
Abstract
As payment policies for surgical complications evolve, surgeons and hospitals need to understand the financial implications of postoperative events. Using data from the National Surgical Quality Improvement Program (NSQIP), the authors estimated mortality, length of stay (LOS), and total cost attributable to multiple postoperative events in general and vascular surgery patients. Data were collected using standard NSQIP practices at a single academic center between 2007 and 2009. LOS and costs were fit to linear regression models to determine the effect of 19 postoperative events in the setting of 1, 2, or 3+ events. Of 2250 patients sampled, 457 patients developed at least 1 postoperative event. LOS increased by 2.59, 5.18, and 10.99 days (P < .0001) for 1, 2, and 3+ postoperative events; excess costs were $6358, $12 802, and $42 790 (P < .0001), respectively. Multiple postoperative events have a synergistic effect on mortality, LOS, and the financial cost of patient care.
The payment landscape is changing dramatically for hospitals and for their surgical outcomes. The Centers for Medicare and Medicaid Services has determined that it will no longer cover the extra costs associated with treating preventable errors, injuries, or infections that occur in the hospital setting. 1 This change provides a strong incentive for hospitals to identify and prioritize postoperative complications and implement quality improvement programs to reduce them.
Rates of many postoperative complications have been well documented in the surgical literature. For example, depending on the surgical procedure and method of identifying the complications, surgical site infections (SSIs) have been estimated to occur in between 1.8% and 8% of cases, myocardial infarction in between 0.5% and 1%, pneumonia in between 0.7% and 2.4%, and cerebrovascular accidents (CVAs) in <1%. 2 Much less is known about the contribution of these complications to mortality, length of stay (LOS), and costs 3 in specific populations, particularly when they occur in combination. Studies have reported that postoperative complications result in significant resource consumption but only reported on complications with single procedures, selected populations, or small groups of patients.4-6 In previous work, the authors used data from the National Surgical Quality Improvement Program (NSQIP) to estimate the excess costs and LOS associated with SSIs in our institutional general and vascular surgery population and found them to be approximately $10 800 and 4.3 days, respectively. However, SSI is only 1 of 19 surgical complications tracked by NSQIP, and many patients had more than 1 complication.
The objective of this study was to examine mortality, LOS, and the excess cost associated with all 19 measured complications in general and vascular surgery patients using NSQIP data. An important challenge to conducting this analysis was that many of the complications co-occur, making it difficult to isolate the specific impact of a single complication. This was dealt with by estimating the effects of single complications separately from aggregate effects when complications occurred in clusters of 2 and 3 or more.
Methods
Data
Data came from the Penn State Milton S Hershey Medical Center NSQIP and consisted of patient data randomly collected on 2250 adult general and vascular surgical inpatients at a single academic center between 2007 and 2009 using standard NSQIP methodology.7-11 Selected cases were the first 40 eligible vascular and general surgery operations during an 8-day cycle, where each cycle started on a different day of the week, thus capturing approximately 20% of the hospital’s surgical volume. A trained clinical nurse reviewer collected data on 60 preoperative patient characteristics, 18 intraoperative factors, and 22 postoperative occurrences up to 30 days following the procedure. Chart review, information from morbidity and mortality conferences, and communication with patients by telephone or letter completed the 30th postoperative day data collection.7-11
Postoperative occurrences under the NSQIP program are divided into 5 categories: wound occurrences (superficial, deep, organ-space SSIs, and fascial dehiscence); respiratory occurrences (pneumonia, unplanned intubation, pulmonary embolism, and intubated >48 hours duration); urinary occurrences (progressive renal insufficiency, acute renal failure requiring dialysis, and urinary tract infection); central nervous system occurrences (cerebral vascular accident, coma >24 hours, and peripheral nerve injury); and cardiac occurrences (cardiac arrest requiring cardiopulmonary resuscitation [CPR] and myocardial infarction). Other occurrences included postoperative blood transfusions, deep venous thrombosis, sepsis/septic shock, and graft/flap failure. To assign a postoperative occurrence, the clinical nurse reviewer identifies medical documentation that specifically meets the American College of Surgeons NSQIP definitions criteria for the selected postoperative occurrence. The definitions criteria are adapted from those used by national regulatory agencies.
