
Abstract
No published research has assessed the specific steps that primary care practices actually take to carry out screening for colorectal cancer (CRC). A written survey was distributed to clinicians and staff at 15 primary care practices to determine whether they perceived that personnel in their practices performed a series of 4 steps associated with screening colonoscopy and 7 steps associated with stool blood test screening. For each discrete step, the percentage of respondents from each practice who indicated that a given step is performed in that practice was calculated along with the mean of practice percentages. Survey results indicate wide variation in the degree to which these screening steps are performed across the 15 practices. Variation was greater for steps that involved contacting nonresponders (reminders), scheduling, and rescheduling. Survey responses suggest substantial variation and much room for improvement in practice performance of evidence-based steps in the CRC screening process.
Screening rates for colorectal cancer (CRC) have improved substantially in the past decade but remain suboptimal. For 1000 plans in 2009, the Healthcare Effectiveness Data and Information Set (HEDIS) rates for CRC screening for individuals ≥50 years of age were 55% for Medicare and 61% for commercial insurance. In contrast, in 2008, the rates for breast cancer screening with mammography (ages 40-69 years) within 2 years were 68% and 70%, and for cervical cancer screening with a Pap test (ages 18-69 years) within 3 years, the rate was 81% for commercial insurance. 1 Increasing CRC screening is an important public health priority. In primary care practice, achieving high CRC screening rates is an important measure of quality of care.
Although health plans are held responsible for screening rates, a recommendation from the provider has proven impact. There is strong evidence supporting the value of delivering a physician’s recommendation for screening to every eligible patient.2,3 Additional attention is needed on “organizational factors,” as defined by Price et al, 4 that can have a strong influence on cancer screening rates, which may be explored by examining “steps and interfaces” in the screening process. Other evidence-based approaches that boost screening rates have been defined.5,6 Provider reminders and patient reminders have been shown to lead to higher screening rates and improved quality scores and outcomes. Tracking of tests and referrals as well as audits with provider feedback are shown to improve screening rates.7-13 The value of assisting with appointment scheduling is supported by growing evidence.14-16 The degree to which these specific evidence-based steps are actually taken in primary care practices has been characterized for some but not for others. 17 The purpose of this report is to document the steps taken in practice to accomplish CRC screening.
Data presented here represent the first report in the literature that seeks to assess practice performance of the CRC screening process in a network of primary care practices. Findings are based on a written survey that collected information from practice clinicians and staff. Respondents were asked to indicate whether specific steps in the CRC screening process were performed in their practice. The sequence of steps was identified over a 20-year period through work by the research team with primary care practices in Pennsylvania and Delaware.18,19,3,20
The survey may be found in a toolbox available for use by primary care practices. 21 It was administered as part of an intervention to track and improve CRC screening and follow-up rates. 22 The data reported here were collected in the course of implementing an intervention intended to boost CRC screening among practice patients. These survey data provide a measurement of variation in the performance of specific steps in the screening process and a starting point for identifying aspects of primary care practice where variability reflects failure to use evidence-based strategies and highlights useful targets for improvement.
Methods
Setting
The System Approach to Tracking and Increasing Screening for Public Health Improvement of Colorectal Cancer (SATIS-PHI/CRC) intervention was part of a study sponsored by the Agency for Healthcare Research and Quality (AHRQ) and funded by the Centers for Disease Control and Prevention through an AHRQ program called Accelerating Change and Transformation in Organizations and Networks (ACTION).21,22 The ACTION program is designed to speed translation of evidence-based strategies into practice. The intervention was developed and implemented through a collaboration among (1) the Lehigh Valley Health Network (LVHN), whose affiliated primary care practices were the site of the intervention; (2)Thomas Jefferson University (TJU), an academic health center and health sciences university; and (3) CNA, a nonprofit research and analysis organization that is an AHRQ ACTION prime contractor.
Sample
The baseline survey and the SATIS-PHI/CRC intervention were carried out in 15 primary care practices that are part of a Practice-Based Research Network (PBRN) called the Eastern Pennsylvania Inquiry Collaborative Network or EPICNet. EPICNet is affiliated with the Lehigh Valley Physician Hospital Organization (LVPHO), which is a joint venture of the LVHN and the Greater Lehigh Valley Independent Practice Association. The LVPHO provides incentives to providers to engage in integrated efforts to improve quality and outcomes, and EPICNet brings practices together to answer community-based health care questions and translate research findings into practice. EPICNet staff completed a preimplementation assessment of participating practices, which included the baseline survey, focus groups, and key informant interviews. EPICNet also organized academic detailing education sessions for the participating practices, managed the day-to-day implementation and operation of the intervention, and collected postimplementation results.
