inhibitors on triglyceride levels was modest but statistically significant in the pooled analysis of 2 trials (comprising 4 dosage arms). The overall MD was −6.56 mg/dL (95% CI: −12.30 to −0.83, P = 0.02). Notably, while the pooled result reached statistical significance, none of the individual study arms (Koren 2024; Koren 2025) demonstrated a statistically significant reduction in triglycerides when analyzed independently, as evidenced by their individual 95% CIs crossing the line of null effect (0). There was no evidence of heterogeneity among the studies (I² = 0.0%) (Figure 3d).
Change in Total Cholesterol
A consistent and statistically significant reduction in total cholesterol was observed with oral PCSK9 inhibitor treatment across 2 trials with 4 comparators (Koren et al; Koren et al). The pooled analysis demonstrated a MD of −25.22 mg/dL (95% CI: −30.90 to −19.54, P < 0.01), with moderate heterogeneity across the included trials (I² = 70.8%) (Figure 4a). Sensitivity analysis was performed to address this heterogeneity.
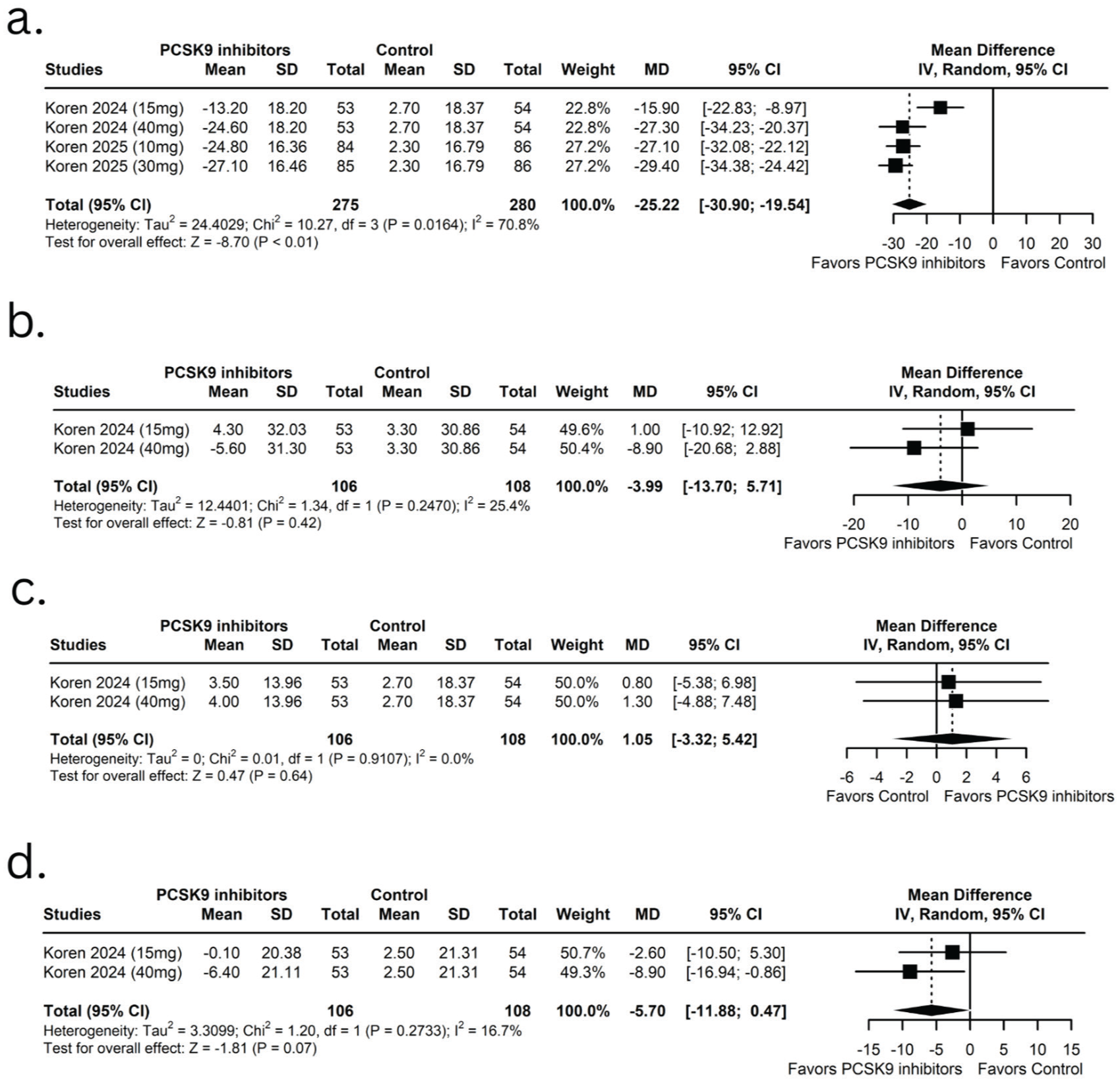
Forest plots of additional lipid profile outcomes with oral PCSK9 inhibitors vs placebo. (A) Change in total cholesterol; (B) change in very-low-density lipoprotein (VLDL); (C) change in high-density lipoprotein (HDL); and (D) change in Apo-CIII.