The total cost of admission data were obtained from the hospital’s accounting database (Horizon Performance Manager; McKesson, San Francisco, CA). These represented fully loaded operating costs for the surgical admission estimated using a ratio of costs-to-charges (CCR) methodology. The CCR approach is a standard cost accounting technique, whereby costs are estimated as a percentage of hospital charges. Although the CCR approach has limitations for estimating hospital costs, it is by far the most prevalent technique, and previous research has shown department-level CCRs to be a reasonable approach to estimating costs within a hospital and costs across hospitals for patients within a common diagnosis-related group. 12
Statistical Analysis
The statistical analysis was designed to estimate the excess cost, LOS, and mortality associated with postoperative events controlling for other patient- and surgery-specific confounders. Age, sex, ethnicity, and preoperative patient comorbidities were controlled for because these variables are not only associated with increased risk of developing postoperative complications but contribute to an increase in total hospital costs independent of infection risk. 13
Patient characteristics were compared using the Student t test for continuous variables and the χ2 test for binary and categorical variables. Logistic regression was used to determine which postoperative events had a significant effect on mortality. Total cost and LOS were fit to generalized linear regression models assuming a gamma family of distributions and a log link function. These models were chosen because the cost and LOS data were highly skewed and did not meet the normality assumption of the classical linear regression model. The generalized linear regression models allowed the estimation of the effect of each postoperative event as well as the effect of having more than 1 postoperative event. All statistical analyses were performed using STATA, version 11 (StataCorp LLP, College Station, TX). Statistical significance was defined as a P value <.05.
