
Abstract
Educational outreach is a common quality improvement (QI) strategy used alone and in combination with other interventions. However, a meta-analysis of educational outreach has failed to identify reasons for variation in its impact. To better understand such variation in findings, a more comprehensive set of characteristics about educational outreach is needed. This article describes the contribution that diffusion of innovations theory and evidence-based continuing education practices can make toward standardizing a set of characteristics to guide QI and research efforts using educational outreach. The article offers a set of characteristics and describes the implications of the set for research and QI efforts.
Educational outreach is a common intervention used by quality improvement (QI) professionals to improve the quality of patient care. 1 Also referred to as university-based educational detailing, academic detailing, and educational visiting, among other titles, 2 educational outreach is 1 or more face-to-face visits by a trained person with a clinician in his or her practice setting in order to provide information in support of practice change.2,3 The most recent Cochrane Review of educational outreach—as a single intervention and as part of a multifaceted strategy—identified this intervention as one that has a small but consistent effect on prescribing behavior and one that has a small to modest effect on other types of clinician behavior. 2 Despite examining a variety of predetermined variables that included 3 intervention characteristics (ie, number of clinicians included at each visit, number of visits, and the contribution of educational outreach as a component of a multifaceted intervention), the review was not able to explain the variation in impact associated with educational outreach (Table 1). 2 The review mentioned 2 other intervention characteristics that the authors did not statistically assess as contributors to variation but that may be important nonetheless: tailoring visits to barriers to change and using an influential person to conduct the visits. 2 The purpose of the current article is to consider how theory and evidence may help standardize the set of educational outreach characteristics that QI leaders and researchers should consider in guiding and in understanding the use of this valuable intervention strategy.
Potential Characteristics and Ideas for Characteristics of Educational Outreach by Source
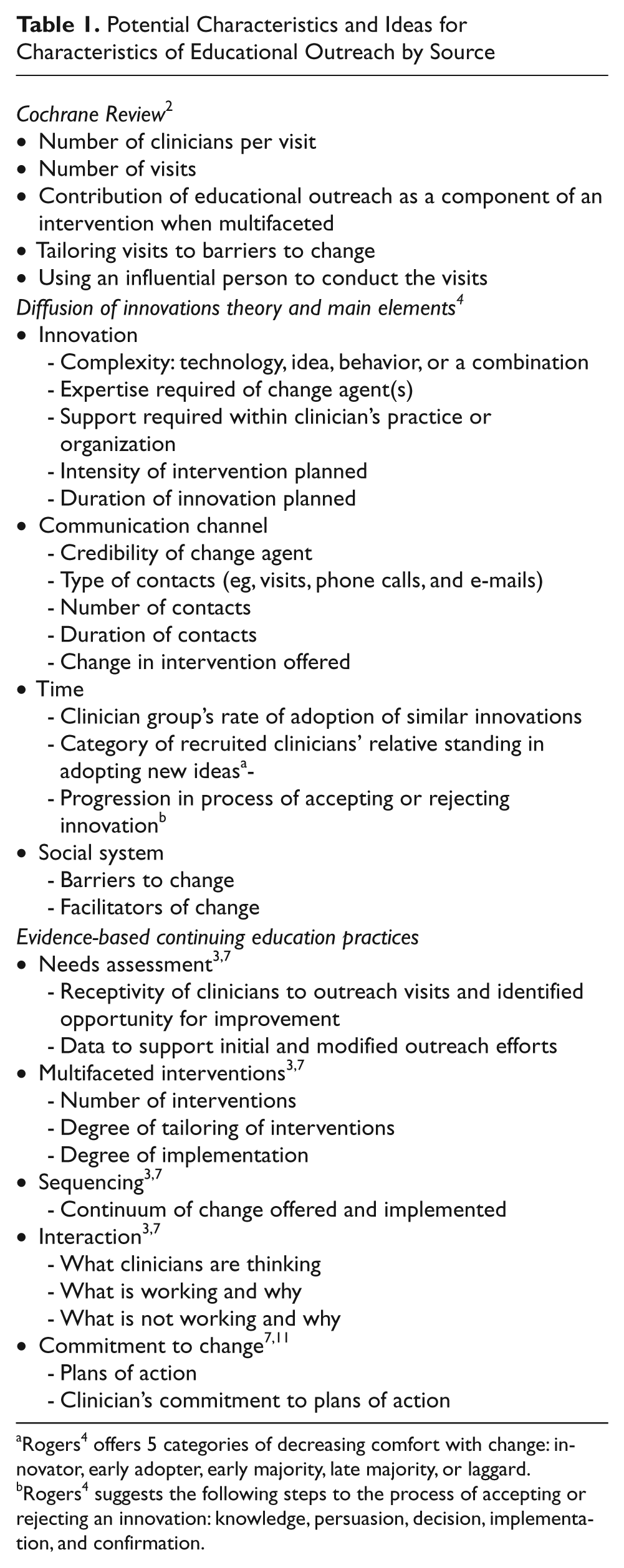
Rogers 4 offers 5 categories of decreasing comfort with change: innovator, early adopter, early majority, late majority, or laggard.
