
Abstract
Background:
Lyme carditis is a cardiovascular complication of early disseminated Lyme disease. Although guidelines recommend treatment with ceftriaxone followed by doxycycline, limited data support this recommendation.
Objective:
The purpose was to describe treatment strategies and outcomes of hospitalized patients treated for Lyme carditis.
Methods:
An institutional review board-approved, retrospective descriptive study was conducted within a large hospital network in an endemic region. Adults admitted with Lyme carditis were included. Outpatients, patients from external hospitals, or those without treatment were excluded. Electronic health record review was performed. The primary outcome was 30-day readmission; secondary outcomes included antibiotic days of therapy (DOT), length of stay (LOS), cardiac pacing, degree of heart block, PR interval reduction, and 30- or 90-day mortality. Data were analyzed using descriptive statistics.
Results:
Sixty-two patients (80.6% male, 93.5% white, median 47 years) were included with a median 4-day LOS; 28 (45.2%) had an intensive care unit admission. Fourteen (22.6%) received ceftriaxone alone for a median 28 DOT; 41 (66.6%) received a median 5 DOT ceftriaxone followed by 20 DOT doxycycline. Fifty-seven (91.9%) experienced heart block, 18 (29.0%) required temporary pacing, and 10 (16.1%) required a permanent pacemaker. A 7.3% reduction in median PR interval was observed from presentation to discharge. Three (4.8%) patients experienced Lyme carditis-related 30-day readmission. No mortality was observed.
Conclusions and relevance:
Readmission among patients treated for Lyme carditis was low across antibiotic regimens. This represents one of the largest analyses to evaluate Lyme carditis treatment and outcomes for hospitalized patients, helping clinicians better understand expected outcomes and management timelines.
Background/Introduction
Lyme disease, caused by Borrelia burgdorferi, is the most common tick-borne illness in the United States. 1 The earliest and most prevalent manifestation of Lyme disease is the erythema migrans (EM), a bulls-eye appearing rash. 2 If left untreated, Lyme disease can progress to serious complications including carditis, arthritis, and/or neurological complications such as neuroborreliosis. 3 Although approximately 30 000 cases of Lyme disease are reported yearly in the United States, with a majority of cases originating in the Midwest and Northeast, the true incidence is estimated to be approximately 476 000 cases yearly due to vast underreporting of the disease. 3
Lyme carditis is a rare and potentially fatal manifestation of early disseminated Lyme disease, with recent data suggesting an incidence of approximately 1% of all cases of Lyme disease in the United States and 10% of cases in hospitalized patients.4-7 It occurs when bacteria enter heart tissue, leading to disruption of electrical conduction and often atrioventricular (AV) block. An initial PR interval >300 ms at presentation is considered to be a high-risk marker of progression to complete AV block. 8 Suspicion for Lyme carditis is heightened in patients with symptoms of dizziness, palpitations, and syncope. 9 Although electrocardiogram and serology tests such as enzyme-linked immunosorbent assay (ELISA) and Western Blot tests can be utilized to aid diagnosis, clinical manifestations of Lyme carditis are the primary diagnostic drivers. 9
According to Infectious Disease Society of America (IDSA) guidelines 10 and European Society of Cardiology (ESC) guidelines, 11 preferred initial treatment for hospitalized patients with Lyme carditis is intravenous (IV) ceftriaxone followed by oral (PO) antibiotics with clinical improvement. PO antibiotics such as doxycycline, amoxicillin, and cefuroxime are preferred for use in hospitalized patients responding to initial therapy as well as for treatment in the outpatient setting.10,11 Both IDSA and ESC guidelines suggest 14 to 21 days of total antibiotic therapy.10,11 Patients who experience high-degree heart block may require further intervention such as cardiac pacing to help reduce cardiac complications.10,11 Guideline recommendations for treatment of Lyme carditis are based upon limited evidence of a small number of patients in trial subgroup analyses, case reports, and/or observational data.12 -14 Given these recommendations are based on low-quality evidence, a single preferred treatment strategy has not been well established, and comparative outcomes across treatment strategies are not well understood. Accordingly, the objective of this study was to describe treatment regimens and outcomes of hospitalized patients with Lyme carditis.
Method
Study Design and Setting/Data Source
This study was a retrospective, multicenter, descriptive study. Data were collected through electronic health record (EHR) review of a health network located in Western Pennsylvania, an endemic region for Lyme disease. 15 The study was classified as exempt by the relevant institutional review board.
