
Abstract
Background:
Delays in intravenous antiseizure medication (ASM) administration may worsen seizure outcomes. Intravenous push (IVP) administration reduces administration time for several ASMs, but evidence for IVP valproate loading is limited.
Objective:
To compare time from pharmacist verification to documented administration for IVP versus intravenous piggyback (IVPB) valproate loading doses and compare adverse event frequencies.
Methods:
This single-center retrospective study included adults from October 2023 to May 2025 who received an IV valproate loading dose (≥15 mg/kg). On August 15, 2024, institutional practice changed from IVPB valproate more than 60 minutes to undiluted IVP valproate at 500 mg/min. The primary outcome was time from pharmacist verification to loading dose administration. Secondary outcomes included order-to-administration time, adverse events, intensive care unit (ICU) admission, length of stay, and mortality.
Results:
One hundred thirty-one patients met the inclusion criteria (IVP, n = 60; IVPB, n = 71). Median (interquartile range [IQR]) age was 63 years (44-71), and 85 (65%) patients were male. Valproate indications were witnessed seizure in 92 (70.2%), suspected seizure in 29 (22.1%), and agitation/psychiatric in 10 (7.6%). Sixty-four (48.8%) patients received loading doses for status epilepticus. The median (IQR) loading dose was 28 (20-34.5) mg/kg. Median time to administration was 36 (95% CI, 22-52) minutes shorter with IVP than with IVPB (median [IQR], 28 [13-48] vs 63 [50-84] minutes; P < 0.001). Cardiovascular events occurred in 38.3% and 27.8% of IVP and IVPB patients (P = 0.27); sedation in 3.3% and 0% (P = 0.20); and valproate-associated adverse events in 6.7% and 1.4% (P = 0.18). No phlebitis or infiltration occurred.
Conclusion and Relevance:
Intravenous push valproate loading reduced time to administration without an observed increase in adverse events.
Keywords
Background
Prompt administration of antiseizure medications (ASMs) is a crucial component of managing acute seizures and status epilepticus. Delays in administering intravenous (IV) ASMs can contribute to the progression of status epilepticus and downstream complications, including neuronal injury and worsened clinical outcomes.1 -3 For this reason, rapid delivery of effective antiseizure therapy is a key component of emergent seizure management. 4 Changing how ASMs are administered, such as giving IV ASMs as intravenous push (IVP) rather than as intravenous piggyback (IVPB), can improve time to administration and has been shown to be safe for agents such as levetiracetam, lacosamide, and brivaracetam.4 -8 Valproate, however, has been challenging to administer expeditiously because it is considered a hazardous medication due to its teratogenicity risk and reproductive harm, and thus requires preparation via a hazardous compounding process when diluted for IVPB infusion.9,10
At our institution, handling concerns for IV valproate was addressed by using standard precautions and avoiding additional dilution-related manipulations, which allowed bedside preparation for acute seizure management. Although IVP valproate has been reported to be well tolerated, data comparing IVP and IVPB valproate loading doses, including adverse event frequencies, remain limited. 11 Thus, we sought to determine the speed and safety of administering valproate loading doses as IVP versus IVPB.
Methods
Study Design and Participants
This was a single-center, retrospective cohort study of adult patients admitted to a large academic medical center between October 2023 and May 2025 who received an IV valproate loading dose. Patients were included if they received ≥15 mg/kg of IV valproate and were ≥18 years of age. Patients were excluded if the initial dose was not a loading dose (eg, initial maintenance dose was >15 mg/kg). Loading dose status was confirmed by manual chart review. A dose was classified as a loading dose if it was the first IV valproate dose during the encounter, was ordered as a one-time dose, was ≥15 mg/kg using actual body weight, and was administered for an acute indication. Doses that represented the first dose of a scheduled maintenance regimen were classified as initial maintenance doses and were excluded, even if they were ≥15 mg/kg. The valproate loading dose was defined as the initial IV valproate dose administered and was recorded as both an absolute milligram (mg) dose and a weight-based dose (mg/kg), using the patient’s actual body weight at the time of administration. At our institution, IV valproate orders are not auto-verified and require pharmacist verification. Emergency department (ED) and intensive care unit (ICU) pharmacists prospectively verify orders in real time, and this workflow did not change during the study period. Patients were grouped according to whether they received valproate by IVP or IVPB. This retrospective study was approved by the institutional review board with a waiver of informed consent and is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Table S2).
Prior to August 15, 2024, IV valproate doses were prepared in the hazardous drug compounding hood in the chemotherapy pharmacy and administered as IVPB more than 60 minutes. After August 15, 2024, institutional practice changed to allow undiluted IVP valproate at 500 mg/min without a dose cap. Before implementation, pharmacy, nursing, medical staff, and the informatics team coordinated a multidisciplinary rollout. Staff education included presentations reviewing the rationale and supporting evidence, and an SBAR document outlining administration procedures and precautions was distributed to nursing and pharmacy staff. Nurses were instructed to use standard handling precautions, including gloves and consideration of an N95 mask. Order sets were updated to default to IVP administration, and the institutional Lexicomp monograph was revised. Pharmacist verification workflow, pharmacy staffing, and order-priority defaults did not change. Valproate vials were stocked in Omnicell pockets on high-use units to increase immediate availability.
We collected data on baseline characteristics, neurological comorbidities, valproate indication and dose, and the location of valproate administration (ED, general floor, or ICU). If the patient was loaded for status epilepticus, the STESS was calculated. 12 Data on hospital and ICU length of stay, and on whether the patient was intubated before or after the loading dose, were also collected. Patients were identified through the institutional data warehouse, with supplemental manual chart review performed to confirm eligibility and clinical data. The study data were collected and managed using REDCap.13,14 Data abstraction was performed by a single trained investigator using a standardized REDCap form with built-in field validation. To assess data accuracy, a co-author independently conducted peer-review spot checks on a subset of records to ensure data integrity. A complete data dictionary, including the source and operational definition of every variable, is provided in Supplemental Table S1.
