
Abstract
The recent release of the RAND survey of internal medicine education has garnered attention largely because the study was commissioned by the Medicare Payment Advisory Commission (MedPAC), an independent Congressional advisory body, which wields the specter of federal cuts to crucial indirect medical education monies. These funds are critical to the bottom line at our nation’s academic health centers. Although the survey has many inherent limitations, it has called attention to shortcomings in the current state of graduate medical education in the United States. 1
Important criticisms of the RAND methodology include the failure to survey a critical number or representative sample of training programs and the challenging topics in the competencies of problem-based learning, systems-based practice, and interpersonal and communication skills. Nonetheless, there is a growing consensus, developed over the past decade, that training for residents in internal medicine is lacking in key skills critical to the evolving health care environment. In the Health Professions Education Summit held in June 2002, leaders focused on the importance of delivering patient-centered care, working as part of interdisciplinary teams, practicing evidence-based medicine (EBM), focusing on quality improvement (QI), and using information technology (IT). 2 This report provided a road map that built on earlier calls for change from the Council on Graduate Medical Education and other health care leaders.3,4
Medical educators have begun to evolve education in a number of important ways and on both small and large scales.5-7 However, these efforts have been limited as attention in medical education has been diverted to important but noncurricular issues such as duty hours and health insurance reform. It is clear from the dialogue coming from Washington that educators must accelerate the pace of change. 8
This commentary reviews the conclusions of the RAND study of medical education in internal medicine and discusses what steps would need to be taken to meet the challenges as described by the RAND authors. Although some would continue to challenge their methods, we propose meeting the challenge head-on and discuss specific recommendations to more effectively prepare residents for practice in the 21st century.
RAND Report
Investigators from RAND conducted semistructured 60-minute interviews with a random sample of 26 of a total of 381 eligible internal medicine program directors representing 320 allopathic, 45 osteopathic, and 16 dual-accredited residency programs. Although marginally representative, the sample did meet MedPAC’s request for 25 interviews. The interviews explored 5 areas: 3 Accreditation Council for Graduate Medical Education (ACGME) competencies as well as care setting and IT infrastructure. The 3 ACGME competencies included practice-based learning and improvement, systems-based practice, and interpersonal and communication skills. There were specific areas of focus within these domains (Table 1).
ACGME Core Competencies Targeted by the RAND Interviewers
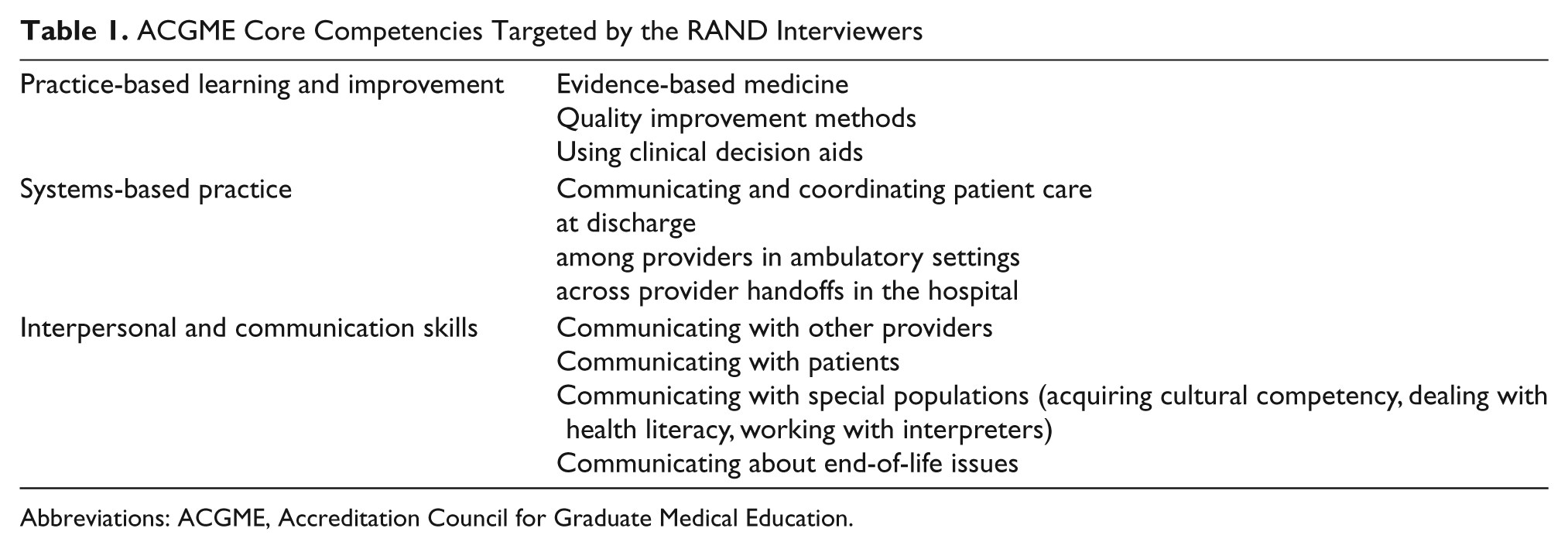
Abbreviations: ACGME, Accreditation Council for Graduate Medical Education.