Patient Selection and Study Outcomes
Since there is no ICD-10 (International Classification of Diseases, 10th Revision) code that is exclusively specific to Lyme carditis, patients were identified using Systematized Nomenclature of Medicine—Clinical Terms (SNOMED-CT) codes for diagnosis of Lyme carditis, either as a portion of patient diagnosis or medical history sections within the EHR. A list of patients associated with this specific SNOMED-CT code was generated for hospital encounters between January 1, 2016 and May 1, 2024.
Adult hospitalized patients treated for Lyme carditis were selected for this study, including patients with emergency department (ED) admissions for short-stay or observation unit visits. Patients who did not receive antibiotics, did not get admitted from the ED, treated exclusively in the outpatient setting, or treated for Lyme carditis at a non-network hospital for >48 hours prior to in-network hospital admission were excluded. Patients without documented treatment completion, including those who continued care at an out-of-network facility, were excluded. The primary outcome of this study was 30-day readmission rates for persistent or worsening Lyme carditis. Secondary outcomes included antibiotic days of therapy (DOT), length of stay (LOS), need for cardiac pacing, degree of heart block, PR interval duration, and 30- or 90-day mortality.
Patients were stratified into one of three treatment groups based on antibiotic regimen: ceftriaxone only, ceftriaxone with transition to PO doxycycline, and other/combination therapy. Patients were allocated into the ceftriaxone only group if ceftriaxone was exclusively given in the inpatient and (if applicable) outpatient setting. If a patient received less than 2 sequential days of antibiotic therapy by a single agent or if they received only PO doxycycline or amoxicillin, they were included in the other/combination therapy group.
Data Collection and Analysis
Data were obtained through chart review by the research team. Patient demographics and clinical characteristics were collected, including age, sex, race/ethnicity, height, weight, insurance type, LOS, intensive care unit (ICU) admission, month of hospital admission, cardiovascular (CV) comorbidities prior to admission, home medications, and blood pressure and heart rate (HR) measures upon admission. A suspicious index in Lyme carditis (SILC) criteria score was calculated for each patient by collecting relevant data from the EHR; this tool helps to estimate the likelihood of Lyme carditis in patients. 16 It is assigned by assessing the presence of constitutional symptoms, outdoor activity or location in an endemic area, patient sex and age, tick exposure, and presence of an EM rash. 16 Based on these variables, patients are stratified into low, intermediate, and high pretest probabilities of Lyme carditis. 16 Additional pertinent CV findings (troponin, PR interval, AV block) and Lyme-relevant laboratory values (serology testing, erythrocyte sedimentation rate [ESR], and c-reactive protein [CRP]) were collected; EHR documentation from medical teams such as infectious diseases, cardiology, and electrophysiology were reviewed for relevant details and context. Inpatient antibiotic doses, intervals, and DOT were recorded. Outpatient antibiotic prescriptions were recorded from discharge summary documentation and confirmed during in-network follow-up appointments for regimen changes or treatment completion.
Patient demographics, clinical characteristics, and outcomes were descriptively analyzed for the sample as a whole in addition to the stratified treatment subgroups. Continuous variables were represented by median ± interquartile range (IQR). The limited subset of patients who experienced readmission due to Lyme carditis were narratively highlighted as a concise case series for pertinent characteristics and outcomes.
Results
Patient Characteristics
A total of 143 patients were reviewed, with a final sample of 62 (43.4%) patients included in this study. Reasons for exclusion included no diagnosis of Lyme disease, lack of CV involvement, exclusive outpatient or out-of-network treatment, among others (Figure 1). Stratified by treatment group, a total of 14 (22.6%) patients received ceftriaxone only, 41 (66.1%) patients received ceftriaxone transitioned to PO doxycycline, and 7 (11.3%) received other/combination antibiotics including doxycycline prior to ceftriaxone (n = 4), doxycycline monotherapy (n = 2), and amoxicillin monotherapy (n = 1).
