
Abstract
Objective:
To summarize the clinical evidence for zopapogene imadenovec-drba (Papzimeos, Precigen Inc) in the treatment of recurrent respiratory papillomatosis (RRP), address pharmacy-specific operational considerations for this drug and provide an overview of emerging human papillomavirus (HPV)-directed immunotherapies that may expand the pharmacist’s role in RRP management.
Data Sources:
PubMed, Scopus, Google Scholar, and ClinicalTrials.gov (through May 2026); prescribing information; treatment guidelines; AMCP Format 5.0 dossier; and FDA clinical review.
Study Selection and Data Extraction:
Efficacy and safety data were derived from the pivotal PRGN-2012-201 trial (NCT04724980). Pipeline therapies were identified from IPD Analytics.
Data Synthesis:
In the phase 1/2 PRGN-2012-201 trial (n = 35 at recommended dose), zopapogene imadenovec demonstrated a 51% complete response rate at 12 months (43% at 24 months), an objective response rate of 66%, and no serious treatment-related adverse events. INO-3107, a DNA immunotherapy under FDA review, has shown complete response rates from 28% to 50% by year 2.
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs:
Zopapogene imadenovec-drba is the first FDA-approved therapy for RRP, a condition historically managed through repeated surgical debulking. Off-label adjuvant therapies such as intralesional cidofovir, bevacizumab, and HPV vaccination have been used with variable efficacy.
Conclusions:
The shift from primarily surgical management of RRP to HPV-directed immunotherapy creates an expanded role for pharmacists in high-cost drug stewardship (including formulary evaluation, manufacturer and payer engagement, and revenue cycle optimization), operational management (including procurement, ultra-cold storage, and biosafety handling), clinical monitoring, and patient education on a mechanistically novel therapy.
Keywords
Introduction
Recurrent respiratory papillomatosis (RRP) is a rare, chronic disease characterized by benign papillomatous growths throughout the respiratory tract, most commonly in the larynx. RRP is caused by human papillomavirus (HPV) infection, with HPV subtypes 6 and 11 responsible for roughly 90% of cases. 1
RRP-associated vocal fold lesions frequently can cause dysphonia, which can lead to significant patient distress. 1 In the Recurrent Respiratory Papillomatosis Foundation–Coordination of Rare Diseases (RRPF-CoRDS) international patient registry (n = 73), 97.3% of patients reported feeling debilitated by their diagnosis, 79.5% reported social anxiety, and 94.5% avoided career or social activities due to voice quality. 2 A larger analysis from the same registry (n = 122) found that 70% of respondents reported feelings of isolation, and 45.1% reported depression. 3
RRP has historically been managed with repeated surgical debulking, with approximately 20% of patients requiring four or more surgical procedures annually. 4 Surgery aims to remove papillomas while preserving the vibratory layers of the vocal folds to minimize scarring and further voice impairment. However, cumulative surgical trauma can result in iatrogenic complications such as anterior glottic webbing, interarytenoid scarring, endolaryngeal glottic stenosis, and vocal fold fibrosis. 5 The surgical burden of RRP can be extraordinary, with some patients having more than 100 procedures in a lifetime. 6 Adjuvant pharmacologic therapies, including intralesional cidofovir, bevacizumab (intralesional or systemic), and HPV vaccination (Gardasil 9), have been used off-label with variable efficacy to reduce papilloma recurrence. 7
Zopapogene imadenovec-drba (Papzimeos, Precigen Inc) is the first FDA-approved treatment for RRP. 8 It utilizes a nonreplicating gorilla adenovirus vector to deliver DNA encoding a fusion antigen derived from selected regions of HPV types 6 and 11 proteins. 8 Following subcutaneous injection, the vector enters host cells and delivers its genetic payload, leading to expression of HPV fusion antigen on the cell surface. This elicits a targeted T-cell-mediated immune response against HPV 6 and HPV 11 viral proteins. As a mechanism-based therapeutic approach, zopapogene imadenovec can provide durable disease control and reduce the need for repeated surgical interventions.