Outcomes
The primary outcome was time to loading dose administration, defined as the interval, in minutes, from pharmacist order verification to documented medication administration. This outcome was selected because the institutional practice change was implemented primarily to reduce delays in medication preparation and administration. As a secondary analysis, we also evaluated the interval from order entry to documented medication administration. Among orders entered as STAT, administration occurring more than 60 minutes after pharmacist verification was classified as delayed, and the frequency of delayed STAT administration and the documented reason for delay were collected and compared between groups. Secondary safety outcomes included immediate adverse events occurring within 4 hours of valproate administration, including cardiovascular events, sedation, and IV phlebitis/infiltration. Valproate-associated adverse events, including hyperammonemia, pancreatitis, and thrombocytopenia, were assessed up to 24 hours after receiving IV valproate. Cardiovascular events were defined as tachycardia (heart rate [HR] > 100 bpm), bradycardia (HR < 50 bpm), or hypotension (any SBP < 90 mmHg) occurring within 4 hours of valproate administration. Sedation was defined as a decrease in Richmond Agitation-Sedation Scale score of ≥2 points or a decrease in Glasgow Coma Scale score of ≥2 points within 4 hours of valproate administration.15,16 Infusion-site complications were assessed using standardized phlebitis and infiltration grading criteria.17,18 For cases of phlebitis or infiltration, concurrent IV medications administered through the same IV access site were recorded, including vasopressors, and IV sedation.
Valproate-associated adverse drug events included hyperammonemia, pancreatitis, and thrombocytopenia. Hyperammonemia was defined as a serum ammonia level ≥50 μmol/L, which reflects our institutional upper limit of normal. Pancreatitis was defined as new-onset acute abdominal pain or gastrointestinal symptoms with serum lipase or amylase ≥3× the upper limit of normal or imaging findings consistent with pancreatitis, after exclusion of other common causes, including gallstones, alcohol use, hypertriglyceridemia, or hypercalcemia. 19 Clinically significant thrombocytopenia was defined as a platelet count <50 000/µL. 20 These safety outcomes were obtained from the patient’s electronic health record (EHR) documentation.
Post-load concentration timing was not standardized by protocol. For patients with an available post-load concentration, the interval from loading dose completion to laboratory collection was calculated using medication administration and laboratory collection timestamps. To account for administration duration, IVPB completion time incorporated the 60-minute infusion duration, and IVP completion time was estimated using the institutional administration rate of 500 mg/min. Valproate concentrations collected after the initial loading dose were considered post-load concentrations and were compared between IVP and IVPB patients to assess potential differences in goal concentration attainment between administration methods.
Statistical Analysis
Baseline characteristics were summarized as counts and percentages for categorical variables and as means with standard deviations (SDs) or medians with interquartile ranges (IQRs), as appropriate based on data distribution. Differences between categorical variables were assessed using the chi-square test or Fisher exact test when appropriate. Continuous variables were compared using the Student t test for normally distributed data and the Wilcoxon rank-sum test for nonnormally distributed data. The primary outcome, time from pharmacist order verification to medication administration, was analyzed as a continuous variable and compared between IVP and IVPB groups using the Wilcoxon rank-sum test. To quantify the effect size for the primary outcome, the between-group difference was estimated using the Hodges-Lehmann estimator, calculated as the median of all pairwise differences in time to administration between IVPB and IVP patients. Differences were calculated as IVPB minus IVP, such that positive values indicated longer time to administration with IVPB. A 95% confidence interval (CI) for the difference in medians was generated using bootstrap resampling with 10 000 iterations. Time-to-administration was evaluated categorically for STAT orders, with administration classified as not delayed if documented ≤60 minutes after pharmacist verification and as delayed if documented >60 minutes after pharmacist verification. The frequency of delayed STAT administration was compared between IVP and IVPB groups using Fisher exact test. Secondary outcomes, including adverse drug events, infusion-site complications, ICU admission, length of stay, and mortality, were compared between groups using nonparametric methods based on variable type and distribution. All statistical analyses and data processing were conducted using R version 4.4.3 (2025-02-28) (R Foundation for Statistical Computing, Vienna, Austria), and Python with JupyterLab version 4.2.5 (Project Jupyter, 2024), and significance was defined as a P value <0.05.21 -23
Results
Patient Characteristics
One hundred forty-two patients were screened for inclusion; 131 met the inclusion criteria and were included in the final analysis (Figure 1). There were 60 patients in the IVP group and 71 in the IVPB group. There were no significant differences in baseline characteristics between groups. The median (IQR) age was 63 years (44-71), and 85 (65%) patients were male. Valproate indications were witnessed seizure in 92 (70.2%), suspected seizure in 29 (22.1%), and agitation or psychiatric indications in 10 (7.6%). A total of 64 (48.8%) patients were loaded for status epilepticus. Among these patients, median (IQR) STESS was 0 (0-3) in the IVP group and 1 (0-3) in the IVPB group (P = 0.43). The median (IQR) valproate loading dose was 28 mg/kg (20-34.5). A summary of baseline characteristics is shown in Tables 1 and 2.