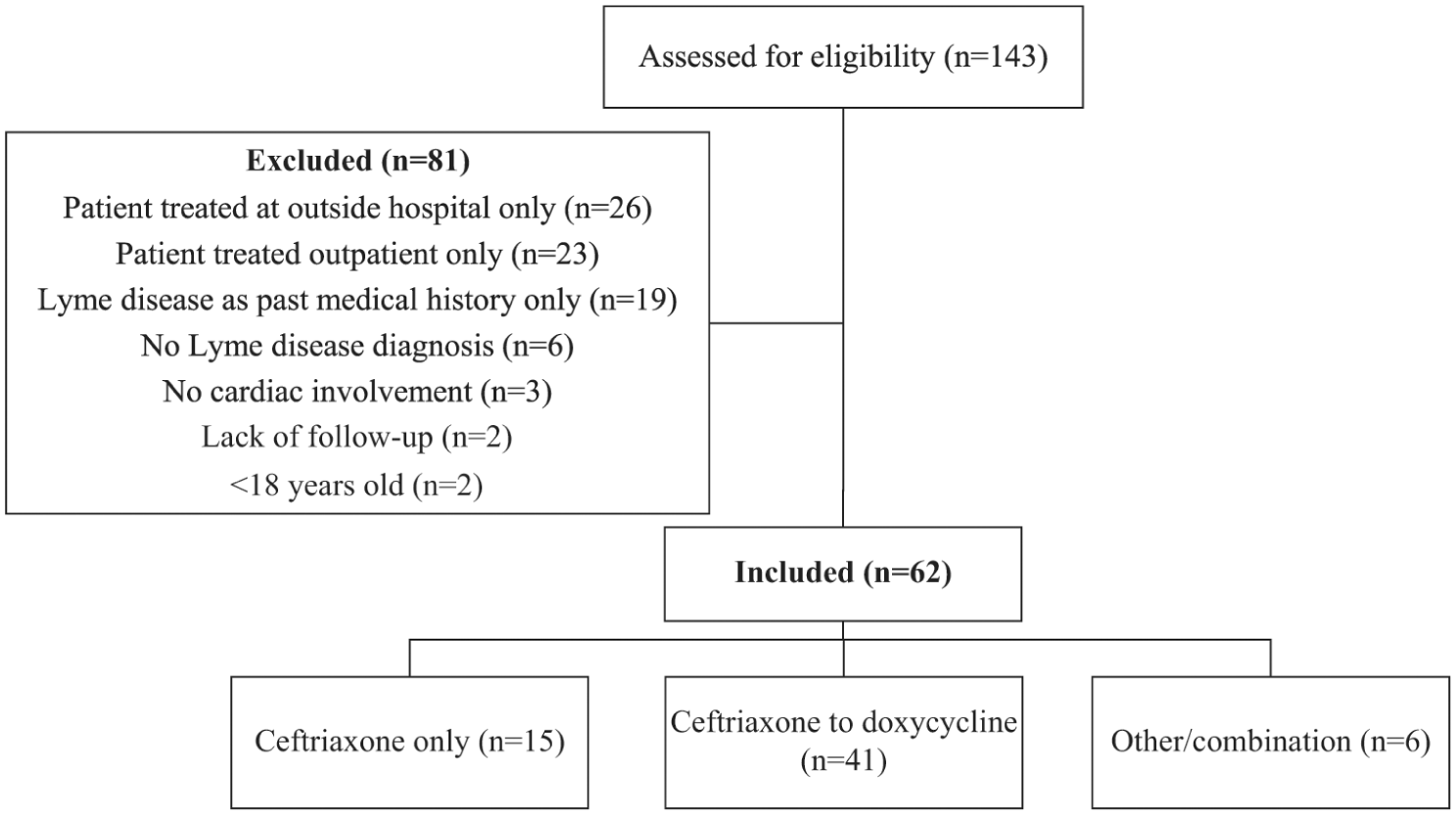
Flowchart of patient inclusion.
The overall sample of patients included 80.6% men, 93.5% white, with a mean age of 50 ± 19.3 years (Table 1). Patients had a variety of CV comorbidities, with the most common being hypertension; no patients had a permanent pacemaker prior to admission. Most common presenting symptoms were lightheadedness, followed by malaise and dyspnea. Almost half of patients required ICU admission during their hospitalization. July (19; 30.6%), followed by August (15; 24.2%) and June (12; 19.4%) were the most common months of admission. Patients who ended up receiving ceftriaxone only were older (61 vs 45.4 years) and had higher rates of selected CV comorbidities (hypertension 53.3 vs 24.4%; dyslipidemia 40 vs 12.2%), beta blocker use (26.7 vs 9.8%), and median PR interval lengthening (311 vs 258 ms) prior to admission, compared with those who received ceftriaxone/doxycycline.