Results
Demographics
During the period 2007 to 2009, there were 2250 general and vascular surgery inpatients captured in the NSQIP database at our institution. The majority of patients underwent surgery of the colon and rectum (26.2%), the foregut (15.9%), bariatric surgery (11.5%), and vascular procedures (9.0%). Patient characteristics stratified by the occurrence of at least 1 postoperative complication are reported in Table 1. Patients were similar in patient and preoperative characteristics, such as ethnicity, body mass index, smoking status, and alcohol use. The groups also were alike with regard to intraoperative characteristics, including clean and contaminated wound classes and operative time of 4 to 8 hours. There were, however, some significant differences between the 2 groups, suggesting risk factors for developing postoperative complications. For example, the postoperative event group was more likely to be male, to have insulin-dependent diabetes, and to have an operative time longer than 8 hours.
Characteristics of Inpatients Without and With More Than 1 Postoperative Complication
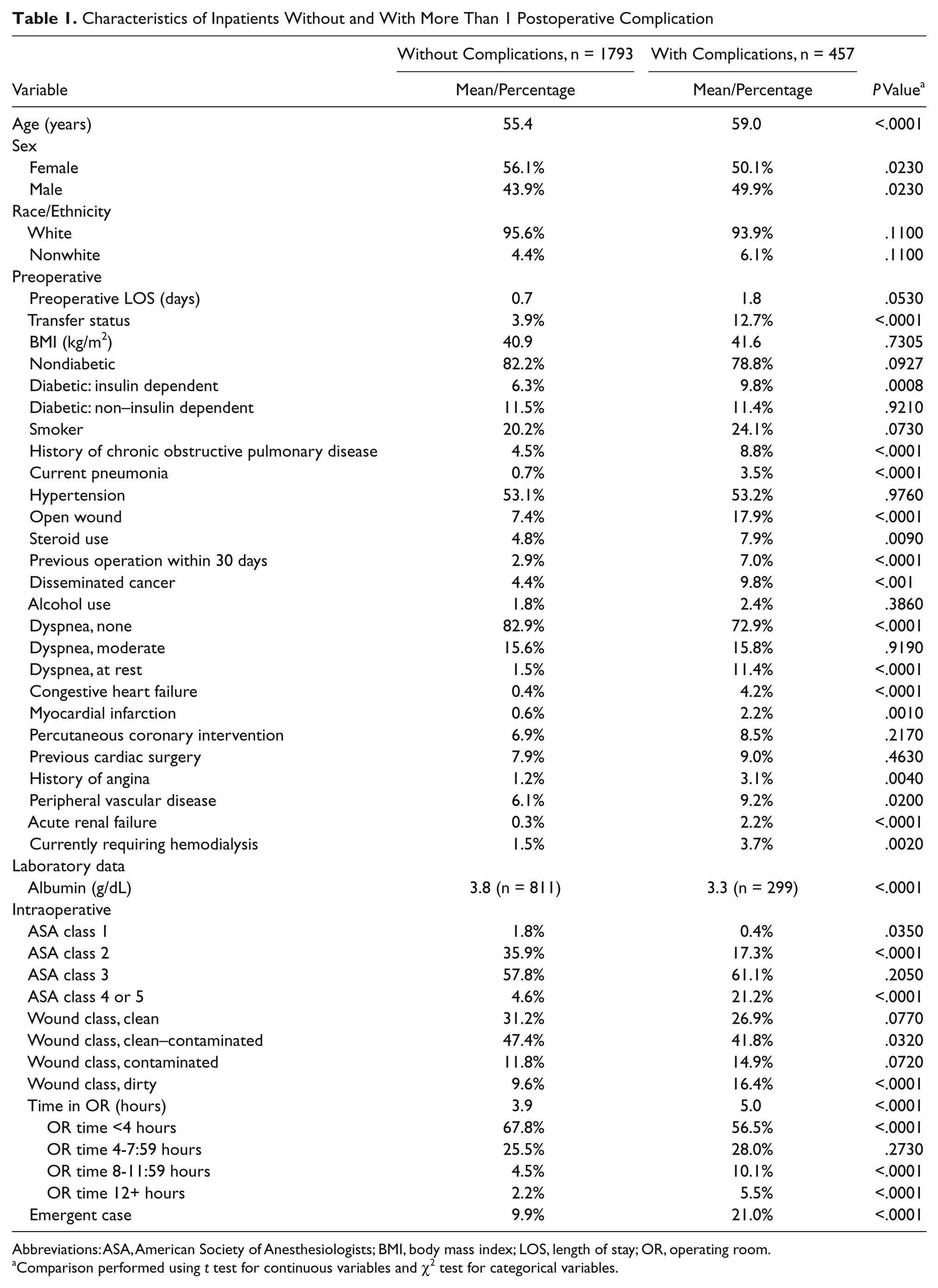
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; LOS, length of stay; OR, operating room.
Comparison performed using t test for continuous variables and χ2 test for categorical variables.
Mortality
In all, 226 patients developed 1 postoperative event; 5 of those events resulted in death (Table 2). Mortality rates for venous thromboembolism, intubated >48 hours, and transfusion requirement were not statistically significant. However, mortality rates for cardiac arrest requiring CPR and CVA were statistically significant. Also reaching statistical significance were the number of patients with 2 and 3 or more postoperative events who died.
Mortality Rate for Postoperative Events
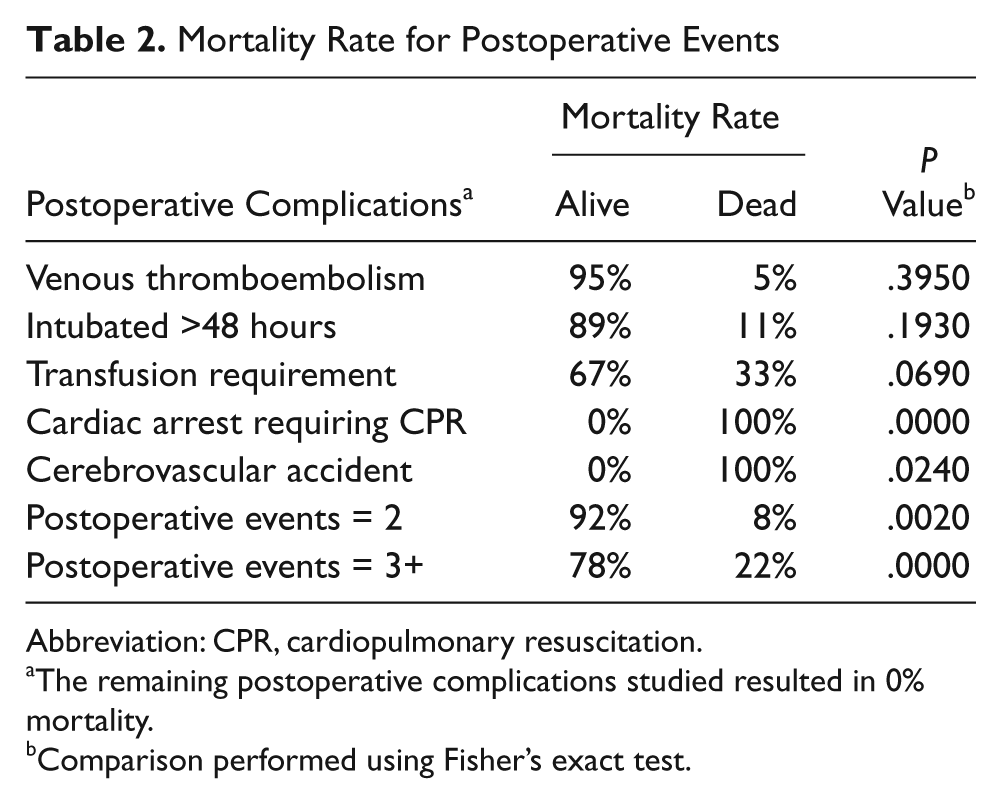
Abbreviation: CPR, cardiopulmonary resuscitation.