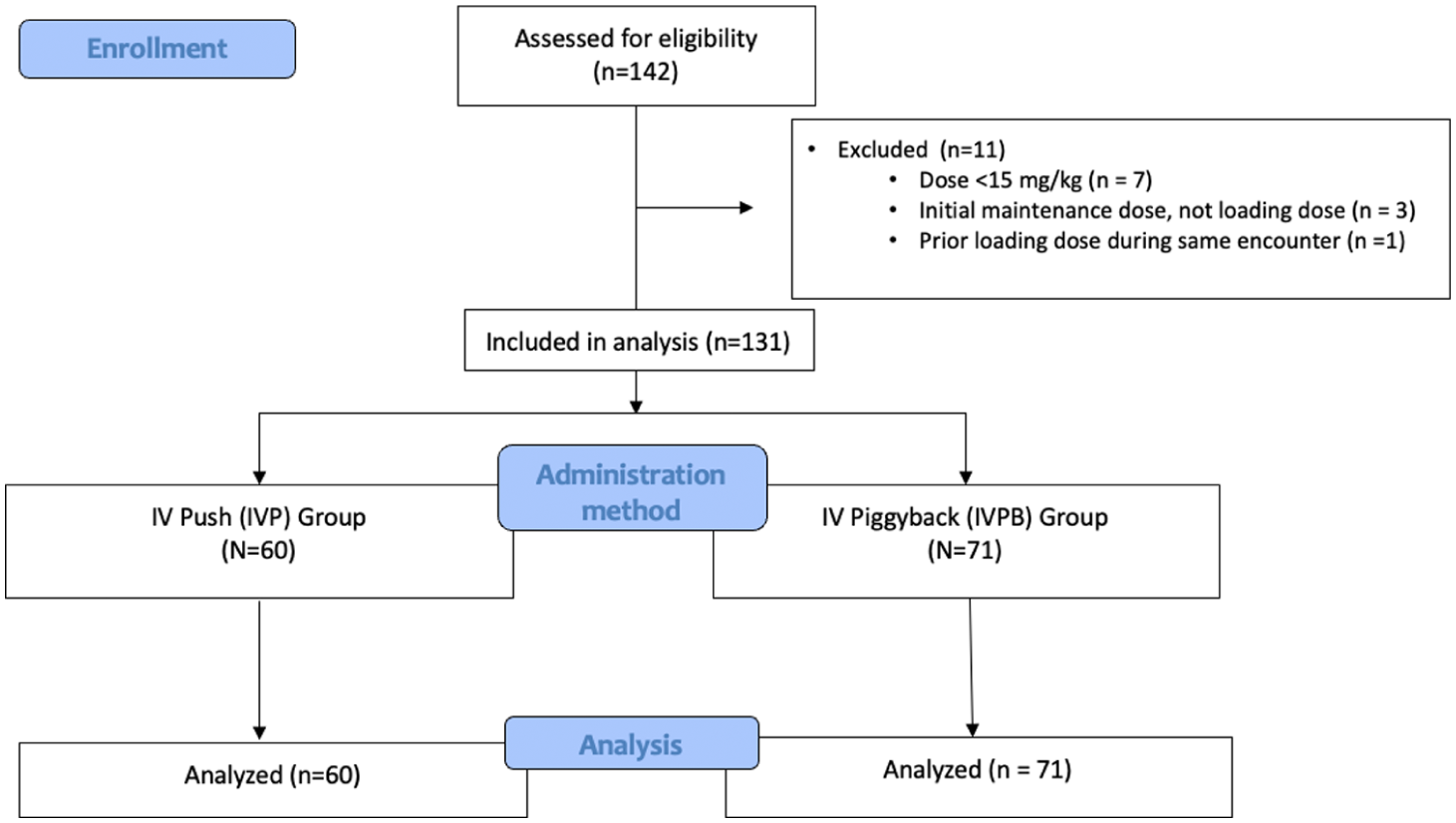
Flow diagram of cohort selection and analysis. Of 142 patients assessed for eligibility, 11 were excluded: 7 received a dose <15 mg/kg, 3 received an initial maintenance dose rather than a loading dose, and 1 had a prior loading dose during the same encounter. The final cohort included 131 patients: 60 in the IVP group and 71 in the IVPB group.
Baseline Characteristics.
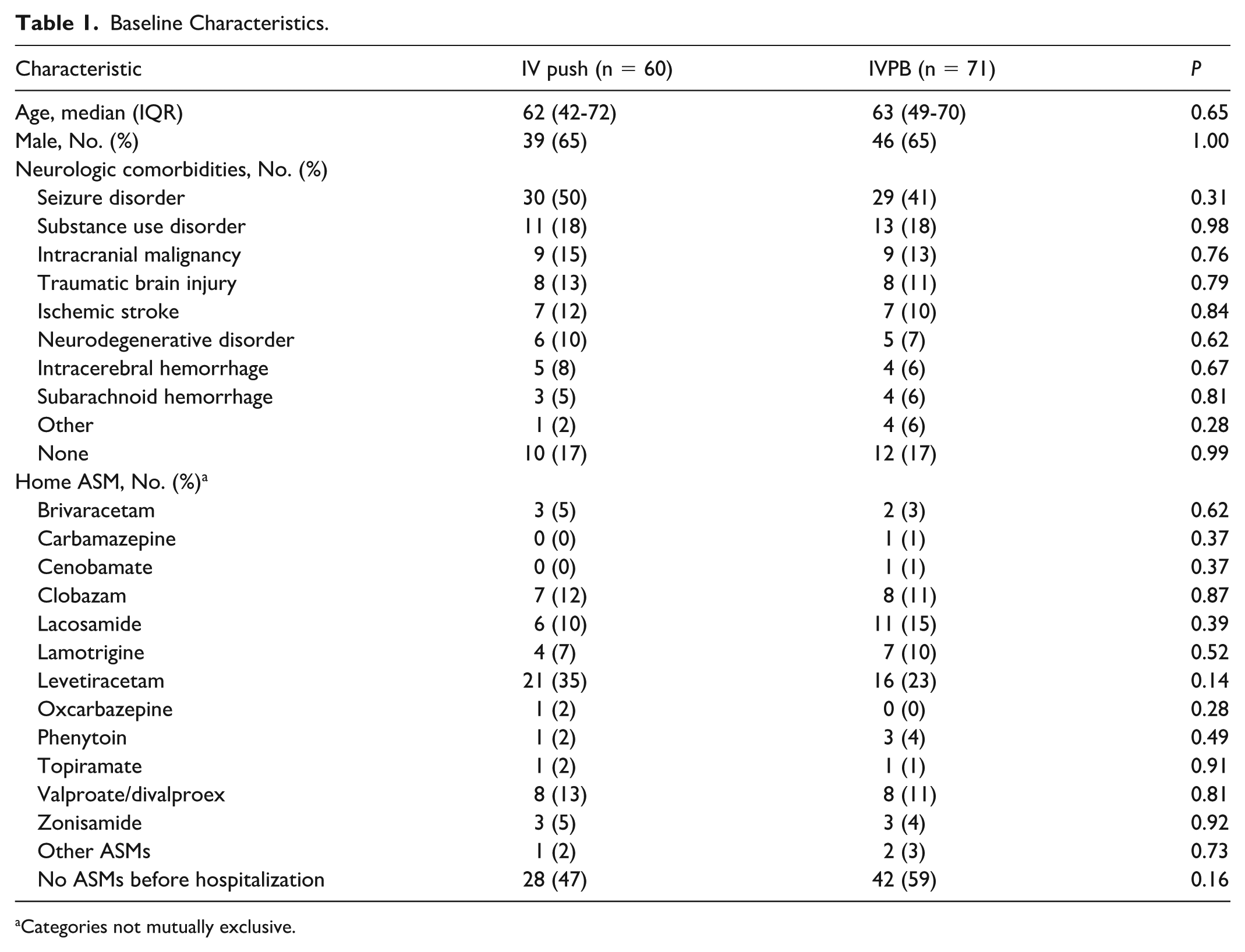
Categories not mutually exclusive.
