
Abstract
The objective of this study was to test the efficacy of a standardized form used during transfers between long-term care facilities (LTCFs) and the acute care setting. The intervention consisted of development and implementation of the transfer form and education about its use. Charts from 26 LTCFs and 1 acute care hospital were reviewed at 1 and 6 months prior to initiation of the transfer form (2007) and at 1 and 6 months after initiation of the transfer form (2008); 210 patient charts were reviewed in 2007 and 172 in 2008. There was 79% concordance between documented LTCF advance directives (ADs) and hospital ADs in 2008—an increase from 66.6% in 2007 (P = .038). Inpatient hospice/palliative care admissions rose from 1.5% in 2007 to 7.7% in 2009 (P = .015). The standardized transfer form improved communication of ADs between LTCFs and the hospital. Secondarily, it may have increased admissions to the acute palliative care unit.
As developments in medical technology improve our ability to prolong life, the issue of physicians and families making proactive decisions regarding the use of CPR and life-sustaining treatment gains increasing importance.1-3 Without these proactive measures, costly medical care will be given to patients who may have preferred to forgo life-sustaining treatment and active medical intervention. 4 In addition, when these decisions are postponed until patients are no longer competent to make them, families may be forced to make decisions about their loved ones’ lives, causing them much distress.5,6
Advance directives (ADs) provide a way for patients to make their wishes regarding future care options known.5-8 Following Congress’s approval of the Patient Self-determination Act (PSDA) in 1990, the use of ADs has become increasingly commonplace. This act required organizations and facilities that receive funds from Medicare and Medicaid to educate patients on their right to choose end-of-life treatment, including do-not-resuscitate (DNR) orders. 9 Because ADs are legally binding documents, 10 their presence in the medical chart ensures that, in case of an emergency or if the patient loses their mental competence, their decisions about treatment are still honored.5,11 After the PSDA was enacted by Congress, the number of patients in long-term care facilities (LTCFs) who were given the option to create an AD increased from 2% to 90%. 9
Although ADs play a prominent role in LTCFs, this information inconsistently reaches the acute care setting during a patient transfer.12,13 Current transfer processes do not ensure that ADs are shared with all providers across all settings. Indeed, studies have shown that only 4% to 8% of emergency department (ED) patients transferred from LTCFs are accompanied by ADs. 14 Because of this, medical resources can be expended at times when these interventions may not be necessary or desired.4,5 Not only does this waste valuable resources, but it also can lead to a contradiction of a patient’s formally expressed wishes and mistrust in the medical system.4,15 Likewise, there is poor communication regarding ADs when patients are transferred from the acute care hospital to a LTCF, and studies have shown that changes in processes of care in other transitional interventions can greatly improve the appropriate use of ADs.
Thus, transitions from the LTCF setting to the hospital seem to be an area where there is need for improvement in communication of ADs. Coleman 16 describes transitions as an area in which “care fragmentation” occurs. Health care is often “divided into discrete loci of care that often function in isolation of one another,” 16 with little communication between providers.
To date, there have been multiple attempts to make AD communication and transitions in health care easier for the patient to navigate and easier for health care personnel to obtain necessary information. Published articles on transitional care, patient activation, and decreasing unwanted and unneeded steps or barriers in these transitions have focused on transfers from the hospital out into the community or care facility and not on the transitions from care facilities into the hospital.17-19 Also of note, the patients in the majority of these studies were community-dwelling elders. Recently, a systematic review was published that identified and evaluated interventions to increase the accuracy of transfer of medications and ADs between nursing homes and hospitals. 20 There were only 5 studies that met the criteria to be in the systematic review, and only 1 of these studies sought to increase communication about both medications and ADs. Overall, this review agreed that these interventions may increase communication, but there were not yet enough studies published to prove their efficacy. Because the majority of these frail elderly patients are unable to communicate for themselves or are not activated to do so, good communication between providers is especially important. 21
To narrow the communication gap between LTCFs and our acute care hospital, a new transfer form was implemented in 2008. This initiative involved 26 of the 36 LTCFs that comprise the Care Coordination Network affiliated with Summa Health System in Akron, Ohio. Numerous quality improvement initiatives have already been completed by members of this network. This transfer form provides background information on each patient’s health history and other pertinent information helpful and necessary for receiving hospitals (see appendix). It also records the presence of ADs. If a DNR order exists, a copy is attached directly to the form.