Because zopapogene imadenovec uses a viral vector to deliver genetic material into human cells, it meets the FDA’s regulatory definition of a gene therapy product.8,9 The FDA defines gene therapy as interventions involving the deliberate alteration of genetic material in living cells or the introduction of genetic material into cells to prevent, treat, or diagnose disease. 9 As a viral vector-based product that carries foreign DNA into host cells for expression, zopapogene imadenovec is regulated as a gene therapy and appears on the FDA’s list of approved cellular and gene therapy products. 10
The 2026 RRP Foundation Position Statement recommends HPV-specific immunotherapy as first-line medical treatment for patients seeking alternatives to repeat surgery, alongside HPV vaccination for all patients and baseline HPV typing and pulmonary imaging.7,11 These updates signal a pivotal shift from surgical management toward biologic and gene therapies for RRP, with direct implications for pharmacy practice.
Objective
The objectives of this review are to (1) summarize the clinical evidence supporting the safety and efficacy of zopapogene imadenovec; (2) address pharmacy-specific operational considerations including drug handling, storage, preparation, administration, formulary evaluation, and adverse event monitoring; (3) raise awareness of RRP as an underrecognized disease with substantial patient burden; and (4) provide an overview of emerging HPV-directed immunotherapies that will further expand the pharmacist’s role in the multidisciplinary management of this disease.
Data Sources
Sources were identified using PubMed, Scopus, Google Scholar, and ClinicalTrials.gov from database through May 30, 2026, using search terms “zopapogene,” “recurrent respiratory papillomatosis,” “respiratory papillomatosis,” “gene therapy,” “immunotherapy,” “adenoviral vector immunotherapy,” “RRP,” and “Papzimeos.” References of retrieved articles were screened to identify additional relevant studies. The manufacturer’s prescribing information and clinical treatment guidelines for RRP were reviewed for current treatment approaches and the role of zopapogene imadenovec. The AMCP Format 5.0 formulary dossier and the U.S. Food and Drug Administration clinical review were also evaluated.12,13
Study Selection and Data Extraction
The efficacy and safety of zopapogene imadenovec was supported by the pivotal PRGN-2012-201 trial (NCT04724980).8,14 Drugs currently under FDA review were identified from the IPD Analytics clinical pipeline database. 15
Data Synthesis
Zopapagene Imadenovec
PRGN-2012-201 was a single-center, open-label, single-arm phase 1/2 clinical trial conducted at the National Institutes of Health that enrolled 38 adults with severe, aggressive RRP requiring at least 3 surgical interventions in the 12 months prior to enrollment (Table 1).12-14 The trial tested 2 dose levels of PRGN-2012 (now marketed as Papzimeos), with 35 patients ultimately treated at the recommended phase 2 dose of 5 × 10¹¹ particle units administered as 4 subcutaneous injections over 12 weeks on days 1, 15, 43, and 85. Patients underwent surgical debulking before the first dose to establish minimal residual disease, with optional debulking procedures before the third and fourth doses if visible papilloma regrowth occurred. The enrolled population had a median age of 50 years, a median of 4 surgeries in the prior year, and a median of 40 lifetime interventions, reflecting severe disease burden. In the trial, 51% of patients (18/35) achieved complete response at 12 months, defined as no surgical intervention required in the year following treatment, and 43% (15/35) maintained a complete response at 24 months. Responses were durable, with 83% (15/18) of complete responders requiring no further interventions beyond 12 months at a median follow-up of 36 months (range 30-51 months), and with 3 patients having response lasting more than 4 years. 15 The objective response rate (complete plus partial response) was 66% (23/25, 95% CI 48-81), and 86% (30/35) of patients had fewer interventions in the 12 months after treatment compared with the 12 months before treatment.
