
Abstract
Background:
Critical illness-associated hyperglycemia is common and frequently results in new antidiabetic agent (ADA) initiation. However, new ADA use after an intensive care unit (ICU) hospitalization remains poorly characterized.
Objective:
To describe ADA prescribing in the 2 months after an ICU hospitalization in American adults (ADA-naïve prior to ICU admission) and the factors associated with this prescribing.
Methods:
This retrospective cohort study analyzed data from the US insurance claims database PharMetrics Plus for Academics (P+) for adults admitted to an ICU requiring mechanical ventilation during 2021 who were discharged directly to home. Patients with an ICU hospitalization in the prior 2 months or admitted with diabetic ketoacidosis or a hyperosmolar hyperglycemia state were excluded. The primary outcome was the proportion of ADA-naïve patients prescribed ≥1 ADA in the 2 months after discharge. Age, diabetes mellitus (DM) history, baseline Diabetes Comorbidity Index, Charlson Comorbidity Index, Hospital Frailty Risk Score, and medical (vs surgical) admission were entered into a multivariable logistic regression to identify factors associated with this prescribing.
Results:
Among the 28 798 817 patients in the P+ database in 2021, 2733 met study criteria. Among the 2346 (87.3%) who were ADA-naïve, 100 (4.2%) were prescribed ≥1 ADA in the 2 months after hospitalization. Most (88/100, 88%) were prescribed only 1 ADA; a biguanide (39%) or insulin (29%) was most common. A diagnosis of DM was similar 2 months before-and-after ICU hospitalization. Pre-existing DM (adjusted odds ratio [aOR] [95% CI]) was associated with greater new ADA prescribing (4.90 [2.91-8.19]), while age (0.99 [0.97-1.00]) and frailty (0.96 [0.93-0.99]) were associated with less new ADA prescribing.
Conclusions and Relevance:
Newly prescribed ADA therapy after an ICU hospitalization in critically ill adults who are discharged to a home setting is rare but more common in patients having a diagnosis of DM prior to ICU admission.
Introduction
Critical illness-associated hyperglycemia (CIAH) occurs in up to half of adults admitted to the intensive care unit (ICU) and may result in increased infections and greater mortality.1-4 The release of cortisol, norepinephrine, and growth hormone during critical illness leads to increased insulin resistance and reduced insulin secretion. 5 While preexisting diabetes mellitus (DM) remains an important risk for stress hyperglycemia in the ICU, 6 adults free of DM prior to their ICU admission who develop CIAH are twice as likely to develop new-onset DM after discharge. 7 Multiple treatment factors are known to exacerbate CIAH including total parenteral nutrition, vasopressors, glucocorticoids, and dextrose-containing IV admixtures.8,9
Current adult ICU practice guidelines recommend the protocolized initiation of insulin for patients having persistent serum glucose levels ≥180 mg/dL 10 and thus patients with CIAH are often started on insulin during their hospitalization. 11 With CIAH frequently persisting after ICU hospitalization,1,2,7 it is suspected that antidiabetic agents (ADAs) may be continued or newly initiated after discharge. However, ADA prescribing patterns in ICU survivors not taking an ADA before critical illness remains poorly characterized. Given the challenges of post-ICU medication reconciliation during transitions of care 12 and the potential safety concerns associated with unwarranted long-term ADA use (eg, hypoglycemia), 13 it is important to characterize new post-ICU hospitalization ADA use and the patient and ICU factors associated with it.
Better knowledge of post-ICU hospitalization ADA prescribing patterns in critically ill adults is essential to optimize the post-hospital care of ICU survivors and to inform future research on ADA reconciliation and prescribing practices. We therefore sought to characterize post-ICU ADA prescribing in a large US cohort of critically ill adults, without ADA use prior to ICU admission, and the factors associated with it. In an additional analysis to evaluate the impact of CIAH on patients already prescribed an ADA(s) before ICU admission, we compared ADA prescribing practices and documented DM diagnosis before-and-after the ICU hospitalization.
