
Abstract
Foley catheterization (FC) is known to result in complications. Validated checklists are central to teaching/assessing procedural skills and may result in improved health care quality. The results of the first step of the validation of male and female FC checklists are described. A comprehensive literature review of articles published on FC did not yield a checklist validated by the Delphi method. A modified Delphi technique involving a panel of 7 experts was used to develop FC checklists. The internal consistency coefficients using Cronbach’s α were .91 and .88, respectively, for males and females. Developing a 24-item male FC checklist and a 23-item female FC checklist for teaching/assessing FC is the first step in the validation process. For these checklists to become further validated, they should be implemented and studied in the simulation and the clinical environments.
Foley catheterization (FC) is an invasive procedure commonly performed in inpatient and outpatient medical care. Numerous health care professionals such as nurses, nurse practitioners, physician assistants, residents, and attending physicians routinely insert Foley catheters. Nearly 450 000 catheter-associated urinary tract infections (CAUTIs) occur in the United States each year, resulting in an annual cost of $340 million to $450 million. 1 CAUTI is the most common nosocomial infection, accounting for more than 30% of infections reported by US acute care hospitals each year. 2 CAUTI is the most common type of health care–acquired infection in critical care and non–critical care settings.3,4 Approximately 17% of hospital-acquired bacteremias are from a urinary source, with a mortality rate of about 10%. 2 The significance of the complications associated with FC has led to the need for development of a validated checklist for this procedure.
