
Abstract
Background:
Insulin is commonly used to manage steroid-induced hyperglycemia. However, optimal dosing strategies for long-acting steroids like dexamethasone remain unclear.
Objectives:
This study evaluated insulin glargine use for dexamethasone-induced hyperglycemia (DIH) and evaluated factors associated with achieving glucose targets (AGTs).
Methods:
This retrospective, single-centered cohort study included adult, noncritically ill patients who received once-daily insulin glargine and dexamethasone for at least 3 consecutive days during admissions between July 1, 2021, and July 31, 2023. Patients were excluded if they had type 1 diabetes mellitus or received intravenous insulin within the first 3 days. The primary outcome was the percentage of patients AGT, defined as mean blood glucose 70 to 180 mg/dL on day 3 of combination therapy. Patients were then stratified into AGT and persistent hyperglycemia (PH) cohorts to evaluate secondary outcomes which included hypoglycemia incidence and patient or treatment characteristics associated with AGT.
Results:
Among 118 patients included, 28 (24%) were in the AGT cohort and 90 (76%) were in the PH cohort. The AGT cohort had a lower mean body mass index (29.1 vs 33.7 kg/m2, P = .02) and fewer patients with preexisting type 2 diabetes mellitus (85.7% vs 97.8%, P = .03). Median insulin glargine units standardized by dexamethasone dose was similar between cohorts (2.25 [1.08-3.33] vs 2.00 [1.17-4.00] units/mg/day, P = .98). The PH cohort required significantly higher median daily bolus insulin doses (24 vs 6 units/day, P < .01). There was 1 patient, who was in the AGT cohort, who experienced hypoglycemia.
Conclusion and Relevance:
This study suggests that current practice underdoses insulin glargine initially for DIH management and relies on reactive bolus insulin with limited success. Earlier and more assertive insulin glargine dosing is warranted to improve early glycemic control without substantially increasing hypoglycemia risk. Limitations include the retrospective single-centered study design and limited sample size with imbalanced cohorts.
Background
Hyperglycemia is a common adverse effect associated with glucocorticoids, often occurring even with short-term use. Studies have shown as high as an 86% incidence rate for steroid-induced hyperglycemia (SIH) 1 and patients on systemic steroid therapy have previously demonstrated an increased risk of developing new-onset diabetes.2,3 Known risk factors for SIH include high dose/potency of corticosteroid, tobacco smoking, age > 60 years, body mass index (BMI) > 25 kg/m2, hemoglobin A1c (HbA1c) ≥ 6.0%, estimated glomerular filtration rate (eGFR) < 40 mL/min/1.73 m2, and family history of diabetes mellitus. 4 In addition, the presence of inpatient hyperglycemia has been associated with prolonged hospital stay, increased infection risk, and mortality.5,6
Dexamethasone, a potent long-acting corticosteroid, presents unique challenges in SIH management owing to its extended half-life. Several retrospective studies and a systematic review have evaluated insulin dosing for dexamethasone-induced hyperglycemia (DIH) in the coronavirus disease 2019 (COVID-19) population. Fornwald et al 7 observed no significant difference in 5-day mean blood glucose (BG) when using any of the following strategies: average total daily dose (TDD) of insulin at 0.3 units/kg with insulin glargine, 0.2 units/kg with insulin neutral protamine hagedorn (NPH), or 0.2 units/kg with combination of insulin glargine and NPH. Ketaroonrut et al 8 explored the initial insulin TDD in 4 weight-based ranges and found patients receiving a TDD ≤ 0.29 units/kg with 99% as basal insulin was associated with lowest treatment failure in COVID-19 patients receiving steroids. Brooks et al 9 have previously proposed a basal-bolus insulin (BBI) regimen without NPH starting at 0.5 to 0.6 units/kg, distributed as 40% basal and 60% prandial with correctional insulin (1 unit per 25 mg/dL above 150 mg/dL), and a BBI plus NPH approach based on prednisone-equivalent dose from their systematic review.
Additional retrospective studies have examined insulin use for DIH outside the COVID-19 population, however, all had a limited sample size. Gosmanov et al 10 reported twice-daily insulin detemir initiating at 0.33 ± 0.13 units/kg/day plus prandial and correctional aspart at 0.33 ± 0.12 units/kg/day resulted in improved mean BG compared with aspart alone by day 3 in patients with diabetes and hematologic malignancies receiving dexamethasone therapy (8-40 mg/day). Brady et al 11 reported use of BBI with a TDD of 1 to 1.2 units/kg/day, distributed as 25% basal and 75% prandial, for acute leukemia and lymphoma patients on 40 mg/day dexamethasone.
Aside from the Gosmanov study, most prior research on insulin dosing tends to combine different types of insulin as basal therapy or extrapolate dosing strategies used for SIH with intermediate-acting steroids to DIH.7-9,11,12 However, grouping multiple insulin and steroid types together overlooks the significant differences in their pharmacokinetic profiles, particularly between intermediate-acting and long-acting agents, which may not provide the best assessment for DIH management.