EPICNet staff purposively recruited primary care practices that varied in specialty (family medicine/internal medicine), size (numbers of clinicians), location (urban, suburban, rural), ownership (LVHN/physician-owned, corporation/independent), and having paper-based versus electronic medical record systems. The LVHN practices were a mixture of hospital clinics, including residency clinics and community practices. A total of 15 practices participated in the survey. The LVPHO endorsed participation in the intervention as a quality improvement activity and reimbursed its physician members for their time. This participation included completing the survey.
Institutional review board approval for this project was provided by LVHN and the Office for the Protection of Human Subjects at TJU.
Survey Questionnaire and Administration
A 4-section, 75-item written survey was adapted from prior surveys used by TJU researchers.13,18,23,24 The initial page of the survey allowed respondents to indicate their role in the practice (ie, physician, other clinician, clinic staff, other staff). Respondents were instructed that 3 of the survey’s 4 sections were to be completed only by physicians or other clinicians. These sections inquired about preference for various CRC screening tests supported by current guidelines, perception of test effectiveness, how positive screens are usually followed up, and respondent demographics, specialty, education/training, and practice experience. All survey respondents were instructed to complete the fourth section, which is the focus of this article.
The fourth section of the survey asked respondents whether they or anyone else in the practice completed each of a series of steps associated with 2 CRC screening modalities: stool blood tests (SBTs) and colonoscopy, the modalities that were targeted by the SATIS-PHI/CRC intervention. The steps for screening colonoscopy were as follows: (C1) orders screening colonoscopy, (C2) schedules screening colonoscopy, (C3) contacts colonoscopy no-shows, and (C4) reschedules colonoscopy no-shows. The steps for SBT were as follows: (S1) gives SBT cards to patients, (S2) contacts SBT nonresponders, (S3) gives SBT results to patients, (S4) refers SBT-positive patients for follow-up, (S5) schedules SBT-positive patients for follow-up, (S6) contacts SBT follow-up no-shows, and (S7) reschedules SBT follow-up no-shows. The survey asked who in the practice performs each of these steps. The four response options were as follows: “I do it,” “Another person [in the practice] does it (specify job title),” “No one [in the practice] does it,” and “Don’t know.” Results from this section of the survey, along with information on practice characteristics obtained from administrative data, are presented in this report. The step sequence did not include the clinician’s recommendation for screening and the decision by the patient to be screened because the focus of this survey was on the steps taken by the practice (the organization) following an agreement to screen between clinician and patient.
EPICNet researchers distributed survey forms to the office managers of participating practices, who then distributed them to all clinicians and staff. The completed surveys were collected by the EPICNet researchers prior to the academic detailing session held at each practice that was part of the SATIS-PHI/CRC intervention. Scanned survey forms were sent by EPICNet to TJU on a password-protected compact disc. TJU researchers coded the surveys, entered the coded responses into an electronic data set, and imported the data set into SAS, version 9 (SAS Institute Inc, Cary, NC) for analysis. Analysis was conducted by TJU and CNA.
Data Analysis
For analysis purposes, the first 2 response options for a given step were classified as, “Yes,” indicating that it was being performed widely enough or consistently enough within the practice for the respondent to be aware of it being performed. The remaining 2 response options were categorized as, “No,” indicating that the step either was not being performed widely enough or consistently enough in the practice for the respondent to be aware of it being performed or that it was not being performed in the practice. For each step in the CRC screening process with either SBT or colonoscopy, the authors calculated the number and percentage of respondents in each practice with “Yes” and “No” responses. Respondents who did not respond to 1 or some (but not all) individual steps were coded as having given a “No” response.
For each step, the authors then compared the percentage of “Yes” responses in each practice and calculated the mean, standard deviation, and coefficient of variation of the 15 practice percentages. They looked both for steps that had relatively high or low means and for steps that had relatively high or low variability (as measured by standard deviations and coefficients of variation) between practices. Finally, they identified practices with high reported performance percentages across all screening steps for colonoscopy and/or SBT screening.