The remaining postoperative complications studied resulted in 0% mortality.
Comparison performed using Fisher’s exact test.
Length of Stay
The predicted mean LOS without a postoperative event was 5.5 days. Patients with 1 postoperative event had a LOS that was 2.6 days longer (P < .0001) than patients with no events. The longest statistically significant LOS was attributed to ventilator dependence (Table 3), followed by pneumonia and sepsis.
Multivariate Linear Regression Analysis of Length of Stay Associated With Postoperative Events
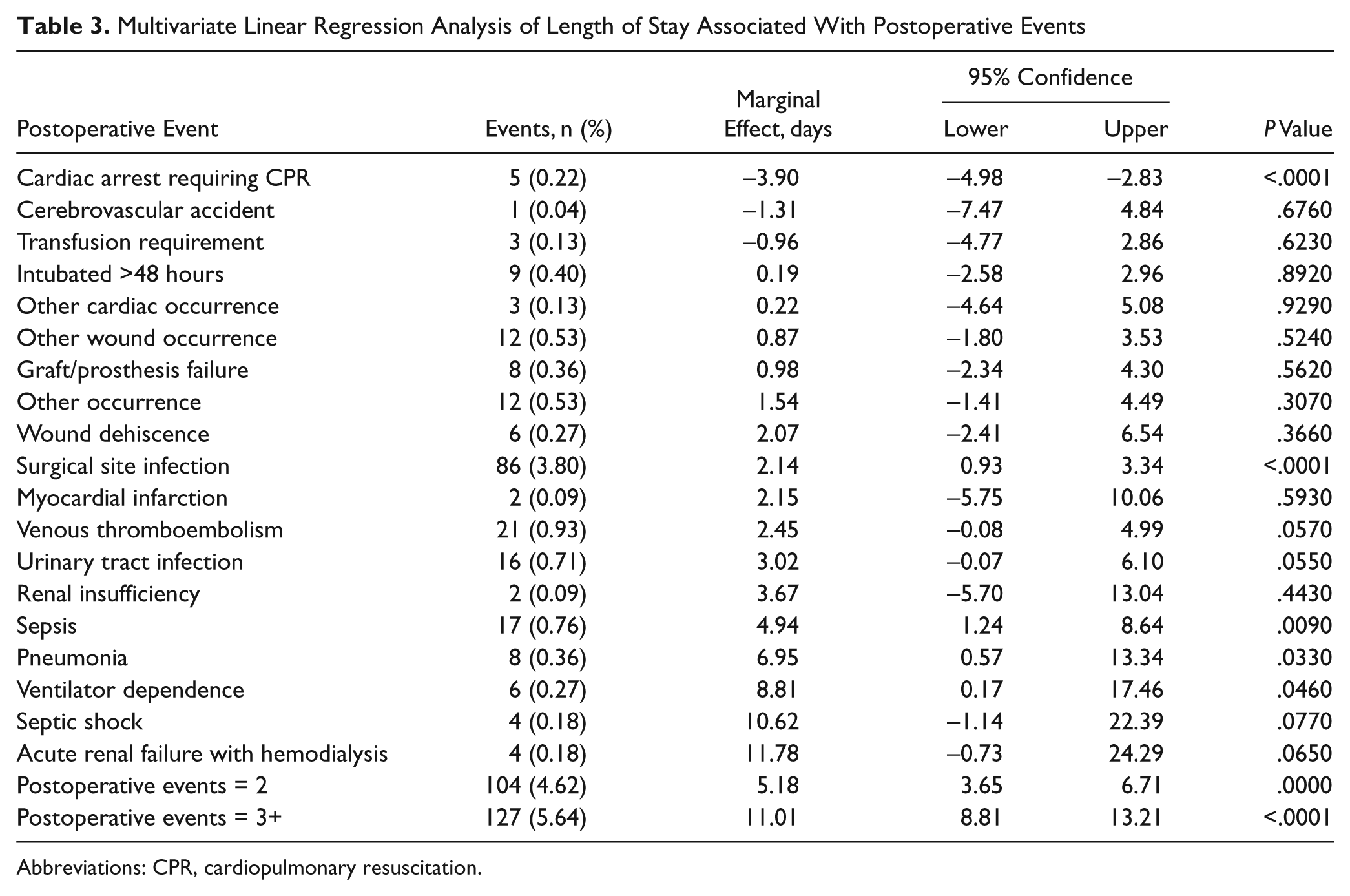
Abbreviations: CPR, cardiopulmonary resuscitation.
As suggested in Table 3, many patients had more than 1 postoperative event, which also was significantly associated with excess hospital LOS. Figure 1 (left panel) illustrates the cumulative effect on LOS of incurring 1, 2, or 3 or more postoperative events.
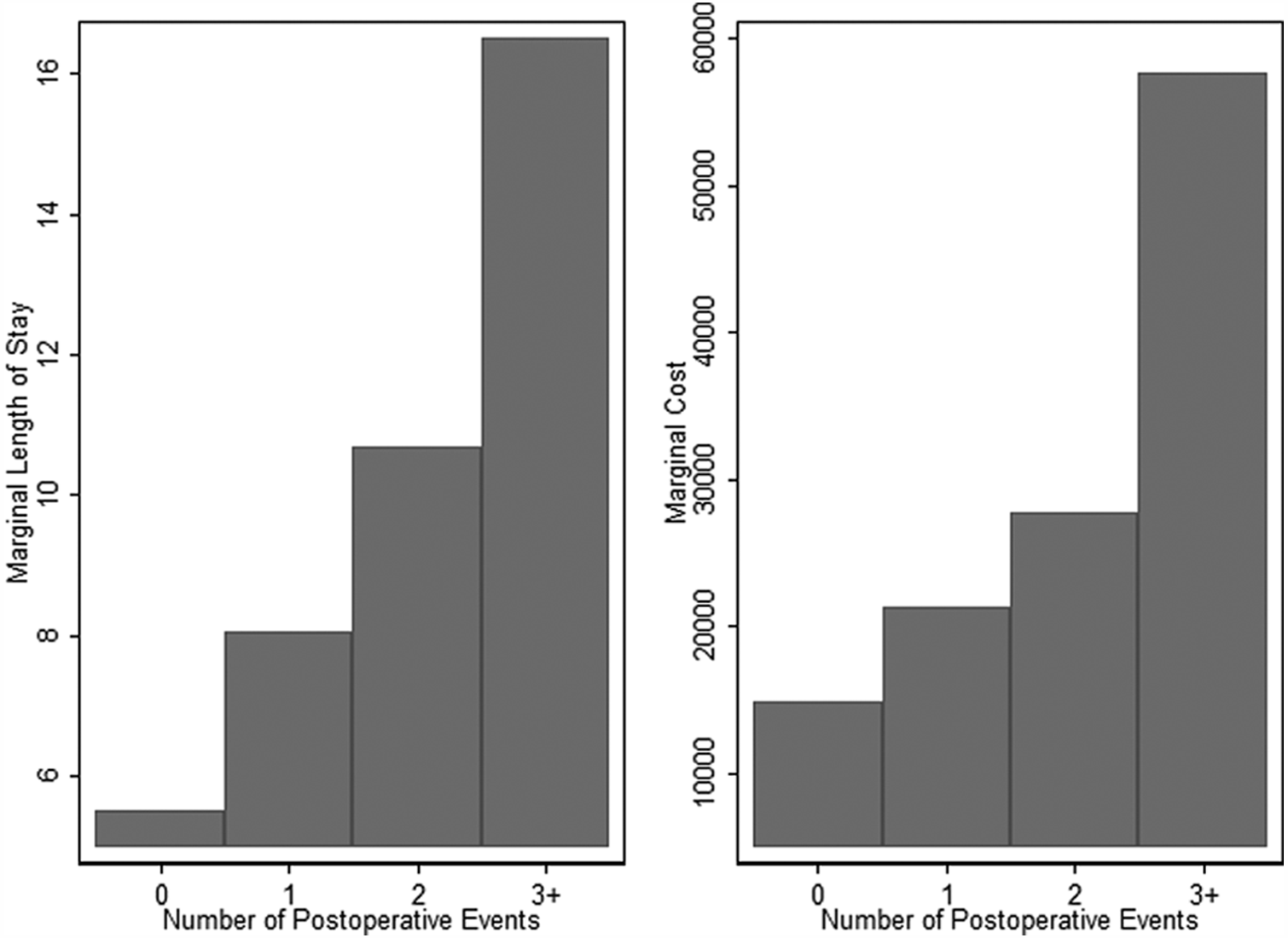
Cumulative length of stay and cumulative cost of postoperative events
Hospital Costs
The predicted mean total cost of a hospital stay across all procedures without a postoperative complication was $14 839. A single postoperative event added an average of $6358 in additional costs. Results of the regression analysis presented in Table 4 suggest that 5 of the 19 postoperative events studied had a significant effect on total hospital costs. Ventilator dependence was associated with the largest statistically significant attributable cost, followed by pneumonia and sepsis.
Multivariate Linear Regression Analysis of Costs Associated With Postoperative Events
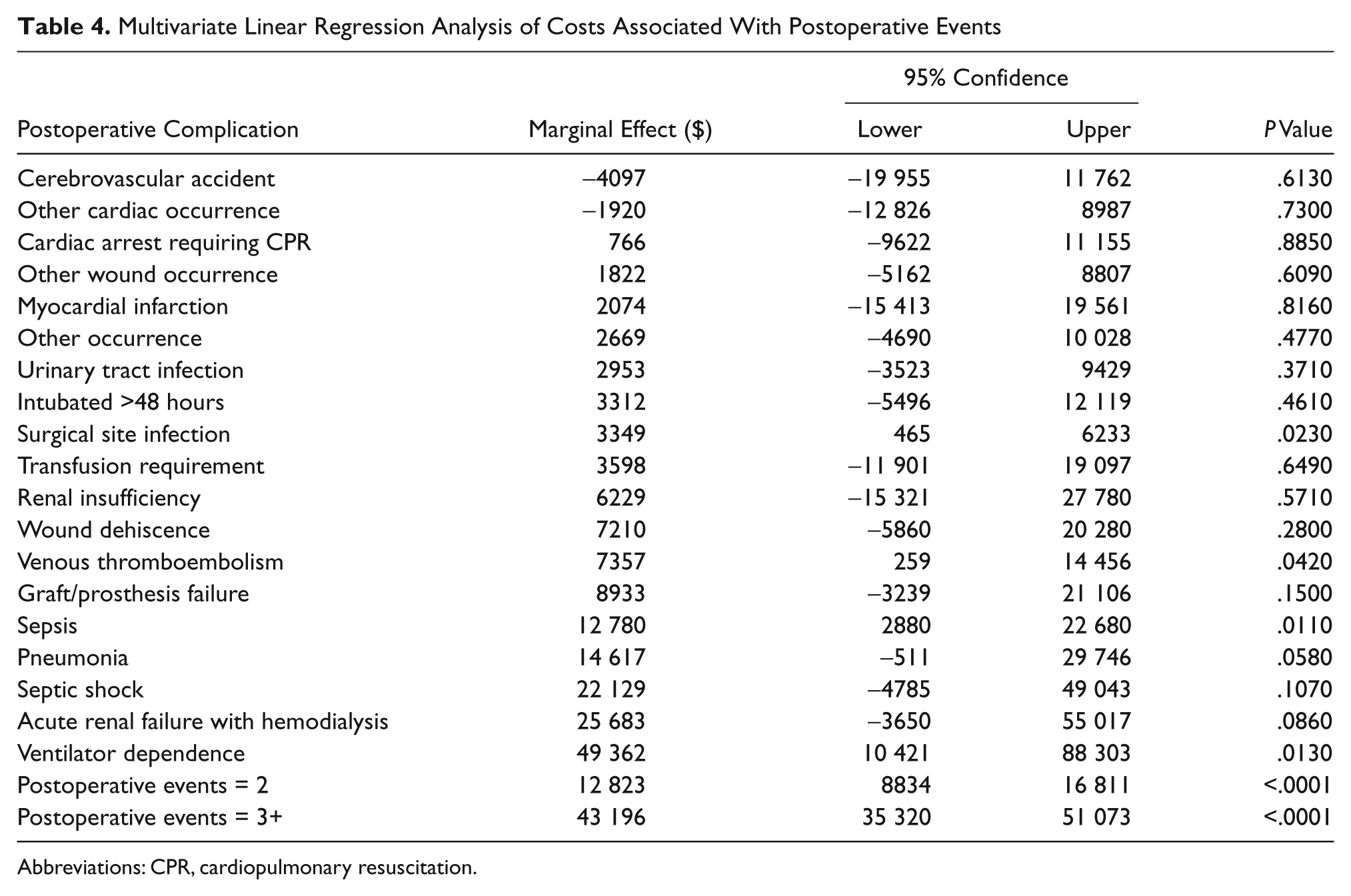
Abbreviations: CPR, cardiopulmonary resuscitation.
The cumulative effect of LOS with 1, 2, and 3 or more postoperative events is shown in Figure 1 (right panel).
Discussion