Rogers 4 suggests the following steps to the process of accepting or rejecting an innovation: knowledge, persuasion, decision, implementation, and confirmation.
Discussion
Theory
We believe that diffusion of innovations is the most relevant theory to inform educational outreach efforts. 4 Starting in the 1940s with an attempt to understand the spread of agricultural innovations through a group of farmers, diffusion research is an interdisciplinary attempt to understand how innovations spread across social groups. 4 Some authors have applied diffusion of innovation ideas specifically to continuing education (CE) in health care. 5 Rogers defines diffusion as “the process in which an innovation is communicated through certain channels over time among members of a social system,” and he identifies 4 main elements of this “special type” of communication: (1) the innovation itself, (2) the communication channel, (3) time, and (4) the social system.4(pp5-6) An innovation can be a technology, an idea, or a behavior, and although the innovation may be new, what matters is only that it is perceived as new to the client whose behavior one is trying to change. 4 The communication channel represents the means by which information is exchanged between the change agent (ideally a person whose background and education are similar to the client’s but with additional expertise concerning the innovation) and the client. Rogers describes this communication as being 2-way and iterative and leading to a mutual understanding between the change agent and client about the innovation and its relevance to the client’s practice. 4 For diffusion of innovations, time has 3 separate meanings: time reflecting the anticipated, relative speed of the rate of adoption across a group of clients; each client’s relative comfort and standing with adopting new ideas (ie, whether he or she is in the category of innovator, early adopter, early majority, late majority, or laggard); and the time associated with a 5-step decision process regarding the innovation (ie, acquiring knowledge about the innovation, being persuaded to try it, making a decision to adopt or reject a trial, implementing the innovation, confirming the decision to maintain the innovation). 4 Finally, the social system is the context in which the client is operating, including its structural elements, social norms, involvement of opinion leaders and other influential persons, communication networks, decision control, and consequences (ie, direct and indirect, anticipated and unanticipated, desirable and undesirable) of innovation decisions. 4
Diffusion of innovations theory offers a relevant perspective on educational outreach characteristics. With respect to the innovation, whether it is a technology, idea, or behavior (or some combination thereof) relates to the complexity of the change required, the expertise needed in the change agent(s), the support of various team members (eg, medical assistant and office manager in the outpatient setting) in the clinician’s practice or organization, and the intensity and duration of the intervention planned. The communication channel requires organizations to select change agents carefully (assessing who may be credible to a clinician group) and to be prepared for the outreach efforts to reflect a process that may require change in the approach and multiple visits and other contacts (eg, phone and e-mail support) with each clinician. Time is relevant to the likely duration of the intervention period given the clinician group’s rate of adoption of similar innovations. For example, some disciplines, specialties, or practice sizes may be able to adopt more quickly than others. Time is also relevant to recruitment efforts because certain clinicians (ie, late majority, laggards) within a group may not be ready for the innovation but others (eg, early adopters, early majority) may be. Time is also relevant as a reflection of where in the process (eg, knowledge, persuasion, decision, implementation, confirmation) any clinician is; change agents must be aware of this for each clinician and offer appropriately targeted assistance. Finally, social system is always important, particularly for larger practices and organizations because QI interventions always are influenced by local conditions. 6 Organizations offering changes should not rely on clinicians to be aware necessarily of important contextual variables that may influence the process; change agents must continually assess for barriers and facilitators of change as part of their outreach efforts.
