
Abstract
Background:
Apixaban and rivaroxaban, direct oral anticoagulants (DOACs) used for acute venous thromboembolism (VTE) treatment, require higher dose lead-in periods of 7 days and 21 days, respectively. The optimal lead-in duration for patients receiving more than 48 hours of parenteral anticoagulation (AC) is unclear. In addition, guidelines lack recommendations for high bleed-risk patients who might benefit from a shortened lead-in.
Objective:
This study aimed to evaluate the effectiveness and safety of a modified lead-in strategy, where parenteral AC counts toward shortening or eliminating the DOAC lead-in period, compared to a full lead-in strategy, where a 7-day apixaban or 21-day rivaroxaban lead-in is prescribed irrespective of parenteral AC received.
Methods:
A retrospective cohort study analyzed patients diagnosed with an acute VTE during hospitalization. Patients were grouped based on a modified versus full lead-in strategy. Primary outcomes of recurrent VTE (rVTE) and bleeding were evaluated at 90 days.
Results:
Of 101 included patients, 47 were in the modified lead-in group and 54 in the full lead-in group. Patients in the modified lead-in group had a higher risk of bleeding at baseline. Recurrent VTE occurred in 4 patients in the modified lead-in group, compared to 2 patients in the full lead-in group (9% vs 4%; P = .4129). Bleeding occurred in 10 patients in the modified lead-in group, compared to 3 patients in the full lead-in group (21% vs 6%; P = .0167).
Conclusion and Relevance:
No significant difference in rVTE was observed between groups. The modified lead-in group had a higher incidence of bleeding, possibly reflecting greater baseline risk and clinical complexity rather than the modification itself. Modified lead-in strategies may be reasonable in select patients, particularly those at high risk for bleeding; however, larger studies are needed to confirm safety and efficacy.
Introduction
Acute venous thromboembolism (VTE) poses a significant clinical burden, affecting an estimated 900 000 individuals annually in the United States. 1 Direct oral anticoagulants (DOACs) such as apixaban and rivaroxaban are commonly used to treat patients with acute VTE. In the AMPLIFY and EINSTEIN trials, these agents were compared to warfarin for the treatment of VTE.x.2,3 Patients received an initial higher dose lead-in: apixaban was dosed at 10 mg twice daily for 7 days, followed by 5 mg twice daily for the remainder of treatment, while rivaroxaban was dosed at 15 mg twice daily for 21 days, followed by 20 mg daily. Although often referred to as “loading doses” in practice, this lead-in period is not solely to achieve steady state more rapidly, as traditionally intended with pharmacologic loading doses. Rather, the higher dosing during the lead-in period primarily mitigates clot propagation and recurrence during the acute phase of VTE, when thrombotic risk is highest. 4
In the aforementioned trials, patients were excluded if they had initially received more than 48 hours of parenteral anticoagulation (AC). In clinical practice, patients diagnosed with VTE during hospitalization often receive parenteral AC for long periods of time while awaiting assessment, imaging, or procedures, before transitioning to apixaban or rivaroxaban. It remains unclear whether parenteral AC should count toward the lead-in period or if the entire lead-in period should be completed orally, irrespective of prior parenteral therapy. Furthermore, guidelines lack specific recommendations for patients at higher bleeding risk who may benefit from a shortened or omitted lead-in period, as the literature available in this population remains limited.
Few retrospective studies have evaluated the effectiveness and safety of apixaban and rivaroxaban with varying lead-in dosing strategies. One single-center retrospective study by Williams et al 5 reported no significant difference in recurrent VTE (rVTE) between modified and full lead-in regimens, although the study was underpowered. Bleeding was higher in the modified lead-in group, attributed to greater baseline risk such as cancer, concomitant antiplatelet therapy, and multiple transitions between parenteral and oral ACs. In contrast, a multicenter retrospective study by Alshaya et al 6 demonstrated no significant differences in rVTE or major bleeding between modified and full lead-in dosing strategies, indicating similar effectiveness and safety. Of note, this study was not powered to detect clinically meaningful differences in rVTE, as the effect size was set at 0.3, notably larger than the differences in rVTE observed in the AMPLIFY and EINSTEIN trials, which were 0.9% and 0.4%, respectively.2,3 The largest study to date by Jolakoski et al 7 found no significant difference in time to rVTE or major bleeding events between modified and full lead-in groups. Importantly, this study was not powered to detect a difference in the incidence of rVTE.
The definition of a full lead-in strategy remained relatively similar amongst the aforementioned studies. However, a modified (alternatively referred to as reduced) lead-in definitions differed. Williams et al 5 defined the modified lead-in group as receiving less than 7 or 21 days, or no oral lead-in at all. Alshaya et al 6 defined the modified lead-in as parenteral AC followed by higher dose apixaban or rivaroxaban to complete at least 6 or 19 days of combined parenteral and oral lead-in therapy, respectively. Finally, Jolakoski et al 7 defined a modified lead-in as at least 7 or 21 days of combined parenteral and lead-in dosing of apixaban or rivaroxaban, respectively.