Results
Practice Characteristics
Respondents from 15 primary care practices in the Lehigh Valley of Pennsylvania participated in the SATIS-PHI/CRC intervention and completed the survey. Practice characteristics are displayed in Table 1.
Characteristics of Participating Primary Care Practices (N = 15)
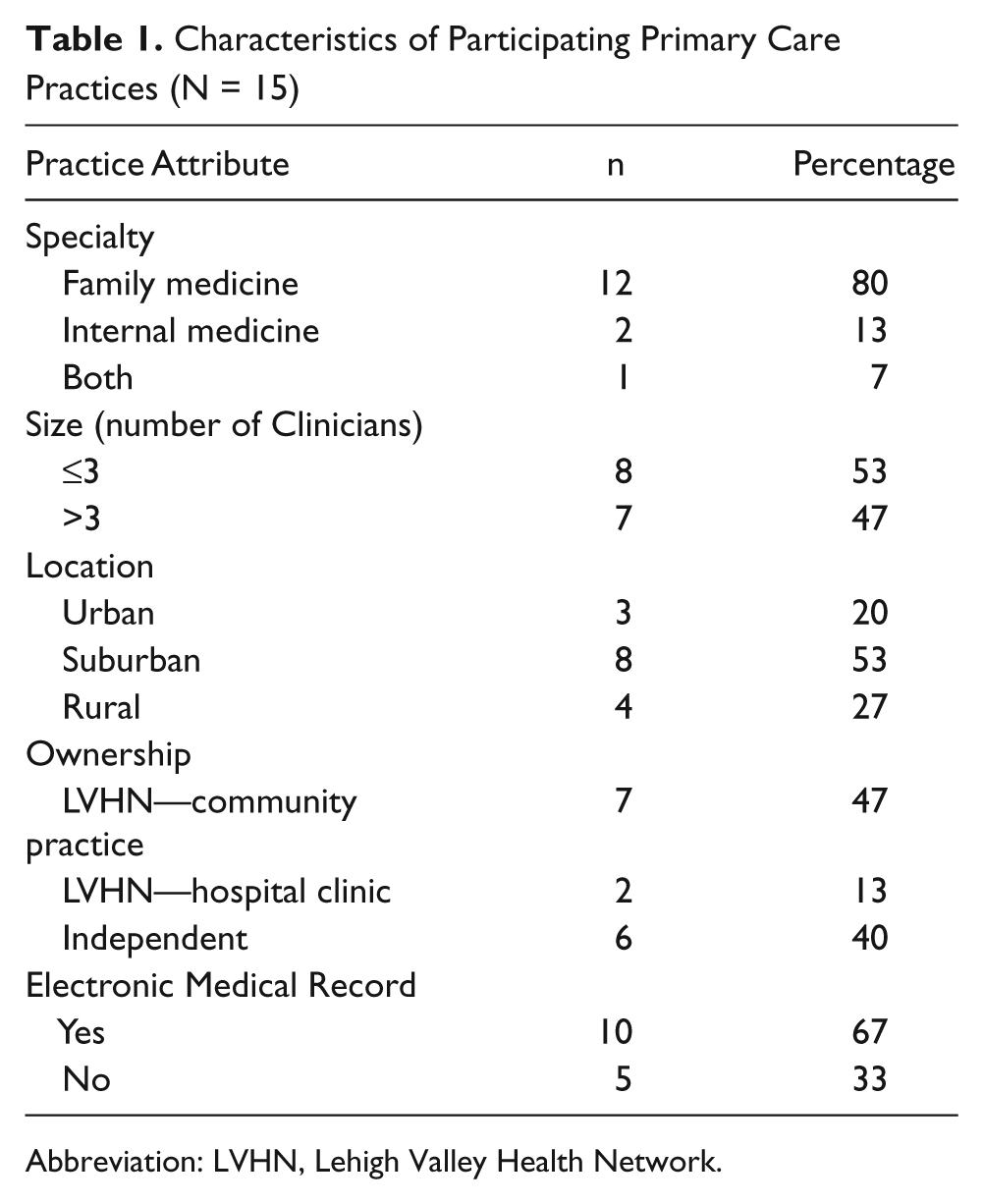
Abbreviation: LVHN, Lehigh Valley Health Network.