Baseline Characteristics of the Sample, Stratified by Treatment Group.
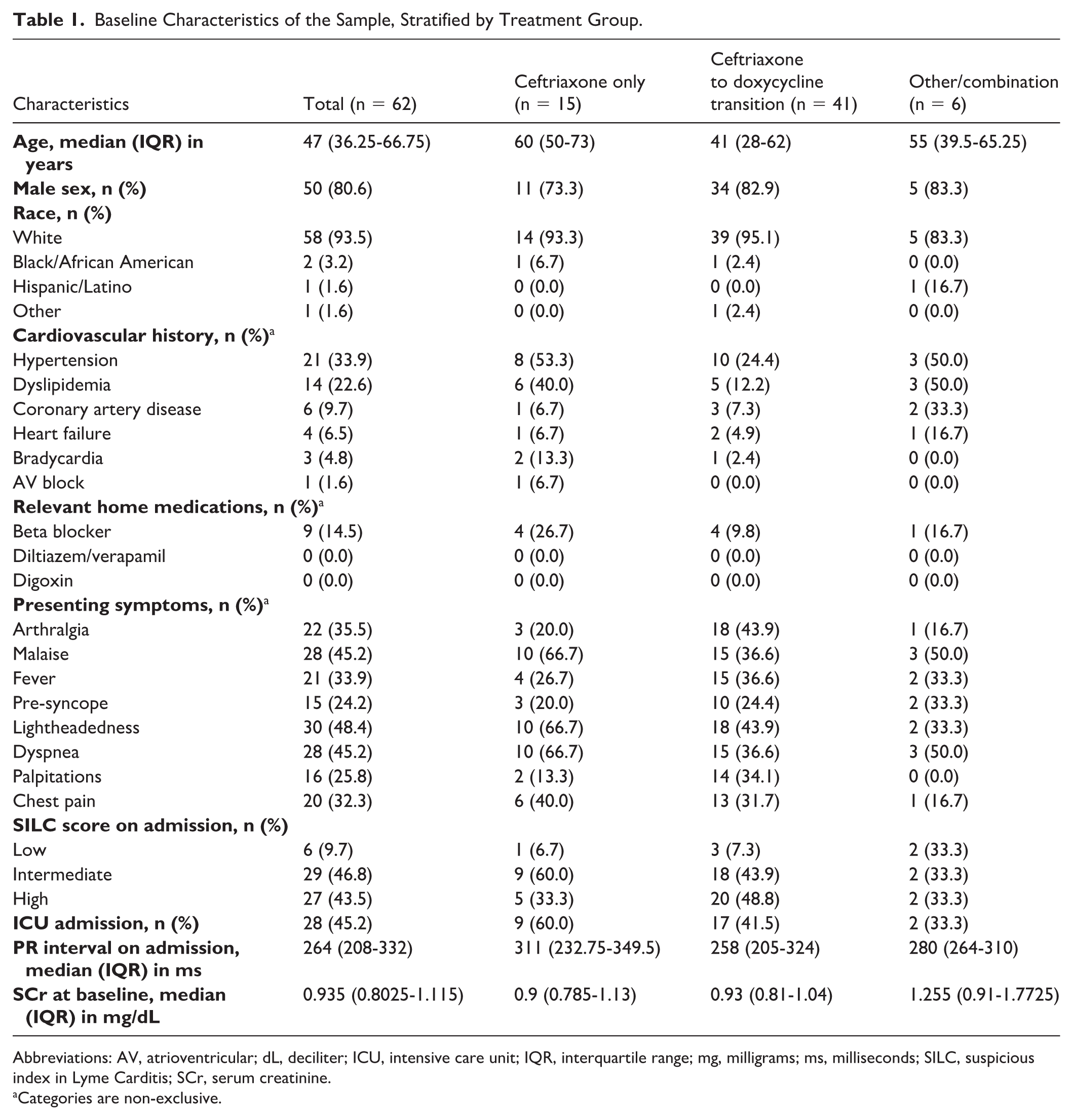
Abbreviations: AV, atrioventricular; dL, deciliter; ICU, intensive care unit; IQR, interquartile range; mg, milligrams; ms, milliseconds; SILC, suspicious index in Lyme Carditis; SCr, serum creatinine.
Categories are non-exclusive.