Change in VLDL
An oral PCSK9 inhibitor did not produce a statistically significant improvement in VLDL cholesterol. The pooled analysis of 1 trial (Koren 2024) contributing 2 dosage arms reported an average change of −3.99 mg/dL (95% CI: −13.70 to 5.71, P = 0.42) in VLDL cholesterol, with low heterogeneity across studies (I² = 25.4%) (Figure 4b).
Change in HDL
The effect of oral PCSK9 inhibitor on HDL was not statistically significant in the pooled analysis of 1 trial (Koren 2024) across 2 treatment arms. The overall MD was 1.05 mg/dL (95% CI: −3.32 to 5.42, P = 0.64), with no heterogeneity observed across the included trials (I² = 0.0%) (Figure 4c).
Change in Apo-CIII
The pooled analysis of 1 trial (Koren 2024), contributing 2 dosage arms, did not show a statistically significant effect of oral PCSK9 inhibitor on Apo-CIII; however, there is a trend toward reduction. The overall MD in Apo-CIII level between the two groups is −5.70 mg/dL (95% CI: −11.88 to 0.47, P = 0.07). The level of heterogeneity was low between trials (I² = 16.7%), suggesting a potential modest decrease in Apo-CIII associated with oral PCSK9 inhibitor treatment; however, this finding did not reach statistical significance (Figure 4d).
Safety Analysis
Risk of Adverse Events
The incidence of adverse events was comparable between oral PCSK9 inhibitor and placebo groups across 5 trials (Ballantyne 2023, Ballantyne 2025, Koren 2024, Koren 2025, and Navar 2026), contributing 8 analysis arms. The pooled analysis reports a RR for oral PCSK9 inhibitor vs placebo of 1:04 (95% CI: 0.98-1.09, P = 0.184), indicating no statistically significant difference in adverse event rate between treatment and control groups. Heterogeneity was negligible across the trials (I² = 0.0%) (Figure 5a).
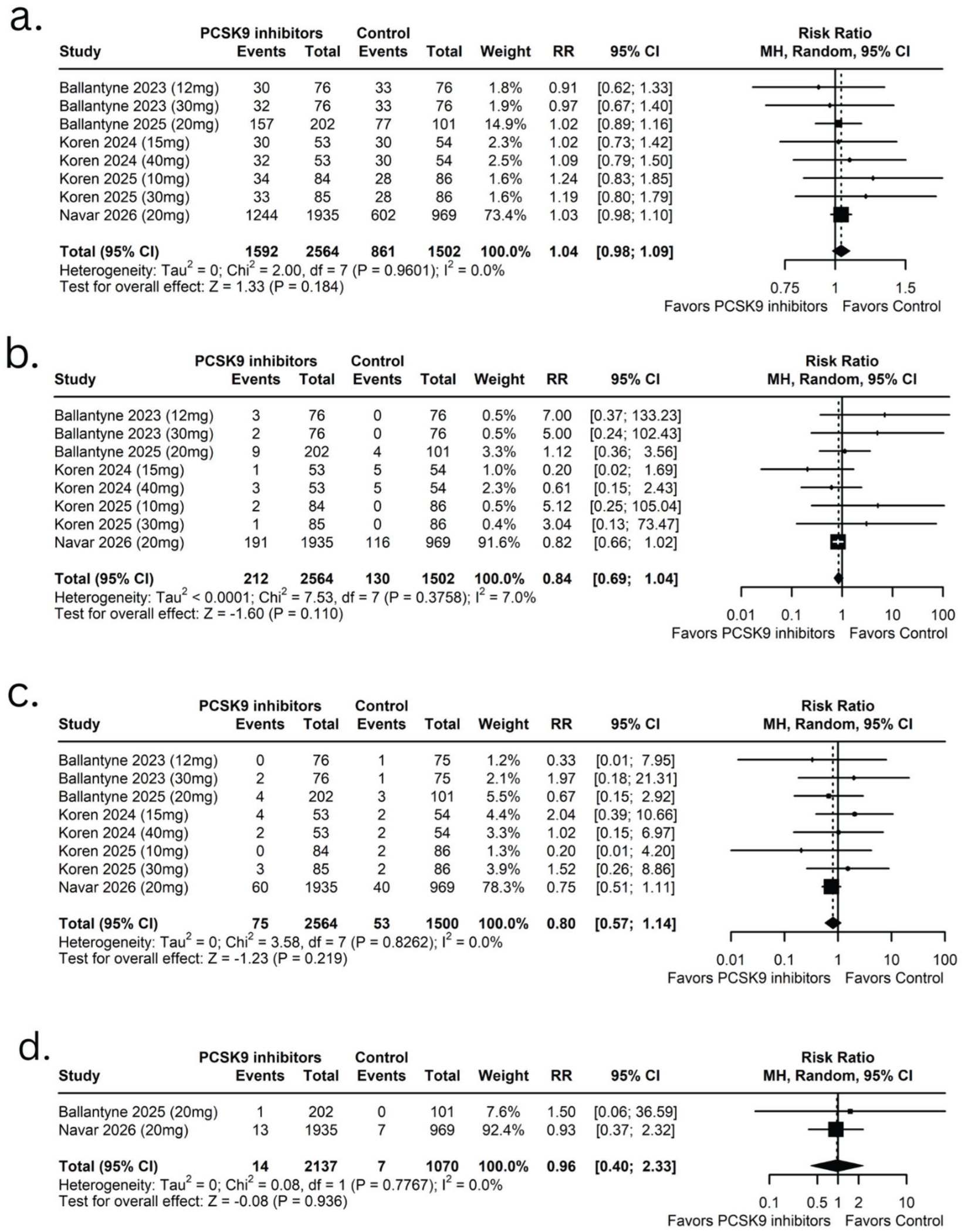
Forest plots of safety outcomes comparing oral PCSK9 inhibitors with placebo. (a) Risk of overall adverse events; (b) risk of serious adverse events; (c) adverse events leading to treatment discontinuation; and (d) adverse events leading to death.