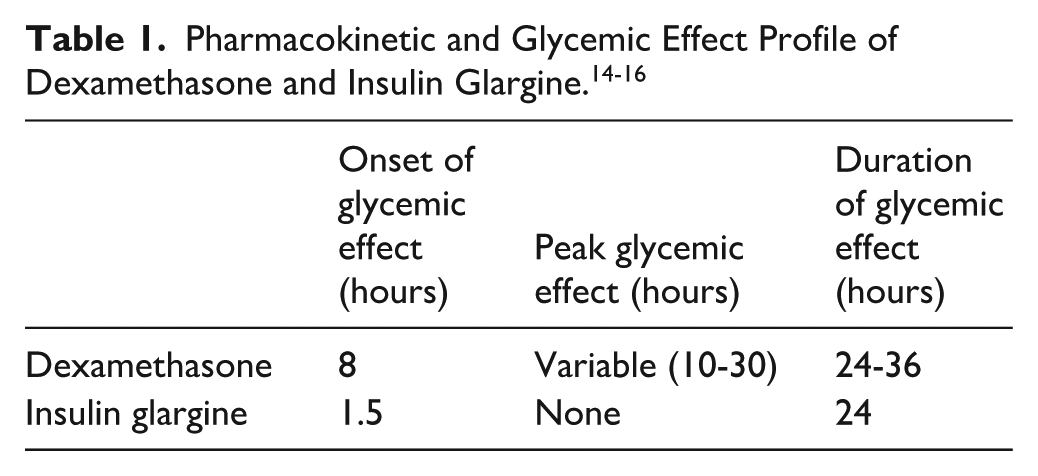
For patients experiencing DIH, a long-acting insulin such as insulin glargine would be pharmacokinetically advantageous given similarities in their peak and duration timelines (Table 1). Indeed, the American Diabetes Association (ADA) recommends the use of long-acting insulin to counteract the hyperglycemic effect from long-acting glucocorticoids such as dexamethasone. 13 However, more research is needed to explore management of DIH with a focus on a single type of long-acting insulin as the basal therapy.
This study aims to evaluate the current “real-world” use of once-daily dosing of insulin glargine to manage DIH from once-daily dexamethasone. The primary objective is to describe the proportion of patients who achieved the target 24-hour mean BG value on day 3 of combination therapy of dexamethasone and insulin glargine therapy. The secondary objectives were to report safety outcomes, primarily the development of hypoglycemia, and evaluate patient and treatment characteristics associated with achieving the glucose target (AGT) on day 3 of combination therapy for future research.
Method
Study Design and Population
This retrospective, single-center cohort study evaluated adult patients admitted during July 1, 2021, and July 31, 2023, who received once-daily dexamethasone and once-daily insulin glargine within 24 hours of each other. Day 1 of therapy was defined as the 24-hour period following the first dose of insulin glargine. Day 3 of therapy was similarly defined as the 24-hour period following the third dose of insulin glargine. After evaluation of the primary outcome on day 3 of therapy, patients were stratified into 2 cohorts based on the outcome of glycemic control: those AGT versus those with persistent hyperglycemia (PH) on day 3 of insulin glargine therapy.
Initial insulin doses were determined at provider discretion. At the time of the study, an institutional guideline for the management of SIH was in place which recommended starting insulin glargine for long-acting steroids at 0.1 to 0.2 units/kg or 50% of the prior 24-hour correction dose. This recommendation reflected expert institutional opinion based on local practice patterns and existing systematic reviews as well as ADA recommendations on long-acting insulin usage for DIH. 17 Noninsulin products for diabetes management were generally held based on common practice at the institution.
Inclusion and Exclusion Criteria
Adult patients who had documented administration of once-daily dexamethasone and once-daily insulin glargine within 24 hours of each other for at least 3 consecutive days were included. Patients were excluded for the following reasons: incarceration, pregnancy, diagnosis of type 1 diabetes mellitus, or in severe hyperglycemic states prior to dexamethasone initiation (defined as any one of admission BG > 300 mg/dL, diabetic ketoacidosis, or hyperglycemic hyperosmolar syndrome). Patients were also excluded if, during the 3-day study period, they received any steroids other than dexamethasone, received insulin detemir or insulin NPH in addition to insulin glargine, had a change in dexamethasone dose, received intravenous insulin, or were admitted to an intensive care unit (ICU).
Patients on dexamethasone and/or basal insulin prior to admission could still be included if the dexamethasone dose was adjusted by day 1 of therapy and/or if insulin glargine was dosed differently from their prior-to-admission basal insulin equivalent dose prior to day 3 of combination therapy. All patients who satisfied the inclusion and exclusion criteria listed above were incorporated into the analysis. As this was a retrospective descriptive study, all patients who met the criteria were included and a power calculation was not completed.
Outcome Measures
Baseline characteristics consisted of age, sex, admission weight and height, admission BG, HbA1c closest to admission (within 3 months prior to admission or 7 days postadmission), history of chronic kidney disease (CKD), and history of type 2 diabetes mellitus (defined as HbA1c ≥ 6.5%, 18 documented diagnosis in history and physical note for admission, or prior use of any antihyperglycemic agents for diabetes management). The prior-to-admission medication list was reviewed for basal insulin and dexamethasone dose, as appropriate. Process of care variables included indications of dexamethasone use based on chart review of progress notes and eGFR values on days 1 and 3 of combination therapy as calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation (mL/min/1.73 m2). 19
Doses of dexamethasone and insulin glargine, time of administration, presence of endocrinology consult, BG values, and TDD of short-acting bolus insulin administered were collected on days 1 and 3 of therapy. Insulin glargine dose was standardized to admission body weight (units/kg), dexamethasone dose (units/mg dexamethasone), and both body weight and dexamethasone dose (units/kg/mg dexamethasone). Standard of care for BG monitoring at the time of this study was 4 times daily timed before meals and at bedtime, with additional point-of-care testing performed as clinically indicated (eg, experiencing hypoglycemia), collected as a capillary point-of-care value. Only these capillary point-of-care BG values were collected, and plasma glucose levels were not. All available point-of-care BG values from days 1 and 3 of therapy were collected for each patient and used in the analysis, even if different from standard of care 4 values in a 24-hour period.