The most common CV manifestations (other than AV block) identified upon workup were sinus bradycardia (27; 43.5%), T-wave inversion (21; 33.9%), right bundle branch block (16; 25.8%), and atrial fibrillation/flutter (7; 11.3%), with other findings, such as myocarditis and pericarditis, occurring in <10% of patients. A total of 15 (24.2%) patients had an elevated ESR >25 mm/h and 21 (33.9%) patients had CRP ≥0.5 mg/dL.
Serology tests were positive for Lyme antibody enzyme immunoassay/indirect immunofluorescence assay (EIA/IFA) (58; 93.5%), immunoglobulin (Ig)G (44; 71.0%), and IgM (48; 77.4%) in most patients. Patients were most commonly categorized with intermediate or high SILC scores. Only a small proportion of patients (9; 14.5%) had a known tick exposure, admitted a median (IQR) 26.5 (13-28) days after said exposure. Thirteen (21.0%) patients presented with an EM rash at admission; 10 (16.1%) patients reported an EM rash prior to admission, with appearance a median (IQR) 19 (14-21) days prior to admission.
Study Outcomes
Outcomes are broadly described in Table 2. Patients given ceftriaxone received a median (IQR) of 28 (23.5-28.5) total DOT. Patients who transitioned from ceftriaxone to doxycycline received ceftriaxone for a median (IQR) of 5 (3-7) DOT before 20 (14-22) DOT for doxycycline. Standard dosing of ceftriaxone 2000 mg IV daily and doxycycline 100 mg PO twice daily was utilized. Approximately one third of patients overall were given another antibiotic before or during admission; the most common concomitant antibiotics were cefazolin (7; 11.3%) and cephalexin (5; 8.0%), often given for either surgical prophylaxis in patients who received permanent pacemaker placement or skin rash upon initial presentation, respectively.
Primary and Secondary Outcomes.
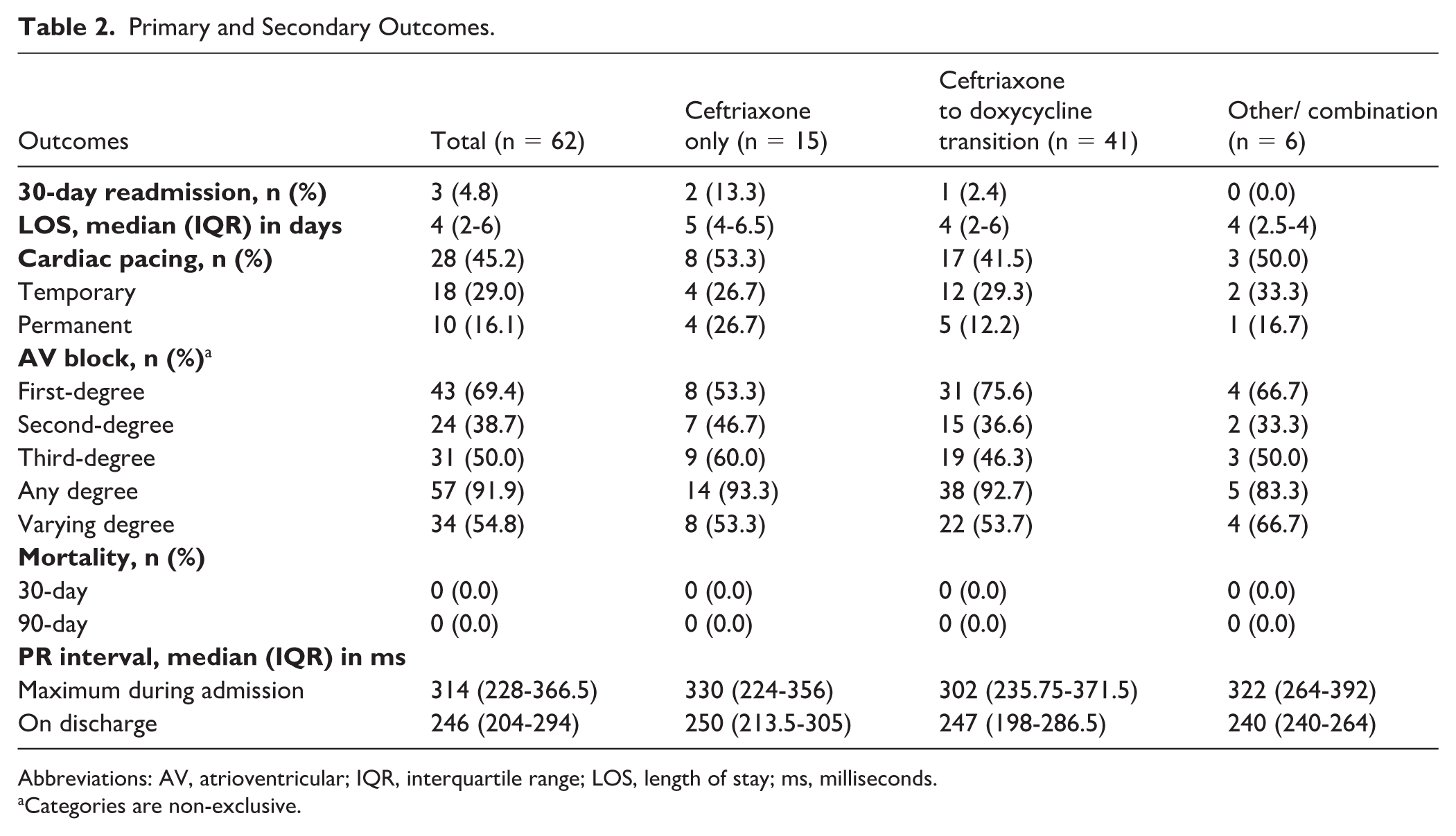
Abbreviations: AV, atrioventricular; IQR, interquartile range; LOS, length of stay; ms, milliseconds.