Despite continued improvement in patient selection, operative techniques, and perioperative management, general and vascular surgery procedures still result in significant perioperative morbidity and mortality. 5 For this patient population, postoperative complications are associated with an increased risk of death, prolonged hospital LOS, and increased hospital costs. It is important to understand the costs and LOS associated with individual postoperative complications in order to develop quality improvement efforts tailored to prevention strategies, thus improving patient outcomes and more efficiently allocating health care resources. 5
In this study of 2250 surgical inpatients at a large academic medical center, 457 patients developed at least 1 postoperative complication. Two of the 19 complications resulted in a statistically significant mortality rate and included cardiac arrest requiring CPR and CVAs. The mortality rate also was statistically significant if more than 1 postoperative event occurred. Significant complications associated with both cost and LOS in order from greatest to least resource use were ventilator dependence, pneumonia, sepsis, venous thromboembolism, and SSIs. The development of ventilator dependence longer than 48 hours following a general or vascular surgical procedure incurred additional costs in excess of $49 362 and increased LOS by 8.8 days for the hospital admission in which the surgical procedure was performed. Additionally, developing pneumonia incurred additional costs of $14 617. Patients with sepsis, venous thromboembolism, and SSIs incurred additional costs of $12 780, $7357, and $3349, respectively. In a previous study, we reported excess costs attributable to SSIs as approximately $10 800. Although we had controlled for preoperative characteristics, unlike this study, we did not account for the possibility that the patient may have had multiple postoperative complications in addition to an SSI, thus increasing the cost. More important, this study highlights the financial implications of treating postoperative complications in surgical patients and the effects of multiple complications or events on