Studies evaluating modified lead-in strategies to date have demonstrated differences in safety outcomes, possibly attributable to confounders, and have been underpowered to detect differences in incidence of rVTE. Continued investigation of real-world prescribing practices and clinical outcomes associated with modified lead-in dosing strategies following variable durations of parenteral AC remains essential. The objective of this study was to evaluate the effectiveness and safety of a modified lead-in strategy compared with a full lead-in strategy in patients receiving parenteral AC prior to transitioning to apixaban or rivaroxaban.
Materials and Methods
Study Design, Setting, and Patients
This study was a single-center retrospective cohort study conducted using data from patients hospitalized at University Health in San Antonio, Texas, between January 2022 and September 2024. The study was approved by the Institutional Review Board at the University of Texas Health Science Center at San Antonio and University Health.
Patients were included if they were 18 years of age or older, had been diagnosed with acute VTE during hospitalization, and had received either continuous infusion unfractionated heparin (UFH) or therapeutic enoxaparin for at least 24 hours before transitioning to apixaban or rivaroxaban. Patients were excluded if they were on AC prior to admission, had received thrombolytics during the current hospitalization, were diagnosed solely with a left ventricular thrombus or cerebral venous sinus thrombus, were pregnant, or were incarcerated.
After inclusion, patients were grouped based on whether they were prescribed a modified or full lead-in strategy. A modified lead-in strategy was defined as any regimen in which the duration of parenteral AC counted toward shortening or eliminating the oral lead-in period. In modified strategies where oral therapy was initiated, dosing followed standard high-dose lead-in recommendations. A full lead-in strategy was defined as completion of the full oral high-dose lead-in, regardless of prior parenteral AC received. Total AC exposure, including therapy continued after hospital discharge, was determined using dispense histories documented in the institution’s electronic health record (EHR).
To facilitate sub-analyses evaluating varying lead-in modifications, patients were further divided into 4 cohorts, as illustrated in Figure 1. Patients in the modified lead-in group were categorized into cohorts 1 and 2. These patients received lead-ins with parenteral AC alone or in combination with oral AC, resulting in omission of a portion of the standard oral lead-in period. Cohort 1 included patients who were prescribed at least 7 days (apixaban) or 21 days (rivaroxaban) of combined parenteral and/or oral lead-in therapy, whereas cohort 2 included those prescribed less than 7 or 21 days of combined therapy. Patients in the full lead-in group were categorized into cohorts 3 and 4 and were prescribed full oral lead-in periods (7 days for apixaban and 21 days for rivaroxaban). Cohort 3 included patients who received less than 48 hours of parenteral AC before transitioning to a full oral lead-in, and cohort 4 included those who received 48 hours or more of parenteral AC prior to full oral lead-ins.
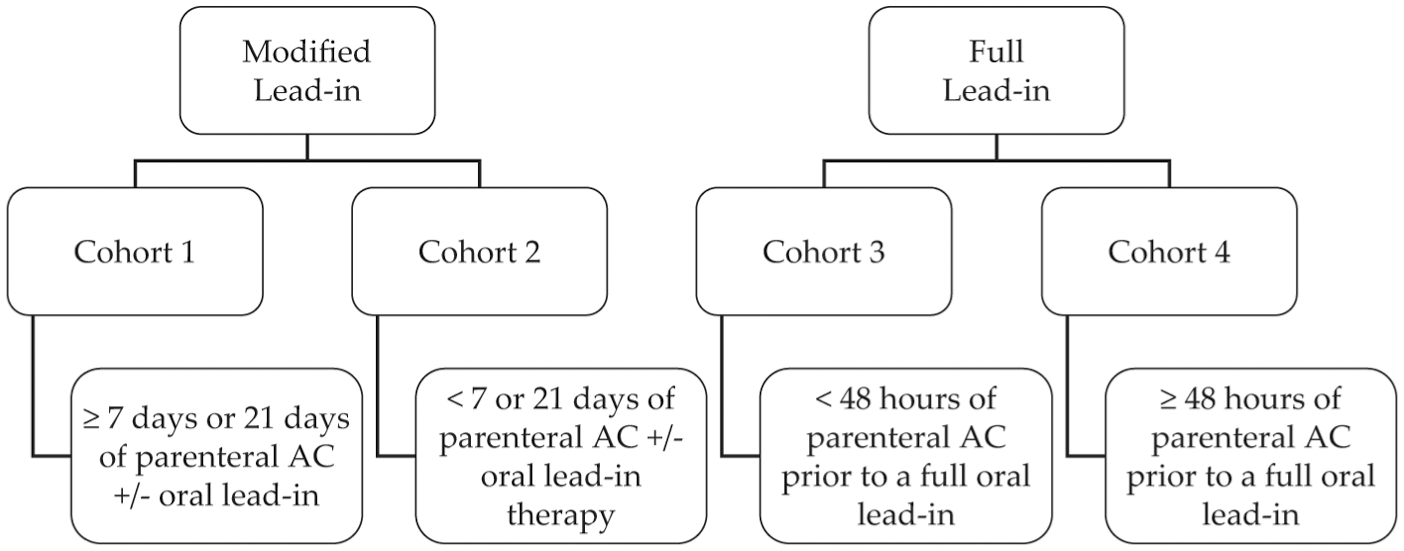
Cohort divisions.