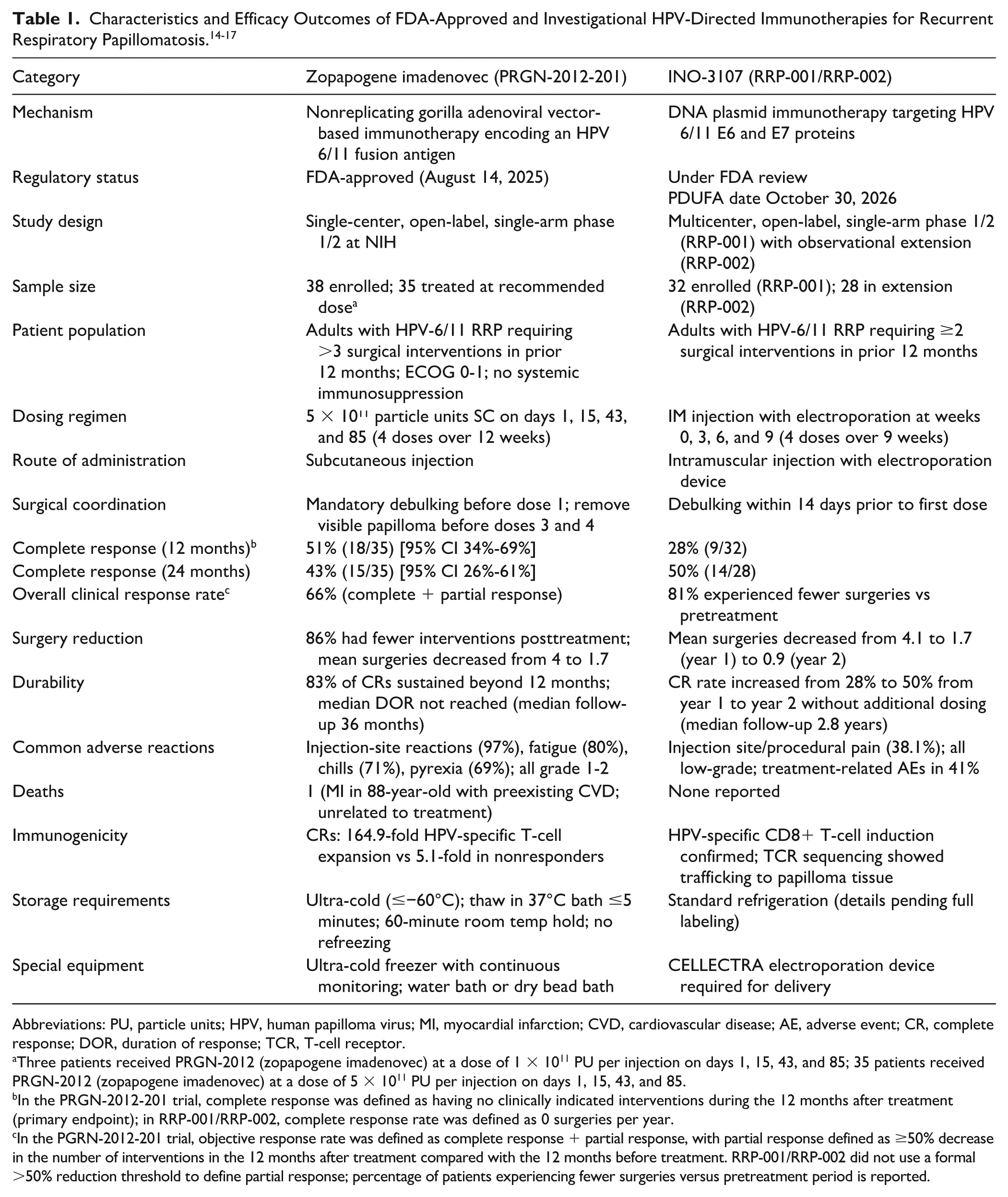
Abbreviations: PU, particle units; HPV, human papilloma virus; MI, myocardial infarction; CVD, cardiovascular disease; AE, adverse event; CR, complete response; DOR, duration of response; TCR, T-cell receptor.
Three patients received PRGN-2012 (zopapogene imadenovec) at a dose of 1 × 1011 PU per injection on days 1, 15, 43, and 85; 35 patients received PRGN-2012 (zopapogene imadenovec) at a dose of 5 × 1011 PU per injection on days 1, 15, 43, and 85.