Respondent Characteristics
A total of 205 surveys were received from 285 staff for an overall response rate of 72%. (The range was 3-34 responses per practice.) The 12 respondents who did not answer the section on performance of screening steps were excluded, leaving a study population of 193. Overall, 53 (27%) of the 193 were clinicians, and 60 (31%) were clinical staff, for a total of 113 clinical staff. Nonclinical staff accounted for 59 (31%) responses. The roles of the remaining 21 (11%) respondents were unknown.
Screening Process Steps
Figure 1 presents the mean of the 15 practice percentages of respondents who indicated that they or someone else in their practice perform a given step in the SBT or colonoscopy screening process (a “Yes” response).
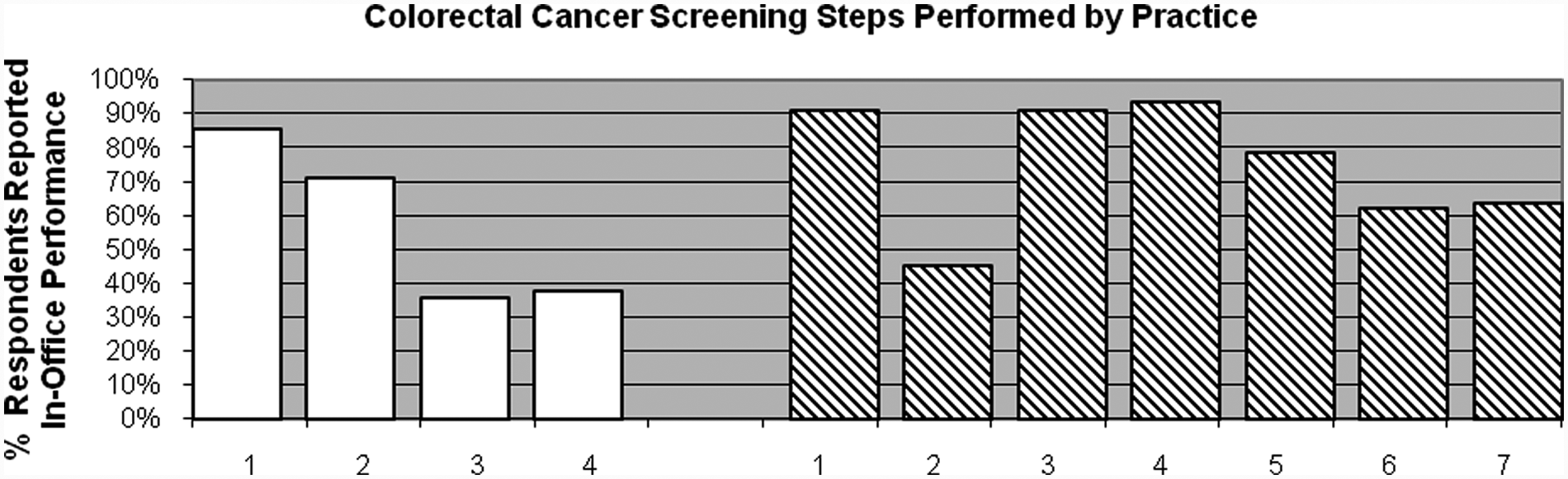
Performance of colorectal cancer screening steps reported by survey respondents (N = 193)a
Table 2 presents the number and percentage of respondents in each practice who indicated that they or someone else in the practice perform a given step in the colonoscopy screening process. In addition to the mean of the 15 practice percentages for each step, the table also presents the standard deviation and coefficient of variation for each distribution of percentages. The standard deviations and coefficients of variation reflect relative uniformity for the first 2 steps across all practices and significant variation for steps 3 and 4. When responses of clinicians and clinical staff were calculated as a single group distinct from the respondents as a whole, the results were similar to the responses from the entire group of practice respondents: C1, 91%; C2, 76%; C3, 35%; C4, 35%.