Categories are non-exclusive.
Most patients (43; 69.4%) experienced first-degree AV block, followed by third-degree (31; 50.0%) and second-degree (24; 38.7%); more than half of patients experienced more than one type during their hospitalization. Cardiac pacing was required for 28 (45.2%) patients, with temporary pacing exceeding placement of a permanent pacemaker. The median duration of the PR interval at discharge demonstrated an overall 7.3% reduction from admission to discharge (264-246 ms). Compared with the step-down therapy group, the mean PR interval for the ceftriaxone only group was longer upon admission and at discharge, but the mean maximum PR interval duration during hospitalization was slightly less.
Overall median (IQR) LOS was 4 (2-6) days, including 5 (4-6.5) days in patients who received ceftriaxone, 4 (2-6) days in patients who transitioned from ceftriaxone to doxycycline, and 4 (2.5-4) days in patients receiving other/combination therapy. Thirty-day readmissions occurred in only 3 (4.8%) patients across the entire sample, with a median time to readmission of 27 (26-27.5) days (Table 3). All three readmitted patients had a history of outdoor exposure, a current or past EM rash, malaise, shortness of breath, and either chest pain or palpitations, along with high SILC scores. Only one of three patients received temporary pacing during their index admission. Each were initially treated with inpatient ceftriaxone, while 2 of 3 patients continued ceftriaxone in the outpatient setting and one patient was transitioned to PO doxycycline prior to readmission. No patients were discharged with AV-nodal blocking medications prior to readmission. Of the 3 patients who were readmitted, 2 continued ceftriaxone, while one was converted from doxycycline to ceftriaxone following readmission. No 30- or 60-day mortality was observed.
Details of Index Admission for Patients With 30-Day Readmission.