Evidence
As an educational intervention, educational outreach may be informed by the growing evidence of effective CE practices. Five specific CE practices in particular have relatively long-standing literature support: needs assessment, multifaceted interventions, sequencing, interaction, and commitment to change.3,7 Needs assessment is the process of collecting data about clinicians (eg, performance data) or about the care they provide (eg, patient outcomes, barriers to care, facilitators of care, incentives) for the purpose of developing a relevant educational activity.3,7 Ideally, needs data will come from multiple sources 8 perceived as credible and actionable by clinicians. 9 A multifaceted intervention is the act of combining 2 or more educational or QI strategies (eg, interactive clinician workshop plus patient reminders) for the purpose of addressing the same opportunity for improvement.3,7 Sequencing is an explicit, logical order underlying an educational activity or series of activities for the purpose of helping participants learn.3,7 For example, performance assessment and feedback with peer and benchmark comparisons may prepare clinicians for a subsequent intervention (eg, clinician reminders) to support behavior change. Although interaction in the social sense can promote the deep thinking 10 necessary for effective learning in CE,3,7 interaction actually refers to what is occurring within the minds of learners that can lead to sustained learning and behavior change. 10 Activities such as role play, case discussion, and active reflection about gaps in performance and barriers to change are consistent with this description of interaction.3,7 Finally, commitment to change is asking clinicians to change a specific and measurable behavior as a result of a CE activity.7,11 An example of a commitment to change request might be asking clinicians to pilot a patient reminder system to increase influenza vaccination rates among eligible patients with diabetes. 7
As with theory, evidence-based CE practices offer an important perspective on educational outreach characteristics. Needs assessment would provide information about whether a group of clinicians would be receptive to educational outreach visits and how interested they are in identified opportunities for improvement. Needs assessment data also would be helpful in designing and adjusting the QI intervention as initial and new barriers to change arise. The practice of multifaceted interventions would suggest that change agents should not use a single intervention strategy but rather a combination of strategies, ideally based on the targeted needs of each clinician. Change agents conducting educational outreach visits are in an ideal position to observe what interventions would be most helpful as the process unfolds; making firm recommendations from a menu of interventions options would support mutual decision making. Closely related to multifaceted strategies is sequencing, which demands that the order of activities should bring clinicians along a logical continuum of change, from awareness to knowledge, knowledge to skill, skill to behavior, and behavior to outcomes, for example. Change agents should describe the logic of the strategy to promote QI sophistication among clinicians. Interaction argues that the more change agents can engage clinicians and help them think critically about their practice and about their patients the more likely that the intervention strategy will be successful in changing clinician behavior and in improving patient outcomes. Mutual exchanges and critical thinking also will help change agents understand what is working, what may not be, and why. Finally, commitment to change sets an expectation that clinicians will commit to trying new ideas and forces change agents and clinicians to develop plans of action for the time between visits, which otherwise may be less productive. Given that change agents presumably are supporting clinicians and their teams, it is reasonable for clinicians to make and honor similar commitments to the process.
Educational Outreach Characteristics
Based on findings from the Cochrane meta-analysis, diffusion of innovations theory, and evidence-based CE practices, we propose a set of educational outreach characteristics organized into 5 categories: content, communication, clinicians, change agents, and context (Table 2). The categories themselves (ie, the 5 Cs) are much less important than the characteristics proposed within them. The characteristics are by no means exhaustive, however, because other characteristics (eg, patient characteristics or a broader set of clinician and contextual characteristics) also may influence the impact of educational outreach. This article focuses primarily on the characteristics that are directly attributable to educational outreach itself.
