
Abstract
Surgical mortality is considered a benchmark for measuring quality of care. This study quantifies the incidence of death on the day of elective pediatric surgery, which generally is considered preventable and might be considered a “never” event. The authors conducted a retrospective analysis of national state inpatient databases from 1988 to 2007 that included elective pediatric surgical patients. A descriptive analysis of same-day mortality by demographics, surgical specialties, and age was performed. Of 835 880 elective pediatric surgical cases identified, 174 patients died on the day of surgery—that is, 2.1 deaths/10 000 cases. Surgical specialty mortality rates ranged from 0.06 (otolaryngology) to 17.4 (cardiothoracic surgery) deaths per 10 000 cases. Death on the day of elective pediatric surgery is rare, limiting its utility to compare performance in pediatric surgery. However, this metric may be useful at individual institutions as a case-finding tool for root-cause analysis in quality improvement efforts.
Beginning with the Institute of Medicine’s report, To Err is Human, 1 published more than a decade ago, there has been an increasing national emphasis on patient safety and surgical quality. This has been manifest in linking reimbursement to quality as well as in the increase in funding and resources geared toward looking at comparative effectiveness and outcomes in health care as measures of patient safety and quality. 2 Different methodologies have been used to measure and report patient safety events, including incident reporting systems, manual medical error review, and administrative data. 3 To standardize a method to detect potentially preventable and harmful events, the Agency for Healthcare Research and Quality (AHRQ) has developed patient safety indicators (PSIs), which use software to identify potential adverse events using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. 4 These PSIs are designed to screen for medical errors resulting in a potential compromise to patient safety, thus helping hospitals identify areas of potential improvement.
However, PSIs are not designed to include all preventable and adverse events. There remains a need for health care facilities to continue to report events that are amenable to systematic learning and improvement. “Never” events are serious reportable medical errors that result in a serious compromise in patient safety and are considered completely preventable. The National Quality Forum has defined 28 events divided into the following categories: surgical, device, care management, patient protection, environmental, and criminal events. Within surgical care, these events include surgery performed on the wrong body part or on the wrong patient, the wrong surgery performed, the unintended retention of a foreign object, or intraoperative/immediate death in an American Society of Anesthesiologists class I patient. 5 An increasing number of hospitals are mandated to report these occurrences, with the ultimate goal being efforts for quality improvement.
Most quality improvement programs to date have begun with the adult population. Although many of these measures apply to the pediatric population, there are significant differences between adults and children that present challenges when assessing health care quality in children using adult indicators. For instance, compared with adults, children are more likely to live in poverty, are treated more often for acute illnesses and preventive care and less often for chronic conditions, are dependent on caregivers, and undergo rapid physical, cognitive, social, and emotional developmental changes.6,7 In an effort to identify markers for quality of care and patient safety in the pediatric surgical population, we evaluate same-day postoperative mortality from elective surgery. Generally, this is considered rare and preventable and, therefore, might be considered a “never” event. In this study, we look to specifically quantify the rate of death on the same day of elective pediatric surgery and thus consider its utility as a reportable quality metric.
Methods
This study was deemed exempt by the Johns Hopkins Hospital Institutional Review Board.