Valproate Indication, Seizure Characteristics, and Loading Dose Details.
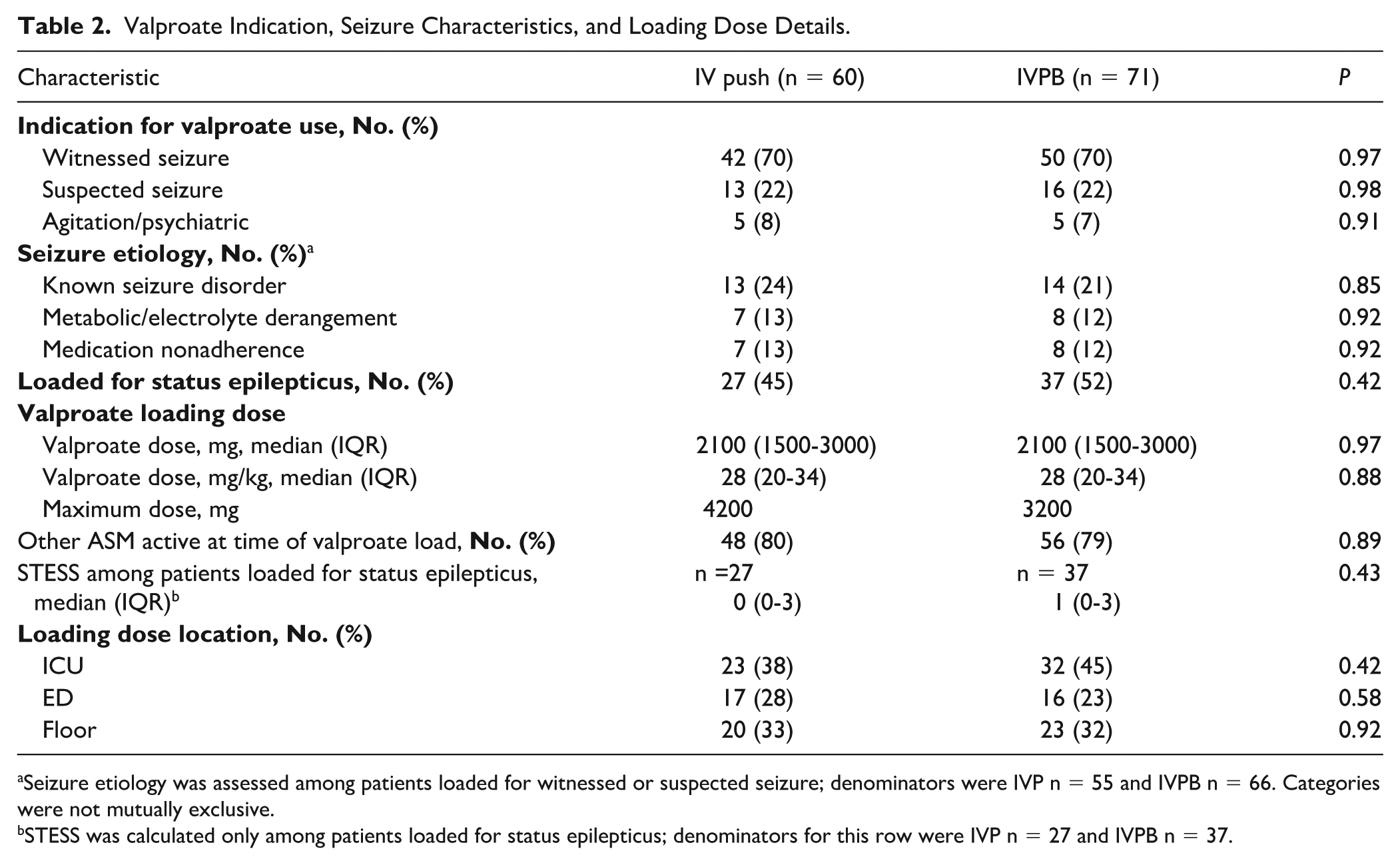
Seizure etiology was assessed among patients loaded for witnessed or suspected seizure; denominators were IVP n = 55 and IVPB n = 66. Categories were not mutually exclusive.
STESS was calculated only among patients loaded for status epilepticus; denominators for this row were IVP n = 27 and IVPB n = 37.
Outcomes
The median (IQR) time from pharmacist verification to loading dose administration was 28 minutes (13-48) in the IVP group and 63 minutes (50-84) in the IVPB group (P < 0.001; Figure 2). The Hodges-Lehmann estimate of the between-group difference (IVPB − IVP) was 36 minutes, with a bootstrap 95% CI of 22 to 52 minutes, indicating that time to IVPB administration was approximately 36 minutes slower than IVP administration. Primary outcome data are summarized in Table 3.