This study examines the effect that the use of the new transfer form had on improving the transfer of ADs between LTCFs and our acute care hospital. Concordance in the documentation of ADs between LTCFs and the acute care hospital was tested before and after the new forms were implemented.
Methods
The AD Communication Protocol was implemented at 26 local LTCFs and our acute care hospital. The intervention involved implementation of a new transfer form (with ADs as a mandatory element as well as pertinent clinical information) that was
used by LTCF staff when contacting primary care physicians regarding changes in patient condition to inform decisions about the appropriateness of resident transfer;
given to emergency medical services (EMS) and then ED/hospital staff on patient transfer; having obtained this information prior to calling, the primary care physicians should have allowed for ready access to the AD forms by EMS.
The directors of nursing and/or the facility administrators agreed to participate in using the protocol. Education of staff and implementation was left to the discretion of each facility administrator/director of nursing.
The primary outcome of interest was whether patients were accompanied by ADs when they were transferred from the LTCF to the hospital and when they were returned to the LTCF from the hospital. This information was collected for every patient transferred from each of the 26 LTCFs to the ED at 6 months prior to implementing the new form. The same data were collected at 6 months after implementing the new form. Secondary outcomes examined included readmission rates within 30 days, concordance of code status between transferring sites, medical interventions during stay, and length of stay. Data were collected by 2 reviewers who reviewed hospital electronic and paper charts as well as nursing facility paper charts. Data were collected about the transfer form use not only from the nursing home to the EMS transport but also if the form was sent with the patient, if that form was present in the ED, if the official DNR form accompanied it, and if the DNR status remained the same or changed from the LTCF to the EMS, from the EMS to the ED, or from the ED to the hospital. If there was a change, data were collected about whether the DNR was accompanied by documented discussion either in the chart or PLATO (the local electronic physician order entry system).
It was our hypothesis that implementation of this new transfer form that mandates knowledge of AD status, along with EMS, LTCF, and acute care staff education regarding AD use, would result in improved communication of AD status between providers.
All analyses were completed using SPSS for Windows, version 6.1.4 (IBM, Chicago, IL). Means were compared using the Student t test, and proportions were compared using the χ2. This study was approved by the Summa Health System institutional review board.
Results
In 2007 (prior to the implementation of the transfer form), 210 patients were included in data collection. Only 130 of these patients were admitted to an inpatient unit from the ED; therefore, they were the only patients included in the final analysis. In 2008 (after implementation of the transfer form), data were collected on 172 patients; 117 were admitted and therefore included in the analysis. Use of the transfer form also was tracked, with completion rate/arrival to ED being less than 50% (49.9%, n = 72). In Table 1, we describe the characteristics of the patients in each sample. The patients in the postimplementation group generally were older and female. The EMS level of acuity was higher in the postimplementation group. There was no significant difference between 2007 and 2008 with regard to gastrointestinal, musculoskeletal, genitourinary, or neurological comorbidities (data not shown).
