
Abstract
Objective:
Urinary tract infections (UTIs) are the most common infection in kidney transplant recipients (KTRs), and the large increase in antibiotic-resistant pathogens is minimizing effective treatments. The objective of this study was to evaluate the safety and efficacy of fosfomycin for the treatment of culture-positive lower UTIs in KTRs.
Data Resources:
A systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards was conducted through June 2025 on Embase, PubMed, Cochrane Central Register of Controlled Trials, Web of Science Core Collection, and the Global Index Medicus.
Study Selection and Data Extraction:
The terminology used to create the search included UTIs and synonyms, fosfomycin and synonyms, and kidney transplant and synonyms. Patients with culture-positive lower UTIs, defined as either cystitis or asymptomatic bacteriuria and with documented clinical and microbiological cure data were included. Records with non-human, non-English, adolescents or children (<18), fosfomycin prophylaxis only, or upper UTI-only analyses were excluded.
Data Synthesis:
Six studies were included for data analysis. A total of 564 culture-positive lower UTI episodes in KTRs were treated with fosfomycin monotherapy. Treatment regimens were generally multi-dose with various frequencies and durations. All studies reported results in the form of clinical cure, microbiological outcomes, and treatment-emergent adverse effects. Many of the causative pathogenic bacteria in the treatment intervention were multi-drug resistant (MDR) in nature.
Relevance to Patient Care and Clinical Practice:
The adequate treatment of UTIs in KTRs is imperative to long-term graft success, low mortality rates, and cost savings. Further randomized controlled trials (RCTs) are needed to assess fosfomycin use for MDR UTIs in this population. In aggregate, oral fosfomycin as monotherapy for UTIs in KTRs demonstrated positive outcomes regarding clinical cure, microbiological outcomes, and treatment-emergent adverse effects.
Keywords
Background
Among kidney transplant recipients (KTRs), urinary tract infections (UTIs) are the most common types of infections. In the first year after transplant, an estimated 74% of patients experience at least 1 UTI episode. Concomitant risk factors that increase this likelihood include age >65 years, female sex, history of UTI, immunosuppressed status, diabetes mellitus, and extended dialysis. Gram-negative bacteria are most commonly the causative pathogen (>70%), with increasing antimicrobial resistance rates threatening the drug treatment in immunocompromised patient populations. 1 Antibiotic-resistant pathogens are estimated in 30% to 80% of patients who are pre- or post-transplant, fluctuating based on bacteria and transplant type. 2
