
Abstract
Adverse events occur in 3% to 16% of hospital patients, half of these during surgery and related to human error. The authors’ objective was to determine the impact of a crew resource management program in collaboration with Swiss International Airlines. Participants included operating room personnel: surgeons, anesthesiologists, nurses, and technicians. Outcome measures were a 10-item questionnaire evaluating participants’ satisfaction and a 32-item survey to analyze participants’ learning. Nine seminars included 99 participants: 22% surgeons, 19% anesthesiologists, 29% nurses, and 30% nurse’s aides/technicians. Satisfaction was very high for course organization (91%), group dynamics (74%), and teaching methods (68%). Significant improvements in learning were observed after the course in 17 out of 32 questions. Surgeons demonstrated the greatest improvement in knowledge (P = .018), specifically teamwork and safety-related issues. Less improvement was seen for all specialties in stress recognition areas. Crew resource management is valuable in improving operating room staff knowledge regarding teamwork, safety climate, and stress recognition. However, program impact varies with participant specialty.
Three percent to 16% of patients will experience an adverse event during their hospital stay.1-4 Between 28% and 51% of these events could be considered preventable and related to human error.1,2,4,5 Human factors leading to errors have been studied extensively in aviation, and it has been known since the early 1980s that human weaknesses such as poor teamwork among cockpit crews contribute to half of all accidents. 6 This led to the introduction of crew resource management (CRM) programs aimed at improving teamwork and communication among flight crews. 7 These programs place a strong emphasis on the process of training crews to communicate and work together as a team.8-10 Such programs aim to develop shared behaviors to improve safety, specifically team resources rather than individual resources. To reduce human error and improve teamwork and communication, an increasing number of hospitals have introduced CRM programs derived from aviation. The implementation of such programs has been associated with several organizational changes, 11 including enhanced personal commitment to patient safety, an increase in the use of checklists and self-reported incidents, 12 improved communication between surgeons and anesthesiologists, 13 better operating room (OR) teamwork, 14 fewer equipment issues, decreased OR delays, 15 and, perhaps the most important benefit, reduced surgical mortality. 16
CRM programs generally are organized as 1- or 2-day group sessions for all OR personnel (surgeons, anesthesiologists, nurses, technicians) to improve communication and coordination in multidisciplinary settings. However, they frequently are designed as stand-alone programs regardless of the participants’ professional culture, which can vary significantly depending on participants’ specialties and whether they are physicians, nurses, or technicians. 17 It is currently unknown how these programs are perceived and how they affect participants, depending on their background and professional culture.
The purpose of this study was to analyze the impact of a CRM program on satisfaction and learning among OR personnel of a tertiary hospital and to compare its specific impact on surgeons, anesthesiologists, nurses, nurse’s aides, and technicians.
Methods
This study was performed in the Department of Surgery of the Geneva University Hospitals, Geneva, Switzerland. This is the only public hospital in the region. It is a 2200-bed health care center that provides primary and tertiary care to the canton of Geneva and the surrounding area (population of approximately 800 000). There were 12 979 surgical interventions performed in 2009. To improve surgical outcomes, we successively introduced a surgical safety checklist 18 and a CRM program. The checklist was launched in July 2009 and comprised 28 items assessed at 3 points in time during the operative procedure (sign in, time out, sign out). The CRM program was introduced in November 2009 and was developed in collaboration with Swiss International Airlines. It was designed as a 1-day group seminar, chaired by an instructor from Swiss and a senior orthopedic surgeon with experience in medical education. Participation was compulsory for all OR staff members of the hospital (surgeons, anesthesiologists, nurses, nurse’s aides, and technicians). Each specialty was instructed to provide 2 to 3 persons in order to achieve a total of 10 to 12 persons for the seminar.
The course seminar is based on 3 interactive workshops complemented by specific lectures. The training day starts with an introductory course on safety in aviation, exploring similarities between aviation and surgery, and providing an overview of the mechanisms underlying medical errors. Participants are then invited to share personal errors as a starting point to an interactive workshop on error management and harm reduction. This course section is completed by a brief lecture on oral communication with special emphasis on the advantages of closed-loop communication and feedback. The second part of the training day centers on conflict resolution. Participants are involved in role-play to experience how the “win-lose” approach may endanger the ability to achieve a common goal, as compared to the “win-win” attitude. The last part of the workshop aims to improve participants’ understanding of the use and benefits of the surgical safety checklist. The day closes with an overview of the group dynamic and the phases of group formation.