Data Collection and Outcome Measures
Patients diagnosed with VTE who received parenteral AC followed by rivaroxaban or apixaban were identified using an EHR report and screened for inclusion. Baseline characteristics and outcomes were collected via manual chart review. To supplement the analysis of bleed risk at baseline, a DOAC score was calculated for each patient. 8 Unlike the Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly, Drugs/alcohol (HAS-BLED) score, which was originally validated in patients treated with vitamin K antagonists, the DOAC score was derived and validated in patients receiving DOAC therapy and demonstrated superior predictive performance in studied cohorts. In this model, scores range from 0 to 20 patients, with higher score corresponding to an increased predicted risk of major bleeding within 1 year. The DOAC score components and their interpretation are outlined in Table A in the Supplementary Material.
The primary effectiveness outcome evaluated was the incidence of rVTE. Recurrent VTE was defined as a new, objectively confirmed VTE event occurring after initiation of AC. The primary safety outcome was a composite of major bleeding and clinically relevant non-major bleeding (CRNMB). Secondary safety outcomes included individual incidence of major bleeding and CRNMB. Major bleeding and CRNMB were defined according to the International Society on Thrombosis and Haemostasis (ISTH) criteria.9,10 Additional outcomes assessed included time to bleeding event and mortality. Recurrent VTE rates and mortality were evaluated up to 90 days following the index VTE event; all safety outcomes were evaluated from the first day of parenteral AC.
Statistical Analysis
The study was designed to compare apixaban and rivaroxaban lead-in strategies with respect to the primary effectiveness outcome. A sample size of 563 patients was estimated to detect an absolute risk reduction of 4%, with 80% power for the primary outcome. This effect size was selected based on rVTE incidence rates estimated or observed in prior trials. Comparisons with P value of <.05 were considered statistically significant. Continuous data were analyzed using the Student t test if normally distributed; ordinal and non-normally distributed continuous data were analyzed using the Mann-Whitney U test. Nominal data were analyzed using the chi-square test or Fisher exact test, as appropriate. Data were collected and managed using Microsoft Excel, version 2016. All statistical analyses were completed using JMP Pro 18 software.
Results
Patient Characteristics
In total, 366 patients were screened, and 101 were included. Reasons for exclusion are shown in Figure 2, and baseline characteristics are outlined in Table 1. The modified lead-in group consisted of 47 patients, while the full lead-in group included 54 patients. Median ages were 58.4 and 56.5 years, and females comprised 51% and 39% of the respective groups. Overall, 58% of patients were identified as Hispanic. Baseline characteristics were not statistically different between groups, except for the incidence of chronic kidney disease, further corroborated by a lower creatinine clearance, documented bleeding event within the prior 12 months, and presence of diabetes – all of which were more prevalent in the modified lead-in group. Additionally, patients in the modified lead-in group had a greater incidence of DOAC scores greater than or equal to 8 at baseline, indicating a high or very high bleed risk (25% vs 6%; P = .0049).
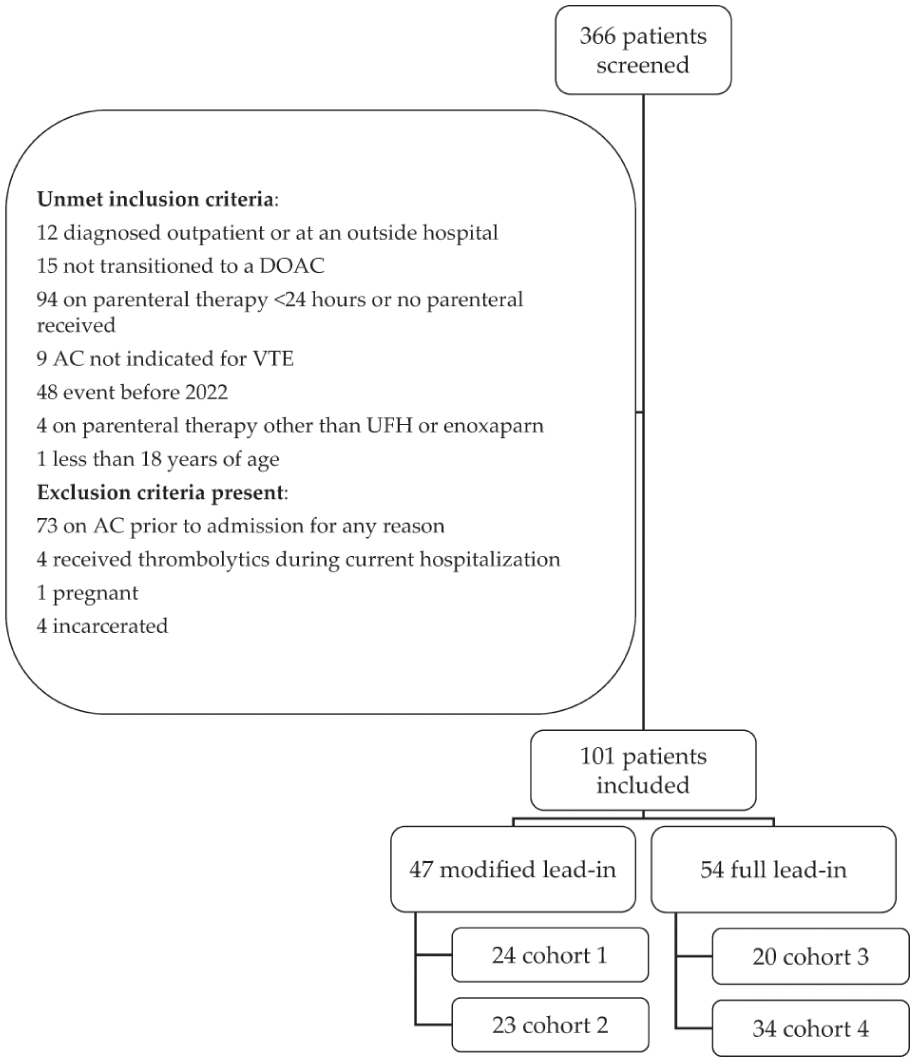
Patients evaluated for study inclusion.