Colonoscopy (CX) Task Performance: All Respondents With Complete Data (N = 193)
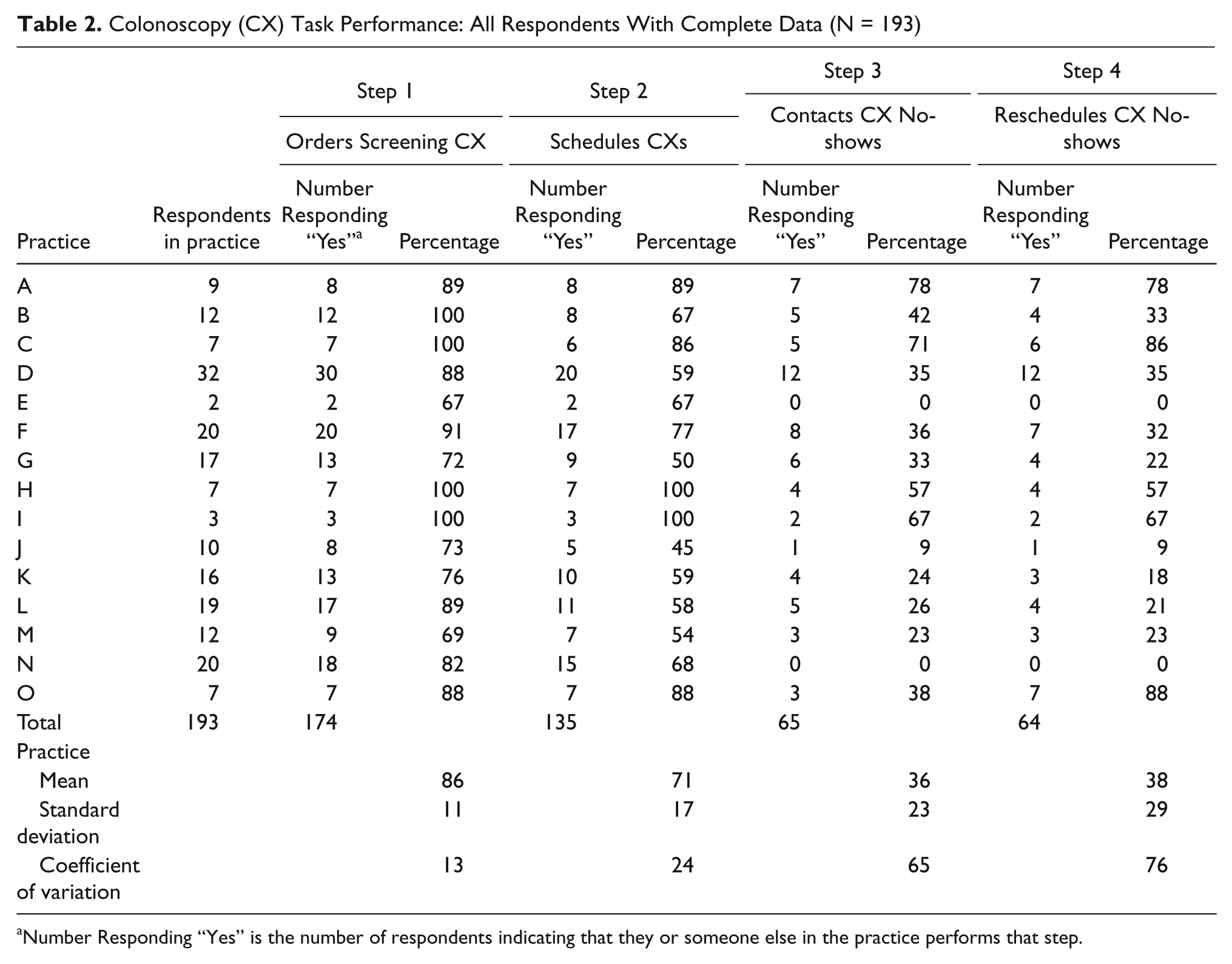
Number Responding “Yes” is the number of respondents indicating that they or someone else in the practice performs that step.
Table 3 presents equivalent results for SBT. Steps 2, 6, and 7 had lower means than steps 1, 3, 4, and 5. When responses of clinicians and clinical staff were calculated as a single group distinct from the total respondents, the results were similar to the responses from the practice respondents as a whole: S1, 96%; S2, 48%; S3, 92%; S4, 96%; S5, 79%; S6, 63%; S7, 65%.