The primary outcome was the percentage of patients in the AGT cohort. AGT was defined as a 24-hour mean BG between 70 and 180 mg/dL on day 3 of combination therapy. Day 3 of therapy was chosen as the cutoff for analysis to allow for some insulin glargine titration by providers based on patient response while still maximizing sample size. Secondary safety outcomes included occurrence of hypoglycemia requiring intervention (BG < 70 mg/dL) during the study period based on point-of-care BG values. 20 Although the ADA recommends a glycemic target of 100 to 180 mg/dL for noncritically ill hospitalized patients, 13 this study defined AGT as 70 to 180 mg/dL as institutional standard of care would require intervention for patients with a BG <70 mg/dL.
To review factors that may have influenced attainment of target glucose, patients were split into an AGT and PH cohort based on the 24-hour mean BG on day 3 of combination therapy. Patient- and treatment-specific factors were included in this analysis between the 2 cohorts, including age, BMI, HbA1c, eGFR, and insulin glargine dose standardized to body weight, dexamethasone dose, or both. eGFR values were categorized to approximate CKD staging to facilitate description of renal function distribution between the AGT and PH cohorts as renal function may influence insulin clearance, although the degree to which it affects insulin requirements remains less clearly defined.4
Ethical Considerations
This study received the institutional review board’s approval and was conducted in accordance with the established requirements. This research involved minimal risk and was approved with a waiver for informed consent.
Data Collection and Statistical Analysis
Study data were collected from the electronic medical record and managed using REDCap electronic data capture tools hosted at our institution.21,22 Baseline demographics, past medical history, hospitalization, and treatment characteristics were assessed using descriptive statistics. Continuous variables were described using medians (interquartile range) or means (±standard deviation) and categorical variables were described using frequencies and proportions, as applicable. The mean BG on day 3 was calculated for each patient and used to classify patients into the AGT versus PH cohort. The primary outcome was reported as proportions of patients classified in the AGT cohort. For the secondary outcomes, potential risk factors were identified a priori based on a review of the literature. Unadjusted odds ratios with 95% confidence intervals were estimated for each selected characteristic with statistical significance assessed at a 2-sided alpha of .05. Potential confounding was explored descriptively but not controlled via multivariate modeling due to overall sample size and cohort size imbalance. Analyses involving HbA1c and prior-to-admission basal insulin dose in glargine equivalence were restricted to patients with available values and no imputation was performed.
Results
A total of 733 adult patients admitted between July 1, 2021 and July 31, 2023 with administrations of dexamethasone and insulin glargine were screened and 118 patients were included in the primary analysis. The most common reasons for exclusion were not receiving administrations of dexamethasone and/or insulin glargine for 3 consecutive days (N = 159) and more frequent than once-daily administration of insulin glargine (N = 129) (Figure 1). Patients were 55.9% male and 94.9% patients had a history of type 2 diabetes, with a mean admission BG of 168 mg/dL. Among the 92 patients with HbA1c values, the mean HbA1c was 7.5%. Most patients in this study received dexamethasone 6 mg daily and the most common indication for dexamethasone was COVID-19 (55.1%) (Table 2).
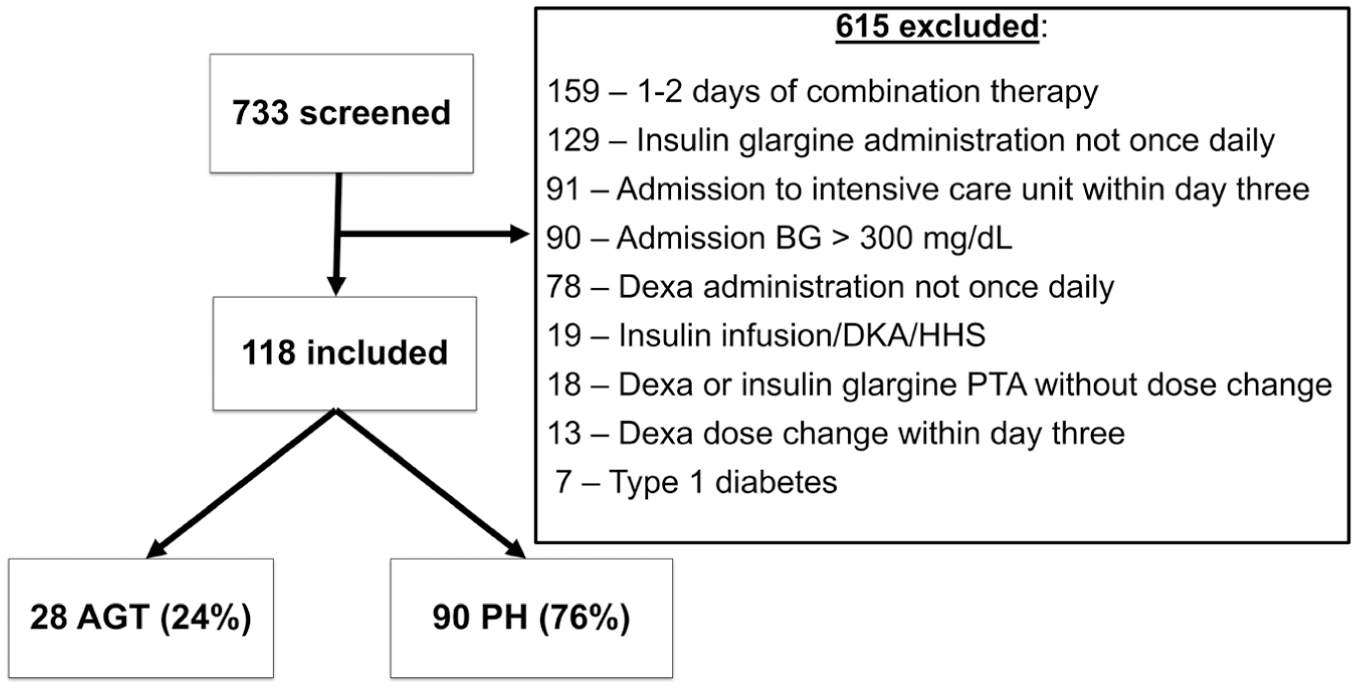
Flowchart of patients screened and included in study.