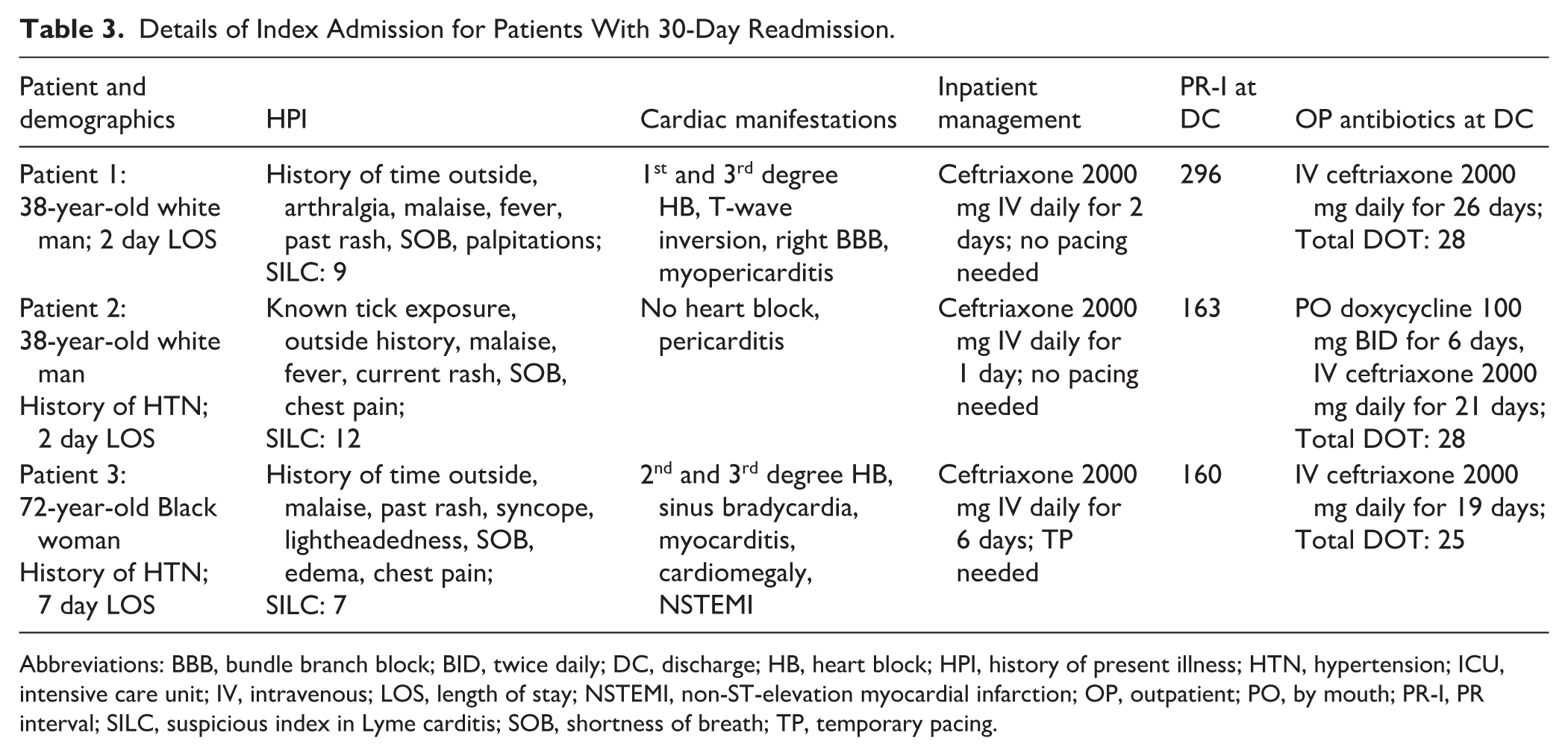
Abbreviations: BBB, bundle branch block; BID, twice daily; DC, discharge; HB, heart block; HPI, history of present illness; HTN, hypertension; ICU, intensive care unit; IV, intravenous; LOS, length of stay; NSTEMI, non-ST-elevation myocardial infarction; OP, outpatient; PO, by mouth; PR-I, PR interval; SILC, suspicious index in Lyme carditis; SOB, shortness of breath; TP, temporary pacing.
Discussion
Although this retrospective descriptive study included a limited sample, it represents one of the largest analyses within an endemic region to evaluate treatment regimens and resulting clinical outcomes for hospitalized patients with Lyme carditis. The literature details a variety of case reports related to Lyme carditis,17-24 many of which illustrate an atypical presentation and/or severity of illness, but only a few broader analyses exist. Recent insurance claims data have found statistically higher incidence of myocarditis and/or pericarditis among patients within a Lyme disease endemic region in comparison with non-endemic regions. 25 Readmissions in our study were low overall (<5%), regardless of treatment regimen received, suggesting broad effectiveness of both ceftriaxone and ceftriaxone/doxycycline-based treatment strategies. With this data, we are unable to draw specific conclusions regarding treatment choice and their effect on short-term clinical outcomes beyond 30 days post-hospital discharge. Although long-term clinical outcomes were not observed in this study, a case series by Wang et al 26 highlighted full recovery of cardiac manifestations, activity level, and symptoms for seven patients across an approximate 20-month follow-up period.