Patient Demographics and Clinical Characteristics.
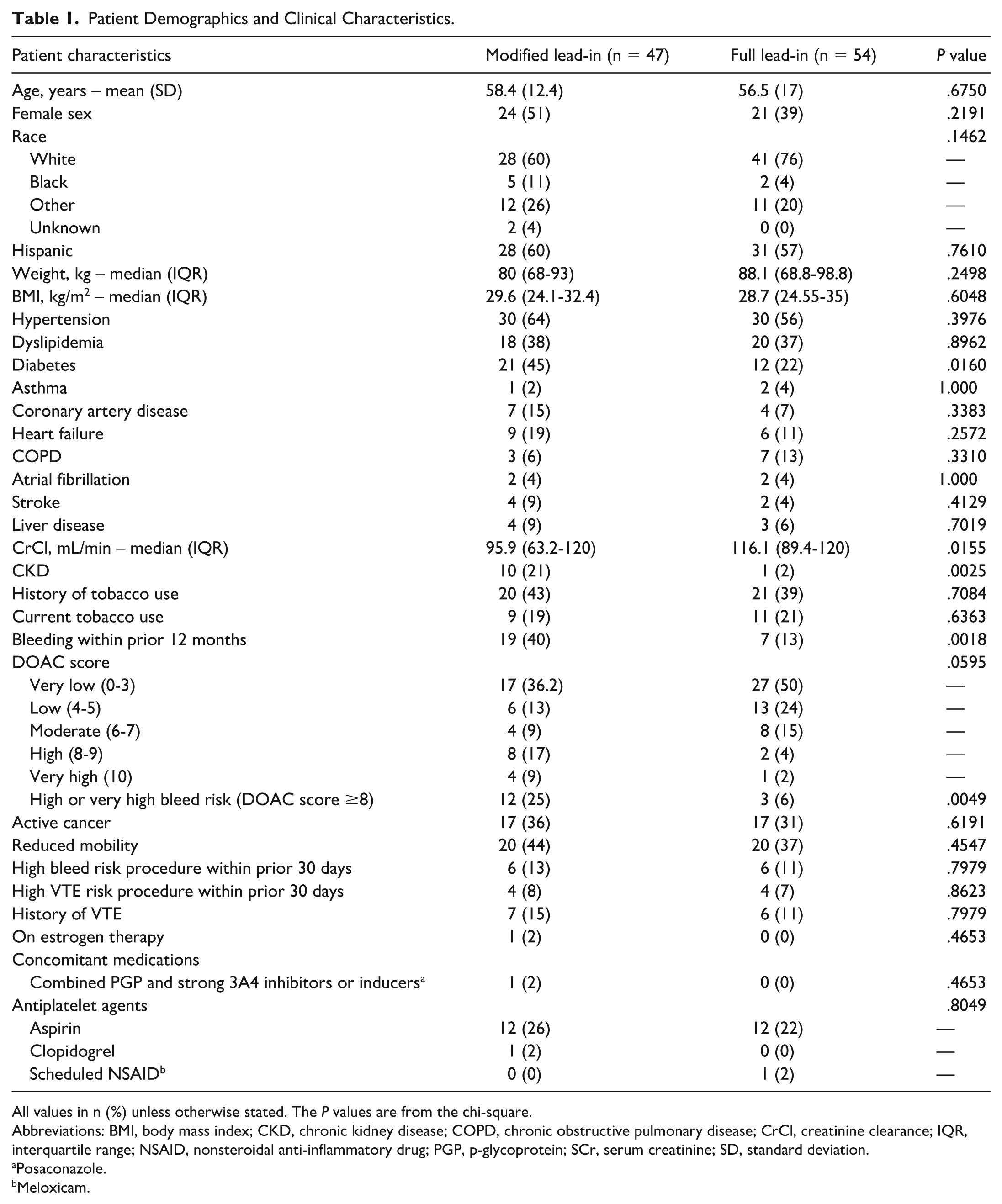
All values in n (%) unless otherwise stated. The P values are from the chi-square.
Abbreviations: BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CrCl, creatinine clearance; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug; PGP, p-glycoprotein; SCr, serum creatinine; SD, standard deviation.
Posaconazole.
Meloxicam.