Databases Used
A retrospective analysis was performed using 20 years of data from the Nationwide Inpatient Sample (NIS; 1988-1996, 1998, 1999, 2001, 2002, 2004, and 2007) and the Kids’ Inpatient Database (KID; 1997, 2000, 2003, 2005, and 2006). The KID was used for the years it was available and the NIS for the remaining years. Both databases are made available from the Healthcare Cost and Utilization Project (HCUP), which is sponsored by AHRQ.8,9 The NIS contains information from approximately 8 million inpatient hospitalizations per year, approximating a 20% stratified sample of US community hospitals. The data are from 1988 to 2007, allowing analysis of trends over time. The number of states participating in the HCUP has increased in each year, such that NIS 2007 contains data from 1044 hospitals in 40 states. 8 The KID contains data from as many as 38 states in 2006 and includes up to 3 million pediatric (younger than 21 years of age) hospital discharges. These pediatric discharges are obtained from 2500 to 4000 US community hospitals. Although the NIS samples at the hospital level, the KID samples individual discharges that are then weighted to obtain national estimates. 9 Both databases contain patient-level variables (ie, age at admission, sex, race, diagnosis and procedure information using ICD-9-CM codes, total hospital charges, discharge location, insurance status, and length of stay) as well as hospital information (state, urbanicity, teaching status, and bed size).8,9
Patient Selection
Pediatric (<18 years of age) surgical patients were identified according to ICD-9-CM procedure codes published by AHRQ for operating room procedures. 10 Inclusion criteria consisted of patients younger than 18 years of age who had an elective admission status, underwent a surgical procedure as defined by ICD-9-CM procedure coding, and died on the same day as the procedure. Patients with ICD-9-CM coding consistent with organ donation were excluded from the study. Our outcome of interest was rates of death on the day of elective surgery. The numerator was any patient who was coded for a surgical operation and died on the same calendar day. The denominator was all patients who met the inclusion criteria. This rate was displayed in number of deaths per 10 000 cases.
Analysis
A descriptive analysis was performed of same-day mortality rate by patient and hospital characteristics, including sex, race, age at presentation, patient comorbidities as defined by counts of concurrent ICD-9-CM diagnosis codes,11,12 hospital demographics, insurance status, and total hospital charges. Different methods have been described for risk stratification, such as comorbidity indices. However, availability of these methods is limited for children. Thus, this study incorporated counts of number of diseases as a measure of comorbidity as referenced in the literature by de Groot et al. 11 Total hospital charges were adjusted for inflation to reflect 2007 dollars. 13 Because a higher risk of mortality has been associated with pediatric patients younger than 1 year, 14 we compared same-day mortality rates across age categories. We stratified same-day death rates by age (<1 year, ≥1 year). Further division of age groups for patients older than 1 year of age was not performed because of the rare occurrence of the event for those ≥1 year of age.
Diagnosis-related group (DRG) procedure codes were used to group patients into the following procedure categories: cardiothoracic, general/gastrointestinal, orthopedic, neurosurgery, transplant, and otolaryngology. Comparisons of same-day mortality rate by DRG category were performed for the total number of patients and then also divided by age category (<1 year, ≥1 year).
Results
Patient Demographics
A total of 835 880 patients younger than 18 years of age were found to have undergone elective surgical procedures. Among these, 174 patients died on the same day as their surgery. As shown in Table 1, there was no significant difference in deaths between boys and girls in total and in both age categories. There was no significant difference in sex or race distribution by age category. Infants were disproportionately represented among those who died on the same day as their elective surgery. The median total number of comorbidities for those who died on the same day of surgery was 4, which was the same for those <1 year and those ≥1 year.