Methods
Study Design and Data Source
This retrospective cohort analysis used data from the IQVIA PharMetrics Plus for Academics (P+) database that is licensed to Northeastern University for the years 2017 to 2021. P+ is a comprehensive US health insurance claims database that includes data from various health plans, including patients fully insured by private insurance or covered by a Medicare Advantage plan, and provides a good representation of diverse Americans across different geographic regions. 14 The P+ database is mapped to the Observational Medical Outcomes Partnership common data model (OMOP CDM) and includes information on patient demographics and comorbidities, outpatient and inpatient visits, diagnoses, therapeutic interventions, and prescription drug fills and has widely been used in other large-scale pharmacoepidemiologic studies.15,16 Northeastern University waived Institutional Review Board (IRB) approval for all studies using P+ given the data are retrospective and deidentified (IRB # 24-03-24). The reporting for this study adheres to the STrengthening and Reporting of OBservational studies in Epidemiology statement. 17
Study Population
Using the OHDSI CohortGenerator R package, 18 we identified adults (≥18 years) with an inpatient hospital admission during calendar year 2021 (the most recent year available in P+) who required admission to an ICU with invasive mechanical ventilation (IMV) who had continuous observation in the database for at least 12 months prior to the ICU admission. While the severity of illness is known to be associated with greater CIAH, 6 most of the data needed to calculate a baseline severity of illness score is not available in P+. We therefore limited our analysis to patients with IMV, as it has been used as proxy for critical illness in other ICU studies.19,20
We excluded patients with an ICU admission in the 2 months prior to the index ICU hospitalization, given a prior CIAH could influence post-ICU ADA prescribing after a subsequent ICU admission or with an International Classification of Disease, Tenth Revision (ICD-10) diagnosis code for diabetic ketoacidosis (DKA) or a hyperosmolar hyperglycemic state (HHS), given post-hospitalization ADA prescribing practices could be different in this population. We also excluded patients discharged from the ICU hospitalization to locations other than the home setting, as data on prescribed ADA use was unavailable for patients discharged to another inpatient setting (eg, acute rehabilitation facility, long-term care). Lastly, to account for the lack of survival data in P+, we excluded patients whose insurance coverage ended within 30 days of the index ICU hospitalization, realizing the insurance coverage end date often lags the date of death.
Study Outcomes and Variables
The following ADA medication types were considered: insulin, ɑ-glucosidase inhibitors, biguanides, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, meglitinides, sodium-glucose co-transporter-2 (SGLT-2) inhibitors, sulfonylureas, and thiazolidinediones. The specific (ADA) medication classes for each of these ADA types are provided in Supplemental Table S1. Each ADA medication type and class was assigned its established Anatomical Therapeutic Chemical (ATC) codes. For ADA combination products, individual agents were allocated to the most appropriate medication class. Each of these medication types and classes prescribed in the 2 months prior to and after the index ICU hospitalization was mapped into the standard coding used in P+, RxNorm codes. Patients were grouped into ADA-naïve or ADA-experienced based on whether an ADA was prescribed in the 2 months prior to the ICU admission. The 2-month post-ICU follow-up window was chosen to ensure the ADA prescribing data were directly tied to the recent ICU hospitalization.
We also collected data on a diagnosis of DM in the 2 months before-and-after the index ICU hospitalization using ICD-10 codes. Data on age, sex, the Charlson Comorbidity Index (CCI), 21 Diabetes Comorbidity Severity Index (DCSI), 22 and the Hospital Frailty Risk Score (HFRS) 23 were collected during the 12 months prior to the ICU hospitalization. Admission type (ie, medical vs surgical) and the primary admitting diagnosis were determined using Current Procedural Terminology (CPT) codes documented in the 3 days prior to the ICU admission. Data on patients with a diagnosed coronavirus disease 2019 (COVID-19) infection during the ICU hospitalization was collected.
The primary study outcome was the proportion of ICU survivors prescribed an ADA medication(s) in the first 2 months after ICU hospitalization discharge among ADA-naïve patients. For this cohort, we characterized only the first ADA prescribed for each ADA class and the ADA classes concurrently prescribed (ie, ≥1 first ADA prescriptions prescribed within ≤1 day of the other). As secondary outcomes, we evaluated the association between the potential risk factors and new post-ICU hospitalization ADA use among the ADA-naïve patients. For this cohort, we also characterized: (1) the ADA classes prescribed post-ICU hospitalization, (2) the number of new ADA prescriptions post-ICU hospitalization, and (3) ADA use relative to the presence of a DM diagnosis before or after ICU hospitalization. For the patients prescribed an ADA in the 2 months prior to the ICU hospitalization (ie, ADA-experienced), we evaluated ADA prescriptions in the 2 months after ICU hospitalization discharge and whether they were newly prescribed or continued from the pre-ICU hospitalization period.