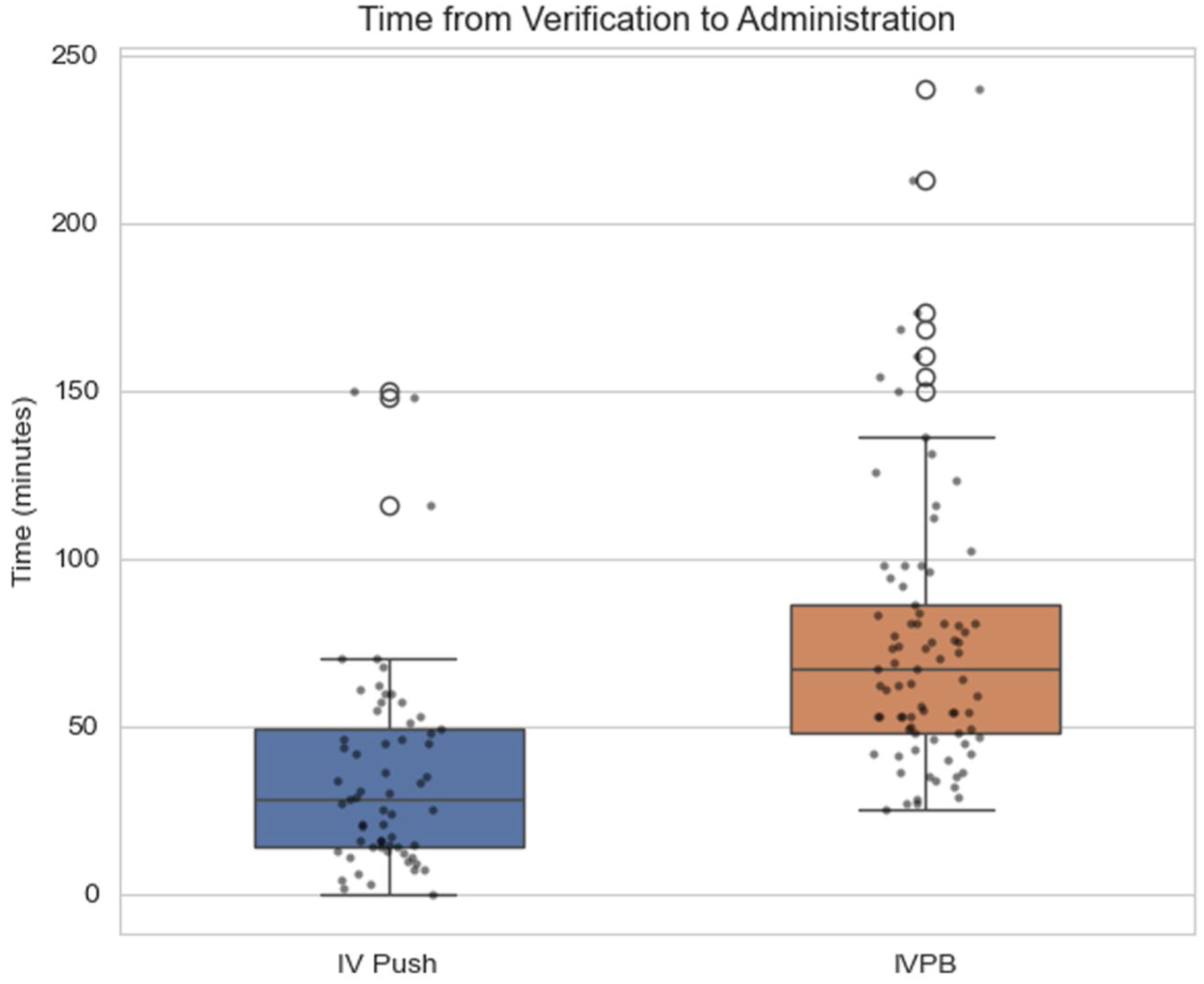
Time from pharmacist verification to documented administration of IV valproate. Filled circles on the graph represent individual patient observations. Open circles represent statistical outliers beyond 1.5 times the interquartile range. Boxes represent the interquartile range, horizontal lines represent medians, and whiskers extend to the most extreme non-outlier values.
Primary Outcome.
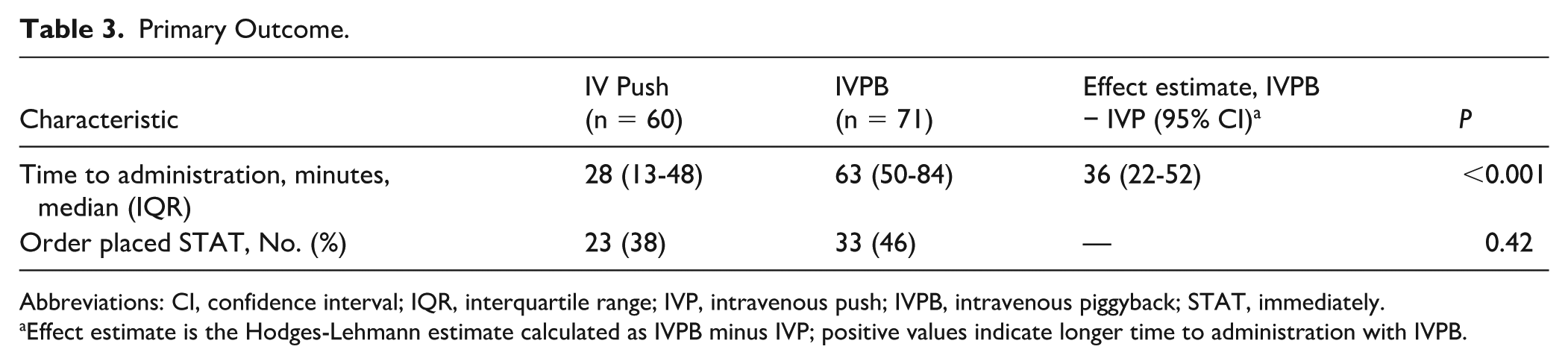
Abbreviations: CI, confidence interval; IQR, interquartile range; IVP, intravenous push; IVPB, intravenous piggyback; STAT, immediately.
Effect estimate is the Hodges-Lehmann estimate calculated as IVPB minus IVP; positive values indicate longer time to administration with IVPB.
In a secondary analysis, median (IQR) order-to-administration time was also shorter in the IVP group than in the IVPB group, 34.0 (19.8-60.0) versus 75.0 (54.0-98.5) minutes; P < 0.001. Time from order entry to pharmacist verification did not differ significantly between groups, 4.0 (1.0-8.3) versus 5.0 (3.0-8.0) minutes; P = 0.157.
The proportion of orders placed as STAT did not differ significantly between groups (23/60 [38%] vs 33/71 [46%], P = 0.42). Among STAT orders, delayed administration more than 60 minutes after pharmacist verification occurred less frequently with IVP than with IVPB (2/23 [9%] vs 12/33 [36%], P = 0.027). The 2 delayed IVP STAT doses had no documented reason for delay. Among the 12 delayed IVPB STAT doses, documented reasons included delay after medication delivery (n = 7), medication not delivered on time (n = 2), and no documented or available reason (n = 3).
Valproate dosing was similar between groups, including median (IQR) absolute dose 2100 mg (1500-3000), P = 0.97, and weight-based dose 28 mg/kg IQR (20-34) versus 28 mg/kg IQR (20-34), P = 0.88, although the maximum administered dose was higher in the IVP group (4200 vs 3200 mg). The proportion of patients receiving another ASM at the time of valproate loading did not differ between groups (80% vs 79%, P = 0.89).