Demographics of Patients Who Died on the Day of Surgery
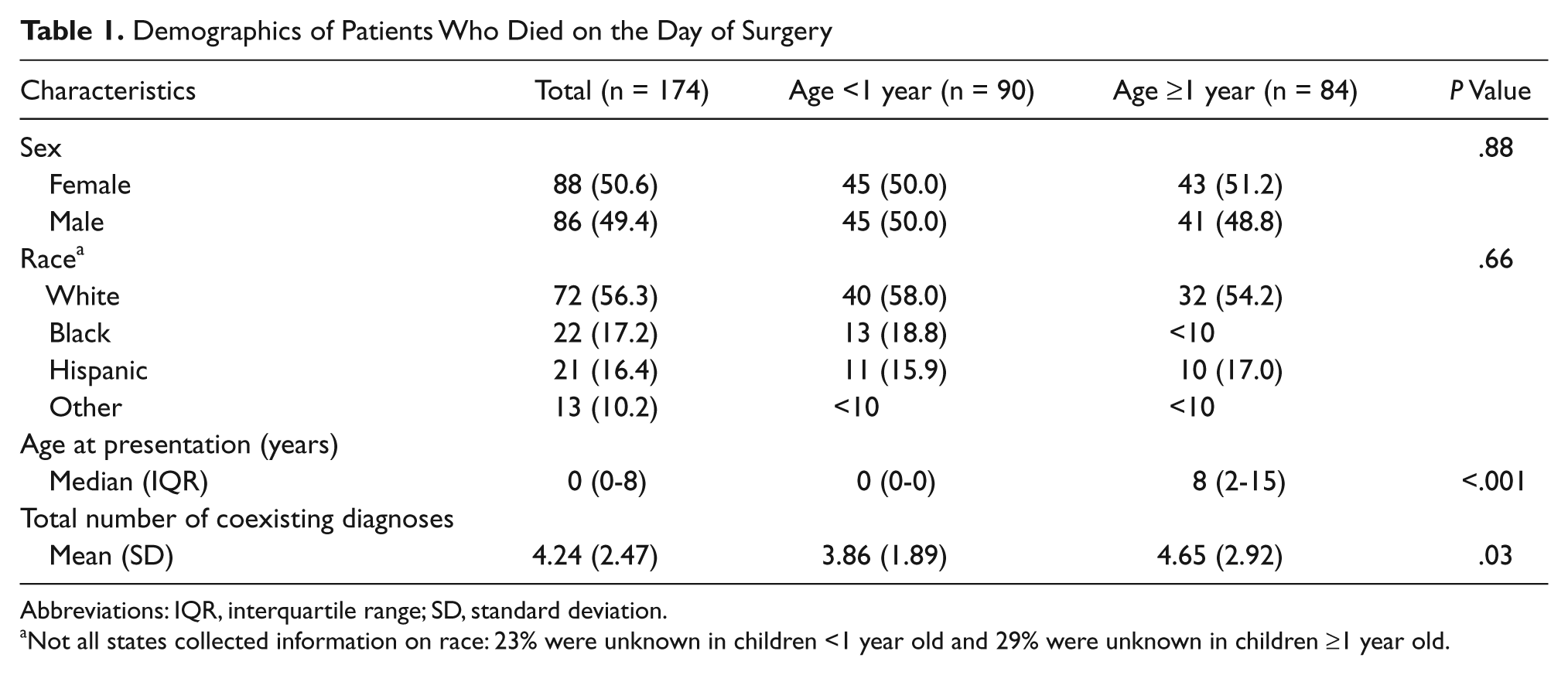
Abbreviations: IQR, interquartile range; SD, standard deviation.
Not all states collected information on race: 23% were unknown in children <1 year old and 29% were unknown in children ≥1 year old.
Of these 174 patients, 9 were transferred from an outside hospital, 3 were admitted from a long-term care facility, 4 were from the emergency room, and the balance were either routine admissions to the hospital (152) or had no information regarding these issues (6).
Hospital Characteristics
Table 2 shows that geographic distributions were not significantly different between age categories. The vast majority of cases occurred within urban teaching hospitals. The difference between age groups with regard to having insurance was not statistically significant. Differences in total hospital charges between age groups also were not statistically significant.