Recommended Educational Outreach Characteristics for Use and Further Study a
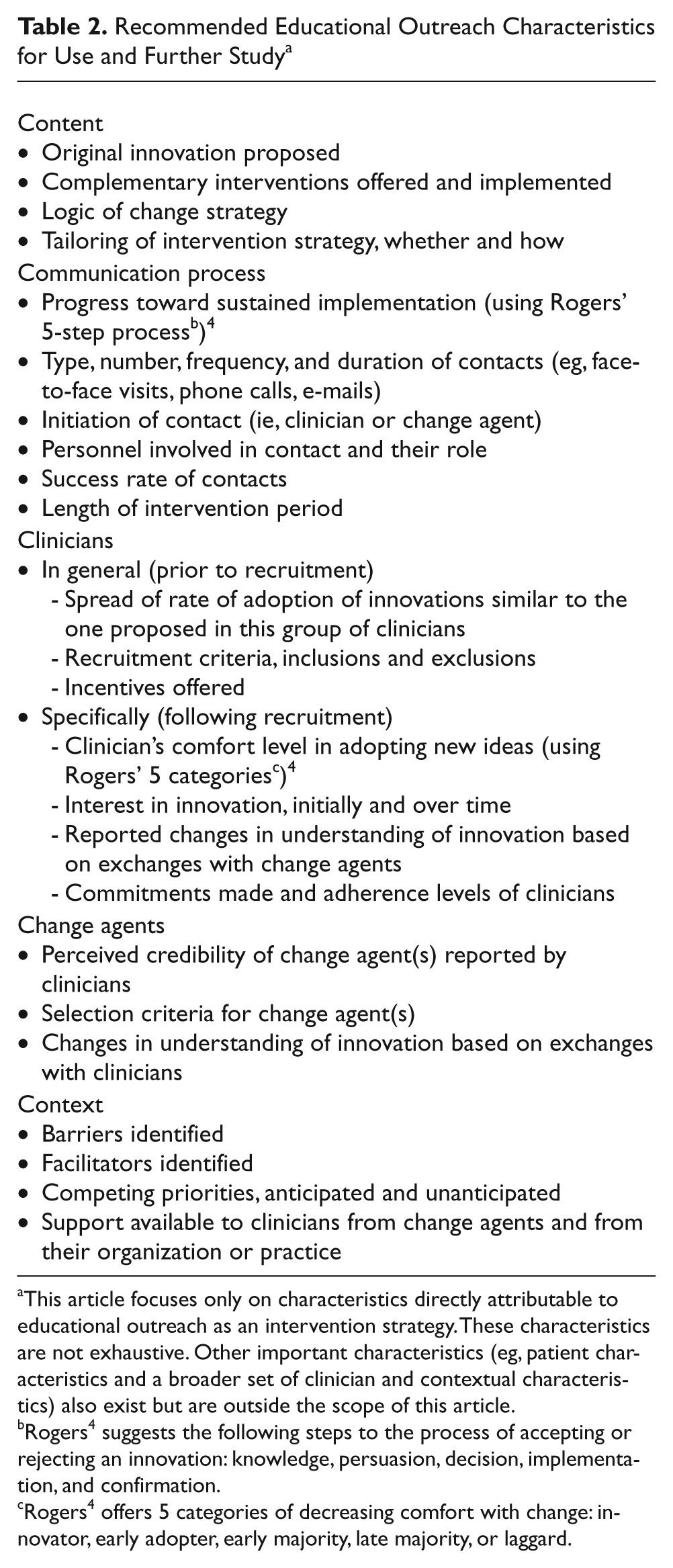
This article focuses only on characteristics directly attributable to educational outreach as an intervention strategy. These characteristics are not exhaustive. Other important characteristics (eg, patient characteristics and a broader set of clinician and contextual characteristics) also exist but are outside the scope of this article.
Rogers 4 suggests the following steps to the process of accepting or rejecting an innovation: knowledge, persuasion, decision, implementation, and confirmation.
Rogers 4 offers 5 categories of decreasing comfort with change: innovator, early adopter, early majority, late majority, or laggard.