Baseline Characteristics of the Achieving Glucose Target and Persistent Hyperglycemia Cohorts.
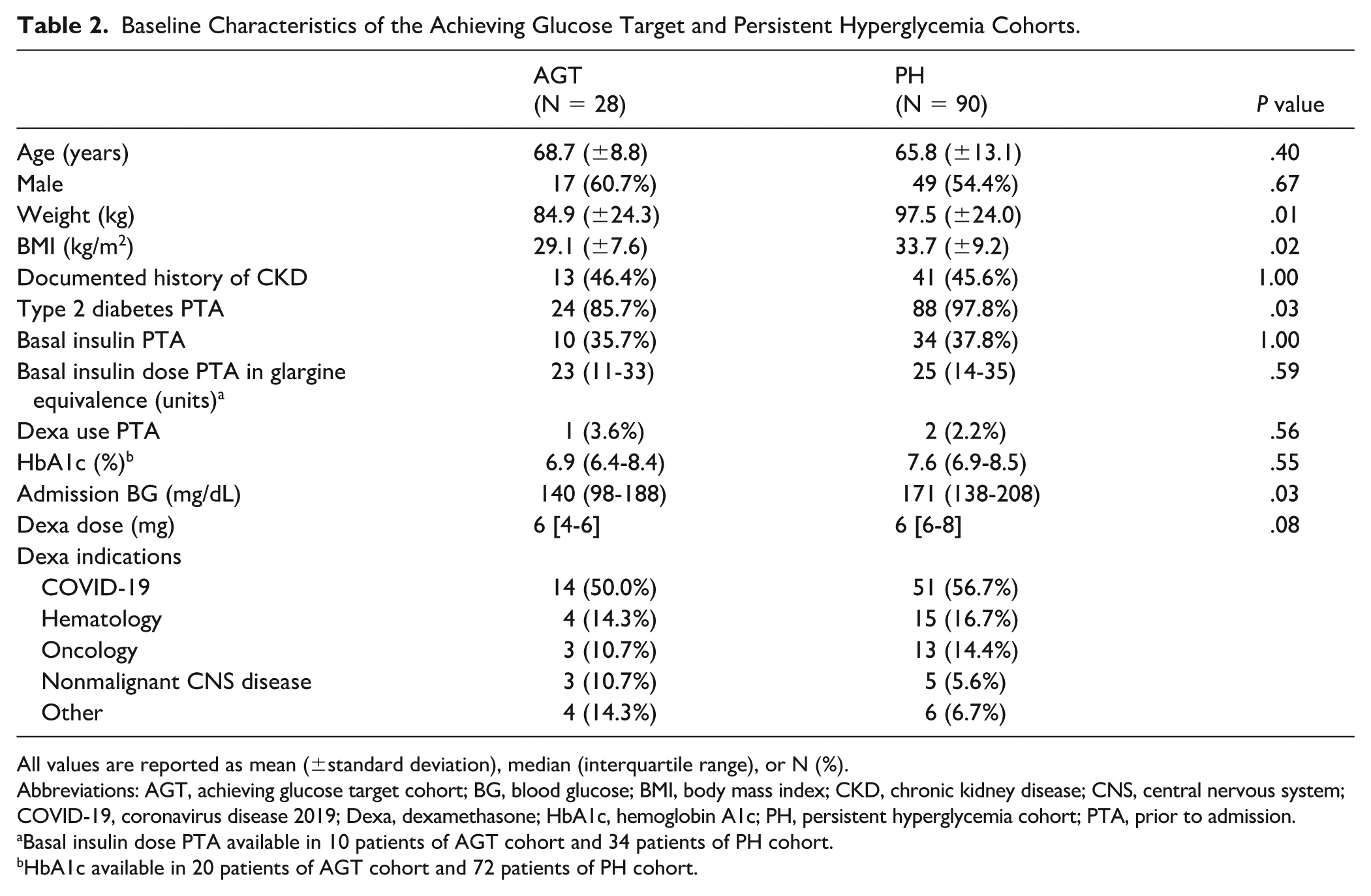
All values are reported as mean (±standard deviation), median (interquartile range), or N (%).
Abbreviations: AGT, achieving glucose target cohort; BG, blood glucose; BMI, body mass index; CKD, chronic kidney disease; CNS, central nervous system; COVID-19, coronavirus disease 2019; Dexa, dexamethasone; HbA1c, hemoglobin A1c; PH, persistent hyperglycemia cohort; PTA, prior to admission.
Basal insulin dose PTA available in 10 patients of AGT cohort and 34 patients of PH cohort.
HbA1c available in 20 patients of AGT cohort and 72 patients of PH cohort.
For the primary outcome, 28 patients (23.7%) met the previously defined glucose target, and 90 patients (76.3%) did not meet this criterion on day 3 of combination therapy (Figure 1). These patients were subsequently divided into AGT and PH cohorts for further analysis.
Comparing baseline characteristics, patients in the AGT cohort compared with the PH cohort had a lower mean admission body weight (84.9 ± 24.3 kg vs 97.5 ± 24.0 kg, P = .01) and mean BMI (29.1 ± 7.6 kg/m2 vs 33.7 ± 9.2 kg/m2, P = .02) as well as fewer patients with a preexisting diagnosis of type 2 diabetes mellitus (86% vs 98%, P = .03). Median BG on admission was also lower in AGT cohort compared with PH cohort (140 mg/dL vs 171 mg/dL, P = .03). No significant differences were found among other baseline characteristics between the 2 cohorts (Table 2).