The use of checklists has been demonstrated to improve quality of care in intensive care units, as noted by Gawande. 5 The authors’ search of peer-reviewed literature identified 9 articles that included the use of a Foley checklist. All were developed and vetted by expert faculty members6-13 or modified from a previously published checklist. 14 Additional Internet searches identified multiple other checklists that are used in various clinical settings as guidelines for FC. To the authors’ knowledge, none of these studies used the modified Delphi technique to validate the checklist. The results of the first step of the validation process for the development of checklists for teaching and assessing male and female FC are described.
Methods
Review of the Literature
One author (EMJ) conducted a comprehensive literature review by searching Ovid MEDLINE 1990 to February week 4, 2012, and Ovid MEDLINE In-Process & Other Non-Indexed Citations 1990 to March 1, 2012, to identify English-language articles published on checklists used for teaching or measuring competence in FC. A combination of relevant Medical Subject Headings (MeSH) and/or keywords were used in the search strategies (details are available from the authors on request). After removal of duplicates, the literature review yielded 279 references. All titles were reviewed for possible inclusion and 86 were obtained for further review. The reference sections of these articles were reviewed and 12 additional references were obtained. All articles obtained were reviewed for possible inclusion of a validated checklist. Nine articles included or referred to a published checklist, as mentioned.6-14