To assess the impact of the training program on participants’ satisfaction and learning characteristics according to profession and specialty, 2 different questionnaires were administered to all participants of the course between November 2009 and September 2010. The first is a standardized 10-item questionnaire developed by the hospital training center. It explores 4 different areas of participants’ satisfaction—course organization, course content, group dynamic, and methods; it uses a 4-point Likert-type scale (dissatisfied to very satisfied). All participants were asked to complete the questionnaire at the end of the seminar.
The second questionnaire is aimed at assessing participants’ learning. It is based on a validated 32-item questionnaire 14 that explores different aspects of CRM course content, particularly teamwork building, shared decision making in emergency situations, and other methods of improving patient safety. The answers are measured using a 5-point Likert-type scale (strongly disagree to strongly agree). The questionnaire was administered to participants at the beginning and at the end of the course to specifically measure the impact of the program on 1 or more dimensions. This questionnaire also included items on professional activity and individual participant characteristics.
Statistical Analysis
For descriptive analyses of participants’ characteristics and responses to the items on the satisfaction questionnaire we used percentages. Results were presented overall and separately for each profession. To assess knowledge improvement measured by the learning assessment questionnaire administered before and after the course, we calculated for each question mean preintervention and postintervention scores, the mean score difference (learning gain), and 95% confidence intervals (CI) as well as the corresponding effect sizes. This is defined as the mean unadjusted difference divided by the pooled standard deviation of the corresponding mean scores. Effect sizes of 0.2, 0.5, and 0.8 were regarded as small, medium, and large degrees of differences, respectively. 19 A paired t test was used to compare the answers before and after course participation. In addition, mean score differences and their 95% CIs were calculated overall (sum of all mean score differences) and separately for the domains