Stool Blood Test (SBT) Task Performance: All Respondents With Complete Data (N = 193)
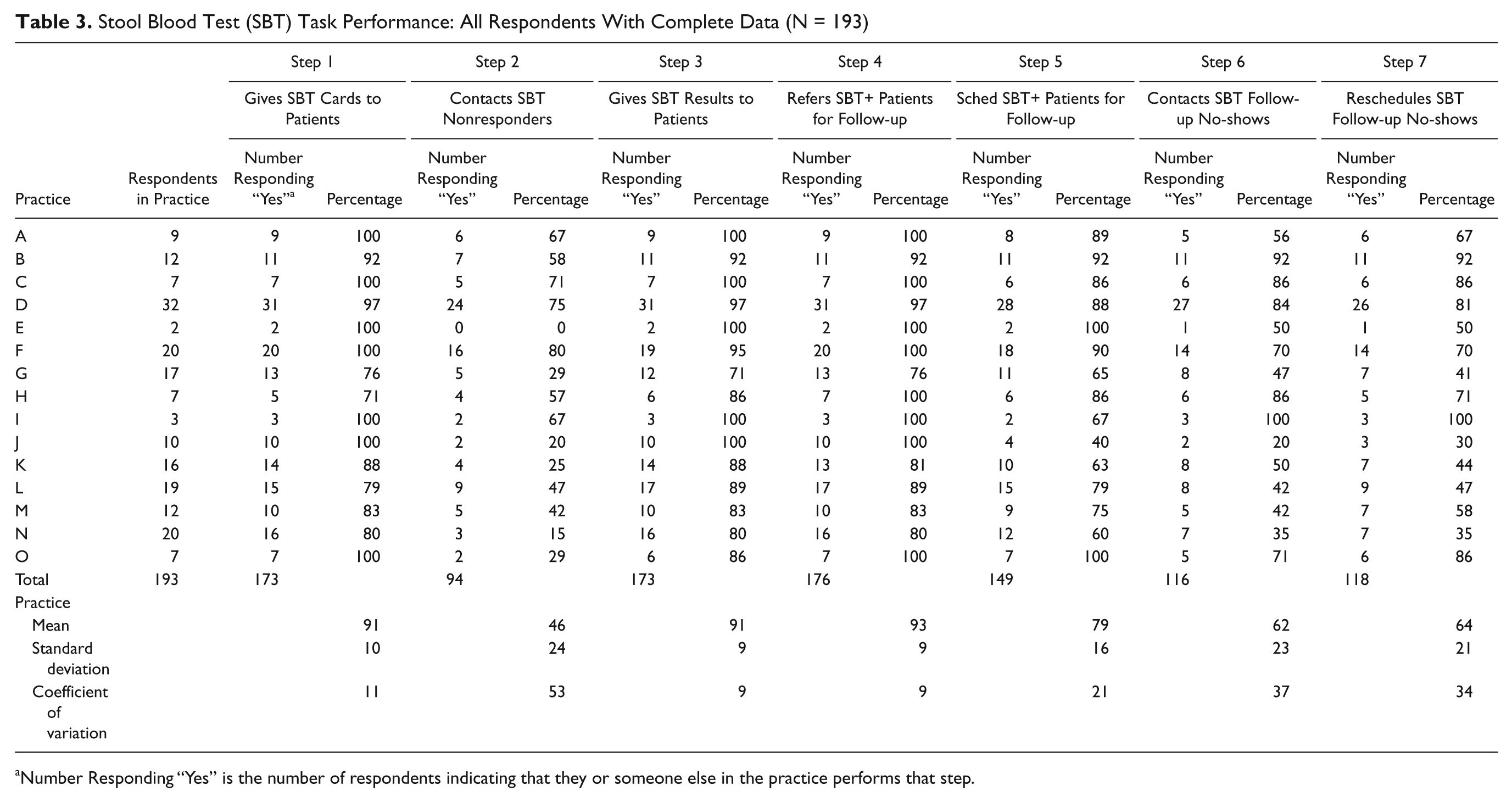
Number Responding “Yes” is the number of respondents indicating that they or someone else in the practice performs that step.
The results for colonoscopy and SBT demonstrate substantial reported variation in some screening steps taken within these primary care practices. A few practices reported step completion of more than 70% across all steps of the colonoscopy sequence, and a few have a similarly high percentage across all steps of the SBT process. Only 1 practice has a high percentage across all steps in both SBT and colonoscopy. The steps that demonstrate the most variation between practices are reminder, scheduling, and rescheduling.