Data Analysis
Descriptive statistics were reported for all variables. Continuous variables were expressed as medians and interquartile range (IQR) or as means and standard deviation (SD) and were compared between groups using Mann-Whitney U tests or t tests. Categorical variables were expressed as counts and percentages and were compared between groups using chi-square tests. We conducted a multivariable logistic regression to determine the association between potential risk factors for post-ICU hospitalization ADA prescribing (ie, age, history of DM, CCI, DCSI, HFRS, and medical [vs surgical] admission) and newly prescribed ADA(s) in the 2 months after ICU hospitalization. Missing data values were reported and handled with simple imputation with the median in the logistic regression. 24 Statistical significance was defined as a 2-sided P-value < .05 in all statistical analyses. Data analysis was performed using R Version 4.0.3. 25
Results
During 2021, data for 28 798 817 adults were found in the P+ database. A subset of 451 628 patients were hospitalized, and 10 866 were admitted to the ICU and required IMV (Figure 1). One third (4,091, 37.6%) of these 10 866 patients were excluded because their insurance coverage ended within 30 days of hospital discharge. Among the remaining 6775 patients, 4042 were excluded because they had one or more of the following: prior ICU admission (341, 8.4%), an ICU admitting diagnosis of DKA (205, 5.1%) or HHS (40, 0.1%), or discharge to a setting other than home (3440, 85.1%). Among the 2733 remaining patients, 2346 (85.8%) were ADA-naïve at the time of the ICU hospitalization and 387 (14.1%) were ADA-experienced.
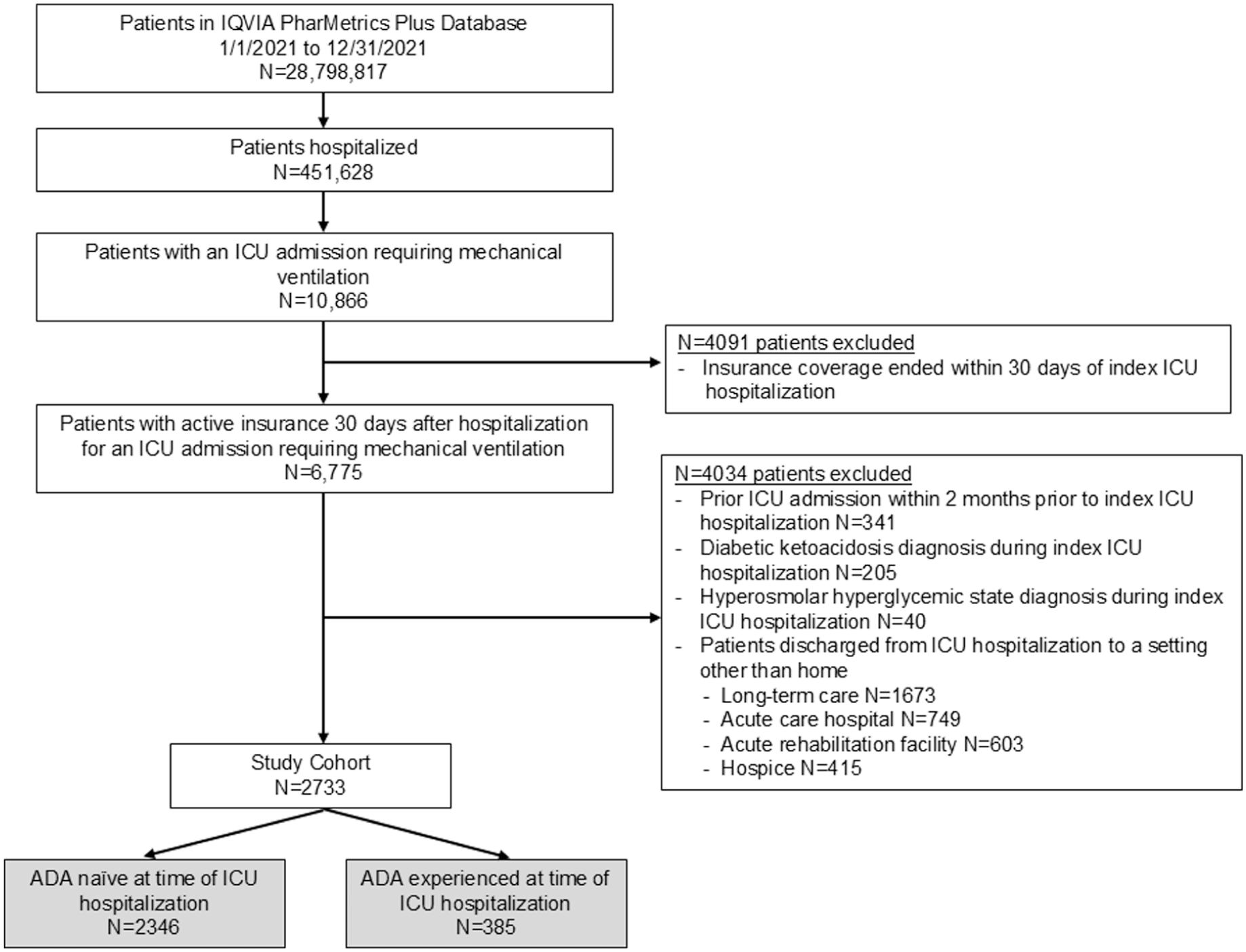
Flow chart of study patients.