of teamwork, stress recognition, and safety culture, and the results were stratified by profession (anesthesiologists vs surgeons vs nurses vs nurse’s aides and technicians). Differences in learning gain between surgeons and the other professions were evaluated with use of the Student t test. We performed all analyses using the SPSS, version 15.0 (IBM, Chicago, IL).
Results
Between November 2009 and December 2010, a total of 99 participants attended the 9 seminars. The mean age was 41 years, and 53% of the participants were male (Figure 1).
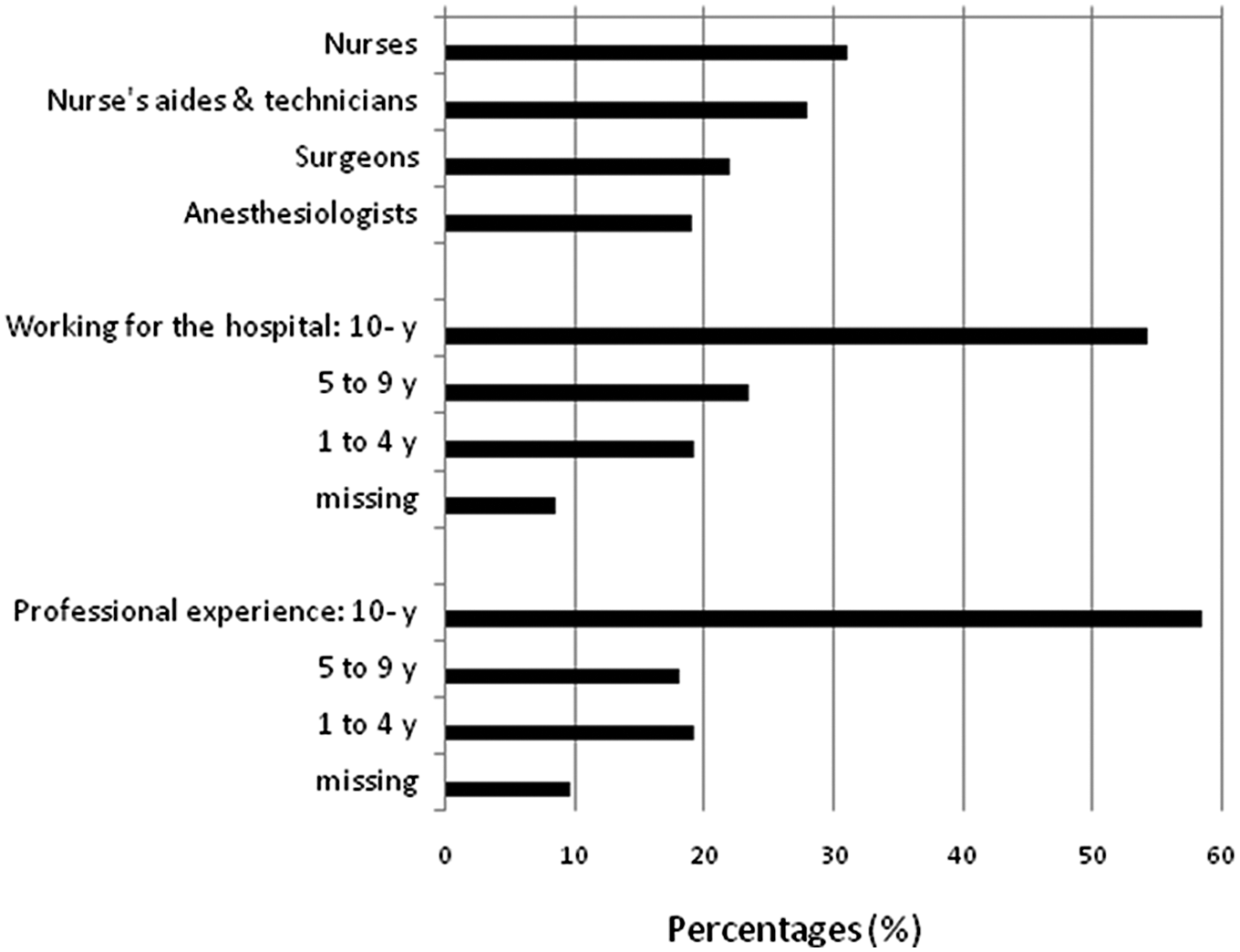
Characteristics of participants
The satisfaction questionnaire was completed by all participants (Figure 2), and the results were as follows: 95% of the participants valued their satisfaction with the overall course organization as high, 94.3% were satisfied to very satisfied with course content, 97.6% with group dynamics, and 95.3% with teaching methods. Nurses were the most satisfied among all professional groups for all measures except group dynamics, which was enjoyed the most by surgeons (Figure 3).
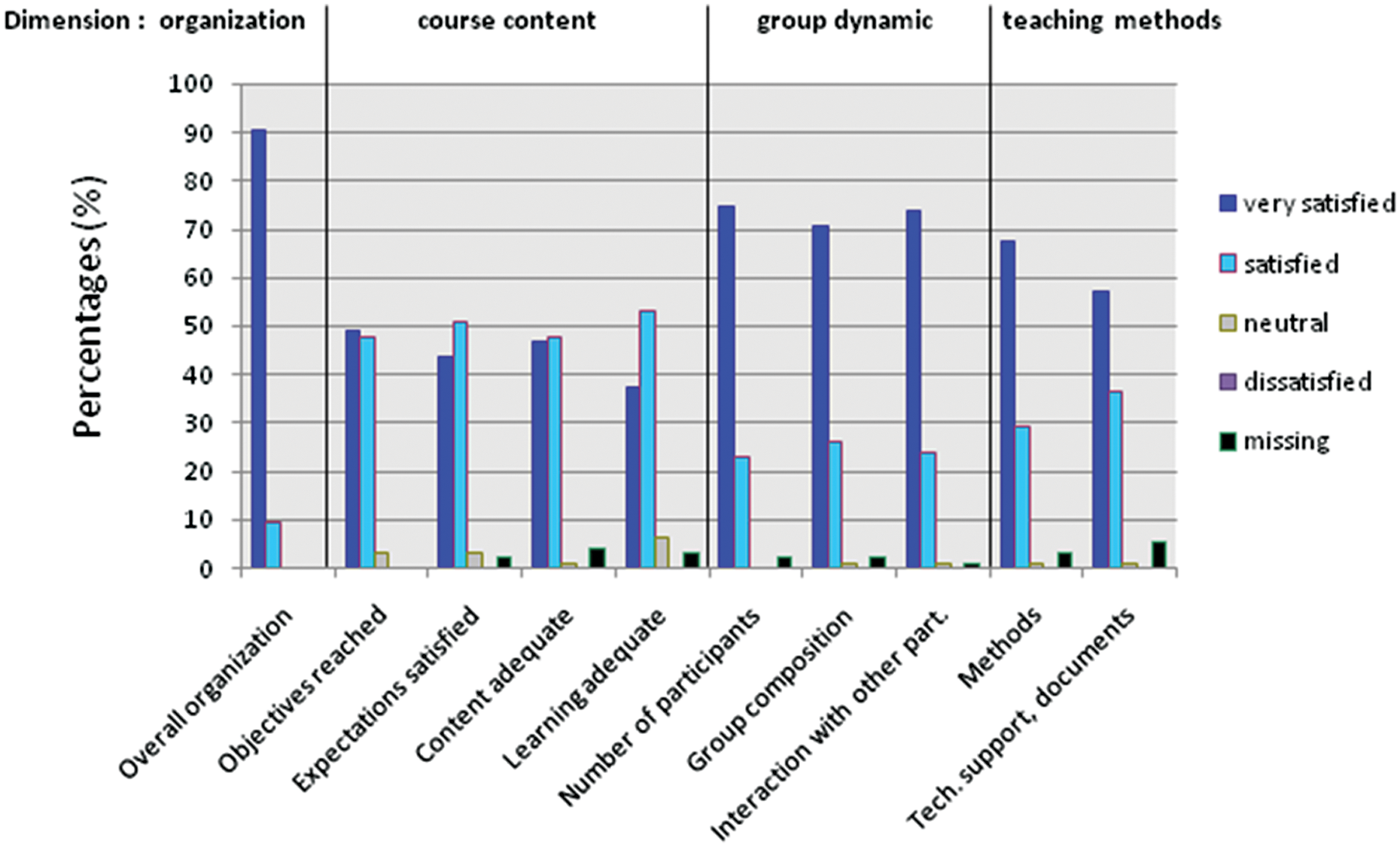