Lack of patient mortality observed in our study aligns with prior literature indicating rapid improvement of clinical condition for most patients following antibiotic therapy. 10 A retrospective cohort analysis of over 10 000 patients hospitalized with Lyme carditis reported a modest 1.5% in-hospital mortality rate, although the impact of treatment on outcomes were not evaluated. 6 Prominent cardiac manifestations observed in this study, such as heart block and arrhythmias, correspond with common clinical presentations depicted in the literature; 27 our findings correlate with literature suggesting first-degree AV block may be most common upon presentation. 28 Our study additionally highlighted sinus bradycardia, T-wave inversion, and bundle branch blockade as common manifestations of Lyme carditis. Almost half of all patients in our study required cardiac pacing in comparison with Uzomah et al, 6 which reported both temporary and permanent pacing in approximately 10% of patients in Lyme carditis. A higher degree of heart block and severity, including half of our sample experiencing third-degree block, likely contributes to this higher incidence of pacing.
While patients in the ceftriaxone only group were admitted with an average PR interval longer than that of the group transitioned to PO doxycycline, the overall maximum PR interval duration in the ceftriaxone only group was slightly lower. These data correspond with prior reports suggesting rapid improvement of the PR interval following initial ceftriaxone therapy, 29 and suggest IV ceftriaxone may play a greater role in controlling the maximum PR interval duration in hospitalized patients. Nevertheless, PR interval changes from admission to discharge were comparable between the ceftriaxone only group and the ceftriaxone/doxycycline group in our study. It is well described in the literature that the degree of AV block and PR interval prolongation due to Lyme carditis can rapidly fluctuate within the same day and in relatively short time intervals.30,31 Interpretation of these data was further complicated by the various levels of PR prolongation at admission, a low sample size, and a higher number of ICU admissions in the ceftriaxone-only group. In this study, the mean PR interval duration at discharge was improved compared with admission but was not completely normalized. Guidance recommends an outpatient electrocardiogram and follow-up visit 4 to 6 weeks after discharge to confirm lack of rhythm and conduction abnormalities. 8
The most common treatment regimens utilized in this study were consistent with recommendations from literature and guideline resources recommending using IV ceftriaxone until clinical stability, followed by PO doxcycline.10,11 Although there are a paucity of data describing the specific days of IV therapy prior to PO transition, a median of 5 days of IV ceftriaxone prior to PO doxycycline was observed in our study, which may align with the approximate time needed for observable clinical improvement. The duration of therapy observed in this study is moderately longer than the 14 to 21 days recommended by clinical treatment guidelines.10,11 Based on a 5-day average LOS in this study, extensions of treatment duration were likely to occur in the outpatient setting and potentially due to scheduling variability and timing of outpatient follow-up visits and/or levels of adherence to PO therapy that could impact treatment duration and outcomes. Furthermore, treatment with 2 antibiotics (eg, ceftriaxone and doxycycline) on the same day, most commonly during IV-to-PO transition, can add an additional DOT to the antibiotic regimen.
Limitations
There were several limitations of this study. This was a retrospective study dependent on the availability and documentation of data within the EHR, including progress notes detailing items such as exposure history and receipt of treatment. Accordingly, there are likely some missing data, particularly with the history of present illness. Adherence to outpatient antibiotic regimens could not be evaluated for each patient, and data on treatment completion were limited to follow-up note documentation only within network facilities. No patients received both temporary and permanent pacing during hospitalization, which was likely due to lack of documentation of temporary pacing in patients receiving a permanent pacemaker. Long-term follow-up to determine the need for implantable cardioverter-defibrillator placement in patients with myocarditis was not assessed in this analysis. In addition, we were unable to ascertain whether some patients may have received antibiotic doses before their hospital admission for Lyme carditis which would impact the study’s estimates of DOT and associated clinical outcomes. Furthermore, it is possible that patients may have been readmitted to outside hospitals which also was not captured in this analysis.
Conclusion and Relevance
Various antibiotic regimens in this study were associated with low readmission rates for Lyme carditis. Patients across treatment groups had similar LOS, need for pacing, degree of heart block, and mortality. The data attained in this study support the need for prospective comparisons of different antibiotic regimens for Lyme carditis, appropriate criteria to transition from IV-to-PO therapy, as well as how to define treatment response in anticipation of hospital discharge among these patients.
Footnotes
Acknowledgements
The authors acknowledge Drs. Branden Nemecek and David Zimmerman for their collaborative scholarly partnership in relationship to this work. They also acknowledge Drs. Madison Plourde, Brooke Aston, Hanna Gosliak, Camren Horton, Madeline Krocker, Rayn Oswalt, and Chloe Potosnak for their work on foundational aspects of this project on their experiential research rotations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.