The Infectious Disease Society of America (IDSA) Guideline Update on Complicated Urinary Tract Infections describe 6 first-line treatment options: nitrofurantoin, trimethoprim-sulfamethoxazole, fosfomycin trometamol (tromethamine), pivmecillinam, fluoroquinolones, and beta-lactams (Trautner et al 2025). 3 International definitions of complicated UTIs, such as those made by the American Urological Association (AUA), European Association of Urology (EAU), and Centers for Disease Control and Prevention (CDC) vary and can lead to differing treatment approaches and options.4-7 These guidelines classify UTIs in KTRs as complicated based on their immunocompromised state. On the contrary, transplant-specific guidelines allow KTRs to fall into the uncomplicated classification. The Guidelines from the American Society of Transplantation (AST) Infectious Diseases Community of Practice classify UTIs as uncomplicated vs complicated by clinical symptoms, laboratory findings, and the presence of severe syndromes. Severe syndromes can include structural/functional irregularity of the genitourinary tract (beyond standard transplantation reconstruction), involving associated organs such as prostatitis, in-dwelling ureteric stents, bladder catheters, or nephrostomy tubes. 4 AST Infectious Disease Guidelines indicate that therapy for cystitis should consist of a third-generation oral cephalosporin OR amoxicillin-clavulanate OR a fluoroquinolone (ciprofloxacin or levofloxacin), OR nitrofurantoin (CrCl >30). Complicated UTI empiric treatment does not include fosfomycin, and several AST Infectious Disease authors do not recommend its use in pyelonephritis due to rapid development of bacterial resistance. 4
Fosfomycin trometamol (tromethamine) is a broad-spectrum antimicrobial agent that was approved by the Food and Drug Administration (FDA) in 1996 for the treatment of uncomplicated cystitis caused by Escherichia coli (E. coli) or Enterococcus faecalis (E. faecalis) in females. 8 The standard treatment regimen consists of a single 3-g dose of fosfomycin trometamol (tromethamine) given orally; however, additional salt forms and routes of administration exist. 9 There has been a restored renewed interest in fosfomycin in the last decade due to the increase in in vitro data demonstrating promising activity in the treatment of multi-drug resistant (MDR) infections. 10 Dose adjustments based on altered kidney function are not required for single-dose regimens, although an extended elimination period can occur with a CrCl of <50 mL/min. 9 Most common adverse effects include headache, diarrhea, vaginal infection/discharge, and upset stomach. 11 Relevant drug interactions to an immunocompromised patient include immune checkpoint inhibitors (anti-PD-1, PD-L1, CTLA4) and mycophenolate, in that fosfomycin may decrease plasma levels of these agents. 9 The AST Infectious Diseases Guidelines express the need for further research in oral treatment options for MDR organisms, specifically fosfomycin as a “promising candidate.” 4