Admission, Anticoagulation, and Venous Thromboembolism Characteristics
Patients in the modified lead-in group experienced longer hospitalizations (9 days vs 4.9 days; P < .0001) and received more days of parenteral AC than those in the full lead-in group (5.3 days vs 2.3 days; P < .0001) (Table 2).
Admission, Anticoagulation, and VTE Characteristics.
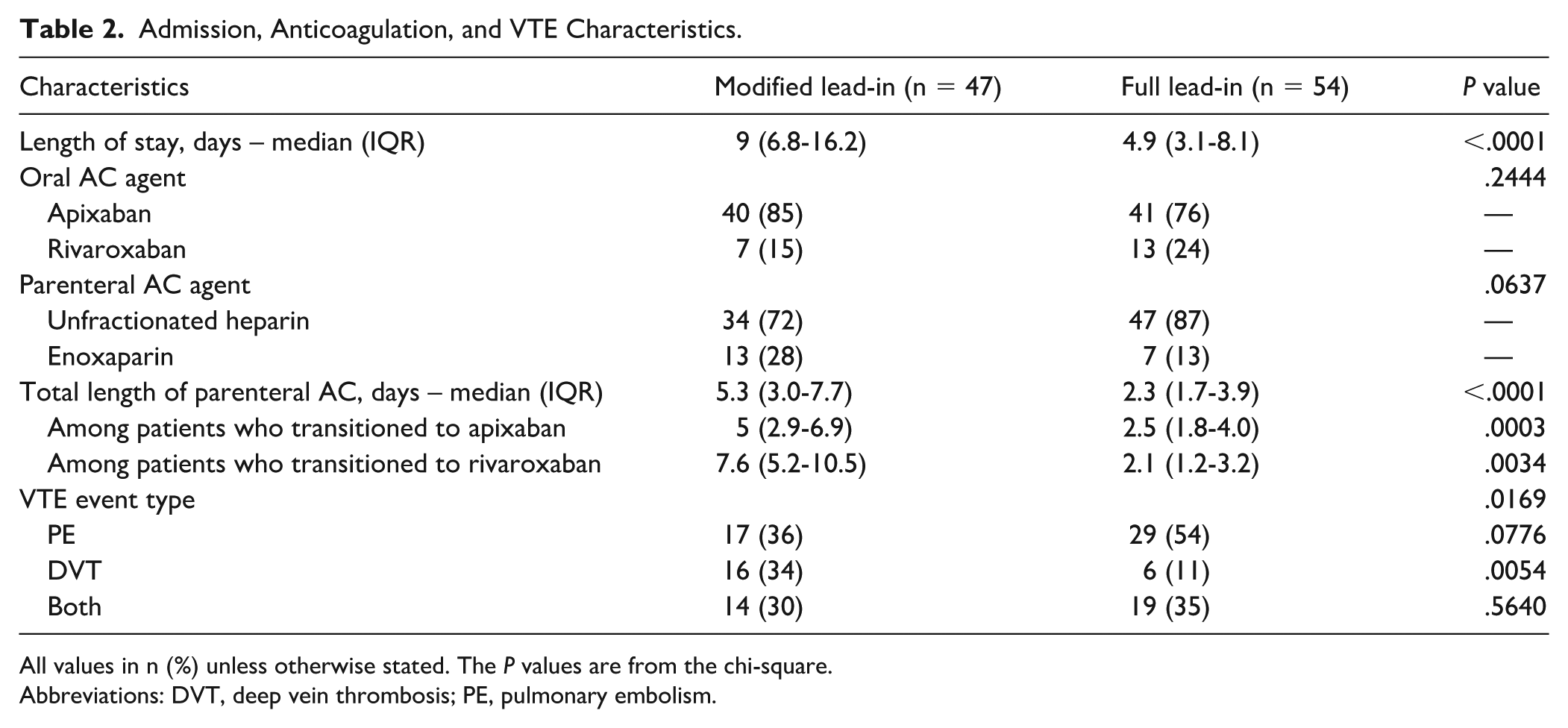
All values in n (%) unless otherwise stated. The P values are from the chi-square.
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
Apixaban was the most commonly used oral AC in both study groups (80% overall). Unfractionated heparin represented 80% of parenteral AC used before transitioning to apixaban or rivaroxaban. The differences in the choice of oral and parenteral anticoagulants between groups were not statistically significant.
The type of VTE was significantly different between groups (P = .0169). The full lead-in group had a higher proportion of patients with pulmonary embolism (PE) compared to the modified lead-in group (54% vs 36%). Conversely, deep vein thrombosis (DVT) was more commonly observed in the modified lead-in group (34% vs 11%; P = .0054).
Outcomes
The difference in rVTE events between study groups was not statistically significant (Table 3), with 2 events occurring in the modified lead-in group compared to 2 events in the full lead-in group (9% vs 4%; P = .4129). Of the 6 patients with rVTE, 4 had active cancer, 3 in the modified lead-in group and 1 in the full lead-in group. There was a statistically significant difference in composite bleeding events, with 10 patients affected in the modified group compared to 3 in the full lead-in group (21% vs 6%; P = .0167). Of the total bleeding events, 5 were classified as major bleeding, while 8 were classified as CRNMB (Table 4). Mortality rates were not significantly different between groups (11% vs 6%), and there were no statistically significant differences in time to bleeding or time to mortality.