In the PRGN-2012-201 trial, complete response was defined as having no clinically indicated interventions during the 12 months after treatment (primary endpoint); in RRP-001/RRP-002, complete response rate was defined as 0 surgeries per year.
In the PGRN-2012-201 trial, objective response rate was defined as complete response + partial response, with partial response defined as ≥50% decrease in the number of interventions in the 12 months after treatment compared with the 12 months before treatment. RRP-001/RRP-002 did not use a formal >50% reduction threshold to define partial response; percentage of patients experiencing fewer surgeries versus pretreatment period is reported.
There were no serious adverse events, no grade 3 or higher treatment-related adverse events, and no early treatment discontinuations.12-15 The most common adverse events were grade 1-2 and included injection-site reactions (97%), fatigue (80%), chills (71%), and fever (69%), which occurred most frequently after the first subcutaneous injection and typically lasted 1 to 3 days. There was 1 death from myocardial infarction followed by cardiogenic shock that occurred 7 months after treatment in an 88-year-old man with preexisting severe aortic stenosis, coronary artery disease, and chronic obstructive pulmonary disease, and was determined to be unrelated to treatments received in PRGN-2012-201.
Exploratory analyses showed that clinical responders had greater HPV 6/11-specific T-cell expansion (164.9-fold vs 5.1-fold in nonresponders) and a papilloma microenvironment characterized by lower baseline HPV gene expression, stronger interferon signaling, and greater T-cell infiltration, in contrast to the higher HPV/CXCL8 expression and neutrophilic infiltration seen in nonresponders.12-14 These immunologic differences aligned with clinical outcomes; complete responders achieved median reductions of 90% in Derkay score and 95% in Voice Handicap Index-10, compared to 32% and 14% in non-complete responders, respectively. 14
Emerging RRP Therapy