Checklist Development and Delphi Rounds
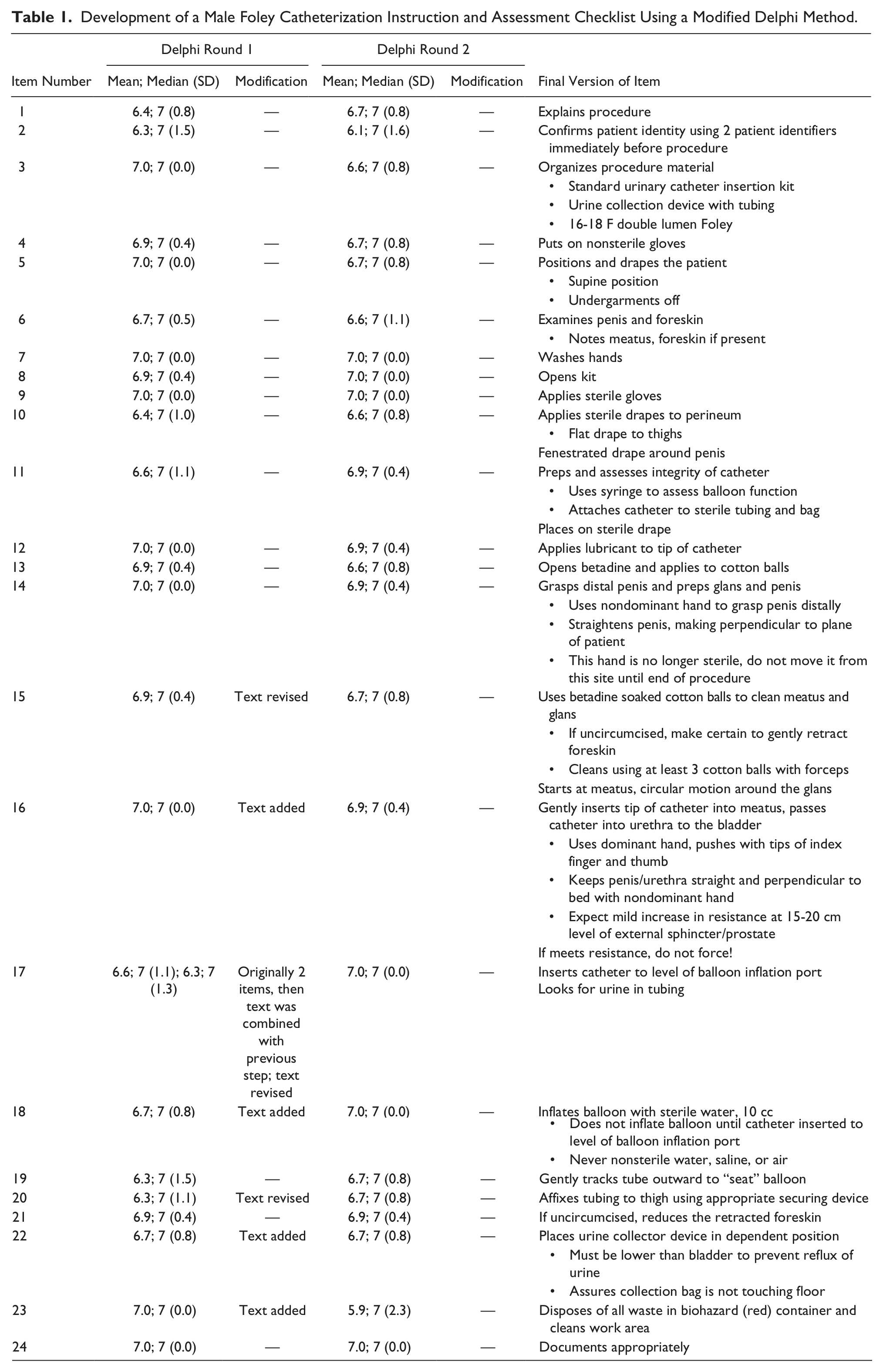
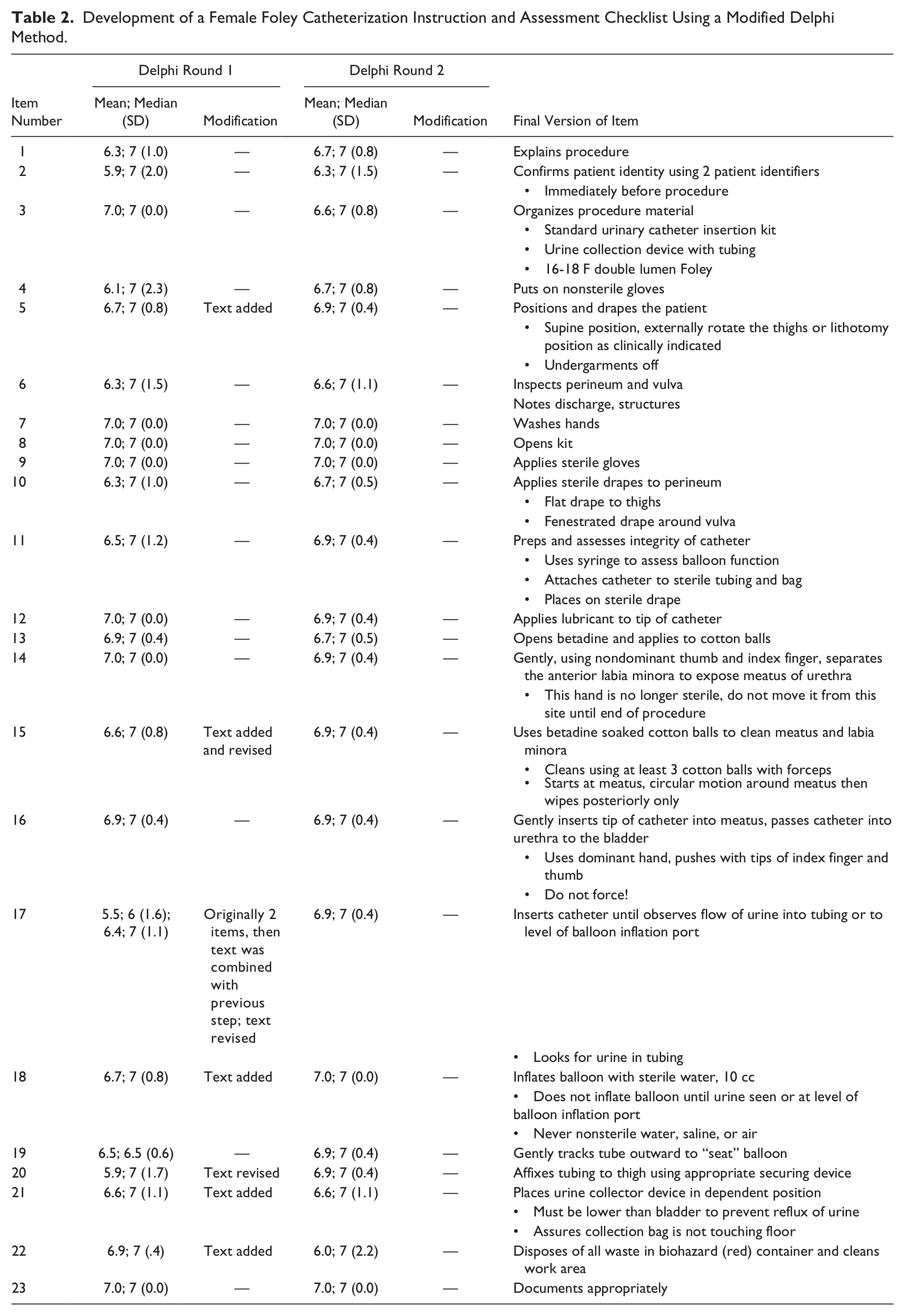
A modified Delphi method, explained in more detail in a previous article, 15 was used to develop the FC checklists. Preliminary checklists of procedural steps were developed by 2 of the authors (DB and KB) based on their experience teaching and performing FC (Tables 1 and 2). Experts were instructed to rate the importance of performing each item on the preliminary checklist on a 7-point scale, wherein 1, 2, and 3 represent not important; 4, 5, and 6 represent somewhat important; and 7 represents mandatory. Items on the checklist with a mean rating of 1 to 3 (not important) were removed from the checklist. Revisions were made based on the free-text edits and comments provided by the experts. The revised checklist was resent to the experts via e-mail for a second round of rating and editing.
Development of a Male Foley Catheterization Instruction and Assessment Checklist Using a Modified Delphi Method.
Development of a Female Foley Catheterization Instruction and Assessment Checklist Using a Modified Delphi Method.
Experts
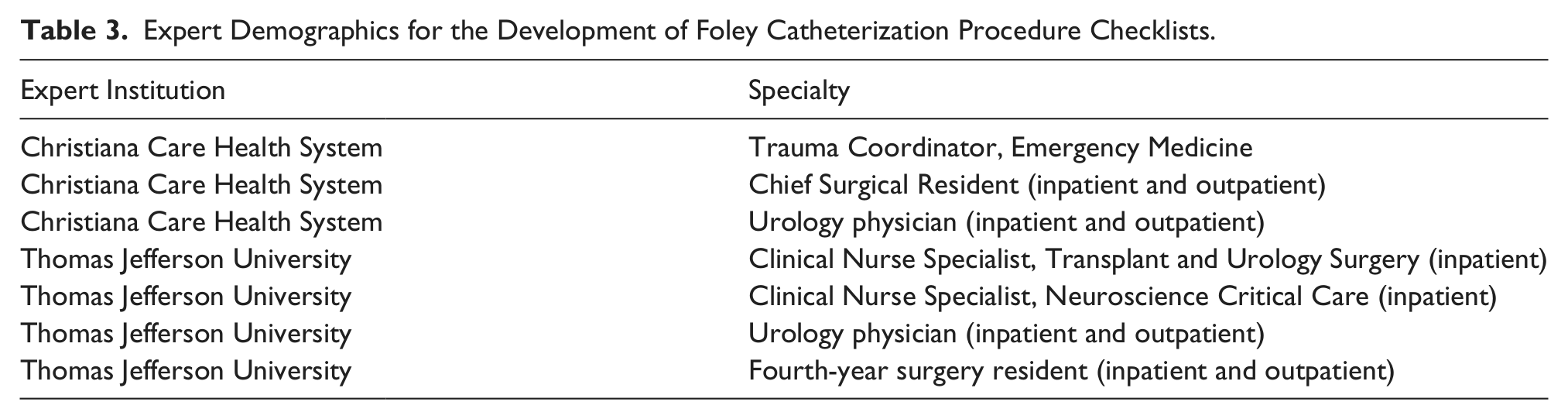
Seven experts, 4 from Thomas Jefferson University and 3 from Christiana Care Health System, participated in this study. Their specialties are shown in Table 3.
Expert Demographics for the Development of Foley Catheterization Procedure Checklists.
Statistical Analysis
The experts’ ratings were used to calculate the internal consistency of the checklists using Cronbach α in SPSS statistical software (IBM, Armonk, NY). The study was reviewed by the institutional review boards at both institutions and granted exempt status.