Discussion
This study reports on a baseline survey that was completed prior to implementing the SATIS-PHI/CRC intervention in a group of 15 primary care practices. The survey examined the steps reported as completed by providers and other practice staff regarding performing CRC screening for 2 modalities—colonoscopy or SBT—within the practice. These 2 screening modalities are the ones most performed by practices in the Lehigh Valley of Pennsylvania according to claims data from the Physician-Hospital Organization.
Responses suggest variation in practice performance of evidence-based steps in the CRC screening process, with some steps performed less often than others within individual practices and across the practices. Within the SBT process, the second step, “contacts nonresponders,” is a reminder function that is reported as performed by a mean of 46% across all practices, with considerable variation among the practices. A second reminder function, “contacts patients with positive stool tests who didn’t show up for follow-up colonoscopy,” had a mean of 62%, and rescheduling of the no-shows had a mean of 64%. (These numbers are so close that they may be virtually the same, especially because the same people did not respond to every question.) These steps have substantial variation around the mean. Given the existence of the evidence base for the effectiveness of reminders 9 and rescheduling14-16 in producing completed screenings, these numbers indicate failure to use strategies that could improve screening rates.
The reminder step in colonoscopy screening (step 3: “contacts colonoscopy no-shows”) had a 15-practice mean of only 36%, with 11 of the 15 practices having percentages of “Yes” responses that were less than 50%, suggesting that this opportunity to raise screening rates also is lost in many practices. Similarly, the mean for rescheduling of colonoscopy no-shows (step 4) was only 38%, with 10 practices having percentages of “yes” responses below 50%. Yet some practices have incorporated these simple strategies. Seven of the 9 respondents in practice A (Table 2) agreed that the practice does in fact contact no-shows and reschedule them. Increased awareness within practices that fail to take these evidence- based approaches used by their peers could instigate self-examination and change and thus contribute to the diffusion of best practices. These results are being shared with all the practices.
It seems reasonable to ask both why there is so much variation and what should be done to disseminate these useful strategies. There are a number of possibilities. Reporting of practice metrics is one that may contribute. There is evidence that health plans that report HEDIS measures adopt evidence-based strategies, although it is less clear to what degree that occurs at the individual practice level. 25 Some plans may be unaware of evidence that favors patient reminders or scheduling/rescheduling. The Guide to Community Preventive Services (www.thecommunityguide.org) posts proven strategies that have been shown to work for preventable conditions, along with the evidence for them, in an easily accessible Web-based location. 26 This resource may be better known to the public health community than to the clinical or managed care communities. Health plans that are aware could play a role in disseminating this knowledge to their participating practices in order to precipitate increased adoption of these evidence-based strategies.
Of course, knowledge about peer practices or even the benefit of those practices may be insufficient. The pressure of time is real and cited frequently. 27 Office staff may not be trained for these tasks, or the tasks may be viewed as secondary in importance to other responsibilities. Some may feel it simply is not the responsibility of the practice to remind patients. For colonoscopy specifically, as opposed to SBT, these primary care practices were significantly less likely to contact no-shows or to reschedule them. This is not surprising because specialists generally perform the colonoscopy and are reimbursed for it. Thus, processes that pertain to colonoscopy may be viewed as outside the responsibility of the primary care practice. However, it should be noted that these processes may not be viewed as outside the responsibility of primary care practices that aspire to be patient-centered medical homes (PCMHs) or seek to achieve maximal screening rates. 28
There are a number of health delivery mechanisms, both structural and financial, that could improve adherence to evidence-based approaches. The PCMH model is an approach that encompasses structural and financial elements. The activities of managed care organizations, insurers, or accountable care organizations also may encompass structural and financial mechanisms. Pay for performance is a financial mechanism that provides monetary incentives for improved outcomes. Addition of specific personnel (eg, navigators, case managers) to the team of care providers who work directly with the patient (by phone or in person) also could enable the added functions to be performed. Navigators can be employed in-house or by a group external to the practice.