Risk of Serious Adverse Events
The pooled analysis for serious adverse events included 5 trials (Ballantyne 2023, Ballantyne 2025, Koren 2024, Koren 2025, and Navar 2026). The RR was 0.84 (95% CI: 0.69-1.04, P = 0.110), indicating no statistically significant difference between groups. Heterogeneity was low across the trials (I² = 7.0%) (Figure 5b).
Adverse Events Leading to Discontinuation
There was a similar rate of adverse events that resulted in treatment discontinuation between the two groups, with no increased risk associated with treatment. The pooled analysis of 5 trials (Ballantyne 2023, Ballantyne 2025, Koren 2024, Koren 2025, and Navar 2026) demonstrated an RR of 0.80 (95% CI: 0.57-1.14, P = 0.219), indicating no statistically significant difference between groups. Heterogeneity was negligible across the trials (I² = 0.0%) (Figure 5c).
Adverse Events Leading to Death
The frequency of fatal events caused by administration of oral PCSK9 inhibitors and placebo was evaluated across 2 trials (Ballantyne 2025 and Navar 2026). The combined data showed an RR of 0.96 (95% CI: 0.40-2.33, P = 0.936), which means there was no statistically significant difference between groups. There was negligible heterogeneity across trial reports (I² = 0.0%) (Figure 5d).
Qualitative Synthesis of Long-Term Primary Outcomes
Change in LDL Cholesterol
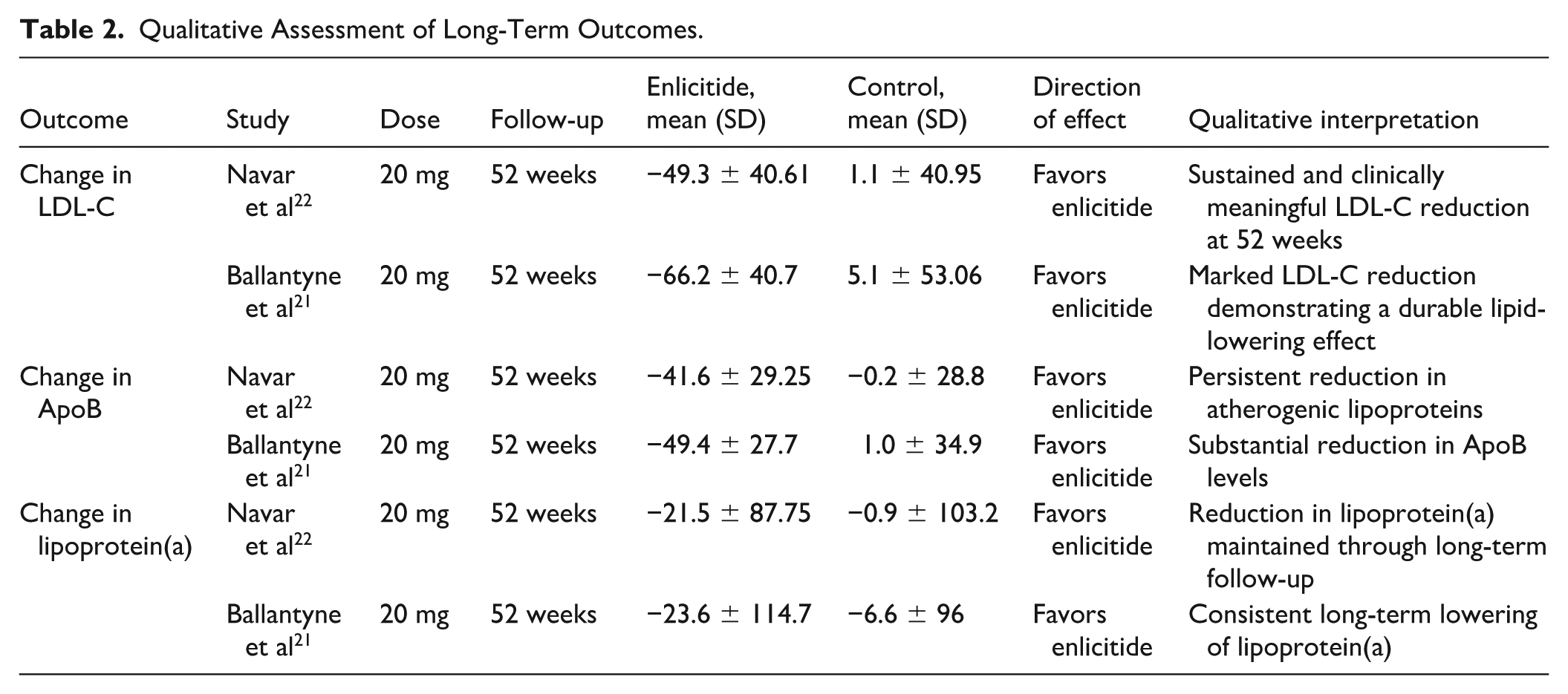
All RCTs conducted after the initial administration showed an overall reduction in LDL-C at the 52-week follow-up. The Navar 2026 (enlicitide) study demonstrated marked and durable lipid-lowering effects, with a change rate of −49.3% from baseline in the 20-mg-dose group, whereas the control group’s decline was only 1.1%. Given the significant decrease observed in the Ballantyne 2025 trial of enlicitide (−66.2% vs 5.1% in controls), we can conclude that there is continuing LDL-C decrease from long-term treatment. In all dose groups tested, the mean and direction of effect of oral PCSK9 inhibitor demonstrated a consistent reduction in LDL-C (Table 2).