Participants’ satisfaction with the crew resource management program
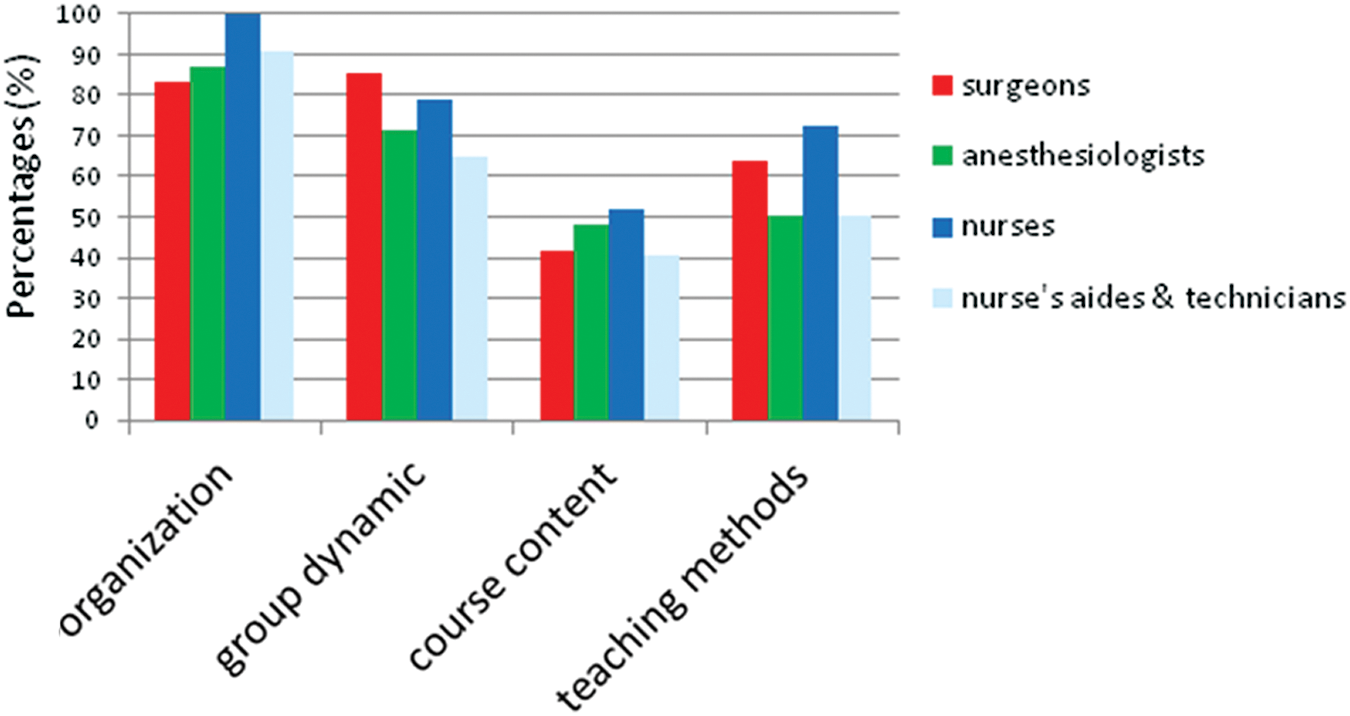
Proportion of very satisfied participants, according to profession
The 32-item before/after course questionnaire analyzing participants’ learning was available for 70 (70.7%) of the participants. The results showed a very good level of learning among participants, with a significant change in 17 questions out of 32 and a change in effect size between 0.2 and 0.5 (Table 1). Knowledge improvement was observed for all professions with the greatest gain in learning in the domain of teamwork (Figure 4). Surgeons, when compared with the other professions, had the most substantial learning gain following program implementation (mean score difference 7.9 vs 3.5, P = .018), and more specifically in the domains of teamwork (mean score difference 5.0 vs 2.6, P = .025) and safety culture (mean score difference 2.1 vs 0.4, P = .026). Less gain was seen for all specialties in areas of stress recognition.
Learning Assessment Before and After the CRM Course
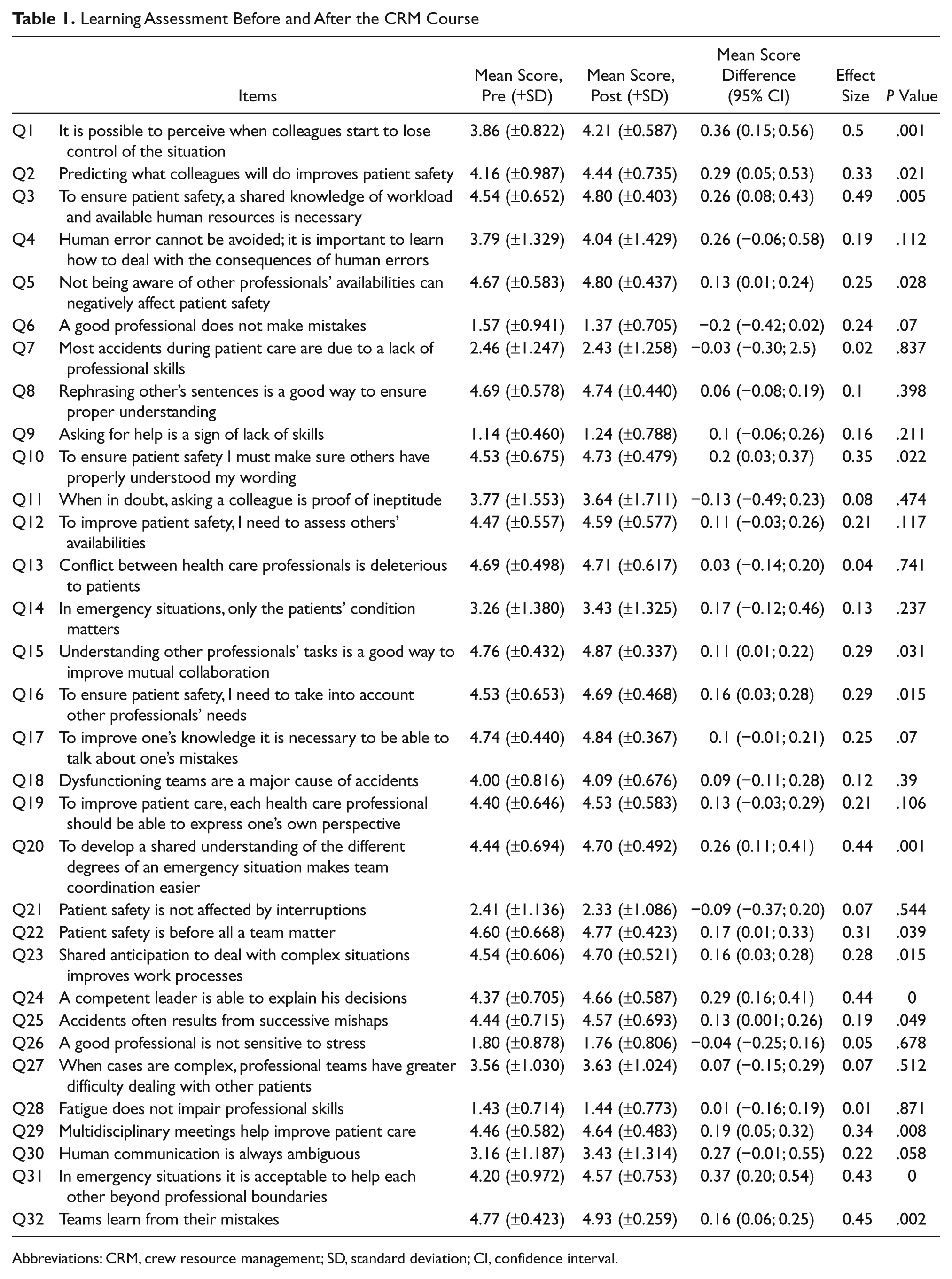
Abbreviations: CRM, crew resource management; SD, standard deviation; CI, confidence interval.