Among the 2346 ADA-naïve patients, 100 (4.2%) were newly prescribed one or more ADAs in the 2 months after the ICU hospitalization. These 100 patients (vs the 2246 patients not newly prescribed an ADA post-hospitalization) were younger (P = .04), more likely to have a pre-hospital diagnosis of DM (P < .01), and have greater multimorbidity (CCI) (P = .01) and DM comorbidity (DCSI) (P < .01) (Table 1). Most (88/100, 88.0%) were first prescribed only 1 ADA, most commonly a biguanide (39/88, 44.3%) or insulin (29/88, 33.0%) (Table 2).
Comparison of Baseline Characteristics in Antidiabetic Agent (ADA)-Naïve Patients Between Patients Prescribed an ADA(s) in the 2 Months After ICU Hospitalization and Those Who Were Not.
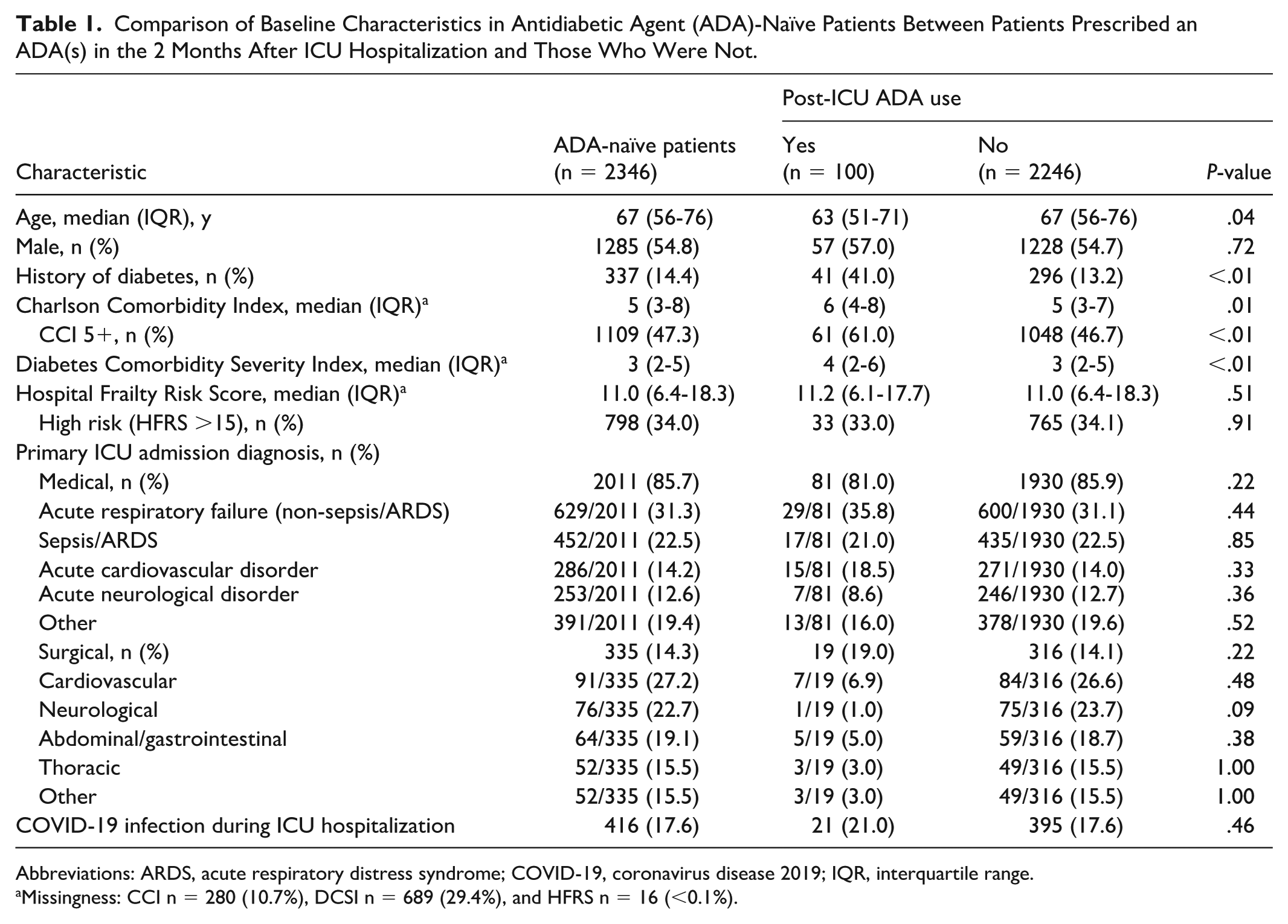
Abbreviations: ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; IQR, interquartile range.