Qualitative Assessment of Long-Term Outcomes.
Change in Apolipoprotein B
The results in relation to the reduction of ApoB in the Navar 2026 study were recollective and consistent with the LDL-C effects. At 52 weeks (20 mg), ApoB was lowered to −41.6% from baseline in the treatment group and to near zero in the control group (−0.2%). Similarly, in the treatment group 20 mg in the Ballantyne 2025 study, ApoB was reduced to −49.4% from the 1.0% change in controls. These reductions in ApoB are supportive of significant and long-lasting reduction in atherogenic lipoproteins, and that long-term treatment will provide the patient with a sustained therapeutic benefit. In both studies and dose groups, oral PCSK9 inhibitors had a consistent effect in the direction of ApoB reduction (Table 2).
Change in Lipoprotein(a)
A reduction in lipoprotein(a) was observed in the Navar 2026 study and maintained through long-term follow-up. After 52 weeks of treatment with 20 mg, the lipoprotein(a) was reduced by −21.5% compared to the control (−0.9%) (Navar 2026). In addition, Ballantyne’s 2025 research found that lipoprotein(a) was reduced by −23.6% in the treatment group compared to −6.6% in the control group. These findings indicate consistent long-term lowering of lipoprotein(a) with oral PCSK9 inhibition, though the variability in standard deviations suggests individual patient responses may differ. The direction of effect consistently favored oral PCSK9 inhibitors across both dose groups (Table 2).
Sensitivity Analysis
In order to identify possible reasons for the large variability seen in a variety of end points, we performed leave-one-out sensitivity analyses for change in total cholesterol, lipoprotein(a), LDL-C, and ApoB levels. The results of the leave-one-out analyses are illustrated in Supplemental Figures 1 to 8; the successive elimination of individual studies produced consistent results with minimal impact on both effect estimates and heterogeneity measures. These analyses demonstrate that the overall pooled estimates are robust and reliable, even though there were clinical or methodological differences among the various trials included in this analysis.
Notably, the only scenario in which heterogeneity was substantially reduced was observed for total cholesterol. Omitting the Koren 2024 (15 mg) dose group decreased heterogeneity from moderate levels to 0%, with a pooled MD of −28.05 mg/dL (95% CI −31.20 to −24.91) shown in Supplemental Figure 5.
Subgroup Analysis
Subgroup Analysis of Efficacy Outcomes
Stratified by Dose
Subgroup analysis stratified by dose demonstrated significant reductions in apolipoprotein B across all dose categories, with evidence of subgroup differences (P = 0.0168). The 10- to 15-mg subgroup included Koren 2024 evaluating NNC0385-0434 at 15 mg and Koren 2025 evaluating AZD0780 at 10 mg, alongside the 12-mg enlicitide (MK-0616) arm from Ballantyne 2023. The 30- to 40-mg subgroup included the 30-mg enlicitide (MK-0616) arm from Ballantyne 2023, 40-mg NNC0385-0434 from Koren 2024, and 30-mg AZD0780 from Koren 2025. The 20-mg subgroup consisted exclusively of enlicitide (MK-0616) evaluated in Ballantyne 2025 and Navar 2026.
The 20-mg subgroup demonstrated the greatest reduction in apolipoprotein B (MD −52.05 mg/dL; 95% CI −54.93 to −49.18), followed by the 30- to 40-mg subgroup (MD −43.52 mg/dL; 95% CI: −52.80 to −34.23) and the 10- to 15-mg subgroup (MD −36.22 mg/dL; 95% CI: −48.89 to −23.56). All subgroup effects remained statistically significant (P < 0.01) (Supplemental Figure 9).