Hospital Characteristics for Patients Who Died on the Day of Surgery
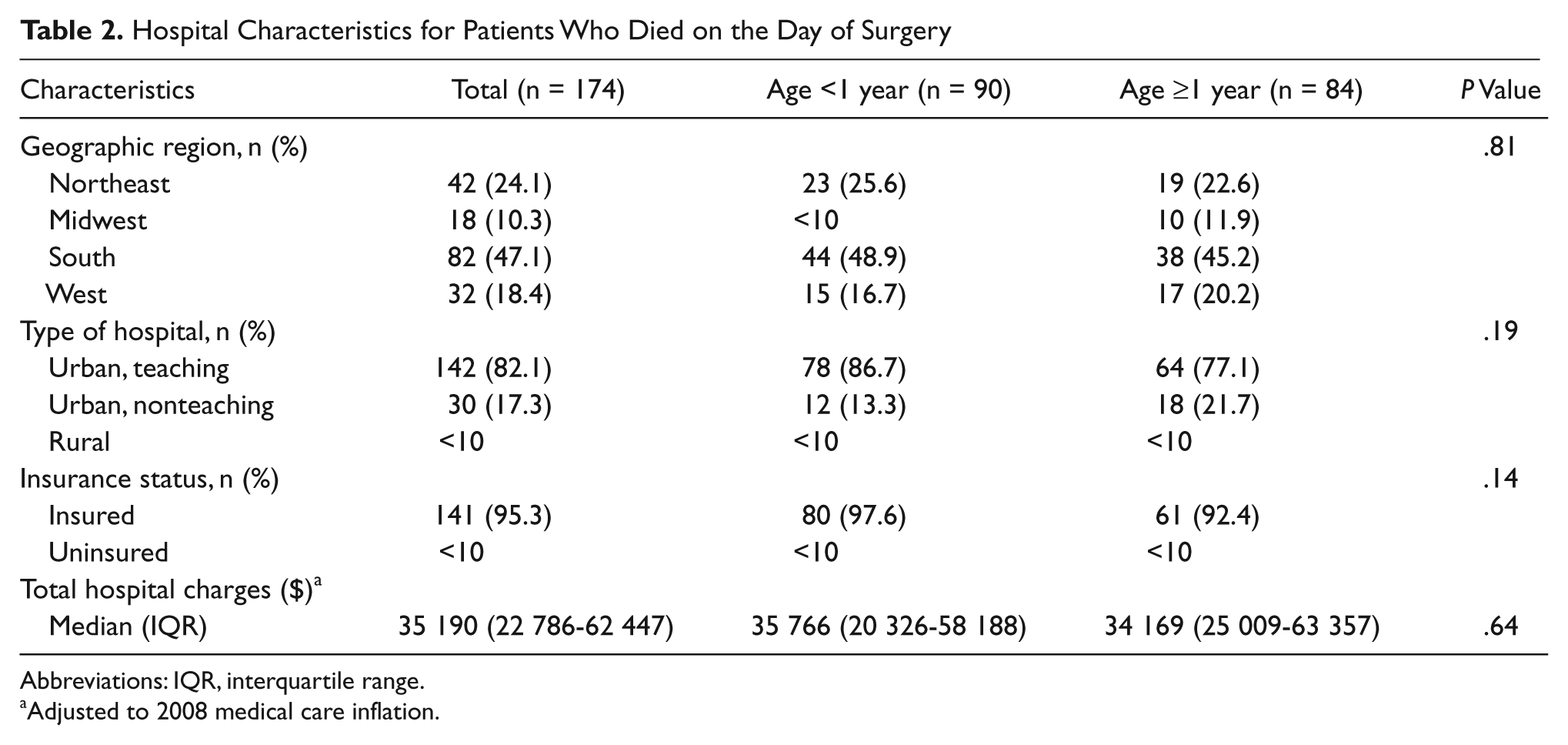
Abbreviations: IQR, interquartile range.
Adjusted to 2008 medical care inflation.
Mortality Rates
Table 3 shows the total mortality rate on the day of elective pediatric surgery. Within this sample who underwent elective pediatric surgery, total mortality rate was highest for cardiothoracic surgery, followed by transplant surgery.