Demographics
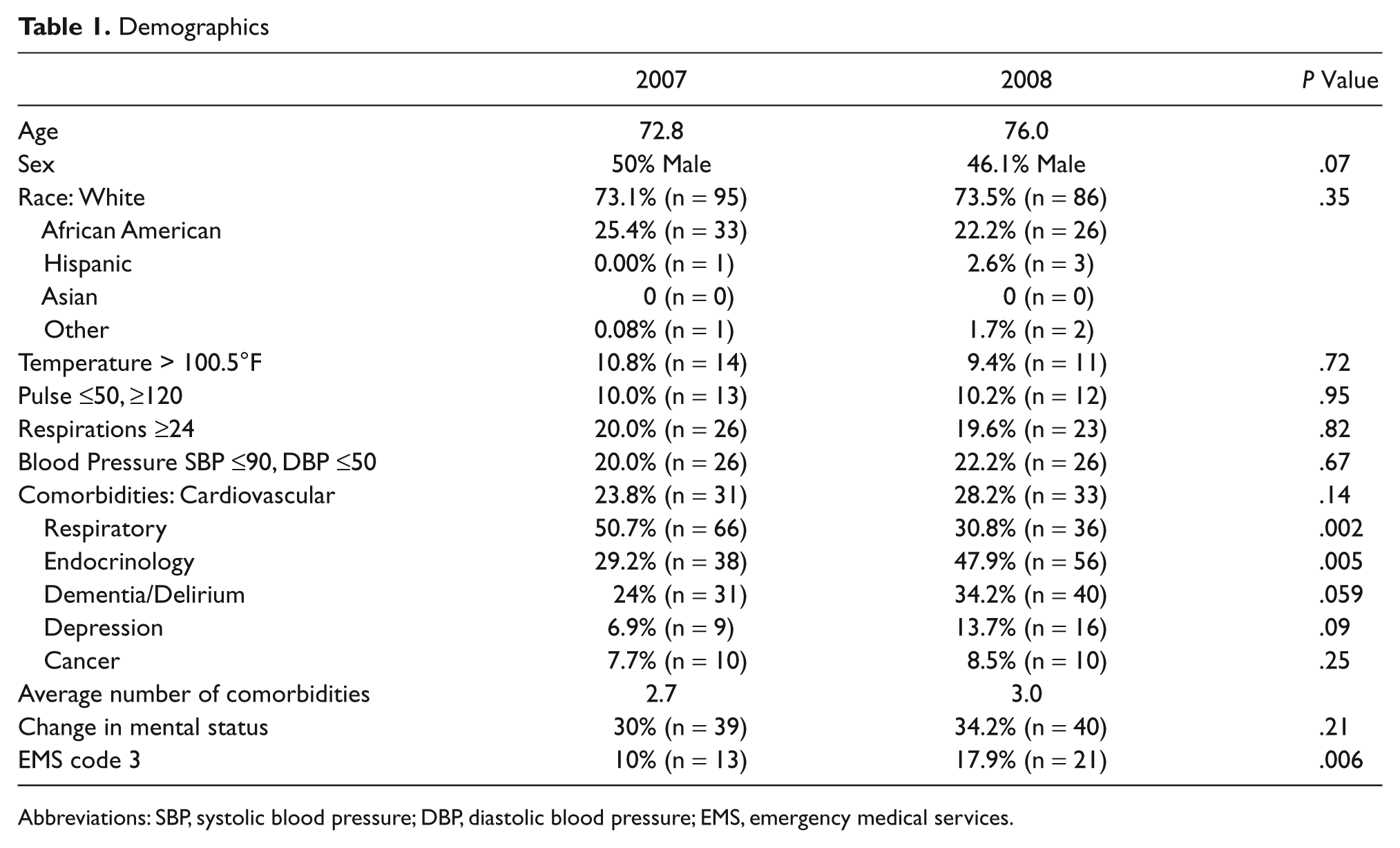
Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; EMS, emergency medical services.
Prior to implementation of the transfer form (2007 data), discordance between the LTCF and the acute care hospital regarding admission AD status was just 26.7%. With initiation of the use of the transfer form in 2008, there was a statistically significant decrease to 16.3% discordance between the documented LTCF ADs and hospital ADs (P = .038). The number of patients who had DNR status changes without any documentation of that change (assuming that these changes were performed unknowingly) or whose DNR status changes were documented incorrectly also was examined. Discordance/paucity of documentation decreased post intervention. Inpatient/palliative care admissions rose significantly postintervention (Table 2). There was no change in CPR, intubation, or feeding tube placement before and after implementation of the new forms.