Similarly, a subgroup analysis for LDL-C demonstrated significant reductions across all dose ranges, without significant subgroup differences (P = 0.17). The greatest LDL-C reduction was observed in the 20-mg subgroup (MD −61.42 mg/dL; 95% CI: −72.79 to −50.05), followed by the 30- to 40-mg subgroup (MD −52.82 mg/dL; 95% CI: −61.97 to −43.67) and the 10- to 15-mg subgroup (MD −44.78 mg/dL; 95% CI: −58.02 to −31.54) (Supplemental Figure 12).
Oral PCSK9 inhibitors reduced lipoprotein(a) levels overall vs control (MD: −35.11; 95% CI −52.86 to −17.36). Significant reduction was observed in the 20-mg subgroup (MD: −22.80; 95% CI −30.20 to −15.40; I² = 0%), while the 10- to 15-mg and 30- to 40-mg subgroups showed larger but nonsignificant effects with high heterogeneity. No significant subgroup differences were detected (P = 0.517) (Supplemental Figure 14).
For all other efficacy outcomes, subgroup differences by dose were not statistically significant. However, total cholesterol was significantly reduced overall (MD −25.22 mg/dL; 95% CI: −30.90 to −19.54), with significant reductions observed in both the 10- to 15-mg subgroup (MD −21.77 mg/dL; 95% CI: −32.73 to −10.81) and the 30- to 40-mg subgroup (MD −28.68 mg/dL; 95% CI: −32.73 to −24.64). For triglycerides, a significant reduction was observed only in the 30- to 40-mg subgroup (MD −9.61 mg/dL; 95% CI: −17.69 to −1.54; P = 0.02) (Supplemental Figures 15 and 16).
These findings are illustrated in Supplemental Figures 10 to 16.
Stratified by Type of Oral PCSK9 Inhibitor
Subgroup analysis by drug type revealed statistically significant differences for several efficacy outcomes, with enlicitide (MK-0616) consistently demonstrating the greatest lipid-lowering efficacy. For LDL-C reduction, enlicitide showed the largest effect (MD −58.82 mg/dL), followed by AZD0780 (MD −47.94 mg/dL) and NNC0385-0434 (MD −38.40 mg/dL), with a highly significant test for subgroup differences (P = 0.0005). Similarly, ApoB reduction varied significantly across drug types (P < 0.0001), with enlicitide again demonstrating the greatest reduction (MD −51.47 mg/dL), followed by AZD0780 (MD −38.54 mg/dL) and NNC0385-0434 (MD −30.80 mg/dL). Lipoprotein(a) reductions were also significantly different between drug types (P = 0.0477), with enlicitide showing greater efficacy (MD −43.63 mg/dL) than AZD0780 (MD −19.50 mg/dL).
For other efficacy measures, tests for subgroup differences were not statistically significant. While AZD0780 demonstrated a statistically significant change (MD −8.84 mg/dL, P = 0.03) in triglyceride levels, the NNC0385-0434 had no such demonstrated change (MD −4.03 mg/dL, P = 0.44). The test of subgroup difference for triglycerides was not statistically significant (P = 0.47). Refer to Supplemental Figures 17 through 21 for further details.
Subgroup Analysis of Safety Outcomes
Stratified by Dose
A subgroup analysis by dose revealed no significant differences in safety outcomes across dose categories. For adverse events, RRs were comparable across the 20-mg (RR 1.03, 95% CI: 0.98-1.09), 30 to 40 mg (RR 1.07, 95% CI: 0.87-1.32), and 10 to 15 mg (RR 1.04, 95% CI 0.84-1.29) dose groups, with no significant subgroup differences (P = 0.9362). Similarly, serious adverse events showed no dose-related differences (20 mg: RR 0.83; 30-40 mg: RR 1.24; 10-15 mg: RR 1.58; P = 0.7624), nor did adverse events leading to discontinuation (20 mg: RR 0.75; 30-40 mg: RR 1.40; 10-15 mg: RR 0.81; P = 0.5887). Based on these data, the overall safety profile of enlicitide will be the same for each dose investigated, and this can be visualized in Supplemental Figures 22 through 24.
Stratified by Type of Oral PCSK9 Inhibitor
Subgroup analysis by drug type revealed no significant differences in safety outcomes across the 3 oral PCSK9 inhibitors. There was a similar RR for all three groups (RR) regarding adverse events (enlicitide (RR = 1.03), AZD0780 (RR = 1.22), and NNC0385-0434 (RR = 1.05). The analysis did not reveal any statistically significant differences between subgroups regarding adverse events (P = 0.5124). Serious adverse events fit this same pattern with RRs of (enlicitide) RR = 0.91, (AZD0780) RR = 4.00, and (NNC0385-0434) RR = 0.44 (P = 0.1974); along with adverse events leading to discontinuation (enlicitide: RR 0.75; NNC0385-0434: RR 1.52; AZD0780: RR 0.82; P = 0.5782). These findings indicate that the safety profile remains consistent across different oral PCSK9 inhibitors, as illustrated in Supplemental Figures 25 to 27.