A recent single-center study in Germany conducted over 10 years assessed the antibiotic resistance of urinary pathogens after kidney transplantation. An increase in the rate of infections caused by extended-spectrum beta-lactamases (ESBL) Klebsiella pneumoniae (K. pneumoniae) and MDR Pseudomonas aeruginosa (P. aeruginosa) has been observed. Specifically, an increase in ESBL E. coli was seen until 2020, with a declining trend thereafter. 12 Two randomized controlled trials (RCTs) have been performed to assess the use of fosfomycin for UTI prophylaxis, yet no RCTs have been performed to assess UTI treatment in this patient population.13,14 Systematic reviews assessing UTIs in KTRs have been published reviewing overall MDR prevalence, risk factor interventions, and other treatment regimens or indications, although the use of fosfomycin in this setting remains poorly elucidated in the literature. This systematic review was performed to assess the safety and efficacy of oral fosfomycin for the treatment of culture-positive lower UTIs in KTRs.
Materials and Methods
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards on the efficacy and safety of fosfomycin for the treatment of culture-positive lower UTIs in KTRs. 15 An extensive search strategy to identify reports was constructed in Embase with the assistance of an experienced health sciences librarian (WL-S), using phrases, truncated keywords, subject headings, and proximity searching. The strategy was converted to PubMed, the Cochrane Central Register of Controlled Trials, the Web of Science Core Collection, and the Global Index Medicus. The terminology used to create the search included UTIs and synonyms, fosfomycin and synonyms, and kidney transplant and synonyms. The search included documents published and indexed through June 2025, using the terminology specified in Supplemental Appendix Table 1. Two authors (SP and JPR) were responsible for executing the search and data extraction, with a third participant being consulted in the event of disagreement. No other limitations were applied to the search databases. Specific phrases such as “treatment” and “culture-positive” were not utilized in the search due to restricting results. Figure 1 depicts the search strategy.
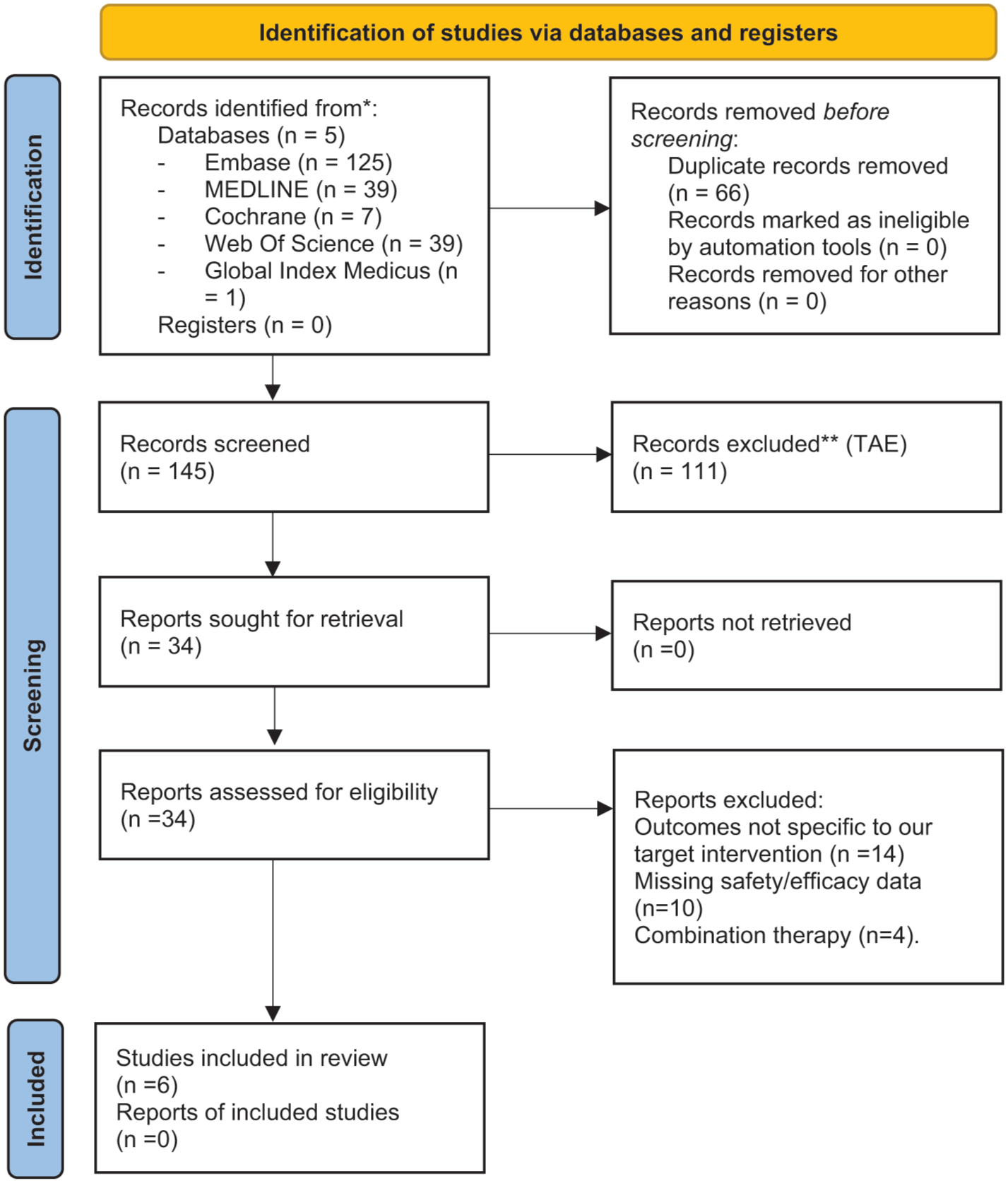
PRISMA search methodology. 15
All results were exported into SciWheel, and duplicates were removed by SciWheel’s duplicate detection algorithms and followed by a manual assessment. Screened records were included if they reported efficacy and safety results of the desired study population in the form of clinical cure, microbiological outcomes, and treatment-emergent adverse effects. Clinical and microbiological cures were extrapolated from the author’s terminology, which varied between studies. Sex and age categories were not unanimously reported.
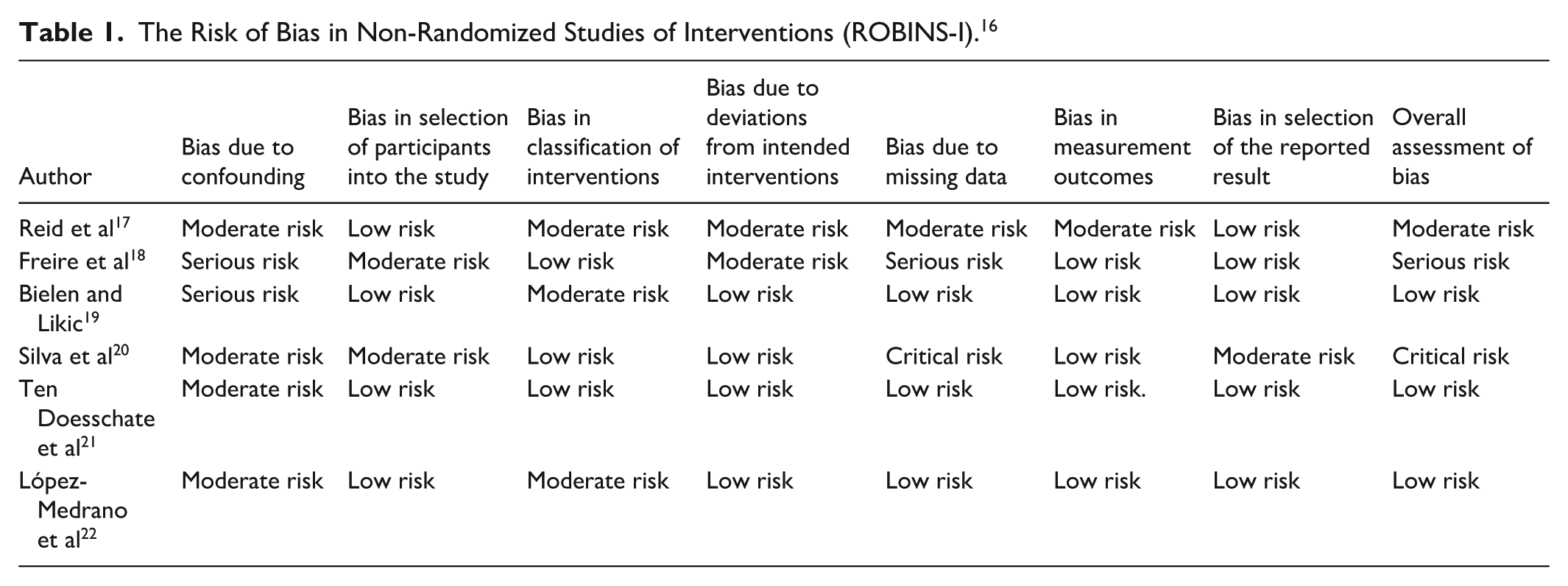
Defining clinical and microbiological outcomes was variable among the studies. For the scope of this review, patients with culture-positive lower UTIs, defined as either cystitis or asymptomatic bacteriuria (AB) and with documented clinical and microbiological cure data were included. Records with non-human, non-English, adolescents or children (<18), fosfomycin prophylaxis only, or upper UTI-only analyses were excluded. The Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool was completed by the 2 authors (SP and JPR) with a medical reference librarian (WL-S) being used to arbitrate conflicting results. The ROBINS results can be viewed in Table 1. 16
The Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I). 16
Results
Following the search strategy and application of inclusion and exclusion criteria, a total of 6 articles were included in this review. Bias was found to be moderate or serious for all included studies, stemming from heterogeneity of definitions and thresholds for diagnosis, clinical and microbiological cure, and characterization of UTI’s within each report. Both men and women were included in the referenced studies. A summary of findings can be viewed in Table 2.
Results.
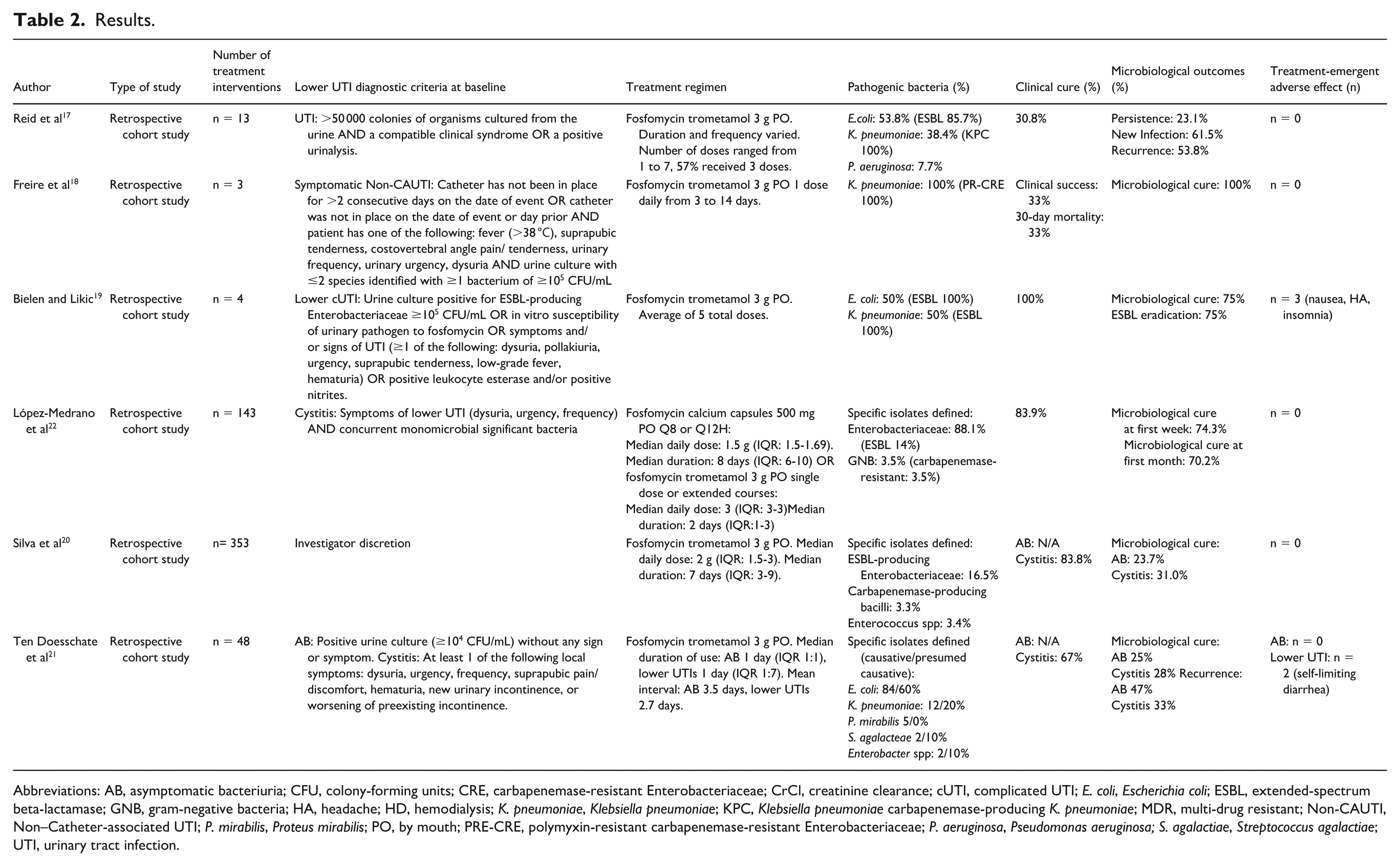
Abbreviations: AB, asymptomatic bacteriuria; CFU, colony-forming units; CRE, carbapenemase-resistant Enterobacteriaceae; CrCl, creatinine clearance; cUTI, complicated UTI; E. coli, Escherichia coli; ESBL, extended-spectrum beta-lactamase; GNB, gram-negative bacteria; HA, headache; HD, hemodialysis; K. pneumoniae, Klebsiella pneumoniae; KPC, Klebsiella pneumoniae carbapenemase-producing K. pneumoniae; MDR, multi-drug resistant; Non-CAUTI, Non–Catheter-associated UTI; P. mirabilis, Proteus mirabilis; PO, by mouth; PRE-CRE, polymyxin-resistant carbapenemase-resistant Enterobacteriaceae; P. aeruginosa, Pseudomonas aeruginosa; S. agalactiae, Streptococcus agalactiae; UTI, urinary tract infection.
Efficacy
Three studies assessed outcomes under a comprehensive UTI definition and did not directly report based on AB or cystitis individually. In Reid et al, 13 UTI episodes were treated with fosfomycin monotherapy in 9 KTRs. The median time to infection post-transplantation was 52.5 months (range = 1-110 months). Fosfomycin was used as a salvage therapy in 57.1% of episodes. Nearly 85% of causative pathogens were MDR; a vast majority were represented by ESBL E. coli and K. pneumoniae carbapenemase-producing K. pneumoniae (KPC-KP). Clinical cure was demonstrated with a 30.8% clearance rate. Regarding microbiological outcomes, infectious persistence was seen in 23.1% of patients, new infections in 61.5%, and recurrence in 53.8%. Non-MDR pathogens were identified in 62.5% of new infections. 17 Furthermore, in Freire et al, 3 patients in a study group of 40 KTRs with a UTI episode were treated with fosfomycin monotherapy. One patient had a combination pancreas-kidney transplant. The median time to infection post-transplantation was 3.1 months (range = 0.2-172 months). All 3 patients were infected with polymyxin-resistant carbapenemase-resistant Enterobacteriaceae (PRE-CRE). Clinical cure was demonstrated by a 33% clinical success and a 33% mortality at 30 days. The microbiological cure rate of survivors was 100%. 