At the time of this writing, the only RRP treatment under FDA review is INO-3107, developed by Inovio Pharmaceuticals Inc, with a Prescription Drug User Fee Act (PDUFA) review date of October 30, 2026.16-18 INO-3107 is a DNA immunotherapy designed to elicit HPV-6 and HPV-11-specific T-cell responses. It is administered intramuscularly at weeks 0, 3, 6, and 9 using the CELLECTRA electroporation device (Inovio Pharmaceuticals Inc). This proprietary device delivers brief electrical pulses at the injection site, transiently increasing cell membrane permeability to enhance cellular uptake of the DNA plasmid up to 1,000-fold compared to injection alone. 19 The pivotal phase 1/2 study of INO-3107 (RRP-001; NCT04398433) enrolled 32 adults with HPV-6/11-associated RRP requiring at least 2 surgical interventions in the preceding year. 16 At 52 weeks, 81% (26/32) of patients experienced a reduction in surgical interventions compared to the pretreatment year, with HPV-specific CD8+ T-cell induction confirmed by RNA sequencing and T-cell receptor sequencing demonstrating trafficking to papilloma tissue. All treatment-related adverse events were low-grade (41% of patients), with injection-site or procedural pain being the most common. 17 Long-term extension data (RRP-002) with a median total follow-up of 2.8 years demonstrated continued improvement: mean surgeries decreased from 4.1 pretreatment to 1.7 in year 1 and 0.9 in year 2, with the complete response rate (0 surgeries/year) increasing from 28% in year 1 to 50% in year 2. No serious adverse events were identified during long-term follow-up. 20
Relevance to Patient Care and Clinical Practice in Comparison to Existing Drugs
Place in Therapy
The approval of zopapogene imadenovec marks a paradigm shift in RRP management, introducing the first FDA-approved systemic therapy for a disease historically managed primarily through repeated surgical debulking. Prior to this approval, off-label pharmacologic adjuncts including intralesional cidofovir, bevacizumab, and HPV vaccination (Gardasil 9) were used to reduce papilloma recurrence, although none has demonstrated predictable or curative efficacy (Table 2). 11
Pharmacologic Management of Recurrent Respiratory Papillomatosis (RRP). 11
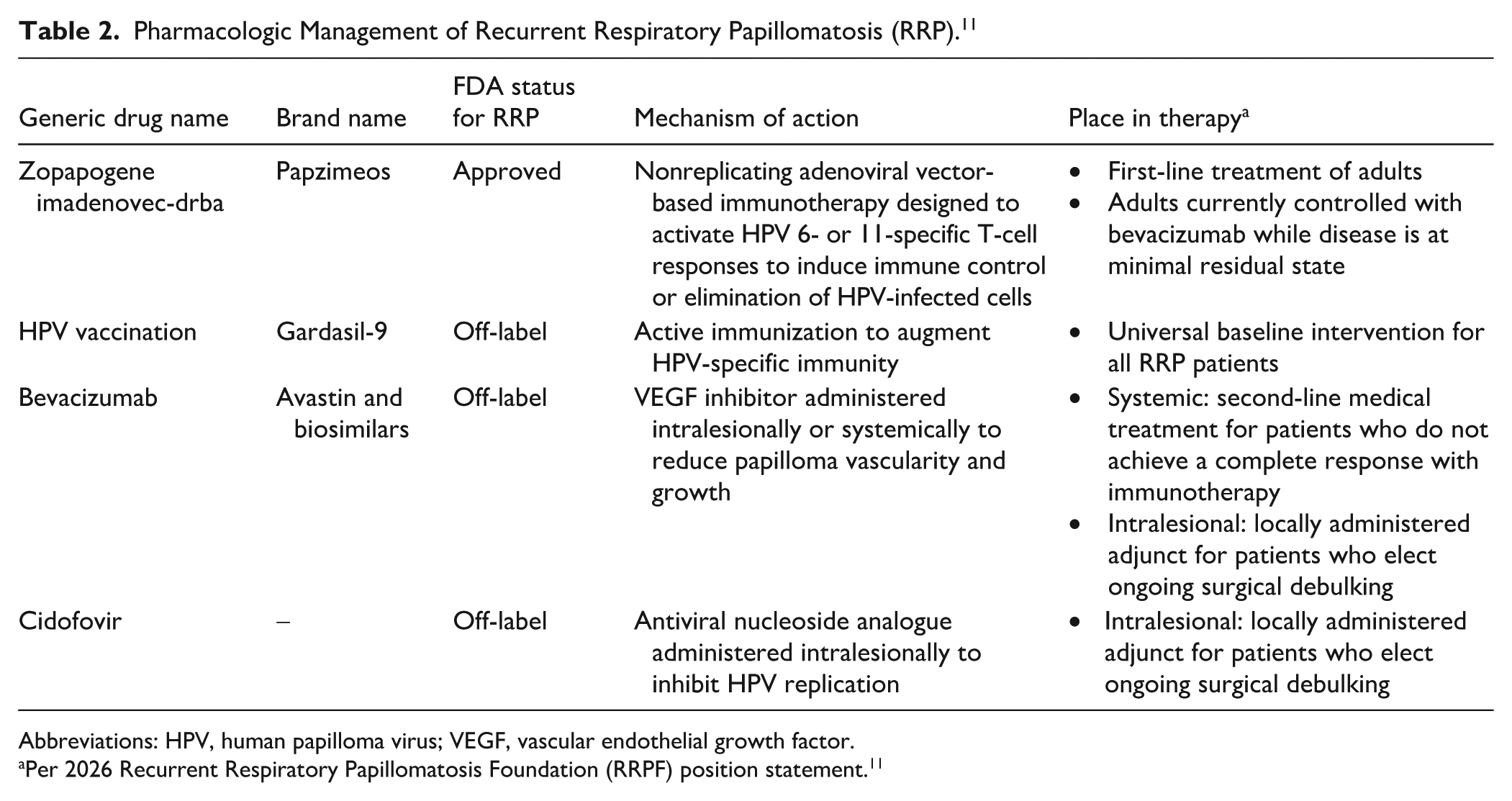
Abbreviations: HPV, human papilloma virus; VEGF, vascular endothelial growth factor.