Publication Bias
Visual inspection of contour-enhanced funnel plots for lipid outcomes (LDL-C, ApoB, Lipoprotein(a), triglycerides, and total cholesterol) showed asymmetry, with a relative absence of small studies reporting null or opposite effects, suggesting possible small-study effects or heterogeneity. For lipoprotein(a) and triglycerides, the limited number of studies resulted in sparse plots outside the central funnel. For safety outcomes (overall adverse events, serious adverse events, and discontinuations), funnel plots also demonstrated some asymmetry. However, several studies fell within statistically significant regions, indicating that the asymmetry may partly reflect true effect differences rather than publication bias. The funnel plot for adverse events leading to death included very few studies, limiting meaningful assessment of publication bias (Supplemental Figures 28–36).
Discussion
This systematic review and meta-analysis synthesized evidence from 5 RCTs evaluating the efficacy and safety of oral PCSK9 inhibitors in patients with established CVD or elevated cardiovascular risk. By incorporating 2 newly published trials in addition to those included in earlier analyses, 13 the present study provides an updated assessment of this emerging class of lipid-lowering therapies. While all five trials contributed to the overall evidence base, the number of studies included in individual outcome analyses varied depending on data availability. Overall, the pooled findings demonstrate that oral PCSK9 inhibitors significantly reduce LDL cholesterol, total cholesterol, triglycerides, apolipoprotein B, and lipoprotein(a), while maintaining a safety profile comparable to that with placebo. These results reinforce the therapeutic potential of oral PCSK9 inhibition as a promising strategy for lipid management. PCSK9 inhibition currently occupies an important role in contemporary lipid management, particularly for patients at high or very high cardiovascular risk who fail to achieve LDL-C targets despite maximally tolerated statin therapy and ezetimibe. According to recent 2026 ACC/AHA guideline updates, PCSK9-targeted therapies are recommended as an adjunct for patients requiring intensive lipid lowering to achieve stringent LDL-C goals. The randomized trials included in the present analysis largely reflect this clinical context, as they enrolled patients with established ASCVD or elevated cardiovascular risk who were already receiving background lipid-lowering therapy. Therefore, the observed efficacy of oral PCSK9 inhibitors aligns with their anticipated role as add-on agents within current treatment algorithms.
A key finding of this analysis was the substantial reduction in LDL cholesterol associated with oral PCSK9 inhibitors. LDL-C is a well-established causal factor in the development of ASCVD, and intensive LDL-C lowering has consistently been associated with reductions in cardiovascular events.23,24 Across the included trials, LDL-C reductions ranged from approximately 49% to 66% from baseline in the treatment groups, highlighting the potent lipid-lowering capacity of oral PCSK9 inhibitors. These findings are consistent with results from early-phase clinical trials investigating oral PCSK9 agents such as enlicitide (MK-0616), which reported LDL-C reductions of approximately 60% when administered in combination with statin therapy.20,21 Emerging evidence from active-comparator trials further supports these findings. Notably, a recent trial by Catapano et al 25 demonstrated that oral PCSK9 inhibition achieves substantial lipid-lowering efficacy even when compared with established nonstatin therapies, reinforcing the robustness of its therapeutic effect. These findings also enhance the clinical relevance of oral PCSK9 inhibitors by demonstrating efficacy in treatment settings that more closely reflect real-world therapeutic decision-making, where patients are often managed with multiple nonstatin lipid-lowering agents. Moreover, the magnitude of LDL-C reduction observed in the present analysis appears comparable to that achieved with injectable monoclonal antibody PCSK9 inhibitors, including evolocumab and alirocumab, which have demonstrated LDL-C reductions of approximately 50% to 60% in large cardiovascular outcome trials such as FOURIER and ODYSSEY OUTCOMES.10,11 The comparable efficacy observed with oral agents may therefore represent an important advancement in lipid-lowering therapy, particularly for patients who prefer oral medications or have difficulty adhering to injectable treatments. Placing these findings within the broader landscape of PCSK9 inhibition is important. Prior network meta-analyses comparing injectable PCSK9 monoclonal antibodies with other lipid-lowering therapies have consistently demonstrated substantial LDL-C reductions and associated cardiovascular risk reduction, reinforcing the central role of intensive lipid lowering in ASCVD management. 26 These analyses suggest that the magnitude of LDL-C reduction achieved with PCSK9 inhibition is a key determinant of clinical benefit, supporting the “lower is better” paradigm. This observation is further supported by a recent network meta-analysis by Raone et al, 27 which demonstrated that greater LDL-C lowering across different PCSK9-targeting strategies was consistently associated with improved cardiovascular outcomes, reinforcing the importance of intensive lipid reduction in patients with established ASCVD. In this context, the degree of LDL-C reduction observed with oral PCSK9 inhibitors in the present analysis appears comparable to that reported with monoclonal antibodies, highlighting their potential clinical relevance. 28 Notably, the observed dose–response relationship for apolipoprotein B reduction further supports this concept, as greater reductions in atherogenic lipoprotein burden may translate into incremental cardiovascular risk reduction. However, it is important to recognize that improvements in lipid parameters do not necessarily translate proportionally into clinical benefit, particularly for a novel pharmacological class with distinct pharmacokinetic properties and adherence patterns. Therefore, in the absence of dedicated cardiovascular outcomes trials, the clinical impact of oral PCSK9 inhibitors on major adverse cardiovascular events remains uncertain and warrants cautious interpretation.