On day 3 of combination therapy, patients had a mean BG value of 157 ± 16 mg/dL in the AGT cohort compared with 238 ± 44 mg/dL in the PH cohort. As a result, patients in the AGT cohort received less short-acting bolus insulin with a median dose of 6 (4-15) units/day compared with a median dose of 24 (15-45) units/day in the PH cohort on day 3 of combination therapy. Presence of endocrinology consult, eGFR values on days 1 and 3, and changes in diet status were similar between the cohorts on day 3 of combination therapy. A reduction in insulin glargine from the prior-to-admission basal insulin dose was observed on day 1 of therapy in both the AGT and PH cohorts. With subsequent insulin glargine escalation by day 3, the PH cohort reached a glargine dose similar to the prior-to-admission basal insulin dose, whereas the AGT cohort remained below the prior-to-admission basal insulin dose. However, the difference between the 2 cohorts was not statistically significant (Table 3).
Comparison of Insulin Glargine and Glucose-Related Variables Between Achieving Glucose Target and Persistent Hyperglycemia Cohorts.
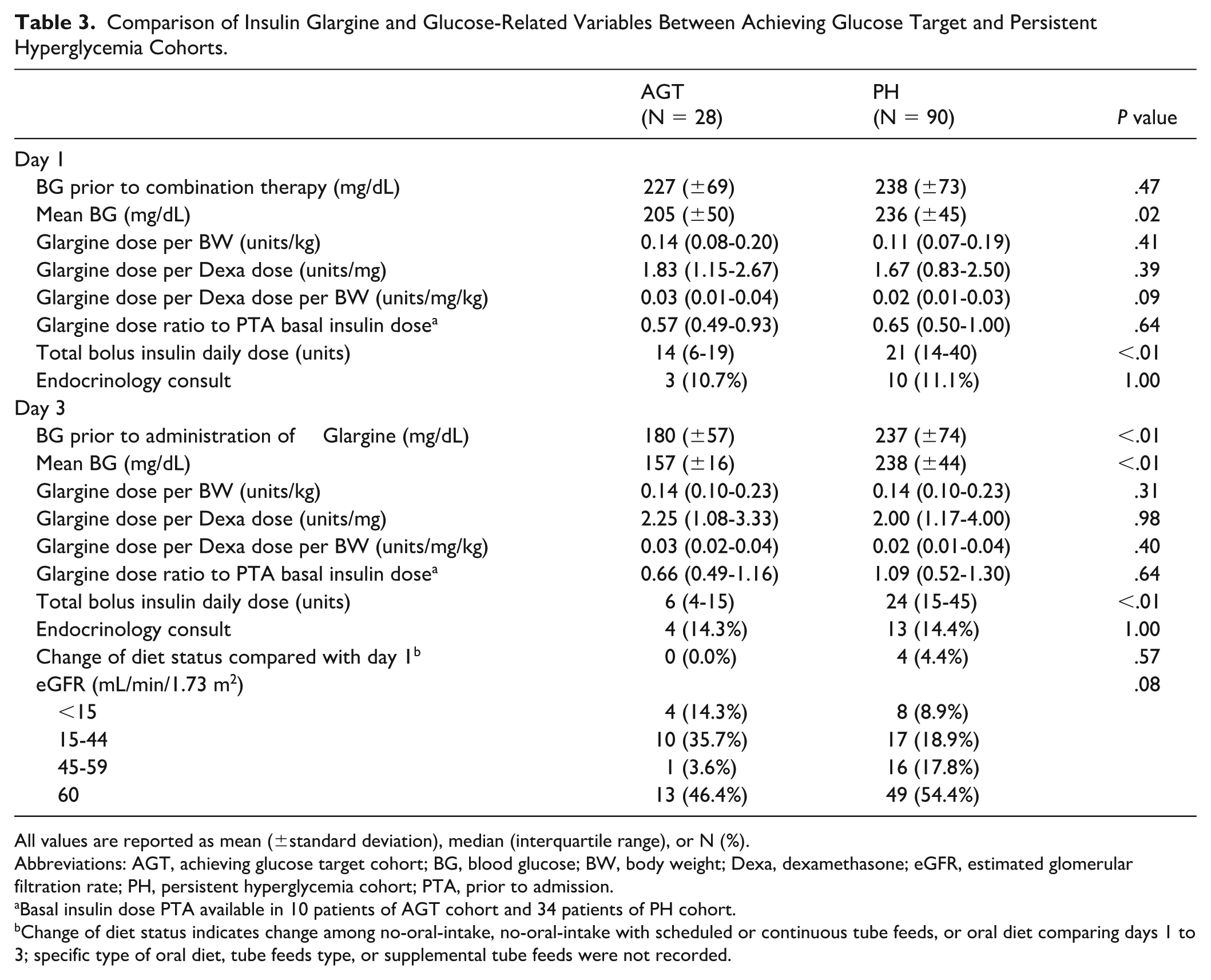
All values are reported as mean (±standard deviation), median (interquartile range), or N (%).
Abbreviations: AGT, achieving glucose target cohort; BG, blood glucose; BW, body weight; Dexa, dexamethasone; eGFR, estimated glomerular filtration rate; PH, persistent hyperglycemia cohort; PTA, prior to admission.
Basal insulin dose PTA available in 10 patients of AGT cohort and 34 patients of PH cohort.