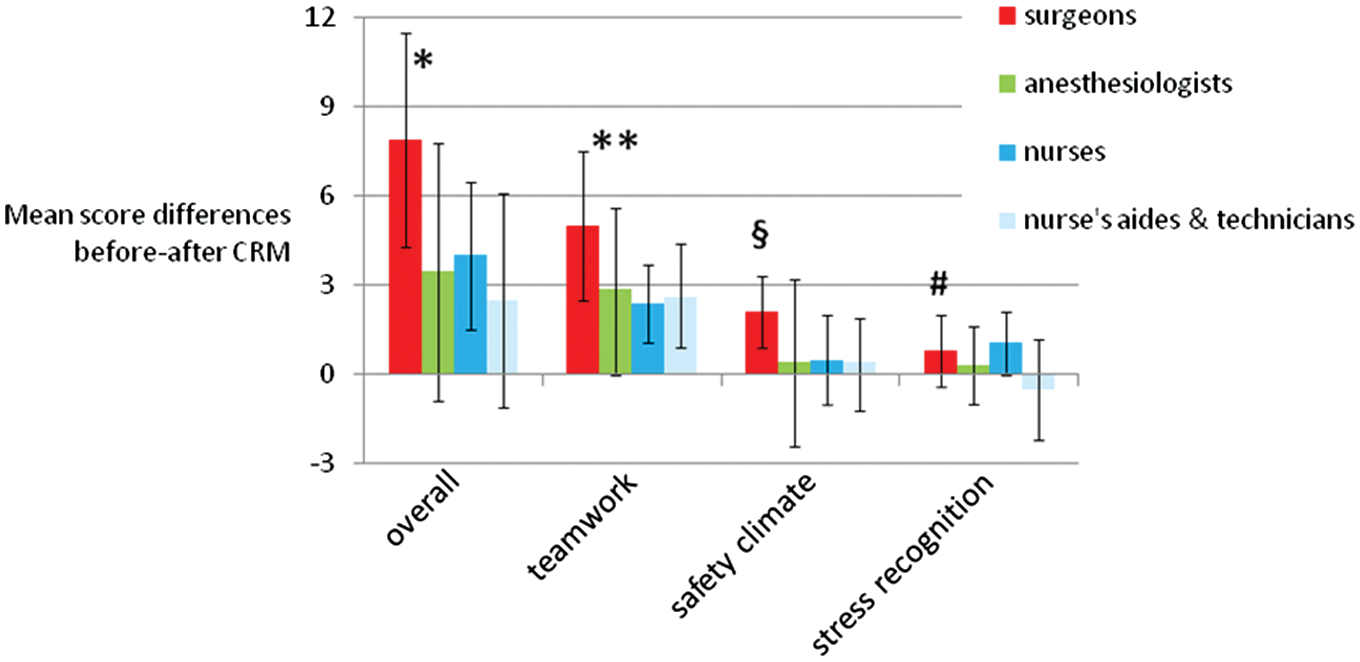
Learning gain after the crew resource management program
Discussion
We introduced a multidisciplinary CRM program to improve teamwork and coordination in the OR of the Geneva University Hospitals. Most of the participants valued this experience highly and rated their level of satisfaction as high or very high for course organization, course content, group dynamics, and knowledge acquisition. Participants also improved their knowledge concerning teamwork and patient safety-related issues, with surgeons demonstrating the greatest learning gain following program participation when compared with other specialties.