Changes in Outcomes Before and After Transfer Form Implementation
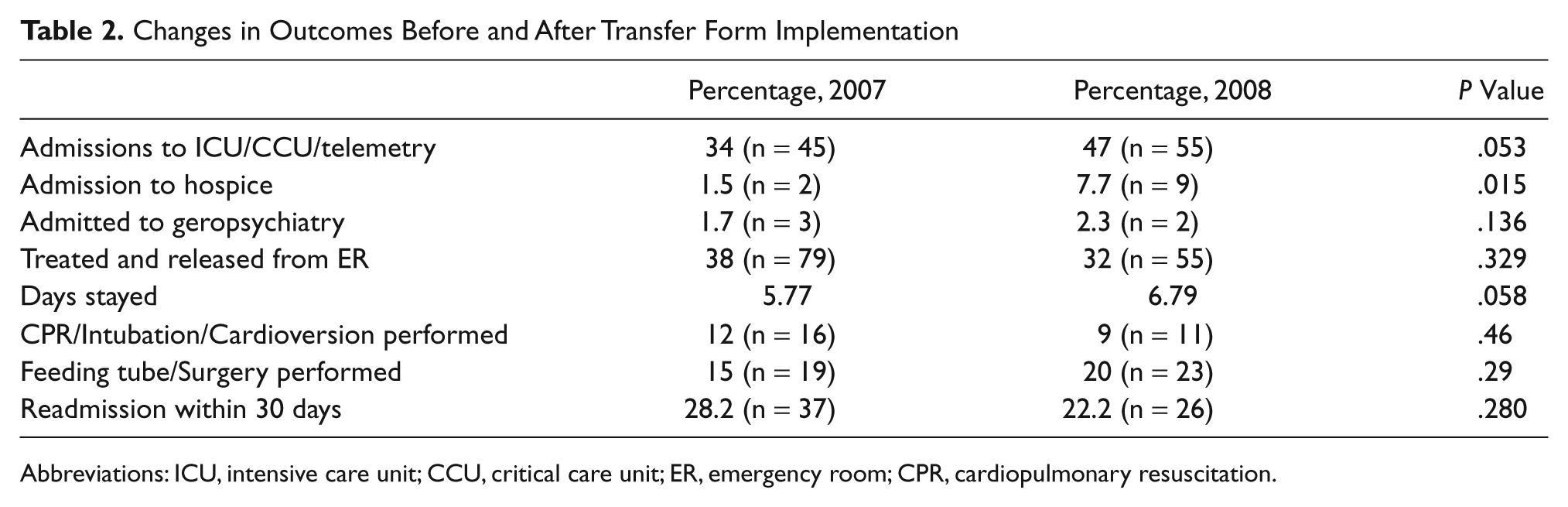
Abbreviations: ICU, intensive care unit; CCU, critical care unit; ER, emergency room; CPR, cardiopulmonary resuscitation.
Length of stay also was of interest (Table 2). When comparing 2007 versus 2008, the trend appears to be toward a lengthier stay. However, this was thought to be explained by the fact that there were higher numbers of hospice admits; therefore, the data were run excluding hospice patients who were admitted. Length of stay excluding hospice patients was not significantly different between the 2 time periods (in 2007, it was 5.8, and in 2008, 6.3; P = .48).
Although the result of increasing the concordance of DNR status from LTCF to hospital was significant after implementing the form, what also was of interest was where the intervention was effective. There are many steps involved in the transfer of information for a patient from the nursing home to the acute care setting. Figure 1 is a graphical representation of this process; it examines DNR status through the sites of care, comparing preintervention (2007) with postintervention (2008). The graph focuses on the discordance between the sites of care, looking at the transfer from LTCF to the ED, ED to the hospital floor, and from the floor back to the LTCF. This graph also takes into account if the DNR status was changed, and if this occurred, whether it was accompanied by documentation. Patients who did not return to the same facility or who died during the study were not included in this figure. Discordance or undocumented changes were in the figure. Comparing 2007 and 2008, there is a slight increase in discordance between the LTCF and the ED, but the larger change occurs between the ED and the hospital floor.