18 In Bielen and Likic, 4 KTRs out of 42 patients treated for a UTI were managed with fosfomycin monotherapy in a study group of 42 patients. All episodes in the KTR assessed group were recurrent UTIs, and 80% of the total episodes were recurrent. All 4 causative pathogens were MDR, with 2 being ESBL E. coli isolates and the remaining 2 ESBL K. pneumoniae isolates. Clinical cure revealed a 100% success rate. Microbiological cure and ESBL eradication were both 75%. Resistance to fosfomycin was demonstrated in 5% of patients post-treatment. 19 Only one of 6 studies assessed their outcomes in the cystitis-only population. In López-Medrano et al, 143 UTI episodes were treated with fosfomycin monotherapy in 133 KTRs. The median time to infection post-transplantation was 15.7 months (IQR = 3.4-75.9). Around 43% were recurrent episodes, and fosfomycin was used as salvage therapy in approximately 17% of total episodes. Around half the episodes were due to MDR organisms, mostly ESBL-producing Enterobacteriaceae. Clinical cure was seen in 83.9% of patients. The microbiological cure was 74.3% within the first week post-treatment and 70.2% within the first month post-treatment. 22 There was no significant difference in outcomes between investigator-defined first-line vs salvage therapy; clinical cure (P = .199) and microbiological cure in the first week (P = 1) or in the first month (P = 1). This was the only study that treated patients with fosfomycin calcium – a different oral formulation than fosfomycin trometamol (tromethamine). No difference was found in achieving a clinical cure between fosfomycin formulations or between repeated daily-dose and single-dose regimens. In addition, there was no clear relationship between the treatment regimen and adverse effects. 22
Two studies assessed their outcomes in 2 different subgroups, AB and cystitis. In Silva et al, 353 UTI episodes were treated with fosfomycin monotherapy in 326 KTRs. Almost 12% of cases were following the failure of a previous antibiotic. Nearly all causative pathogens were gram-negative, with over half of those representing MDR species. Clinical cure was seen in 83.8% of cystitis patients but was not assessed in AB patients. Microbiological outcomes were assessed based on repeat urine cultures. In cystitis patients, 39.4% had a urine culture performed within 2 weeks after stopping treatment. Of those, 78.6% of cultures were sterile, resulting in 31% of total patients demonstrating microbiological cure. In AB patients, 48.3% had a urine culture performed within 2 weeks after stopping treatment, and 50.5% of those cultures were sterile, resulting in 23.7% of total patients demonstrating microbiological cure. 20 In Doesschate et al, 48 UTI episodes in 40 KTRs were treated with fosfomycin monotherapy. All episodes utilized fosfomycin as the initial UTI treatment. About 30% of causative pathogens were ESBL positive, although none were carbapenem-resistant Enterobacterales (CRE) positive. Clinical cures were seen in 67% of cystitis patients and were not assessed in AB patients. Microbiological outcomes demonstrated a microbiological cure of 25% in AB and 28% in lower UTIs. In addition, recurrence was 47% for AB and 33% for lower UTIs. Fosfomycin-acquired resistance was discovered in 6 episodes. 21