Change of diet status indicates change among no-oral-intake, no-oral-intake with scheduled or continuous tube feeds, or oral diet comparing days 1 to 3; specific type of oral diet, tube feeds type, or supplemental tube feeds were not recorded.
To help evaluate treatment-specific factors that influenced the primary outcome, various strategies were explored to standardize insulin glargine dose by body weight, dexamethasone dose, or both. Patients in the AGT cohort received a numerically higher standardized insulin glargine dose based on dexamethasone dose (units/mg) and both body weight and dexamethasone dose (units/mg/kg) on day 3 of combination therapy compared with the PH cohort, but the differences did not achieve statistical significance (Table 3). Variations in standardized insulin glargine dose were observed across different dexamethasone indications, but statistical comparisons were not performed due to limited and uneven sample size within each group (Table 4).
Standardized Insulin Glargine Dose by Different Dexamethasone Indications on Day 3 of Therapy.
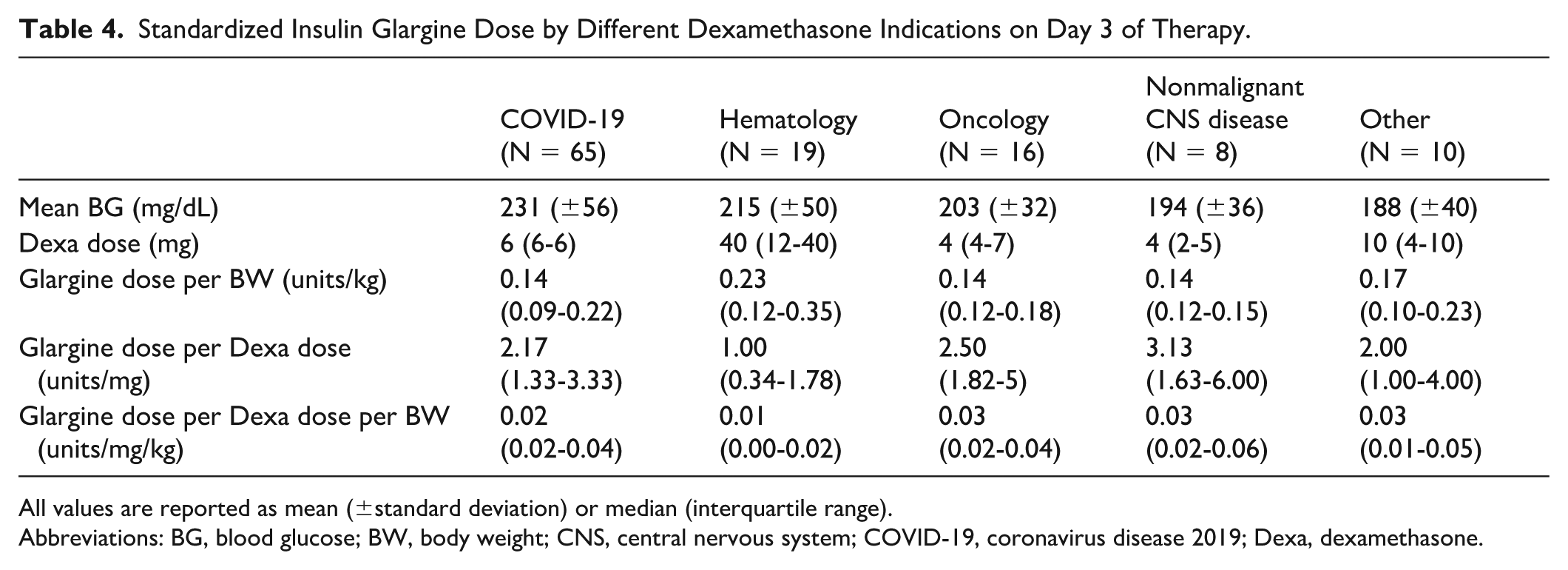
All values are reported as mean (±standard deviation) or median (interquartile range).
Abbreviations: BG, blood glucose; BW, body weight; CNS, central nervous system; COVID-19, coronavirus disease 2019; Dexa, dexamethasone.
In terms of safety outcomes, one patient in the AGT cohort experienced the lone incidence of hypoglycemia. This patient had a documented BG of 42 mg/dL on day 3 of the combination of therapy. This patient received 6 mg dexamethasone and 5 units of insulin glargine on both days 1 and 3, and had an eGFR of 11 mL/min/1.73 m2. No patients in the PH cohort experienced hypoglycemia.
Discussion
In this study, 23.7% of patients met the primary outcome of a 24-hour mean BG within the target range on day 3 of combination therapy. Most patients in our study received dexamethasone for the treatment of COVID-19 infection. Patients who met the primary outcome had a lower admission body weight/BMI, a lower admission BG value, and were less likely to have a preexisting diagnosis of type 2 diabetes mellitus. Our study re-demonstrated the persistent challenges in glycemic control with insulin glargine among patients receiving dexamethasone.
In our study, the patients in the AGT cohort received a median insulin glargine dose of 0.14 unit/kg/day. While the insulin glargine was similar between groups, the PH cohort had roughly 4 times the amount of short-acting bolus insulin administered on day 3 of combination therapy. This further supports that those in the PH cohort had higher insulin requirements that were not being met by their selected basal insulin dosing. Based on the institutional guideline available at the time, providers were recommended to add 50% to 100% of correctional insulin requirements to the basal dose on the subsequent day. Adherence to this was not specifically evaluated in this study.