Missingness: CCI n = 280 (10.7%), DCSI n = 689 (29.4%), and HFRS n = 16 (<0.1%).
Characterization of the ADA(s) First Prescribed in the 2 Months After an ICU Hospitalization in ADA-Naïve Patients.
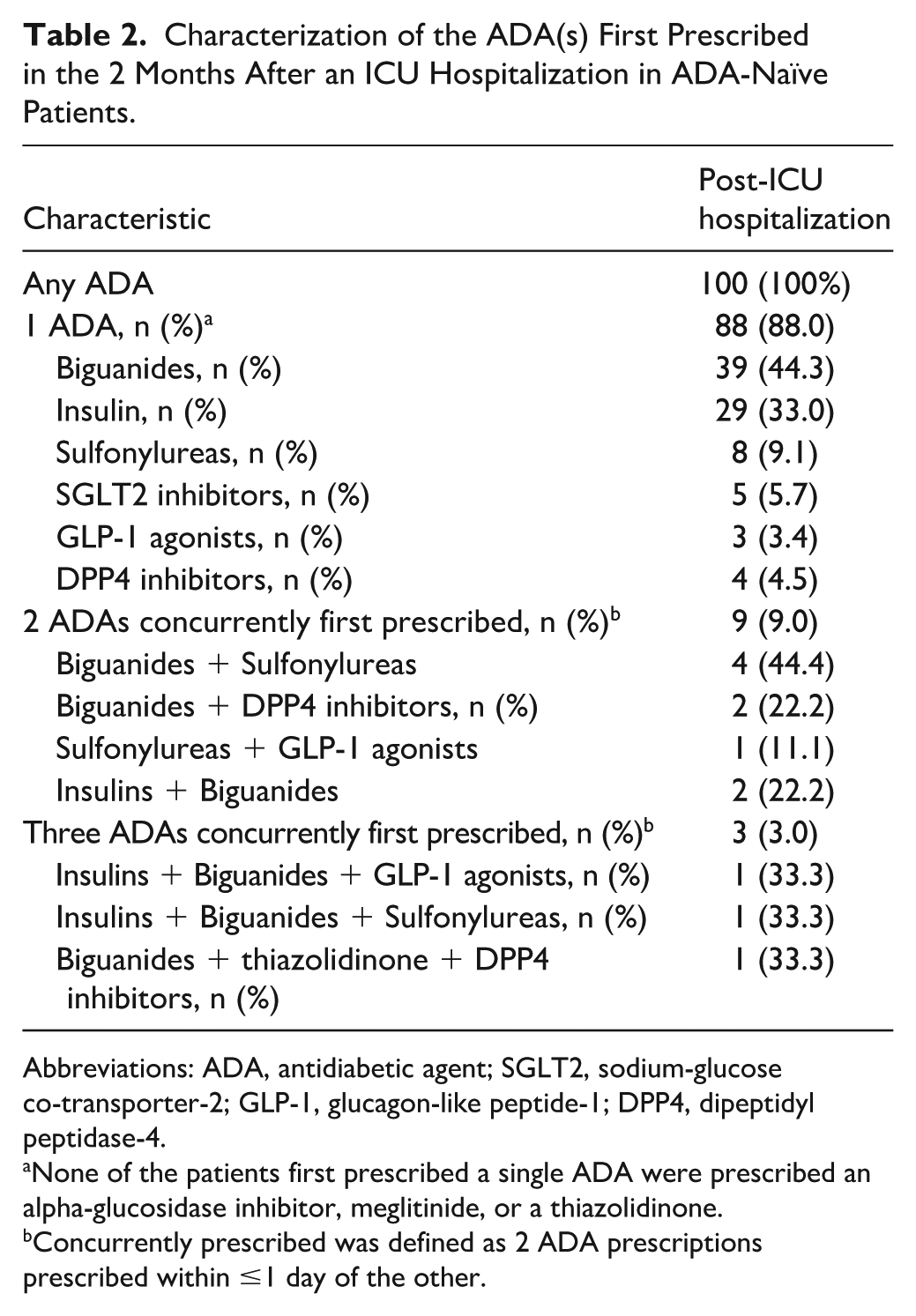
Abbreviations: ADA, antidiabetic agent; SGLT2, sodium-glucose co-transporter-2; GLP-1, glucagon-like peptide-1; DPP4, dipeptidyl peptidase-4.