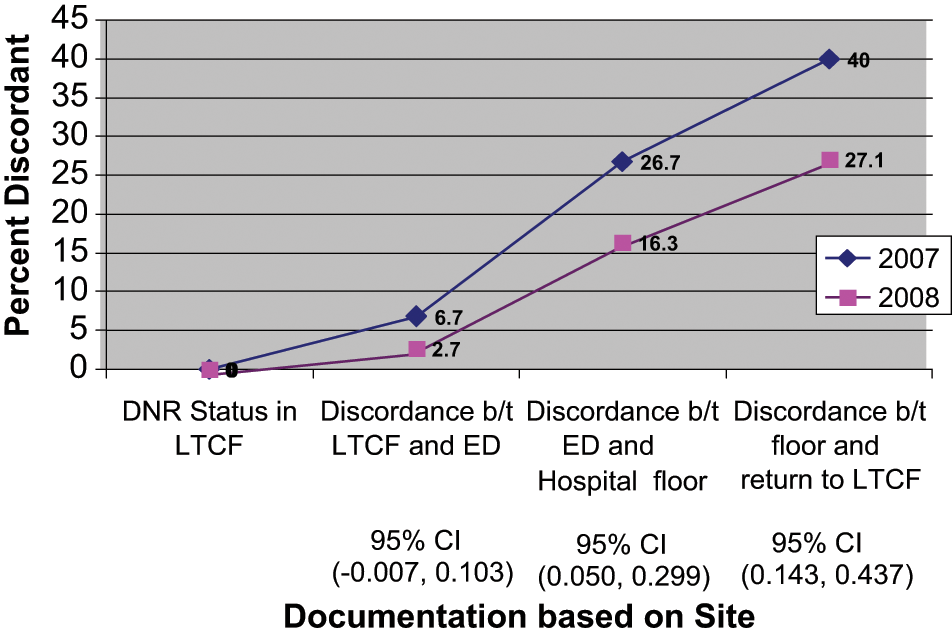
DNR through sites of care
Discussion
As the population of elderly people continues to increase, the number of elderly people who call a LTCF home also will rise. Transitions of care, especially from LTCFs to the hospital, require improved transfer of information among caregivers, including better AD documentation as well as documentation of medical history and medications. Other studies have shown that intervening in this process in health care does make a difference, which is reflected in the findings of the current study. 20 Admissions for palliative care as opposed to general care also rose after the new form was implemented, which would be consistent with an increased documentation of a patient’s wishes. The pretransfer nursing assessments that were part of the new protocol also may have reduced the actual number of patients who were sent to the hospital.
Even though transfer forms were used only 50% of the time post intervention, results of implementation were significant. The use of an AD communication protocol improved the concordance of the AD communication between the LTCF and the hospital. These data also suggest that secondary outcomes, such as increasing admissions to the palliative care unit, were improved with the use of the new form.
Implementing such a protocol is not without difficulties. Both nursing facilities and hospitals are financially incentivized to have patients treated in the hospital. However, this may not always honor patients’ wishes if ADs are not carefully reviewed prior to transfer. Different cultures at different institutions also are a barrier. Nursing home staff tend to favor more aggressive medical treatment than can be provided in their facility, and hospital staff sometimes feel that these transfers are inappropriate. The use of this protocol helps bridge that culture gap. Traditionally, there has been a communication problem because of the lack of a standardized process, and this has resulted in disruptions in continuity of care. This protocol also assists with ensuring that complete information is shared between institutions. Finally, this protocol helps overcome the problems associated with the lack of a common electronic medical record with which clinicians can communicate.
Many of these issues have taken on a new urgency with the passage of the Affordable Care Act in 2010. Having payment structures such as bundled payments will provide a financial incentive to nursing facilities and hospitals to improve communication. Interventions such as this new protocol likely would be a cost-effective initiative given that we saw improved outcomes with no added cost to the respective institutions.
Limitations
There are several limitations to this study, the largest of which is the low rate of use of the transfer form by the intervention group. The actual use was 49.9%; therefore, results potentially would have been more significant if there had been more focus on use. The difference in average age in 2007 (72.8) versus 2008 (76.0) approached significance, which could help explain why some of the results are not significantly different between groups. The difference between groups regarding EMS Triage Level 3 (10% in 2007 vs 17.9% in 2008), which was statistically significant (P = .006), also could explain small differences found throughout the study related to the postintervention patients being sicker. Furthermore, there were outcomes on multiple factors that had only small rates of occurrence (ie, CPR, n = 2).
Conclusions
This intervention should allow patients’ wishes to be known and followed in the hospital setting, even if the patients are unable to speak for themselves. Future studies will need to examine how to further improve these communication efforts. Multiple outcomes approached significance; therefore, a larger study with more power probably would show significance.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Zafirau and Snyder and Ms Hazelett are employees of Summa Health System. The authors disclosed no other potential conflicts of interest regarding this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by an American Medical Directors Association/Pfizer Quality Improvement Award. The funder had no role in the study. Salaries for Ms Bansal and Ms McMahon were partially supported by the award. The study also was funded in part by the Summa Foundation.