Group Outcomes.
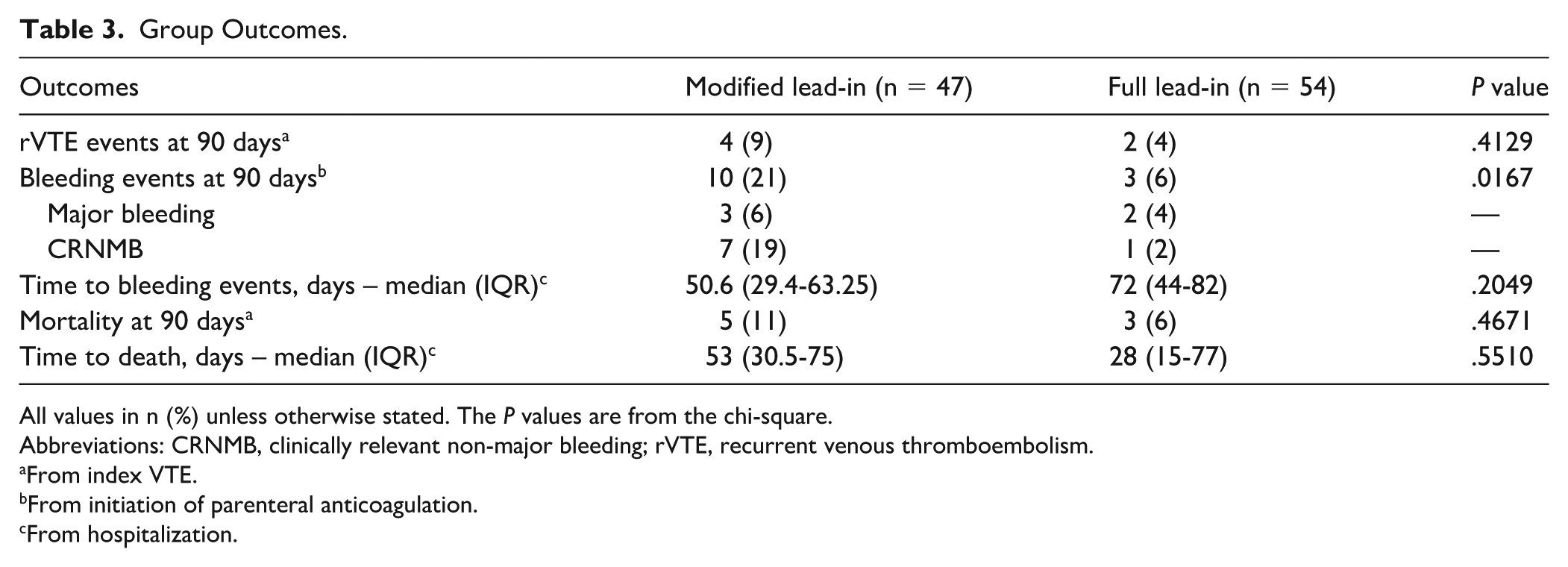
All values in n (%) unless otherwise stated. The P values are from the chi-square.
Abbreviations: CRNMB, clinically relevant non-major bleeding; rVTE, recurrent venous thromboembolism.
From index VTE.
From initiation of parenteral anticoagulation.
From hospitalization.
Bleeding Event Details.
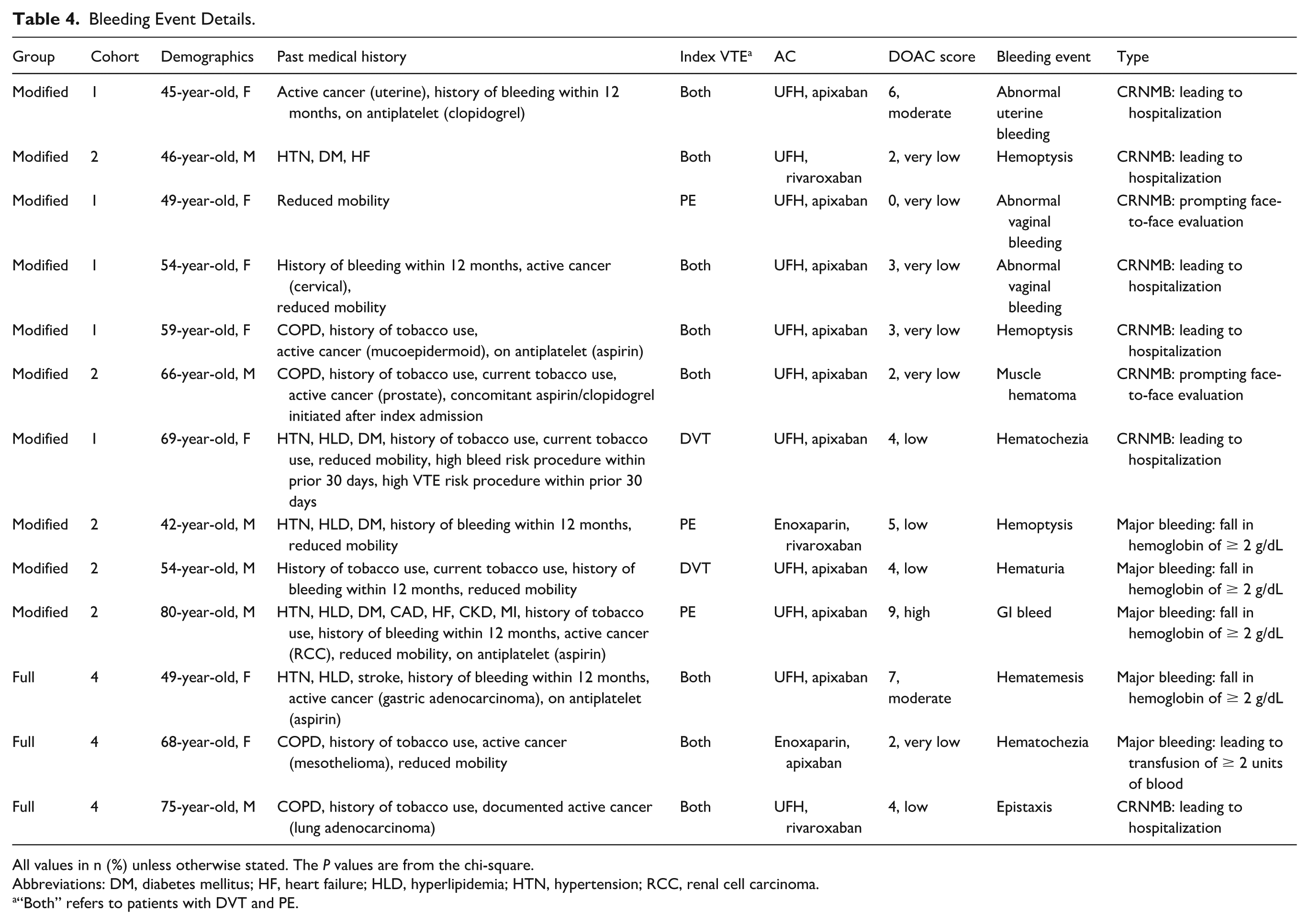
All values in n (%) unless otherwise stated. The P values are from the chi-square.
Abbreviations: DM, diabetes mellitus; HF, heart failure; HLD, hyperlipidemia; HTN, hypertension; RCC, renal cell carcinoma.
“Both” refers to patients with DVT and PE.
The distribution of outcomes across cohorts is summarized in Table B1 in the Supplementary Material. When comparing cohorts within groups (cohort 1 vs cohort 2 and cohort 3 vs cohort 4), no statistically significant differences were observed in the primary effectiveness outcome. The primary safety outcome of bleeding trended toward significance when comparing cohorts 1 to 3 and 2 to 3, with a higher incidence of bleeding in the modified lead-in group; however, differences were not statistically significant. Detailed inter-cohort comparisons are provided in the Supplementary Material.
Discussion
Since the publication of the AMPLIFY and EINSTEIN trials, apixaban and rivaroxaban have become cornerstone therapies for acute VTE.2,3 However, these trials did not evaluate patients who received more than 48 hours of parenteral AC or those at high bleeding risk, leaving the optimal lead-in approach in such patients unclear. This study aimed to compare clinical outcomes between modified and full lead-in strategies and to evaluate prescribing patterns at our institution.