Adverse events are summarized in Table 4. Cardiovascular events occurred in 38% of IVP patients and 28% of IVPB patients (P = 0.27). These events were primarily tachycardia and hypotension. Tachycardia occurred in 14/60 (23%) IVP patients and 10/71 (14%) IVPB patients (P = 0.22), while hypotension occurred in 13/60 (22%) and 8/71 (11%) patients, respectively (P = 0.13). Bradycardia was less common, occurring in 2/60 (3%) IVP patients and 4/71 (6%) IVPB patients (P = 0.40). Treatment was administered to 1 patient with tachycardia and 1 patient with bradycardia, whereas treatment for hypotension was administered to 10/13 IVP patients and 5/8 IVPB patients. Among patients treated for hypotension, vasopressors were used in 4/10 IVP patients and 2/5 IVPB patients, all with norepinephrine; the remaining patients received IV fluids without vasopressors. Sedation occurred in 2/60 (3%) IVP patients and 0/71 IVPB patients (P = 0.20). Neither group experienced IV phlebitis or IV infiltration.
Secondary Outcomes.
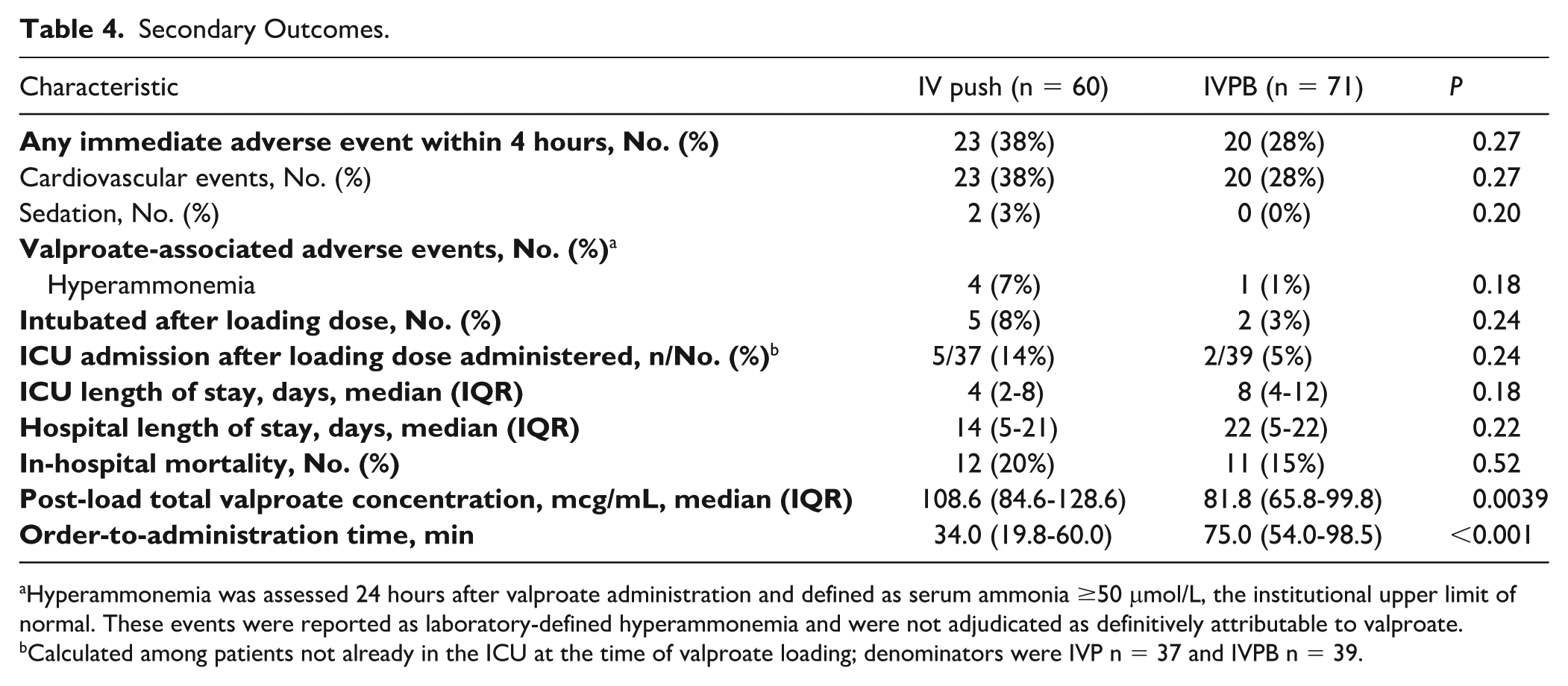
Hyperammonemia was assessed 24 hours after valproate administration and defined as serum ammonia ≥50 μmol/L, the institutional upper limit of normal. These events were reported as laboratory-defined hyperammonemia and were not adjudicated as definitively attributable to valproate.
Calculated among patients not already in the ICU at the time of valproate loading; denominators were IVP n = 37 and IVPB n = 39.
Valproate-associated adverse events occurred in 4 IVP and 1 IVPB patient (P = 0.18), all laboratory-defined hyperammonemia within 24 hours; individual ammonia values, closest albumin values, and available pre-load ammonia concentrations are provided in Supplemental Table S3. These findings should not be interpreted as confirmed valproate-induced hyperammonemia, and no thrombocytopenia or pancreatitis occurred. Post-load valproate concentrations were higher with IVP in the overall cohort (108.6 vs 81.8 mcg/mL; P = 0.0039; Figure 3) and in patients loaded for status epilepticus with available concentrations (109.5 [84.3-125.3] vs 79.3 [65.8-90.2] mcg/mL; P = 0.024; Figure 4). Post-load concentration timing did not differ after accounting for administration duration (73.4 [56.0-127.6] vs 73.0 [57.2-124.2] minutes; P = 0.693). A complete summary of secondary outcomes is shown in Table 4.