Safety
Adverse effects were reported in terms of incidence and severity. Regarding treatment-emergent adverse effects, 4 of the 6 studies did not report any adverse effects from fosfomycin. Specifically, Reid et al reported that there was no notable difference in creatinine between pre- and post-therapy. In addition, no patients developed systemic infection. 17 The 2 studies that reported adverse events were conducted by Bielen and Likic and Silva et al. Bielen and Likic 19 reported 3 non-serious adverse effects including nausea, headache, and insomnia; however, these effects were not specific to KTRs. Silva et al 20 reported no serious adverse events, with only 2 patients in the lower UTI group experienced self-limiting diarrhea. Reid et al 17 found no notable difference in serum creatinine between pre- and post-therapy, and no patients developed systematic infection.
Discussion
The results of this systematic review document the efficacy and safety of oral fosfomycin for the treatment of culture-positive lower UTIs in KTRs. Many systematic reviews presented in the literature were published to assess the use of FDA-approved indication for uncomplicated UTIs. The paucity of data reviewing options for complicated UTIs, including those with an immunocompromised host such as KTRs, remains a clinical concern. Acute graft rejection is estimated to occur in ~10% of patients within 1 year after kidney transplantation, without regard to the presence or absence of infection. 23 A study that linked infections in kidney transplant patients to negative allograft and patient survival found UTIs as the most common infection. 24 The time to infection post-transplantation varied greatly among the 3 studies that reported these data. Although concomitant immunosuppressive usage is not suitably detailed in the studies, it can be contemplated that the variation in infection onset could be impacted by differences in immunosuppressant therapy among participants. The need for continuing studies is especially highlighted in the era of antimicrobial resistance, where effective treatments have become limited. The results analyzed in this review were performed in Brazil, Croatia, the Netherlands, Spain, and the United States, demonstrating the applicability in this global public health crisis.17-22 Many of the pathogens isolated were of MDR nature, allowing the results from this review to be generally extrapolated to cases associated with highly resistant pathogens, including ESBL, KPC, and CRE-producing isolates. In aggregate, fosfomycin had positive outcomes, evidenced by a significant number of cases demonstrating clinical cure, microbiological cure, and non-serious adverse effects. To our knowledge, this is the first systematic review performed to assess the efficacy and safety of oral fosfomycin for the treatment of culture-positive lower UTIs in KTRs.