We did not observe a statistically significant difference in rVTE between groups. Although underpowered, our findings suggest that parenteral AC may serve as an alternative to lead-in doses of apixaban or rivaroxaban during the acute phase of VTE treatment. This may be explained by the efficacy of parenteral AC during the acute phase, indicating that parenteral therapy may reasonably contribute to the lead-in period. Compared to previous retrospective studies evaluating modified and full lead-in regimens, our overall VTE recurrence rates were higher: 9% in the modified lead-in group vs 4% in the full lead-in group. This difference may be attributed to the higher prevalence of malignancy, as 4 of the 6 rVTE occurred in patients with active cancer, a well-known major risk factor for thromboembolism. 11 In contrast to previous studies, which reported 3%, 18%, and 21% of patients with active cancer, 34% of our study population had active cancer.5-7 Additionally, patients in our modified group had a longer duration of parenteral AC prior to transition compared to several previously published studies, further distinguishing our cohort and contributing additional real-world insight to existing literature.
There was a statistically significant difference in the safety outcome of composite bleeding between groups. Patients in the modified lead-in group were at higher risk of bleeding at baseline as evidenced by a higher incidence of risk factors for bleeding, such as chronic kidney disease, diabetes mellitus, and a history of bleeding within the previous 12 months. The number of patients with DOAC scores of 8 or greater also differed significantly between groups. However, most bleeding events occurred in patients categorized as very low to low risk of major bleeding by the DOAC score, consistent with the predominance of CRNMB rather than major bleeds. Because the DOAC score was validated to predict major bleeding risk in patients with atrial fibrillation, its ability to predict non-major bleeding risk may be limited.