Results
The preliminary checklist for male FC included 25 items (Table 1). In the first round of the Delphi process, all items were felt to be “somewhat important” or “mandatory” to the procedure because the mean scores were greater than 4 (range = 6.3-7.0). Thus, all items remained on the checklist.
Based on experts’ comments, 2 items were combined into 1 item, revisions were made to 3 items, and text was added to 4 items. A 24-item checklist was generated (Table 1).
In the second Delphi round, the range of means was 5.9 to 7.0. All items had a median score of 7. No new item recommendations were made. The experts agreed on all items; therefore, the 24-item male FC checklist was finalized (Table 1). The internal consistency coefficient using Cronbach α was .91.
The preliminary checklist for female FC included 24 items (Table 2). In the first round of the Delphi process, all items were felt to be “somewhat important” or “mandatory” to the procedure because the mean scores were greater than 4 (range = 5.5-7.0). Thus, all items remained on the checklist.
Based on experts’ comments, 2 items were combined into 1 item, revisions were made to 3 items, and text was added to 5 items. A 23-item checklist was generated (Table 2).
In the second Delphi round, the range of means was 6.0 to 7.0. All items had a median score of 7. No new item recommendations were made. The experts agreed on all items; therefore, the 23-item female FC checklist was finalized (Table 2). The internal consistency coefficient using Cronbach α was .88.
Discussion
The authors describe the results of the first step of the validation process for the development of checklists for teaching and assessing FC (Tables 1 and 2). A modified Delphi method involving a panel of 7 experts was used to develop these checklists. The advantage of the Delphi method is that it involves an iterative process of review by experts that is designed to achieve consensus. 16 The experts are blinded to the identity of other experts to prevent any 1 individual from influencing the group’s decisions about items. 17 Previously published checklists identified by the authors did not use the Delphi method.
Expert review of the male FC checklist resulted in high agreement, and each item on the checklist met the inclusion requirement. Based on experts’ comments in Delphi round 1, changes were made to 8 items. During round 2, the experts agreed with the checklist.
Expert review of the female FC checklist resulted in high agreement, and each item on the checklist met the inclusion requirement. Based on experts’ comments in Delphi round 1, changes were made to 8 items. During round 2, the experts agreed with the checklist.
For both male and female FC, experts commented that explaining the procedure to a patient may not be possible in some clinical scenarios. Experts emphasized the need to maintain sterility throughout the procedure. For male catheterization, it was noted that if resistance is met while inserting the catheter, one must not force the catheter. There are a number of methods to pass a catheter through a constricted urethra, such as using a Coudee catheter or, paradoxically, using a larger caliber catheter (22-24 French). For difficult insertions, an urologist should be consulted. For female catheterization, there are several ways to increase accessibility of the urethra, including placing the patient in the dorsal lithotomy position.
Limitations of the study include the possibility of expert bias. However, as indicated previously, the experts were drawn from 2 institutions and 5 specialties to minimize institutional and specialty bias. In addition, the number of experts involved is similar to that used in a previous study by Huang et al 18 in their validation of a central venous catheter insertion checklist. The institutions in this study are located in the same geographic region; therefore, biases inherent in practice patterns of this region may have influenced the results.
Conclusion
The authors describe the results of the first step of the validation process for the development of checklists for teaching and assessing male and female FC. A modified Delphi method involving a panel of 7 experts was used to create checklists for these procedural skills. Using validated checklists could lead to fewer complications, decreased cost, and an overall increase in the quality of health care provided. Future studies should further validate these FC checklists by implementing and studying them in the simulation and clinical environments.
Footnotes
Acknowledgements
Special thanks to our experts: Kevin Geffe, DO, Chief Surgical Resident, Department of General Surgery, Christiana Care Health System, Newark, Delaware; Carey Heck, MSN, CCRN, CNRN, Clinical Specialist, Neuroscience Critical Care, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania; Bridget Kelly, RN-BC, MSN, Clinical Nurse Specialist, Department of Transplant and Urology Surgery, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania; Costas Lallas, MD, Jefferson University Physician and Associate Professor of Urology, Thomas Jefferson University, Philadelphia, Pennsylvania; Sidney John Swanson, III, MD, Chief, Kidney Transplant Program, Christiana Care Health System, Newark, Delaware; Vanessa Talbott, MD, fourth-year surgery resident, Thomas Jefferson University, Philadelphia, Pennsylvania; Pamela Woods, RN, ACNS-BC, CEN, Trauma Coordinator, Christiana Care Health System, Newark, Delaware. The authors acknowledge Dolores Ann Moran and Janice Evans, each a medical library assistant II, Lewis B. Flinn Medical Library, Christiana Care Health System, for assistance in locating articles.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: Partial funding for research assistants was provided by Christiana Care Health System, Newark, Delaware, through a resident research grant.