An empiric basal insulin dose reduction of approximately 50% from prior-to-admission dose was observed on day 1 of insulin glargine in both cohorts. By day 3, the AGT cohort continued to require a lower than prior-to-admission basal insulin dose while the PH cohort returned to their prior-to-admission basal insulin dose. This suggests that an empiric dose reduction may not be appropriate in many cases for patients experiencing DIH. However, it is worth noting that admission medication reconciliation was not completed by a pharmacist in all patients at our institution during the study time period so there may have been discrepancies between the documented and true basal insulin dose. In addition, adjustments in diet while in the hospital and overall clinical status may still warrant adjustments to basal insulin.
When comparing our findings with prior studies in COVID-19 populations, several methodological differences limit direct insulin dose comparisons. Fornwald et al 7 reported a mean TDD of 0.3 units/kg in the glargine group but did not specify the basal proportion, preventing comparison with our weight-based glargine dosing. In the review by Brooks et al, 9 a substantial amount of studies included in the review used intermediate-acting corticosteroids, such as prednisone or methylprednisolone, which have different hyperglycemic profiles compared with dexamethasone (hyperglycemic effect onset 4 vs 8 hours; duration 12-16 vs 24-36 hours, respectively). 14 Our observed glargine dose of 0.14 units/kg was therefore lower than the basal dose of 0.20 to 0.24 units/kg suggested by the Brooks et al 9 study, likely reflecting both the steroid differences and smaller peak effect and longer duration of insulin glargine compared with insulin NPH. In the Ketaroonrut study, patients receiving a TDD of ≤0.29 units/kg predominantly as basal insulin were reported to have the lowest treatment failure rate. However, interpretation of their findings are jeopardized by the permissive treatment-failure definition (ie, sustained BG > 280 mg/dL or any BG > 400 mg/dL), methylprednisolone use, and heterogeneous insulin strategies including both BBI and premixed insulin regimens along with variable proportions of basal insulin across the dose groups. 8
When examining across various dexamethasone indications, patients with hematologic malignancies in our study received the highest median insulin glargine dose standardized by weight, 0.23 (0.12-0.35) units/kg, but the lowest glargine dose when standardized by dexamethasone dose, 1.00 (0.34-1.78) units/mg dexamethasone, when compared with other indications. Compared with the Gosmanov et al 10 study with mean dexamethasone dose of 9 mg, our study achieved similar mean BG by day 3 of combination therapy despite using a lower weight-standardized dose of insulin glargine at 0.23 units/kg/day compared with their insulin detemir dose of 0.46 units/kg/day. On the contrary, in scenarios where much higher dexamethasone doses were administered, such as the 40 mg/day regimen reported by Brady et al, 11 hyperglycemia still persisted on 85% of patient-days despite the use of greater weight-based basal insulin doses (0.25-0.3 units/kg/day) compared with our study.
The findings from the above studies in addition to our study collectively suggest that determining the insulin glargine dose solely based on body weight may be insufficient to effectively manage DIH. Incorporating the dexamethasone dose into the dosing strategy appears to be necessary especially for patients receiving high-dose dexamethasone. In addition, standardization to steroid dose should be considered for dexamethasone specifically as opposed to conversion to prednisone-equivalent dosing given the differences in their pharmacokinetic profiles mentioned previously.
Our study also focused evaluation on initial dosing strategy given the evaluation on day 3 of combination therapy. It was observed that small differences in the initial dose of insulin glargine standardized to units/mg dexamethasone and units/mg dexamethasone/kg coincided with the divergence of the mean BG values between the 2 cohorts starting on day 1. On day 3, the difference in median standardized insulin glargine dose between the AGT and PH cohorts were not statistically significant, whether expressed as units per mg dexamethasone, 2.25 (1.08-3.33) versus 2.00 (1.17-4.00) units/mg, or units per mg dexamethasone per kg body weight, 0.03 (0.02-0.04) versus 0.02 (0.01-0.04) units/mg/kg. To help contextualize this, a 95 kg patient receiving dexamethasone 6 mg daily for treatment of COVID-19, the most common dexamethasone regimen in this study, would receive an insulin glargine dose of 14 units in the AGT cohort versus 12 units in PH cohort when calculated as units per mg of dexamethasone. Alternatively, the same 95 kg patient would receive 17 units in the AGT cohort versus 11 units, when calculated as units per mg dexamethasone per kg body weight. Although the differences in standardized insulin glargine dose may appear subtle between the cohorts, dosing insulin glargine more aggressively may prevent glycemic control from lagging behind, especially for large body weight and/or high-dose dexamethasone, considering the duration of dexamethasone may last beyond 24 hours.
Differences in baseline characteristics might also blunt the observed differences in glargine doses between the cohorts. The AGT cohort had significantly lower BMI, percentage of patients with a preexisting diagnosis of type 2 diabetes mellitus, and admission BG. These factors may have reduced the need for higher insulin glargine doses. However, both cohorts had comparable baseline HbA1c and BG values immediately prior to initiation of combination therapy, which supports reasonable comparability at the point of therapy initiation. Despite the relative dose-escalation in insulin glargine, patients in the PH cohort still failed to achieve meaningful reduction in either mean BG or prior-to-therapy BG values between days 1 and 3 of combination therapy, which highlights the necessity of higher initial insulin glargine dose and/or aggressive dose escalation.
From a safety perspective, it is reassuring that the overall incidence of hypoglycemia was low with this combination therapy. Only one patient in the AGT cohort experienced hypoglycemia on day 3 of combination therapy. Per chart review, this patient also had end-stage renal disease and low oral intake. The incidence of hypoglycemia in our study was comparable with the Gosmanov et al 10 and Brady et al 11 studies, but lower than the Ketaroonrut et al 8 and Fornwald et al 7 studies. Of note, Ketaroonrut et al 8 found that patients receiving a TDD ≥ 0.7 units/kg, with 67% administered as basal insulin, was associated with significantly higher frequency of hypoglycemia. This level of basal insulin is much higher than in our study.