Our findings highlighted considerable variability in AC prescribing practices, with a near-even distribution between patients receiving a full lead-in (53%) and those receiving a modified lead-in (47%) strategy – a higher proportion of modified use than previously reported (20-25%).5-7 Furthermore, patients in the full lead-in group were more likely to have a PE rather than a DVT, potentially reflecting provider hesitancy to modify lead-in regimens for PE due to its higher associated mortality risk. 12 Moreover, the higher prevalence of bleeding risk factors in the modified lead-in group suggests that concerns about bleeding influenced providers’ decisions to shorten or adjust the lead-in period. Of the patients in the modified lead-in group, 23 patients (48%) were in cohort 2 having received fewer than 7- or 21-day lead-in with parenteral and oral AC, further reflecting a heightened concern for and emphasis on bleeding risk mitigation.
Among patients in the modified lead-in group who experienced a bleeding event, all had omitted the oral lead-in entirely. The average duration of parenteral AC was 9 days, regardless of the oral agent prescribed. Among apixaban users, 5 patients omitted oral lead-in therapy after completing at least 7 days of parenteral AC, while 2 did so after only 2 days. In contrast, none of the patients receiving rivaroxaban completed at least a 21-day parenteral course before omitting the oral lead-in. These findings suggest that modified lead-in strategies may be clinically justifiable in select patients, particularly those at high risk for bleeding, given higher rates of bleeding events without a corresponding increase in rVTE.
The primary limitation of this study is its small sample size and failure to meet the prespecified power, which limited the ability to detect statistically significant differences in the primary outcome. As a result, the absence of a statistically significant difference, particularly rVTE, should be interpreted with caution and may reflect underpowering rather than true equivalence between strategies. Additional limitations include the retrospective design, which introduces potential confounding and selection bias. Outcome evaluation relied on outpatient follow-up or hospital readmission to document 90-day events, which may have led to underrepresentation of rVTE, bleeding, or mortality outcomes. Detailed assessment of parenteral AC intensity (e.g., heparin levels or activated partial thromboplastin time [aPTT] values) was not performed; however, Table 4 provides detailed clinical context for bleeding events to aid interpretation of outcomes. Furthermore, as discussed previously, patients in the modified lead-in group had a higher baseline bleeding risk and longer hospitalizations suggestive of greater clinical complexity, which likely influenced treatment selection and may have contributed to higher observed bleeding rates. Finally, rivaroxaban accounted for only 20% of the DOACs used in our study, which may limit the generalizability of our findings to this anticoagulant. Notably, this proportion is consistent with distributions reported in previously published studies.5-7
This study reflects real-world clinical practice and highlights the importance of addressing this relevant clinical question. It specifically included patients who were excluded from original landmark trials, thereby contributing to the literature on treatment modifications in high-risk populations. This study adds to the collective evidence by expanding evaluation of modified lead-in strategies to a more heterogeneous hospitalized population with higher bleeding risk and longer parenteral AC exposure, while also providing insight into clinical practice patterns and variability not consistently represented in prior analyses. Additionally, this study included a substantial number of patients who identified as Hispanic, offering insights into a demographic underrepresented in previously published studies. Our analysis also included patients who received fewer than 7 or 21 days of parenteral or oral combined (cohort 2), providing data on adjustments to the lead-in period beyond simply substituting oral therapy with parenteral therapy. Furthermore, the novel DOAC score was utilized to assess baseline bleeding risk, contributing observational data to existing literature regarding the use of this tool in patients with VTE; however, larger studies are needed to determine its validity or applicability beyond atrial fibrillation.
Conclusions and Relevance
No significant difference in VTE recurrence was observed between modified and full lead-in strategies. The modified lead-in group had a higher incidence of bleeding, although this may be related to a higher baseline bleed risk and greater clinical complexity influencing treatment selection, rather than the modification itself. Larger studies are needed to further evaluate the safety and efficacy of modified dosing strategies, particularly in patients at higher bleed risk.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261456308 – Supplemental material for Modified vs Full Lead-in Dose Apixaban and Rivaroxaban for Treatment of Acute Venous Thromboembolism
Supplemental material, sj-docx-1-aop-10.1177_10600280261456308 for Modified vs Full Lead-in Dose Apixaban and Rivaroxaban for Treatment of Acute Venous Thromboembolism by Jeanette Lahoud, Josephine Jacobs, Lauren Ratrut, Amanda Kitten and Crystal Franco-Martinez in Annals of Pharmacotherapy
Footnotes
Acknowledgements
The authors would like to thank Ms Monet Giles, Ms Saumyaa Patel, and Mr Diego Sierrez (student pharmacists) for their contributions to the study.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Texas Health Science Center of San Antonio and University Health (protocol code STUDY0000106, approved November 8, 2024).
Informed Consent Statement
Patient consent was waived by the Institutional Review Board of the University of Texas Health Science Center of San Antonio and University Health, given that this study is a retrospective cohort study.
Author Contributions
C.F.M. and J.J. contributed to the conceptualization. J.L., J.J., L.R., A.K., and C.F.M. contributed to the methodology. A.K. contributed to the formal analysis. J.L. contributed to the investigation. J.L. and A.K. contributed to the data curation. J.L. contributed to the writing – original draft preparation. J.L., J.J., L.R., A.K., and C.F.M. contributed to the writing – review and editing. J.L. contributed to the visualization. J.J., L.R., A.K., and C.F.M. contributed to the supervision. J.J., L.R., and C.F.M. contributed to the project administration. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data are presented in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.