None of the patients first prescribed a single ADA were prescribed an alpha-glucosidase inhibitor, meglitinide, or a thiazolidinone.
Concurrently prescribed was defined as 2 ADA prescriptions prescribed within ≤1 day of the other.
Multivariate logistic regression analysis indicated that patients with a pre-ICU hospitalization diagnosis of DM were almost 5 times as likely to be newly prescribed an ADA after the ICU hospitalization (adjusted odds ratio [aOR] = 4.90, 95% confidence interval [CI] = 2.91-8.19) (Table 3). Age (aOR = 0.99, 95% CI = 0.97-1.00) and pre-admission frailty (aOR = 0.96, 95% CI = 0.93-0.99) were inversely associated with new, post-hospitalization ADA prescribing.
Association Between Baseline Characteristics and 2-Month, Post-ICU Hospitalization ADA Prescribing in ADA-Naïve Patients.
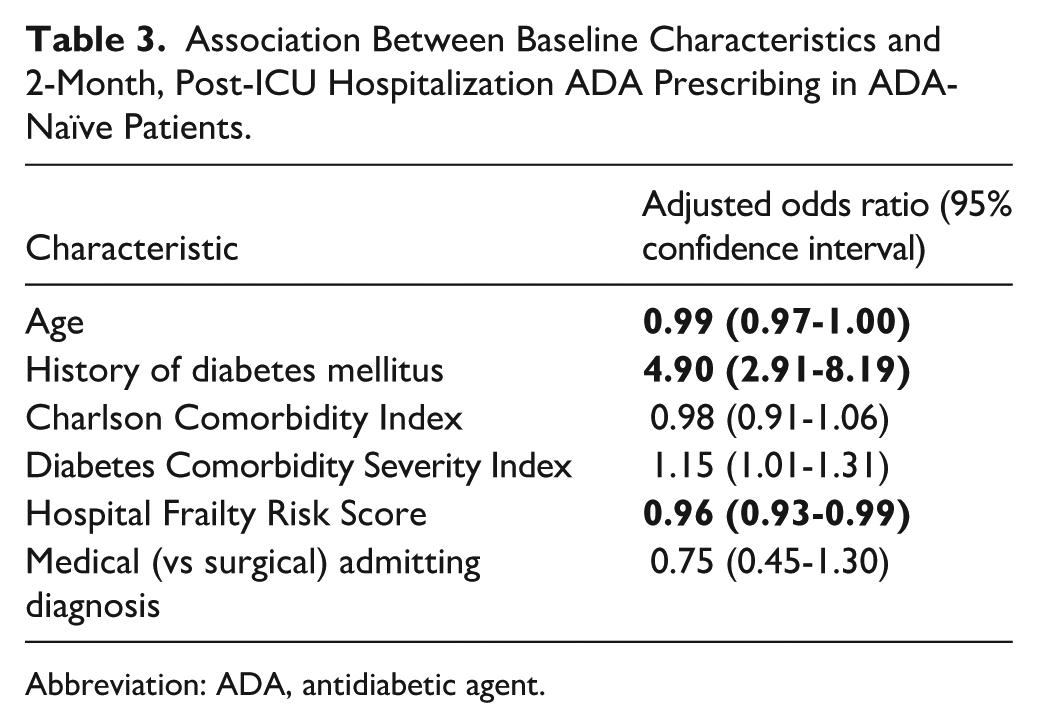
Abbreviation: ADA, antidiabetic agent.
Among the 385 ADA-experienced patients, only 214 (55.5%) were prescribed at least 1 continued or new ADA(s) in the 2 months post-hospitalization (Figure 2), suggesting pre-ICU ADA therapy may not have been restarted up to 173 (44.9%) of these patients after hospital discharge. For example, among the 104 ADA-experienced patients prescribed a biguanide after hospital discharge, 88 (84.6%) were continued on a biguanide from the pre-admission period and 16 (15.4%) were newly initiated on one. Among the 214 patients, most (169, 79.0%) were first prescribed only 1 ADA type, with 37 (17.3%) being prescribed 2 and 8 (3.7%) being prescribed 3 or more. Among 387 ADA-experienced patients, the proportion where a diagnosis of DM was documented was similar in the 2 months prior (vs after) hospitalization (291 [75.2%] vs 292 [75.4%], P = .10). However, the proportion of these DM-diagnosed patients prescribed ADA therapy was significantly greater in the 2 months prior (vs after) hospitalization (291/291 [100%] vs 190/292 [65.1%], P < .01).