The content of educational outreach should include characteristics such as the innovation proposed, complementary interventions (if part of a multifaceted strategy) offered and implemented, the logic of the change strategy (particularly if designed based on a needs assessment), and the degree of tailoring (whether and how) of the intervention strategy. Having provider-specific details would be important if variation exists across different clinicians being served by the intervention strategy.
Communication refers to the process through which the change agent interacts with clinicians and their teams, including progress toward sustained implementation of the innovation reflecting Rogers’ 5-step process (ie, knowledge, persuasion, decision, implementation, confirmation) or a similar construct. 4 Also part of this category is the type, number, frequency, and duration of contacts (eg, face-to-face visits, phone calls, e-mails); who initiated contacts; personnel involved in contacts and their roles; success rate of contacts by change agents; and the total length of the intervention period for each clinician.
Characteristics relating to clinicians include general issues prior to recruitment, such as the spread of rate of adoption of innovations similar to the one proposed in this or a similar group of clinicians, incentives offered for participation if any, and inclusion and exclusion criteria for recruiting clinicians. Characteristics specific to recruited participants include clinician comfort levels with adopting new ideas (using Rogers’ 5 categories of innovator, early adopter, early majority, late majority, or laggard), 4 their interest in the innovation at the outset of the project and as the intervention progresses, their self-reported understanding of the innovation based on exchanges with change agents, and the commitments and follow-through on commitments to change throughout the process.
Characteristics relating to change agents are the criteria their employer uses to select them, their perceived credibility to clinicians with whom they are working, and any evolution in change agents’ understanding of the innovation based on exchanges with clinicians.
Finally, context refers to barriers and facilitators identified by change agents over the course of the intervention period, competing priorities (anticipated and unanticipated) of clinicians, and perceived support available to clinicians throughout the project from their organizations or practices and through change agents.
Implications for Research and Practice
A comprehensive and standardized set of characteristics will be helpful to research efforts that measure the effectiveness of educational outreach and to help explain the variation in findings of this intervention strategy. Given the increasing number of terms and, possibly, meanings associated with educational outreach and given the different types of change agent roles (eg, opinion leaders, outreach educators, academic detail workers, clinical champions) in the literature, 12 having more details about educational outreach efforts will decrease the need to make assumptions about particular educational outreach terms and titles in research articles about such interventions. Some of the characteristics proposed may require new approaches to evaluation, particularly formative evaluation. For example, real-time changes to an intervention approach based on data about interactions between change agents and clinicians will require a rigorous evaluation system accompanied by a formative evaluation model that is detail oriented and accommodates different phases and uses of data. Some organizations are developing evaluation databases for this purpose, 13 and at least 1 formative evaluation model is available to support such research efforts. 14
Characteristics about educational outreach also are very important for QI leaders and experts using educational outreach but not necessarily disseminating the findings in the literature. Although collecting more information will require additional resources, the efforts also may be cost-effective, particularly if such data result in a better intervention design. Such data also may support a better assessment of clinicians’ comfort level with innovations and other relevant factors, which in turn may lead to more informed recruitment of clinicians who are ready for change and receptive to educational outreach efforts. 15 Recruitment represents an investment in project efforts, so it is best to select clinicians and providers carefully with the intervention strategy in mind. Collecting additional data about the process may increase the likelihood that efforts will have an impact on practice because leaders will be able to make adjustments to the approach taking into account the barriers, facilitators, and other factors discovered as QI efforts unfold. Furthermore, having more data about educational outreach efforts will help QI experts discern between “intervention failure” and “implementation failure” in the event that the efforts involving educational outreach are not successful. 16
Conclusion
Educational outreach is a common yet relatively complex intervention strategy, and a meta-analysis of well-conducted studies using educational outreach has failed to explain variation in results involving the intervention. To better understand the use and impact of educational outreach, especially in the context of growing terminology related to it, a comprehensive and standardized set of characteristics is necessary. A synthesis of diffusion of innovations theory and evidence-based CE practices yields some novel and important insights into what characteristics may be important to consider and study. This article has proposed a set of characteristics for discussion, which we believe is essential to advance the appropriate and informed use of educational outreach in QI activities and research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.