Same-Day Mortality Rate by DRG Categories
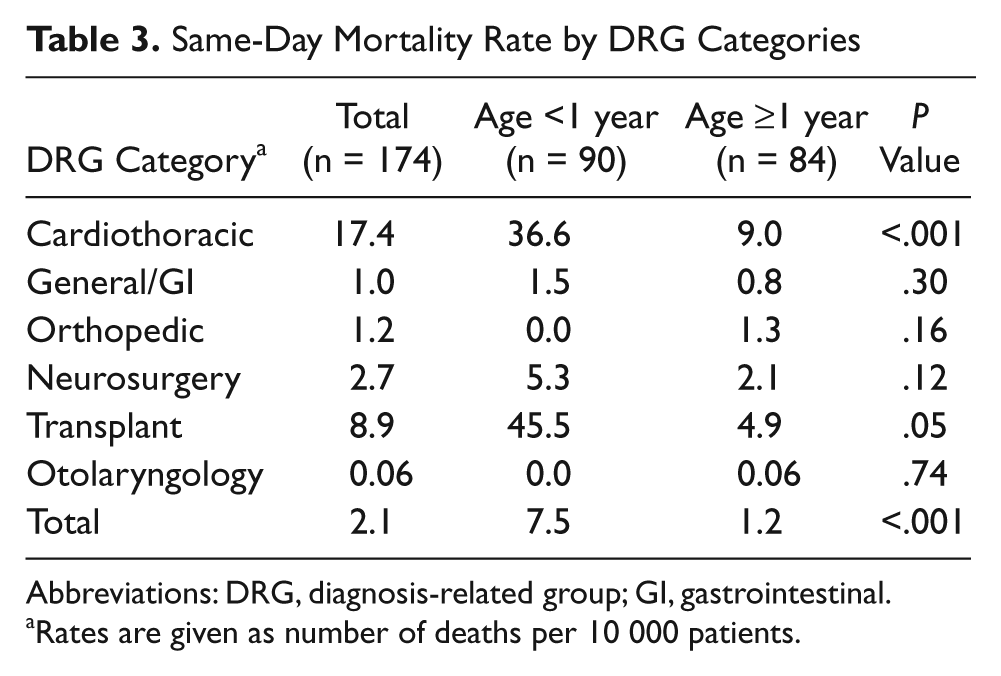
Abbreviations: DRG, diagnosis-related group; GI, gastrointestinal.
Rates are given as number of deaths per 10 000 patients.
Table 3 shows that, when stratified by age, the same-day mortality rates are higher for infants compared with children in all categories except orthopedic and otolaryngology. However, the differences are significant only for cardiothoracic and transplant surgeries.
Discussion
Standardized quality metrics to quantify safe surgery in children have yet to be well defined. Inpatient mortality as well as the incidence of pediatric PSIs are among measures being proposed for widespread benchmarking and hospital comparison to assess surgical outcomes in children. In the present study, we characterized a subset of pediatric surgical patients who died in the hospital on the day of elective surgery based on the premise that death after an elective case potentially may be more preventable. Accordingly, the present study is the first to present national data to quantify the occurrence of death on the day of elective pediatric surgery over a period of approximately 20 years. With an overall same-day mortality rate of 2.1 per 10 000 cases, such events were infrequent. For children <1 year of age, the rate of same-day mortality was more than 6 times higher when compared with that for older children. This age trend is consistent with what has been described previously in the pediatric literature regarding inpatient mortality, 14 both surgical and nonsurgical. The majority of the existing literature on pediatric surgical mortality involves cardiothoracic surgery,15-17 which showed the highest rates of same-day mortality among all surgical specialties examined in this study. Given the significant morbidity associated with the natural history of many of the underlying disease processes (eg, congenital heart disease or organ failure), it is not surprising that these operations performed for life-threatening illness have higher mortality rates than other elective operations in the study. Although cardiothoracic surgery was the most common specialty with death on the same day of surgery in this study, there was a decreasing trend in mortality over time. This is likely attributable to multiple factors, particularly to improvements in overall critical care, including increased use of extracorporeal membrane oxygenation and ventricular assist devices.