In addition to LDL-C reduction, the present meta-analysis demonstrated significant decreases in apolipoprotein B levels. ApoB represents the total burden of circulating atherogenic lipoproteins and is increasingly recognized as a strong predictor of cardiovascular risk because it reflects the number of atherogenic particles rather than cholesterol content alone. 29 The reductions in ApoB observed across the included trials parallel the decreases in LDL-C, supporting the mechanistic role of PCSK9 inhibition in enhancing hepatic LDL receptor recycling and promoting clearance of ApoB-containing lipoproteins from circulation. 30 These findings are consistent with prior investigations of both injectable and oral PCSK9 inhibitors, which have reported similar reductions in ApoB levels alongside LDL-C lowering.10,20 Another notable finding was the reduction in lipoprotein(a), a genetically determined lipoprotein that has emerged as an independent risk factor for ASCVD. 31 Current lipid-lowering therapies generally exert limited effects on lipoprotein(a), making reductions in this biomarker particularly noteworthy. The decreases observed in this analysis align with findings from prior PCSK9 inhibitor trials, where modest but significant reductions in lipoprotein(a) levels have been consistently reported.10,21 Although the precise mechanism underlying this effect remains incompletely understood, enhanced hepatic clearance of lipoprotein(a) particles through upregulated LDL receptor activity has been proposed as a contributing factor.32,33 The pooled analysis also demonstrated modest but statistically significant reductions in triglycerides and total cholesterol. While the triglyceride-lowering effect was relatively small compared with the reductions observed in LDL-C and ApoB, the consistent direction of effect across studies suggests that oral PCSK9 inhibitors may exert broader improvements in lipid metabolism. These findings are consistent with previous investigations of PCSK9 inhibition, which have reported modest reductions in triglycerides and total cholesterol but limited effects on HDL cholesterol.10,20 In line with these observations, the present analysis found no statistically significant changes in HDL cholesterol, VLDL cholesterol, or Apo-CIII levels. This pattern is consistent with the known mechanism of PCSK9 inhibition, which primarily enhances LDL receptor-mediated clearance of LDL particles rather than directly influencing HDL metabolism or triglyceride-rich lipoprotein pathways.
Safety outcomes in this analysis were reassuring, with no significant differences observed between treatment and placebo groups in terms of overall adverse events, serious adverse events, treatment discontinuations, or mortality. These findings are consistent with the favorable safety profile previously reported for injectable PCSK9 inhibitors in large randomized trials and long-term extension studies.10,11,34 The comparable safety observed across oral PCSK9 inhibitors further supports their potential as a well-tolerated long-term therapy for lipid management. Importantly, the absence of increased adverse events suggests that oral inhibition of PCSK9 does not introduce additional safety concerns beyond those already established for this therapeutic pathway. Subgroup analyses provided further insights into treatment effects. A statistically significant dose-response relationship was observed for apolipoprotein B reduction, with higher doses producing greater lipid-lowering effects. This finding is biologically plausible and consistent with pharmacodynamic studies demonstrating dose-dependent inhibition of PCSK9 activity. 20 In addition, a subgroup analysis by drug type revealed that enlicitide (MK-0616) produced the largest reductions in LDL-C, ApoB, and lipoprotein(a) among the evaluated oral PCSK9 inhibitors. While these results suggest potential differences in efficacy between agents, they should be interpreted cautiously given variations in trial design, dosing strategies, and study populations. Sensitivity analyses further confirmed the robustness of the findings. Sequential exclusion of individual studies had minimal influence on pooled estimates for the major efficacy outcomes, indicating that the results were not driven by a single trial. The reduction in heterogeneity observed when 1 dose group was excluded in the total cholesterol analysis suggests that differences in dosing regimens may partially explain variability between studies.
The clinical implications of these findings are significant. Although injectable PCSK9 monoclonal antibodies have demonstrated substantial cardiovascular benefits, their real-world uptake has been limited by factors such as injection requirements, cost, and patient adherence challenges. 35 Oral PCSK9 inhibitors have the potential to overcome several of these barriers by providing a convenient and noninvasive treatment option that maintains potent lipid-lowering efficacy. Oral administration may improve treatment acceptability and adherence in some patients, potentially leading to more consistent long-term lipid control and reductions in cardiovascular risk. However, the presumed adherence advantage of oral PCSK9 inhibitors should be interpreted with caution. Long-acting injectable therapies such as inclisiran, which is administered twice yearly under healthcare supervision, may achieve high real-world adherence due to reduced dosing frequency and provider involvement. In this context, the relative benefit of oral agents in improving adherence compared with such long-acting therapies remains uncertain and may vary depending on patient preferences, healthcare access, and treatment settings. This study has several strengths. It includes only RCTs, ensuring a high level of methodological rigor. The overall risk of bias among the included studies was low, and the certainty of evidence was moderate to high for most outcomes according to the GRADE framework. Furthermore, comprehensive subgroup and sensitivity analyses were conducted to explore heterogeneity and confirm the stability of the results.