Our study includes the largest number of patients to date compared with previous studies specifically evaluating the use of insulin glargine to manage DIH. It is also the first to date to evaluate insulin glargine dosing standardized to both weight and dexamethasone dose. Such strategies of standardizing insulin glargine are relevant given the high glucocorticoid potency of dexamethasone and the substantial dosing differences across different indications. A consideration in our analysis is the use of day 3 therapy as the cutoff for cohort analysis, instead of tracking time to AGT or using mean BG over the entire admission. This was an intentional decision to focus on early glycemic management strategies and initial insulin glargine dosing, while allowing time for glargine titration in response to glycemic trends. Although only a limited number of dose adjustments could be performed, this timeframe was intended to reflect the relationship between initial glargine dosing and early glycemic management rather than average glycemic control through inpatient dexamethasone therapy. Given our most common exclusion reason was patients not receiving at least 3 days of combination therapy, it is likely we would have further limited our patient population and ability to make any conclusions with a more prolonged timeline.
This analysis has several limitations and biases. The retrospective nature of this study limited the accuracy and completeness of data, especially regarding dietary information and oral intake which could impact both efficacy and safety as well as the actual dose/adherence of prior-to-admission basal insulin dose. Active infection can independently increase BG as part of the stress response and the most common indication for dexamethasone in this study was COVID-19. The observed association between dexamethasone dose and DIH severity may therefore be overestimated, which can also lead to overestimation of glargine requirements. In contrast, selection of more stable non-ICU patients and exclusion of those with extremes of hyperglycemia likely underestimated the difficulty of glycemic control and overall insulin requirements in the broader DIH population. Finally, compared with the PH cohort, the AGT cohort had different baseline characteristics, including lower BMI, less prevalence of preexisting diabetes, and overall lower eGFR, which may also have led to underestimation of the glargine dose required to achieve glycemic targets in this DIH patient population. Multivariate regression analysis and matched analysis were considered to adjust for the confounders and differences in baseline characteristics previously noted given potential impacts to glycemic control independent of insulin glargine and dexamethasone dose. However, these approaches were not performed due to the small overall sample size and marked imbalance between the 2 cohorts, which would have produced highly unstable, low precision estimates and would not meaningfully improve confounding control. Therefore, the observed associations from this study should be viewed as hypothesis-generating.
In terms of generalizability and applicability, the study only included non-ICU patients, with typical BMI around 30 kg/m2 and without extreme hyperglycemia at baseline. Applicability is further limited by the exclusion of dexamethasone dose changes, administration of twice-daily insulin glargine and/or twice-daily or 4-times-daily dexamethasone, despite these approaches being commonly used in clinical practice. These exclusions were due to limitations in defining therapy days as well as the difficulty in controlling dose stacking effects of dexamethasone and insulin glargine given their duration of effect can persist for 24 hours or longer. Allowing more than once-daily dosing of either agent or dexamethasone dose changes during the analysis period may have precluded establishing dose-response relationship among dexamethasone dose, insulin dose, and glycemic outcomes, especially because this study focused on evaluating initial insulin glargine dosing strategies. Therefore, caution should be used when applying findings from our analysis to a broader population or to more complex insulin glargine and dexamethasone regimens, as their glycemic effect can overlap over time due to a longer half-life.
Several angles for future studies can be explored. Matched cohort studies are needed to evaluate standardized insulin glargine doses after balancing patient weight, dexamethasone dose, and other factors such as HbA1c and renal function. For once-daily dexamethasone, further investigation is needed to evaluate whether twice-daily insulin glargine administration at the same total daily glargine dose provides additional glycemic control benefit compared with once-daily administration, given the potential for overlapping hyperglycemic effect from consecutive dexamethasone doses that may persist beyond 24 hours. After optimal glargine to once-daily dexamethasone dose ratios are established, further research could evaluate the optimal timing and frequency of glargine administration for patients receiving twice-daily or 4-times-daily dexamethasone given their common use in clinical practice.
Conclusion and Relevance
In summary, achieving early glycemic control with insulin glargine for DIH remains challenging. Observations from this analysis suggest that current practice for initial insulin glargine dosing may be overly cautious and rely heavily on reactive bolus insulin with limited success. This study supports more assertive initial insulin glargine dosing strategies to proactively mitigate DIH without introducing significant risk of hypoglycemia. This approach appears particularly relevant for patients with higher BMI and receiving higher dexamethasone doses, where timely achievement of optimal glycemic control can be more difficult. Collectively, these findings suggest a need to shift clinical practice away from reactive insulin escalation and toward anticipatory, basal insulin strategies that factor in both patient weight and dexamethasone dose.
Footnotes
Acknowledgements
None.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Ethics Committee of The Ohio State University (approval #2023H0360) on October 22, 2023 with the need for written informed consent waived. This is an IRB-approved retrospective study, all patient information was de-identified, and patient consent was not required. Patient data were not shared with third parties.
Consent to Participate
The IRB determined that this research involved minimal risk and approved a waiver for informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Yijie Cheng, Dr Joshua Gaborcik, Dr Rachel Smith, and Dr Andrew Stone have declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Kathleen Dungan has disclosed that she serves as a consultant/member of the advisory board for Eli Lilly, Insulet, and Dexcom Oppenheimer, has received an honorarium from Medscape, Impact Education, Academy for Continued Healthcare Learning, Elsevier, and UptoDate, and has received grant funding from Insulet, Dexcom, Abbott, and Endogenex.
Data Availability Statement
The data underlying this study cannot be shared because they contain protected patient health information and are subject to Institutional Review Board and the Health Insurance Portability and Accountability Act regulations.