Due to the complicated nature of these infections, multi-dose regimens were utilized in all studies; the majority of patients from the included studies received at least 5 doses of an oral fosfomycin product. The frequency and duration of treatment varied among the studies; both oral fosfomycin trometamol (tromethamine) 3 g and fosfomycin calcium 500 mg were prescribed. Although it is not unanimously clear from these studies the effect that treatment regimens have on efficacy, 1 study found no difference in outcomes between formulations or single- vs multi-dose regimens. 22 It can be hypothesized that regardless of the dose, fosfomycin causes minimal treatment-emergent adverse effects, especially to a serious degree, as evidenced by our results. Adverse effects relating to renal toxicity were either not assessed or not present in our study population. A study looking at fosfomycin combination and monotherapy for UTIs caused by MDRs reported that no patients needed new renal replacement therapy (RRT) after fosfomycin treatment. 25 One study in our review assessed and found no evidence of systemic infection after fosfomycin therapy. Although not assessed in our review, the use of fosfomycin in upper UTIs, specifically pyelonephritis, is an area of uncertainty. Current guidelines recommend against fosfomycin treatment in pyelonephritis, but studies looking at its use as a step-down treatment have been performed and demonstrated efficacy.
Although there is promising evidence supporting the use of fosfomycin, including respectable clinical outcomes and minimal adverse effects, clinicians should also consider the need for additional antimicrobial therapy as well as the potential, theoretical decrease in efficacy of concomitant immunosuppressive drugs. This is especially important when attempting to minimize the development of fosfomycin resistance and maintain the received kidney functionality, respectively. Two studies reported post-treatment fosfomycin resistance, noting an average resistance of approximately 7% rate in 91 UTI episodes. The global fosfomycin resistance rate continues to evolve along with renewed interest in the medication.
Although studies assessing the treatment of AB in KTRs do not demonstrate clear evidence, the AST Infectious Disease Guidelines recommend against routine treatment of AB. 4 The decision to include studies that assessed fosfomycin treatment for AB in our review was due to the lack of consistent separation in the literature. Nonetheless, it can be perceived from our results that the AB results demonstrated lower microbiological efficiency than comprehensive UTI or cystitis-specific results. This supports the current recommendation and should be considered by clinicians to determine the necessity of AB treatment in KTRs.
When approaching the treatment of infections in any patient population, it is apparent that symptomatic and microbiological resolution are the focus of treatment. This is especially imperative in patients with a history of transplantation, as the risk of graft rejection is a crucial concern. The true impact of UTIs alone on long-term graft survival is conflicting, but an 11-year study published in 2016 found that UTIs within the first year post-transplantation had a 41% increase in mortality and a 29% increase in allograft loss. First-year post-transplantation costs also increased to approximately $17 000 in patients requiring treatment for a UTI. 26 Additionally, a UTI without sufficient treatment can progress into severe infections including pyelonephritis and urosepsis, which are risk factors affecting graft and patient survival. 27 Acute graft pyelonephritis has been demonstrated to be independently associated with an increased risk of graft loss. 28
In addition, the effect of UTIs on long-term graft survival has been studied more recently in recurrent UTIs. A retrospective cohort study performed from 2017 to 2020 reported that the recurrence of symptomatic UTIs within the first year after a kidney transplant has a long-term consequence effect on graft function. In the same cohort, development of a UTI within the first year was associated with an approximately 60% increase in the risk of UTI recurrence. 29 Fosfomycin usage varied among the studies in this review, as fosfomycin was used as initial treatment, salvage treatment, as well as treatment for recurrent UTIs. One study that utilized fosfomycin as initial treatment demonstrated a low microbiological cure rate. Although a direct comparison to cases where fosfomycin was used after initial antibiotic treatment was not performed, the authors recommended fosfomycin use for difficult-to-treat cases including recurrent UTIs. 21 On the contrary, another study directly compared fosfomycin as initial therapy vs salvage therapy and found no significant difference in clinical or microbiological outcomes. 22 Two studies in our review assessed recurrence rates post-transplant specifically, ranging from 33% to 54%, respectively. More studies are needed to assess the prevalence of recurrence rates after fosfomycin treatment.