outcomes and costs. It is not surprising that the same postoperative events associated with significant increases in additional costs also are associated with significant increases in LOS because the most important determinant of health care spending is the intensity of services provided over the course of a hospital stay. 14 It also should be noted that postoperative ileus contributes significantly to postoperative LOS. During the period 2007 to 2009, the NSQIP database did not include postoperative ileus as a postoperative complication; therefore, this variable was not included in the analysis. However, as of January 2011, the NSQIP program instituted a procedure targeted approach, which allows larger facilities or specialty hospitals to focus on high-volume, high-risk procedures, thereby enabling them to target quality improvement efforts in areas that will yield the greatest return on investment. This may include procedure-specific variables and complications such as postoperative ileus. 15
Even though the economic impact of postoperative complications is acknowledged to be significant, few studies specific to general and vascular surgical procedures exist to quantify the costs to treat these complications. Dimick et al 7 used their NSQIP database to examine costs associated with postoperative events at a single academic medical center. They found that when complications were grouped by infectious, cardiovascular, respiratory, or thromboembolic cause the unadjusted hospital costs increased by $8209, $13 256, $54 430, and $28 355, respectively. However, their study did not isolate individual complications within those groupings for cost comparisons. Another NSQIP study by Davenport et al 13 examined costs attributable to preoperative risk factors, surgical complexity, and individual postoperative complications. Their study concluded that sepsis, acute renal failure, ventilator dependence, septic shock, and pneumonia were associated with the highest increase in