The RAND interviewers identified areas of inconsistent education. The results were not surprising given the challenging areas of inquiry.
On analyzing the key findings of the RAND report, it is clear that the most work is required to enhance education concerning the very topics highlighted in the Institute of Medicine report from 2003. The RAND authors highlight that although internal medicine residency programs are adapting their curricula “there is substantial variation in programs’ approaches to, and implementation of, instruction in the topics of interest.” The report added that “teaching in these topics remains inconsistent and far short from that needed compared to what is recommended by various expert reports.” This report lacked any discussion of marshalling the resources to enhance curricula in the areas of concern.
In the competency of practice-based learning and improvement, one of the greatest needs is to collect and provide feedback of quality data to residents. EBM is easily covered, as the report confirms, through EBM conferences embedded in the residency didactic curriculum. Where the real need lies is in value-added QI programs that are tangible and connected to the work product of individual residents. Although the ACGME requirements emphasize the importance of this QI activity, they do not specify necessary and specific resources. This has led to disjointed and informal processes that lack real-life impact. To achieve this, having dedicated staff to collect and report data on actual resident performance is essential. This will require that hospital QI or case management staff, not typically under the reporting structure of the teaching program, develop and implement staffing to provide residency programs with specific data on key quality performance measures.
Recommendation 1: Sponsoring institutions should provide dedicated quality improvement staff (2 full-time employees/60 trainees) to collect resident-specific data on areas of importance to the nation’s health.
In the competency of systems-based practice, there needs to be a formal team process on rounds for coordinating and communicating patient care. These authors have witnessed the success of one such program initiated at Thomas Jefferson University Hospital in the form of “huddle rounds,” which bring nurses, physicians, therapists, and case managers together for a verbal exchange on important aspects of patient care each day.
Recommendation 2: Programs and sponsoring institutions should work together to mandate team-based rounds with direct face-to-face contact among nurses, physicians, therapists, and case mangers. Teams should be geographically based.
Recommendation 3: Sponsoring institutions should provide funding for teaching in the areas of medical economics, cost-effectiveness, and resource utilization. It is strongly recommended that programs utilize outside expertise to enhance trainee knowledge in these areas. Programs should incorporate didactic instruction in the fundamentals of health systems, health care economics, and public policy.
Recommendation 4: Programs should expand formal training in teamwork and provide specific evaluation of this skill among trainees by expert observers.
In reflecting on the final area addressed in the competency of systems-based practice, there appears to be wide recognition of the important role handoffs play in ensuring quality care overnight and on weekends. Despite this recognition, specific education in handoffs and sign-outs is often lacking. Training programs require dedicated faculty who can oversee and enhance sign-out methods and focus on quality and safety, particularly at night. This need has been reinforced by critical incidents nationally.9,10
Recommendation 5: Sponsoring institutions and programs should provide IT systems for electronic sign-out that is HIPPA (Health Insurance Portability and Accountability Act) compliant, readily accessed, and accurate with key data for night floats and covering medical teams.
Recommendation 6: Sponsoring institutions should provide funding for nocturnal teaching and monitoring of sign-outs and sign-ins to enhance skills in transitions of care, which are especially critical in the new duty hours environment.
In the competency of interpersonal and communication skills, there is a special need for cultural competency and communicating with patients who have special needs. Although this area fared well in the RAND report, receiving the least amount of criticism, the report offered no assessment of outcomes in critical areas such as health literacy in ambulatory clinics or effectiveness in dealing with end-of-life situations.
There is widespread agreement that IT infrastructure in the form of an electronic health record (EHR) is essential for state-of-the-art education in internal medicine. Essential elements include computerized physician order entry (CPOE), e-prescribing, access to test results and consultant opinions, and documentation of care.
Recommendation 7: Sponsoring institutions and programs must provide CPOE for inpatient experiences. Outpatient experiences should be supported by a robust EHR.
Conclusions
With the publication of the RAND report, Congress will begin to scrutinize the curricula at training programs nationally to identify whether they are getting value for the dollars invested in graduate medical education. Our recommendations would require a regulatory imperative from accrediting bodies, such as the ACGME, in order to gain traction. However, these recommendations hold the promise of truly transforming the educational landscape at our academic health centers.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.