These results are similar to previous studies showing that surgical attendings and residents are usually highly satisfied with the level of collaboration developed with other specialties and professions working in the OR, particularly with nurses.20-24 A study by Sexton et al 23 revealed that surgeons had the highest level of positive perception of teamwork, communication, and collaboration in the OR compared with other specialties and professions. Approximately 64% of surgical attendings and 73% of surgical residents rated the rate of communication, collaboration, and cooperation with other surgeons as high, when compared with 39% of anesthesiologists, 28% of surgical nurses, and 25% of anesthesia nurses. This may be explained by discrepancies in the perception of what represents good teamwork and collaboration among nurses, anesthesiologists, and surgeons. Surgeons usually are more supportive of a steep hierarchy between junior and senior staff than those in other specialties. 22 This is not what was taught in our program as it was designed to promote flat hierarchy and horizontal interprofessional collaboration. As a result, surgeons may have modified their understanding of good-quality teamwork and thus improved their knowledge in this area to a greater degree than other specialties. Alternatively, these differences may be explained by a disconnect between surgeons’ beliefs about their personal teamwork and effectiveness skills and the perceptions of these qualities by the rest of the team. Thus, surgeons probably learned more from the program than nurses or anesthesiologists, who already considered the definition of good collaboration to be when everyone’s input is respected. 25
Another interesting finding of our study is that the overall learning gain was higher for surgeons than for anesthesiologists or nurses. This discrepancy raises interesting questions about the reasons for such differences. It may be related to the fact that this kind of training was offered to surgeons for the first time and that their baseline level of knowledge about the course topic was lower. Because anesthesiologists already had such training during their careers, their baseline level of knowledge was higher and the learning gain was less important. This hypothesis is also compatible with the analysis of the satisfaction questionnaire, which showed that twice as many anesthesiologists as surgeons (20% vs 10%, respectively) had no opinion about the learning benefits following the CRM program.
For nurse’s aides and technicians, the results are more difficult to explain. They had the lowest level of satisfaction following the program, and their levels of learning in safety and stress recognition areas were particularly low. This may be related to the fact that most workshops organized during the CRM program were oriented mainly toward patient outcomes and decision-making processes. These are 2 areas in which their interest may have been limited. Furthermore, several documents used in the program were available only in English, a language with which the majority of nurse assistants and technicians are not familiar, and this may have presented a barrier to learning.
Our study has several limitations. First, it was undertaken in a single hospital and analyzed a specific CRM-based training program. Its generalization to other CRM-based programs in other multidisciplinary settings may be limited. Furthermore, even if course participation was compulsory for all OR staff members of the hospital, we cannot exclude a possible selection bias of participants more inclined to participate, enjoy, and learn from such a training program. In addition, the results of this study reflect participants’ perceptions of the course and their newly acquired knowledge on the impact of organization in the OR, but do not evaluate the impact of such learning in the OR itself. Finally, the groups were small; however, small sample sizes are common for team research in operational settings, with the number of teams evaluated typically ranging from 5 to 15. 26 In addition, they represent a substantial proportion of all employees in the Department of Surgery, because nearly 20% of physicians and 50% of nurses have taken the course.
Despite these limitations, the results indicate that professionals highly valued the CRM-based approach and significantly improved their knowledge of teamwork and shared decision making. In the long term, this may improve the overall organizational safety climate and patient safety. CRM-based training programs are highly recommended for routine and emergency practice in multidisciplinary areas where a high level of coordination and collaboration is required. However, when designing these programs it should be understood that their impact may vary depending on the participants’ professions and preliminary knowledge of the different areas discussed in the course. This aspect must be considered when developing such a program for a multidisciplinary audience; these programs should be adapted to the professional background of the participants. Future research should focus on the impact of specifically designed CRM-based training programs aimed at improving interprofessional teamwork and communication in multidisciplinary environments.
Footnotes
Acknowledgements
The authors would like to thank Frédéric Macheret, François Emery, and Manuel Schmidt from Swiss Airlines; Richard Stern, MD, for editorial advice; and Beatrice Moesching for organizing the seminars.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.