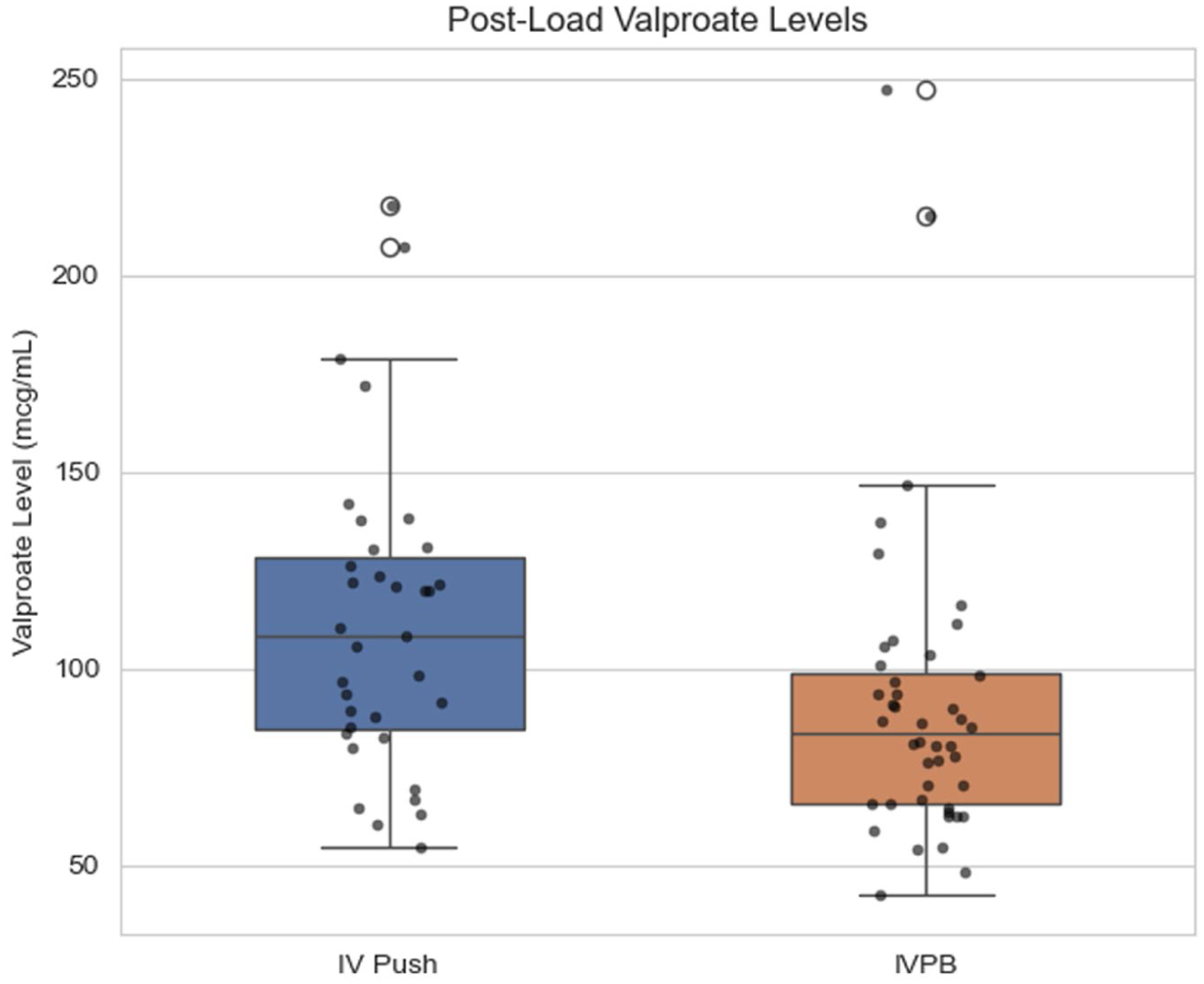
Post-load total valproate concentrations by valproate administration method. Filled circles on the graph represent individual patient observations. Open circles represent statistical outliers beyond 1.5 times the interquartile range. Boxes represent the interquartile range, horizontal lines represent medians, and whiskers extend to the most extreme non-outlier values.
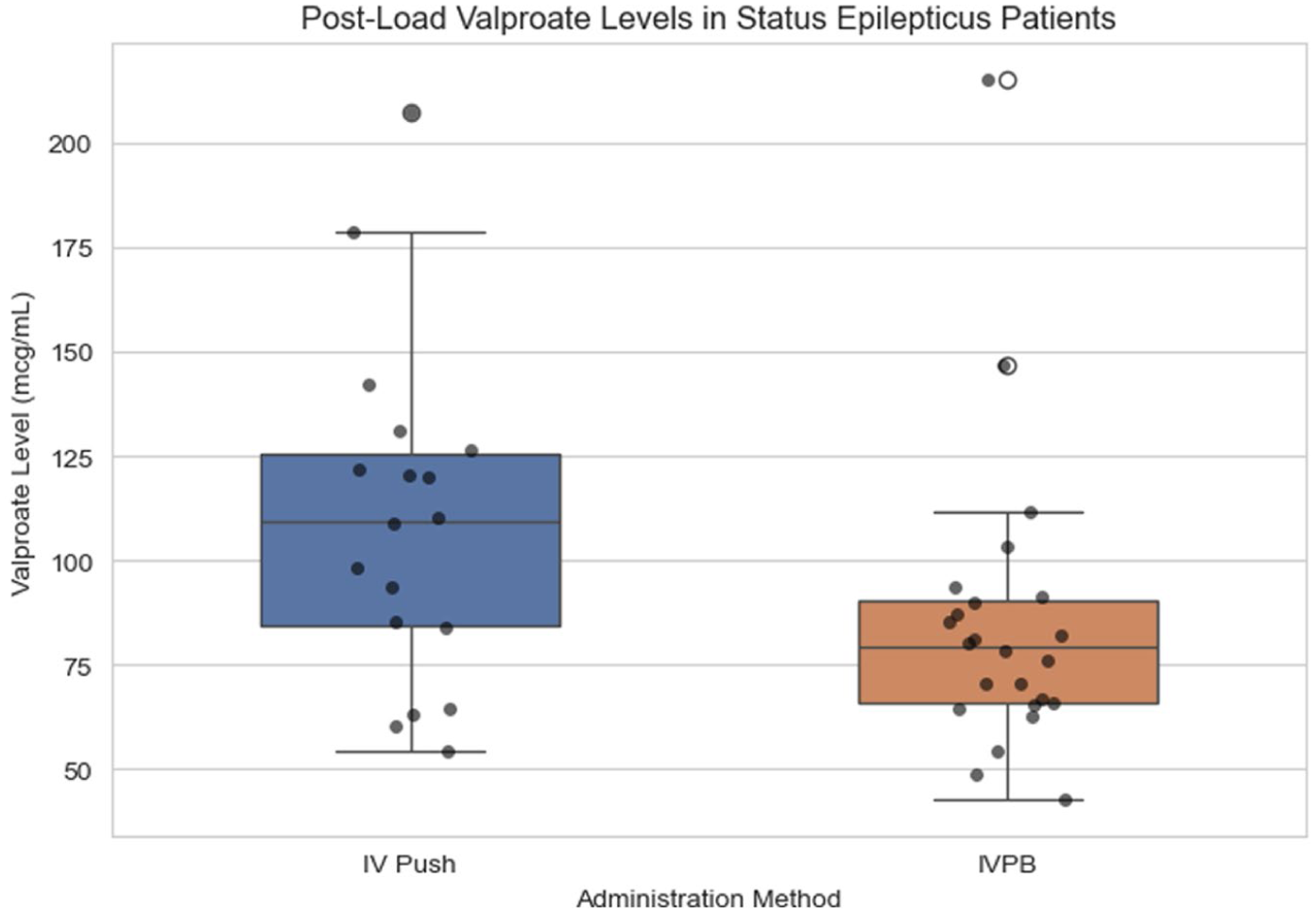
Post-load total valproate concentrations by valproate administration method among patients loaded for status epilepticus. Filled circles on the graph represent individual patient observations. Open circles represent statistical outliers beyond 1.5 times the interquartile range. Boxes represent the interquartile range, horizontal lines represent medians, and whiskers extend to the most extreme non-outlier values.