There are several limitations that warrant discussion related to this work. Significant heterogeneity exists in the data set identified in this systematic review, both in regard to definitions of UTI diagnostic criteria and the number of patients enrolled in each study. Assessed bias of the studies adds a confounding variable that must be considered in the context of these results. This made the process of including and excluding studies difficult, especially in this case, where upper UTI data were excluded. We attempted to minimize the effects of this limitation by combining AB and cystitis into 1 group defined as culture-positive lower UTIs. Also, the small sample size of this review could be deemed a limitation. In the case of limited supportive evidence available in this patient population, extrapolation of results may be difficult. Further research in the realm of MDR UTI treatment for kidney transplant patients is a necessity. Studies of RCT nature analyzing fosfomycin use for MDR culture-positive lower UTIs would be immensely beneficial to examine the causal relationship between fosfomycin treatment and clinical and microbiological outcomes. When assessing the study’s individual biases, it is important to note the presence of one study with an overall assessment of serious risk and another study deemed critical risk.
Relevance to Patient Care and Clinical Practice
Urinary tract infections in KTRs represent a frequent and clinically consequential challenge, with implications that extend beyond short-term symptom burden to long-term graft and patient survival. Given the high prevalence of MDR gram-negative organisms in this population, clinicians are often confronted with limited oral treatment options. The findings of this systematic review suggest that fosfomycin may offer a valuable, kidney-sparing alternative for patients with culture-positive lower UTIs, particularly when resistance or intolerance limits standard therapies.
From a practical standpoint, fosfomycin’s favorable safety profile is highly relevant in transplant care. Across the included studies, treatment-emergent adverse effects were infrequent and generally mild, with no consistent signal of nephrotoxicity or deterioration in graft function. In a population where preservation of renal function is paramount and calcineurin inhibitor exposure already poses nephrotoxic risk, an oral agent that does not require dose adjustment for reduced kidney function when administered as a single dose and demonstrates minimal renal adverse effects is clinically attractive. Evaluation of dose adjustments in patients requiring multiple doses requires further evaluation. Furthermore, the lack of significant systemic complications in most reports supports its consideration in carefully selected lower UTI cases.
Efficacy outcomes varied across studies but were generally encouraging in cystitis-specific cohorts, with several demonstrating substantial clinical cure rates even in the presence of MDR pathogens, including ESBL-producing Enterobacterales. These data support current guideline suggestions that fosfomycin be reserved for difficult-to-treat or MDR cystitis rather than routine first-line use.
An intravenous formulation of fosfomycin was approved for use in the United States in late 2025, although its defined role in the clinical space has not yet been extensively published in the literature. It would be reasonable to assume comparable outcomes with the data presented in this systematic review and would be most appropriate in patients without enteral access.
While current evidence does not support its use in pyelonephritis, fosfomycin may serve as an oral option for lower UTIs when other agents are contraindicated or ineffective. As antimicrobial resistance continues to narrow therapeutic choices, fosfomycin represents a potentially important adjunct, pending further high-quality RCTs.
Conclusion
Fosfomycin is FDA-approved for the treatment of uncomplicated cystitis in women; however, it is commonly used for other infections of the urinary tract. The AST Infectious Disease Guidelines Community of Practice recommends fosfomycin for the treatment of MDR cystitis. This review sought to identify the efficacy and safety of fosfomycin for the treatment of culture-positive lower UTIs. After applying the methodology and appropriate filters, 6 articles were discovered to have met the inclusion and exclusion criteria. Overall, fosfomycin as monotherapy in this population demonstrated positive outcomes regarding clinical cure, microbiological outcomes, and treatment-emergent adverse effects.
Supplemental Material
sj-xlsx-1-aop-10.1177_10600280261457449 – Supplemental material for The Safety and Efficacy of Oral Fosfomycin for the Treatment of Culture-Positive Lower Urinary Tract Infections in Kidney Transplant Recipients: A Systematic Review
Supplemental material, sj-xlsx-1-aop-10.1177_10600280261457449 for The Safety and Efficacy of Oral Fosfomycin for the Treatment of Culture-Positive Lower Urinary Tract Infections in Kidney Transplant Recipients: A Systematic Review by Sadie Pyle and Justin P. Reinert in Annals of Pharmacotherapy
Footnotes
Acknowledgements
The authors would like to recognize Wade Lee-Smith, BS, MLS, for his efforts in assisting with the systematic search strategy development and execution.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.