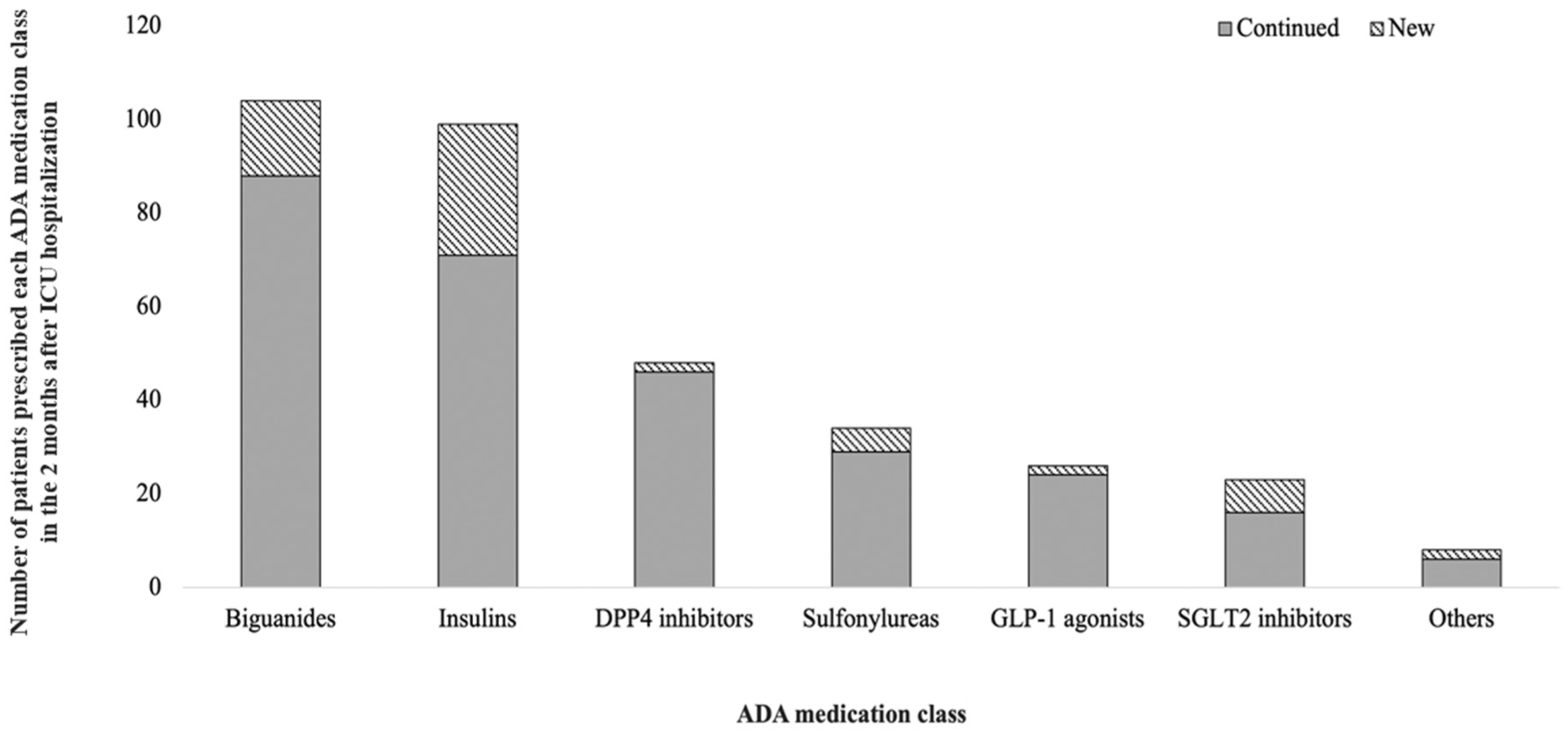
Total ADA prescriptions per medication class in the 2 months prior to and 2 months following an ICU hospitalization in the 385 ADA-experienced patients.
Discussion
This article, to the best of our knowledge, represents one of the first published large US cohort analyses of post-hospital ADA prescribing in critically ill adult ICU survivors and has a number of interesting observations. Despite the high prevalence of CIAH and the frequent use of insulin during ICU admissions,1,6,7,9 only 4.3% of adults ADA-naïve at ICU admission were newly prescribed an ADA in the 2 months after hospital discharge. Among these patients, the new prescriptions for insulin (33/100, 33.0%) were surprisingly low compared to non-insulin ADAs (67/100, 67.0%). A substantial (41.0%) proportion of the ADA-naïve patients with a new post-ICU hospitalization ADA prescription had an underlying diagnosis of DM prior to ICU admission. Patients with a diagnosis of DM after ICU discharge were 5 times more likely to be prescribed a new ADA prescription.