costs. However, their costs were reported as an increase in mean costs associated with complications. When examining metrics of financial performance, marginal costs as opposed to average costs are the key to cost-effectiveness assessments because those are the costs to consider when making budget allocation decisions. 16
A study by Kalish et al 6 abstracted data from 372 680 major surgery patients in 404 California acute care hospitals and identified 26 complications. They found, on average, that patients with postoperative complications had higher total charges of $30 896 versus $9239 for no complications and longer stays of 13.5 versus 5.4 days. Another study by Khan et al 2 determined total hospital costs and LOS in all noncardiac surgical patients admitted to a single tertiary care center over a 2-year period. A total of 6.9% of their 7457 patients developed at least 1 postoperative complication. Overall complications increased hospital costs by 78% and LOS by 114%. However, the latter 2 studies relied on administrative databases to assess surgical quality and determine postoperative complications, which may underestimate the true incidence of complications. Administrative databases are not designed to model morbidity directly and, unlike NSQIP, which measures postoperative events directly, rely on billing codes to identify postoperative complications. 17 In a study by Davenport et al, 17 a direct comparison of the NSQIP data set and the University HealthSystem Consortium Clinical database found that, where the data sets described similar severe complications, NSQIP identified them more accurately and reliably.
It is important to identify those postoperative complications that are costly and contribute to prolonged LOS in order to develop the best quality improvement efforts to maximize prevention strategies. At our institution, the first risk-adjusted NSQIP semiannual report for the institution was released in 2008 and indicated postoperative SSIs in general and vascular