Discussion
In this retrospective cohort study of 131 adult patients who received IV valproate loading doses, IVP administration significantly reduced time to administration compared with IVPB (28 vs 63 minutes; Hodges-Lehmann estimate [IVPB − IVP], 36 minutes; 95% CI, 22-52 minutes; P < 0.001) without an observed increase in adverse events. Among STAT orders, IVP administration was also associated with fewer doses delayed by more than 60 minutes after pharmacist verification (9% vs 36%, P = 0.027). Despite similar weight-based dosing, IVP valproate was associated with higher post-load total valproate concentrations, likely reflecting more rapid loading dose administration compared with IVPB infusion.
To our knowledge, this is the largest cohort to describe IVP valproate loading doses and expands the prior literature supporting the safety of IVP valproate. Valproate has previously been shown to be well tolerated when administered rapidly by Wheless et al, 24 who noted that infusion rates up to 6 mg/kg/min resulted in only mild and reversible adverse effects. Limdi et al 11 found that rapid undiluted valproate infusion was generally well tolerated, though higher rates of 10 mg/kg/min were associated with infusion-related symptoms. Based on these findings, our institution administers IVP valproate at a maximum rate of 500 mg/min. This was consistent with the approach of Wang et al, who demonstrated comparable safety between IVP and IVPB valproate, with a significantly shorter time to administration in the IVP cohort, although the tolerability of loading doses was not specifically described. Wang et al 25 did report a higher frequency of infusion-site phlebitis with IVP administration, which is distinct from our findings, but these patients tended to be on vasopressors or other medications, which could confound the incidence of phlebitis. We did not observe any cases of phlebitis, and this may reflect differences in concurrent medications, sample size, institutional administration practices, or documentation of infusion-site reactions.
Interestingly, we observed that post-load concentrations were higher after IVP compared with IVPB, a finding observed both in the overall cohort and in the subgroup analysis of patients with status epilepticus. This could be related to the faster administration time of IVP doses compared with IVPB, or to the complex pharmacokinetics of IV valproate. Valproate is highly protein-bound, which can influence the free fraction and clinical effects, particularly in critically ill patients, where elevated free concentrations may be associated with adverse effects.10,26,27 In a prospective safety and pharmacokinetic study, Dutta et al 27 found that rapid valproate infusions of 20 to 30 mg/kg at 6 to 10 mg/kg/min produced transient increases in total and unbound concentrations, with disproportionate free-drug elevations at higher loading doses due to saturable protein binding. These pharmacokinetic changes were transient and not associated with clinically significant adverse events; thus, the difference in post-load concentrations observed in our study is not considered clinically meaningful.
Overall, this study adds to the growing body of evidence supporting IVP administration of ASMs to reduce treatment delays in acute seizure management. Prior studies have shown that IVP administration of ASMs, including levetiracetam, lacosamide, and brivaracetam, can reduce medication preparation, delivery, or administration time without clear safety concerns.4 -8,28,29 This has been demonstrated across multiple ASMs, with IVP levetiracetam and lacosamide showing safety profiles comparable with those of IVPB administration, and brivaracetam demonstrating adverse event frequencies similar to those of infusion-based administration.5 -7,28,29 Collectively, these findings support IVP administration as a safe and operationally effective strategy that meaningfully reduces treatment delays in managing acute seizures such as status epilepticus. Given the association between prolonged seizure duration and the risk of neuronal injury, workflow modifications that expedite initiation of second-line antiseizure therapy may have important clinical implications.
Our study has several limitations, including its retrospective design and reliance on EHR documentation, which may be incomplete in acute clinical situations such as status epilepticus. The sequential pre/post design may have been influenced by temporal changes in clinical practice or workflow independent of administration method. The primary outcome relied on pharmacist verification and medication administration timestamps, which may not reflect actual preparation or bedside delivery time. Identification of infusion-site reactions also depended on nursing documentation and may have led to underreporting. Adverse events, particularly sedation or changes in mentation, could have been confounded by ongoing seizure activity, postictal state, sedative exposure, critical illness, and limitations of retrospective EHR documentation; therefore, sedation events were reported as temporally associated safety outcomes rather than definitively attributable to valproate. Finally, the single-center design may limit generalizability, and the sample size may limit the detection of uncommon adverse events associated with IVP valproate administration.
Relevance to Patient Care and Clinical Practice
Delayed ASM administration may worsen outcomes in acute seizures and status epilepticus. At our institution, switching IV valproate loading doses from IVPB to undiluted IVP administration at 500 mg/min shortened the time from pharmacist verification to administration, without an observed increase in adverse events. For institutions where IVPB preparation may delay medication delivery, IVP valproate may be a practical strategy to improve timely loading dose administration in acute care settings.
Conclusion and Relevance
Administering IV valproate loading doses as IVP versus IVPB significantly reduced the time to administration without affecting the frequencies of adverse drug events. These findings support IVP as a safe and more efficient method for valproate loading in acute care settings.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261459930 – Supplemental material for Speed and Safety of IV Push Versus IV Piggyback Valproate Loading Doses: A Retrospective Cohort Study
Supplemental material, sj-docx-1-aop-10.1177_10600280261459930 for Speed and Safety of IV Push Versus IV Piggyback Valproate Loading Doses: A Retrospective Cohort Study by Morgan Crawford, Riley Johnson and Andrew J. Webb in Annals of Pharmacotherapy
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AJW accepts consulting fees from Grace Therapeutics. The remaining author(s) report no conflicts of interest in this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.