The 2-month 4.3% incidence of newly prescribed ADA in ADA-naïve patients after ICU discharge we identified is similar to the 4.8% prescribing incidence reported from 1 center, where the presence of CIAH was shown to increase the risk of post-discharge diabetes nearly 2-fold. 1 While data suggest that COVID-19 hospitalizations increase the risk for new DM by 66%, 26 we found post-ICU hospitalization ADA not to be greater in patients with COVID-19.
Surprisingly, only slightly over half of the ADA-experienced patients were continued or newly initiated an ADA(s) after hospital discharge. Given the nature of the P+ database, we were not able to determine the rationale for not resuming pre-ICU ADA therapy after discharge. Prior research in older, hospitalized veterans with pre-admission diagnosis of DM, only some of whom were admitted to an ICU, compared outcomes between patients with ADA medication intensification (ie, a newly prescribed ADA or dose increased more than 20% from pre-hospital) to a propensity-matched cohort without intensification. 27 Similar to our cohort, more than one third of these Veterans Administration patients previously diagnosed with DM were not receiving DM therapy prior to admission. This study also reported that post-hospitalization ADA intensification in the 30 days after discharge was associated with a more than 2-times greater risk for a hypoglycemic event(s). A concern for hypoglycemia in older adults after initiation of new ADA therapy is likely to be the primary reason older adults in our cohort were significantly less likely to be initiated on a new ADA after ICU hospitalization. Although the proportion of surgical ICU patients was small, an association between admitting service and ADA prescribing was not detected.
Our study had important strengths. Our analysis represents the first attempt to identify new ADA use and the factors associated with it in adults after an ICU hospitalization. Our national cohort was large and represents ADA prescribing practices across the United States. We focused our study on ICU patients who were critically ill. We excluded patients with recent ICU admissions or who were admitted to the ICU with an acute hyperglycemic event. We explored key variables hypothesized to be associated with new post-ICU ADA prescribing using a rigorous multivariable model.
Our study also has potential limitations, some of which are related to the use of claims data. Hospital clinical or medication data were not available, and we cannot comment on whether the frequency or severity of CIAH during the ICU hospitalization influenced post-hospital ADA use. The retrospective design and lack of clinical provider notes eliminate insights into the decision-making process of prescribers both during-and-after the hospital stay. Although we excluded 4042 patients whose insurance ended within 30 days post-discharge to avoid including those who died or switched plans, only 3 were newly prescribed an ADA, suggesting minimal impact on our findings. Limiting our analysis to only adults who were discharged to home may underestimate the use of ADA hospitalization, given that patients who transition to another acute care hospital or long-term care may be more likely to have long-term glycemic dysregulation. While claims data capture prescriptions, they do not provide information on whether patients adhered to their prescribed ADA. We relied on ICD-10 codes for DM diagnosis rather than clinical parameters (eg, glycosylated hemoglobin, Hb1Ac), so data may have been missing, especially for the pre-diabetic population. In addition, the data were reported for the 60-day post-ICU hospitalization period; we evaluated may be different during later post-hospitalization periods. However, we feel this time frame represents a valid snapshot of post-ICU hospital discharge ADA use, given most ADA prescribing and prescribing adjustments have been shown to take place within 60 days of hospital discharge. 27 Finally, our results may not represent current ADA post-ICU prescribing practices, particularly given the ever-increasing use of GLP-1 receptor agonists in patients both with and without DM, but data from 2021 were the most recent year we had access to.
Conclusion and Relevance
Our results suggest that ADA therapy after an ICU hospitalization in critically ill adults is infrequent but more common in patients with pre-existing diagnosis of DM prior to ICU admission. Important areas for future research include the prospective evaluation of the timing of ADA initiation during the ICU hospitalization, characterizing persistent ADA use beyond 2 months, evaluating the association between ICU factors, including ICU insulin protocol use and intensity and post-ICU ADA needs, and the adherence and safety of post-ICU ADA prescribing.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261455748 – Supplemental material for Characterization of Antidiabetic Medication Prescribing After Hospital Discharge in US Critically Ill Adults
Supplemental material, sj-docx-1-aop-10.1177_10600280261455748 for Characterization of Antidiabetic Medication Prescribing After Hospital Discharge in US Critically Ill Adults by Ting-Ting Wu, Judi Jacobi, Caroline Cullen, Nora O’Neil, Julia Vigorito, Robert Cavanaugh and John W. Devlin in Annals of Pharmacotherapy
Footnotes
Author Contributions
T-TW, JJ, and JWD conceived the protocol. SET, BLE, AM, JV, KS, JPK, and JD contributed to data acquisition. All authors contributed to data analysis and interpretation. All authors drafted or revised the manuscript for important intellectual content, ensured the accuracy and integrity of the manuscript, and approved the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.