Per 2026 Recurrent Respiratory Papillomatosis Foundation (RRPF) position statement. 11
The RRP therapeutic pipeline continues to expand, with each agent carrying distinct operational demands. Zopapogene imadenovec requires ultra-cold storage and specialized preparation, while INO-3107, an HPV-specific DNA immunotherapy currently under FDA review, would necessitate electroporation device coordination if approved. In addition, a 2026 systematic review and meta-analysis identified HPV-specific immunotherapies and PD-1/PD-L1–directed agents such as pembrolizumab (Keytruda, Merck Inc.) as showing encouraging early-phase activity; however, data remain too heterogeneous for quantitative pooling, and further studies are needed to define optimal sequencing and the role of checkpoint inhibition in RRP management. 20 This evolving landscape underscores the growing need for pharmacist expertise in the handling, delivery, and clinical integration of novel RRP biologics.
As the first FDA-approved therapy for RRP, zopapogene imadenovec introduces new pharmacist responsibilities in formulary evaluation, financial oversight, operational management, clinical monitoring, and patient education.
Formulary Evaluation and Access
Zopapogene imadenovec presents unique formulary evaluation challenges as a gene therapy for an ultra-rare disease.12,21 Because no prior FDA-approved pharmacologic treatment existed for RRP, there is no drug comparator against which to benchmark clinical or economic value. Traditional cost-effectiveness frameworks may not adequately capture the value of therapies such as zopapogene imadenovec that deliver potentially durable, disease-modifying effects in a single treatment course. 22 In the US multipayer system, the payer who covers the upfront treatment cost may not be the same payer who benefits from years of avoided surgical procedures; this creates a potential misalignment of incentives that traditional cost-effectiveness analyses do not address.22,23
The zopapogene imadenovec regimen requires 4 subcutaneous injections over 12 weeks (on days 1, 15, 43, 85), with mandatory surgical debulking before the first dose and removal of visible papilloma, if present, before the third and fourth doses. 8 This hybrid surgical-plus-immunotherapy model complicates cost modeling, as the total cost of treatment must incorporate procedural costs, anesthesia, and facility fees alongside drug-acquisition cost. Following FDA approval, Precigen set a list price of $115,000 per vial, or $460,000 for a full course of treatment. 24 Storage requirements (≤−60°C) add cold-chain infrastructure costs with continuous temperature monitoring and contingency planning for equipment failure.8,22 Institutions must weigh the short-term operational complexity of a single zopapogene imadenovec course (e.g., ultra-cold storage, biosafety handling, surgical coordination) against the long-term costs and resource utilization associated with repeated surgical interventions. Pharmacy-coordinated management of zopapogene imadenovec should encompass formulary evaluation, prior authorization navigation, specialty pharmacy procurement logistics, revenue cycle optimization, payer engagement, and contract negotiation to ensure sustainable institutional access.22,25
Procurement, Storage, and Preparation
Zopapogene imadenovec is supplied as a sterile frozen suspension at a concentration of 5 × 10¹¹ PU/mL in single-dose vials that must be kept at ultra-cold storage at ≤−60°C (≤−76°F). 8 When ready to administer, the product must be rapidly thawed in a 37°C water bath or dry bead bath with the vial held in an upright position until no visible ice crystals remain. Total exposure to the bath must not exceed 5 minutes, as prolonged heat exposure can compromise adenoviral vector capsid integrity through thermal stress and degradation. 8 Once thawed, the product has a maximum room-temperature hold time of 60 minutes and must not be placed back in the refrigerator, freezer, or on dry ice. 8 A 3-mL syringe with a filter-less 18G–22G needle should be used to withdraw the 1 mL dose from the thawed vial. After withdrawal, the needle is replaced with a 23G to 25G subcutaneous injection needle for administration. The cold-chain requirements, time-sensitive thawing protocol, and narrow administration window for zopapogene imadenovec underscore the importance of establishing robust standard operating procedures to ensure product integrity and safe delivery.21,25
Biosafety Handling
Since the NIOSH List of Hazardous Drugs does not yet include any FDA-approved gene therapies, institutions must independently conduct their own risk assessments for agents such as zopapogene imadenovec to maintain USP ∙800∙ compliance.26,27