The PCMH is a practice model that combines an expansive definition of primary care practice with a higher rate of reimbursement. In this model, increased reimbursement supports evidence-based features shown to improve outcomes, such as reminders, audits, performance feedback, assistance with scheduling, and better use of practice staff. Many of these features are expected to put prevention into practice in conjunction with improvements in information technology systems (exemplified by “meaningful use” criteria). 5
Despite the fact that this is a preliminary look at step performance with an imperfect measure, these data suggest that there are many opportunities to benefit patients and improve outcomes from the use of evidence-based strategies that should garner better adherence. There is significant variation in the uptake of these effective strategies. The work of Klabunde et al 17 has documented limited use of either provider or patient reminders in primary care practices across the country. Research is needed over a wider geographic area that documents the variation in other evidence-based steps. If in fact this variation is widespread, as seems likely, the survey may be a useful tool to identify specific weaknesses in the management of the CRC screening process in primary care and to identify practices that need support to address these weaknesses. A related need will be support to design and test intervention approaches to meet those needs and to assess their impact on screening processes and related outcomes. Although electronic health records may hold promise as a basis for future interventions, focus group data with the same practices, also collected as a prelude to this intervention, documented limited use of the relevant electronic health record functionalities.
A limitation of this study is that the measures of step completion are based on self-report by the people who are employed by the practices. There is no outside verification of step completion beyond their judgment. Furthermore, this survey was conducted in only 1 PBRN, in 1 area of the country, and the results may not be generalizable. Further research will help clarify this point. This study also does not verify whether a recommendation to screen is given to every eligible patient. Focus groups with clinicians, followed by continuing medical education, were a part of the larger study. The focus groups solicited input regarding screening practices; the education stressed the importance of giving a recommendation to screen to every eligible patient. The continuing medical education also provided updates on consensus guidelines. Physician recommendation is the most consistently influential factor in whether or not patients are screened. 3
Another limitation is that specialty practices were not surveyed, so there are no data on whether the colonoscopists and their staff use reminders or reach out to reschedule no-shows. A lack of information about the process steps completed in specialty practices is typical of the milieu in which primary care is practiced. In addition, this survey of step completion may or may not be associated with higher screening rates. That analysis is forthcoming using additional data from the SATIS-PHI/CRC study.
We might ask whose role it is to ensure that colonoscopy is completed. Our results suggest that some primary care practices execute steps toward completion of colonoscopy in their own practices, whereas others do not. To what extent specialty practices complete these steps is an unanswered question. Answering this question for each primary care practice will require coordination between the primary care practice and colonoscopy practice. Lack of communication for the purposes of coordination prevents either party from gaining a complete picture of the services that are delivered. Coordination between practices is vital and will decrease the odds of confusion on the part of primary or specialty practices, as well as the patient, if it is implemented in a patient-centered way. Communication, clearly, is a major part of this; however, the current communication between primary care and specialty practices varies widely.29-32,4
In the spirit of patient-centeredness promoted by the Institute of Medicine and included in the vision of the PCMH model, it is important that those who work within the delivery system find a way to address the missing steps and improve quality of care. The central principles of the PCMH model stress the relationship between patient and provider, with increased reimbursement for the practice in return for an expanded definition of primary care that includes reminders, test/referral tracking, and the use of information technology to optimize information sharing, population management, and quality reporting. If increasing numbers of primary care practices pursue designation as a PCMH, as seems likely, they will need to examine their own processes and put in place new office policies, structures, and processes that incorporate reminders and tracking systems, scheduling assistance, and improved communication and coordination with specialists for screening and follow-up.
CRC screening is regarded as one of the highest priority preventive services. 33 The description of steps involved in CRC screening presented in this report points to many opportunities for practices to benefit from implementation of evidence-based components of practice. The survey that uncovered these opportunities is 1 method by which a practice may obtain a complete picture of its own process. In the primary care setting, such examination of the practice is likely to be increasingly viewed as an essential move toward attaining quality goals, including better CRC screening rates and transformation to a PCMH.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research report is based on the System Approach to Tracking and Increasing Screening for Public Health Improvement of Colorectal Cancer (SATIS-PHI/CRC) intervention study conducted as a task order under the Accelerating Change and Transformation in Organizations and Networks (ACTION) program of the Agency for Healthcare Research and Quality (AHRQ), contract number HHSA-290200600014, task order 1, and funded by the Centers for Disease Control and Prevention. Primary care practices affiliated with the Lehigh Valley Physician-Hospital Organization (LVPHO) and the Eastern Pennsylvania Inquiry Collaborative Network (EPICNet) served as the sole clinical setting for this project.