Operative mortality traditionally has been defined as death occurring within 30 days of operation. 18 In looking at same-day death for elective surgery, this study seeks to find sudden or immediate deaths occurring in the stable patient that result from nonurgent procedures, intending to capture events that are beyond the expected risks of an operation. For same-day mortality to be a statistically useful indicator of surgical quality for comparisons across providers, procedures under evaluation ideally would have a high mortality rate and be performed frequently.19,20 Because of its infrequent occurrence, death on the day of elective surgery is of limited use as a measure of direct comparison across institutions or providers. However, same-day mortality after elective pediatric surgery meets the criteria for a serious reportable event that can be used as a case-finding tool and should be given consideration in the ongoing development of safety metrics for the pediatric population. The National Quality Forum, a nonprofit national coalition of physicians, hospitals, businesses, and policy makers, uses specific inclusion criteria for a list of serious reportable events in health care. These criteria include events that are of concern to both the public and providers, clearly identifiable and measurable in a reporting system, and of a nature such that the risk of occurrence is significantly influenced by the policies and procedures of the health care facility. 5 Death on the day of elective pediatric surgery is concerning and clearly identifiable, potentially preventable, and can be affected by hospital system policy and procedures. Thus, reporting of these events can be used as a case-finding tool for root-cause analysis for quality improvement efforts in the pediatric population.
As mentioned, death on the same day as elective surgery in children is an uncommon event. Thus, large sample populations are required to capture these rare outcomes. Administrative databases are extremely useful for this type of study because their large sample size encompasses a sizable number of events for evaluation. The databases used for this study, the NIS and KID, are nationally representative databases with information from 40 states. The NIS contains 20 years of discharge data for approximately 8 million inpatient hospitalizations per year, and the KID contains data from 2 to 3 million hospital discharges for children.8,9 Both databases are relatively inexpensive, easy to use, and readily available. These characteristics of the NIS and KID allow the rare event of death on the day of elective pediatric surgery to be a readily accessible and nationally representative quality metric.
However, there are important limitations to using death on the day of elective pediatric surgery as a quality metric. First is defining death on the day of surgery. The databases allow recognition of the day of surgery and day of death, but do not give information on specific time, which may lead to missing several cases. For instance, if a patient receives an elective operation in the evening but dies immediately after midnight, he or she would not be included in our study, although a patient who had surgery early in the morning and dies just before midnight would be included. Thus, the data do not standardize how close to the operation these deaths occur.
Another limitation of using death on the same day of elective pediatric surgery is the lack of clinical information provided by administrative databases. Although patients are presumed to be stable prior to surgery, given that only elective surgeries were included in the study, one cannot assume that all levels of comorbidities, risk factors, and risks of the surgery itself are comparable. An obvious example is that the risks associated with cardiac surgery for a congenital defect are different from those for an inguinal hernia in a child. High-risk operations such as those in transplant and cardiac surgery are expected to have higher mortality, as shown in our results, raising the question of whether the deaths captured in our study in the high-risk surgery categories are preventable. Clinical information for risk adjustment, which is difficult to establish from administrative data, would help define which events are potentially preventable and improve the utility of death on the day of elective pediatric surgery as a reportable event for quality improvement.
A third limitation of this study is that these databases are dependent on accurate data entry, which is variable by institution and over time. Studies have been performed evaluating the validity of administrative data for measuring mortality rates, with 1 study finding that mortality rates from administrative databases were higher compared with those in clinical databases. 15 This highlights the need for a standardized and reliable method of data entry across institutions and also warrants caution in the use of this information by various stakeholders to compare quality of care and patient safety between health care providers and institutions.
Conclusion
Death on the same day of elective pediatric surgery is a rare event. However, a certain percentage of these events is likely to be preventable, even for surgical operations that carry a greater risk. Thus, while not common enough of an event for direct comparison of quality in pediatric surgery, death on the day of surgery may be a potentially useful metric worthy of tracking as a serious reportable event for quality improvement in pediatric care.
Footnotes
Acknowledgements
The authors would like to thank the Robert Garrett Fund for Treatment of Children, which helped support this study.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Robert Garrett Fund for Treatment of Children helped support this study.