The manufacturer’s prescribing information classifies zopapogene imadenovec as a viral vector-based product requiring universal biohazard precautions during handling, preparation, and disposal.8,27 Spills must be decontaminated with a virucidal agent (0.5% sodium hypochlorite or 6% hydrogen peroxide) for 15 minutes, and all contaminated materials must be disposed of in biohazard containers. 8 Pharmacy staff training should incorporate biosafety principles drawn from USP ∙800∙ and NIH biosafety guidelines adapted for viral vector products.8,26 Potentially contaminated materials from the injection site should be placed in sealable bags, with biohazard precautions maintained for 1 to 2 weeks post-injection. 8
Multidisciplinary Coordination
The zopapogene imadenovec dosing schedule of 4 injections over 12 weeks requires coordination with surgical debulking—mandatory before the first dose and as needed before the third and fourth doses. 8 This creates a unique operational challenge requiring alignment between otolaryngology scheduling and pharmacy dispensing timelines. Pharmacists are well positioned to develop clinical pathways and standard operating procedures that integrate surgical scheduling, product preparation, and administration workflows, particularly in institutions where otolaryngologists may have limited experience with systemic immunotherapies. 28
Clinical Monitoring and Patient Education
Pharmacists can play a central role in patient education and safety monitoring throughout the zopapogene imadenovec treatment course. Before treatment initiation, patients should be counseled on expected adverse reactions, including injection-site reactions, fatigue, chills, and pyrexia. In clinical trials, these adverse effects occurred most frequently after the first dose and typically resolved within 1 to 3 days. 8 Following the initial administration, patients must be monitored for injection-site reactions for at least 30 minutes. 8 The prescribing information also includes a warning regarding thrombotic events, as adenoviral vector-based therapies are associated with the potential development of prothrombotic antibodies. Patients should be educated on warning signs of thrombotic events, including shortness of breath, chest pain, leg swelling, and neurological symptoms such as severe headache or blurred vision. 8
Beyond safety counseling, pharmacists are well positioned to address the broader educational needs of patients with RRP. Many of these individuals have endured years of repeated surgical interventions, and the introduction of a mechanistically distinct immunotherapy may prompt questions about treatment expectations and outcomes. Pharmacists can reinforce the importance of completing the full 4-dose regimen and help patients understand the fundamental difference between surgical debulking, which reduces symptomatic papilloma burden, and immunotherapy with zopapogene imadenovec, which is designed to generate an immune response against the underlying HPV infection.
Unmet Needs and Future Directions
While the approval of zopapogene imadenovec addresses a critical unmet need in adult RRP, significant gaps in the evidence base and therapeutic landscape remain. Zopapogene imadenovec is approved only for adults, leaving pediatric and juvenile-onset RRP without an approved systemic therapy. 8 INO-3107, an investigational DNA immunotherapy targeting HPV 6/11, has demonstrated increasing complete response rates from 28% in year 1 to 50% in year 2 in adults and may expand the immunotherapy landscape if approved.16,17 Optimal sequencing of immunotherapy relative to off-label agents such as bevacizumab, the role of combination treatment strategies, and the potential integration of checkpoint inhibitors remain areas of active investigation. 20 As the RRP therapeutic landscape continues to evolve, pharmacists will play a key role in developing institutional protocols, tracking clinical outcomes, and participating in registries to further define the place in therapy of emerging treatments.
Conclusions
As the first FDA-approved RRP therapy, zopapogene imadenovec represents a paradigm shift from symptomatic surgical management to mechanism-based immunotherapy. With emerging HPV-directed agents such as INO-3107 advancing through the clinical pipeline, the pharmacist’s role in multidisciplinary RRP care will continue to expand. Pharmacists are integral to every stage of care delivery, including cold-chain management, thawing and preparation, biosafety handling, clinical monitoring, financial oversight and tracking, payer approval workflows, and patient education. Equipping pharmacists with the knowledge and institutional infrastructure to support these novel biologics will be essential to achieving safe, effective, and sustainable access for patients with RRP.
Footnotes
Acknowledgements
The author wishes to acknowledge colleagues within Stanford Health Care pharmacy and multidisciplinary committees whose formulary and institutional review processes informed this manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.