surgery patients as an area for improvement with an observed to expected (O/E) ratio of 1.31. The NSQIP data indicated that 19.3% of SSIs in general and vascular surgery patients occurred in patients with diabetes, whereas it was 8% in patients without diabetes. A multidisciplinary task force was formed to develop a glucose control protocol, which was implemented for all surgical patients later that year. The following risk-adjusted report yielded an O/E ratio of 0.78 for SSIs.
This study has several limitations. First, all the patients studied were from a single academic medical center, and results may not be representative of general and vascular surgery patients who develop postoperative complications in other institutions. It also is not known whether the costs or LOS associated with the postoperative complications at academic facilities translates to smaller, community-based institutions. In addition, this study only examines cost from the hospital’s perspective. The occurrence of a postoperative complication not only increases hospital costs but has an effect on patient, society, and opportunity costs as well. Therefore, our study almost certainly underestimates the real cost attributable to postoperative complications for the surgical patient.
Postoperative complications are associated with higher mortality and increased LOS and hospital costs. Given the excessive resources required to treat complications, it is necessary to establish quality improvement programs directed at preventing those postoperative events that are the most costly and result in the longest LOS. Reducing the number of postoperative complications may result in cost savings that offset the initiation of the quality improvement programs that rely on clinical data, in particular the NSQIP. This study clearly demonstrates the financial imperative in addition to the patient care imperative for reducing the incidence of postoperative complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.