This meta-analysis has several limitations. First, the number of available RCTs evaluating oral PCSK9 inhibitors remains limited, reflecting the early stage of development of these agents and resulting in a relatively modest overall sample size. Second, most included studies primarily assessed surrogate lipid outcomes rather than long-term cardiovascular endpoints such as myocardial infarction or stroke; therefore, large cardiovascular outcomes trials are needed to confirm the clinical benefits of these therapies. Third, some clinical heterogeneity existed across studies, particularly regarding dosing regimens, treatment duration, and types of oral PCSK9 inhibitors evaluated. However, sensitivity analyses demonstrated stable pooled estimates, supporting the robustness of the findings. In addition, as multiple oral PCSK9 inhibitors were included, nominal dose categories are not directly comparable across agents due to differences in pharmacokinetics and potency. Therefore, dose-stratified findings should be interpreted cautiously and considered exploratory. Future studies using exposure-normalized metrics or agent-specific dose-response analyses are needed to better define this relationship. Another limitation is the inability to assess whether the efficacy of oral PCSK9 inhibitors varied according to background lipid-lowering therapy. Although baseline use and intensity of therapies such as statins and ezetimibe were reported across included trials, these were presented only as aggregate baseline characteristics and not stratified by treatment outcomes. Therefore, subgroup or meta-regression analyses based on background therapy were not feasible. Given that PCSK9 inhibition may act synergistically with statins through upregulation of LDL receptors, variations in baseline therapy could potentially influence treatment response. Despite these limitations, the present study provides an updated and comprehensive synthesis of randomized evidence on oral PCSK9 inhibitors using rigorous methodological approaches, including risk-of-bias and GRADE assessments.
Future research should focus on large cardiovascular outcomes trials to determine whether the lipid improvements observed with oral PCSK9 inhibitors translate into reductions in major adverse cardiovascular events. Additional studies examining long-term safety, comparative effectiveness with established lipid-lowering therapies, and real-world adherence will also be important for defining the role of these agents in clinical practice.
Relevance to Patient Care and Clinical Practice
The findings of this meta-analysis have direct implications for the management of hypercholesterolemia in clinical settings. Despite the established efficacy of injectable PCSK9 monoclonal antibodies, their real-world utility is often hampered by patient-related barriers, including needle phobia, injection-site reactions, and the logistical burden of cold-chain storage.26,27 Transitioning PCSK9 inhibition to an oral, once-daily formulation fundamentally alters the patient experience by providing a noninvasive alternative that fits seamlessly into existing multidrug regimens. This convenience is likely to enhance long-term adherence, a critical factor in chronic cardiovascular risk management, potentially leading to more consistent lipid control across broader patient populations. Furthermore, by removing the need for specialized storage and administration training, oral agents may reduce healthcare system overhead and expand access to intensive lipid-lowering therapy in primary care settings, where the burden of ASCVD management is highest.
Conclusions
This updated meta-analysis demonstrates that oral PCSK9 inhibitors significantly improve multiple atherogenic lipid parameters while maintaining a favorable safety profile. These findings support the growing body of evidence suggesting that oral PCSK9 inhibition may represent an effective and convenient therapeutic strategy for patients with CVD or elevated cardiovascular risk. Continued investigation through large-scale outcome trials will be essential to confirm their long-term cardiovascular benefits and guide their integration into future lipid-management strategies.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261455109 – Supplemental material for Efficacy and Safety of Oral PCSK9 Inhibitors in Adults With Hypercholesterolemia: An Updated Systematic Review and Meta-Analysis of RCTs
Supplemental material, sj-docx-1-aop-10.1177_10600280261455109 for Efficacy and Safety of Oral PCSK9 Inhibitors in Adults With Hypercholesterolemia: An Updated Systematic Review and Meta-Analysis of RCTs by Amna Amir Jalal, Shaikh Muhammad Daniyal, Zainab Arif, Erum Siddiqui, Syed Ibad Hussain, Fatima Qazi and Muhammad Burhan in Annals of Pharmacotherapy
Footnotes
Acknowledgements
None to declare. We confirm that there are no prior conference presentations, no additional contributors to acknowledge outside the listed authors, and no AI-based tools were used in the generation or editing of this manuscript.
Authors’ Note
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Author Contributions
Amna Amir Jalal: Conceptualization, Methodology, Data curation, Formal analysis, Investigation, Writing – original draft, Visualization, Supervision. Shaikh Muhammad Daniyal: Data curation, Investigation, Validation, Writing – review & editing. Zainab Arif: Data curation, Investigation, Writing – review & editing. Erum Siddiqui: Data curation, Validation, Writing – review & editing. Syed Ibad Hussain: Formal analysis, Software, Visualization, Writing – review & editing. Fatima Qazi: Methodology, Validation, Writing – review & editing. Muhammad Burhan: Supervision, Methodology, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Writing Assistance Disclosure
No writing assistance was utilized in the production of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.