
Abstract
There is limited information about how to transform primary care practices into medical homes. The research team surveyed leaders of the first 132 primary care practices in Minnesota to achieve medical home certification. These surveys measured priority for transformation, the presence of medical home practice systems, and the presence of various organizational factors and change strategies. Survey response rates were 98% for the Change Process Capability Questionnaire survey and 92% for the Physician Practice Connections survey. They showed that 80% to 100% of these certified clinics had 15 of the 18 organizational factors important for improving care processes and that 60% to 90% had successfully used 16 improvement strategies. Higher priority for this change (P = .001) and use of more strategies (P = .05) were predictive of greater change in systems. Clinics contemplating medical home transformation should consider the factors and strategies identified here and should be sure that such a change is indeed a high priority for them.
Keywords
If health care reform is to successfully move American medicine closer to the Triple Aim of improvement in health, patient experience, and affordability, both the payment system and the care delivery system will need to be transformed.1,2 Great hope and some evidence suggests that the changes embodied in the medical home concept will be critical to preparing primary care to serve its important role in such a transformed care system.3-5 Thus, there are now many initiatives and demonstration projects aimed at incenting and achieving transformation of traditional primary care practices into patient-centered medical homes (PCMHs). 6 Multiple recognition, certification, and identification mechanisms have been established, although NCQA (National Committee for Quality Assurance) recognition is most widely used, and Hollingsworth et al estimate that less than half of the existing primary care practices could be considered medical homes on the basis of those criteria. 7 Another force encouraging this change is the Patient-Centered Primary Care Coalition, a national organization with many health care, professional association, and large business members (http://www.pcpcc.net).8,9
This combination of national attention and local initiatives has created high awareness of the medical home concept among primary care physicians. However, without payment reform, it seems unlikely that many of the small independent practices that still constitute the great majority of primary care practices in the United States will be able to implement and sustain the practice systems needed to function as medical homes.10-12 Other restraints on this transformation are the lack of a common definition or measure of PCMH functions, the culture and resources of most independent practices, and knowledge about which strategies and changes are most important.
In 2010, Minnesota established standards and a process for certification of primary care practices as medical homes (here called health care homes) as well as a payment system change, all intended to address the barriers to transformation described. As of May 2013, about 242 (33%) of the 728 primary care practices in Minnesota have been certified. The research team conducted a study aimed at learning from the first clinics achieving certification which organizational factors and systems were most important and which change strategies they had used in their transformation process.
Methods
The state standards required for clinics to become certified were focused on 5 areas: access, a patient registry, care coordination, care plans, and quality improvement methods. The certification process involved an application and self-assessment, an on-site visit with chart audits and interviews with both staff and patients, and review by a multistakeholder advisory committee. The research team obtained agreement to cooperate with this study from leaders of all 132 clinics that had been certified as of October 2011. However, parts of this report are limited to the 120 certified clinics that provide care to adults, because those are the ones for which the team has performance measures for adults with diabetes or vascular disease.
Descriptive information was collected about these clinics from a survey constructed to identify their size, relationships, and patient population. The research team also obtained a survey (and has reported the results previously) to measure the presence of practice systems for medical homes that is the research version of the original Physician Practice Connections–Patient-Centered Medical Home survey used by NCQA to recognize practices as medical homes. 13 This instrument (the Physician Practice Connections–Readiness Survey [PPC-RS]) is completed by the medical leader of each clinic for both systems present at the current time and those present 3 years earlier, each on a scale of 0% to 100%, where 100% means that all measured systems are present and working well. The results from this instrument have been reported previously for the subset of clinics that serve adults. 13
The research team also obtained standardized performance rates for each study clinic from Minnesota Community Measurement for composite all-or-none measures for diabetes and vascular care. Such measures have been recommended by Berwick and Nolan and are reported yearly on a public Web site—www.mnhealthscores.org. For a patient with diabetes to be scored as positive on this measure, the HbA1c must be ≤7%, the blood pressure must be ≤130/80, the low-density lipoprotein must be ≤100, and the patient must be on aspirin and be a nonsmoker. The criteria for each patient with vascular disease are the same except for not including an HbA1c value. A single criterion not met results in that patient counting only in the denominator for these measures.
Finally, the research team also surveyed the clinic manager of each study clinic to measure its readiness to improve care using the Change Process Capability Questionnaire (CPCQ). 14 This instrument was created from items identified and prioritized by experienced clinic implementers in an iterative modified Delphi process. 15 The CPCQ has 34 items and 2 scales. 16 The first scale consists of 18 items that assess organizational factors and are rated on a 5-point scale from strongly agree (+2) to strongly disagree (−2). These 18 items were rated by these implementation leaders as having the most effect on the ability to implement guidelines out of 87 identified from the literature or by this group. The organizational factors are scored as the mean response to all items, with higher values representing more favorable factors for successful change. The second component assesses strategies that have been used to implement improved depression care, and contains 16 items answered as Yes, worked well (scored 1); Yes, but did not work well (scored 0.5); or No, not used (scored 0). These strategies were rated by the implementer panel as the most effective out of 25 similarly identified strategies. As with the PPC-RS, the strategies scale was scored as the proportion of all items present. The CPCQ also included a single question asking about the priority that clinic leadership attached to this specific medical home improvement effort relative to all other clinic initiatives on a scale of 1 to 10.
Measures of central tendency and dispersion were calculated to describe clinic characteristics in a distribution-appropriate manner. Clinic-based PPC-RS and CPCQ scale scores were summarized as mean and standard deviation; changes in the PPC-RS score for systems were calculated as the raw difference between current and 3-year previous scores. The significance of change in PPC-RS scores was assessed using paired t tests. Continuous bivariate relationships between clinic characteristics, CPCQ scale scores, PPC-RS scores, and Minnesota Community Measurement outcomes were assessed using Spearman rank correlations. Differences in scores between categorical variables were assessed using one-way analysis of variance and further explored using least-squares means comparisons.
A multivariate linear model was fit to model the 3-year change in PPC experienced by the sample of clinics in relation to the variables that were significant in bivariate analyses. Several variables had to be dichotomized because of their skewed distribution. Complete data with all predictor variables for use in this model was present for 102 of the clinics. Variables included in the model were the following:
Physician makeup: multispecialty versus primary care
Number of primary care physicians at the clinic
Number of practice sites (clinics) in the medical group: 0-5 versus 6 or more
Percent of patients with commercial health insurance
Priority score for transformation: 6-10 versus 1-5
Organizational factors CPCQ score
Strategies CPCQ score: 0.6-1 versus <0.6
This project was reviewed, approved, and monitored by the HealthPartners institutional review board.
Results
Of the 132 certified health care home clinics in the study, 131 clinic managers were sent CPCQ surveys (one was a 1-physician practice with no employees), and completed CPCQ surveys were obtained from 129 (98.5%). The PPC-RS survey was completed by 121 (91.7%) physician leaders. For clinics serving adults, 117 out of 119 (98.3%) CPCQ surveys were returned, but only 108 (90.8%) of these also had completed PPC-RS practice systems questionnaires. Performance measure rates were available for 101/108 adult clinics for diabetes and 98/108 for vascular disease.
Table 1 provides a description of the characteristics of the 129 clinics with CPCQ results. Fully 70% of the clinics were part of large organizations, so 55% contained other specialties besides those in primary care. The average number of primary care physicians in a clinic was 13.6 ± 18.0 and nearly all had both fully functional electronic medical records and at least one nurse practitioner or physician assistant.
Characteristics of Certified Health Care Homes (n=129).
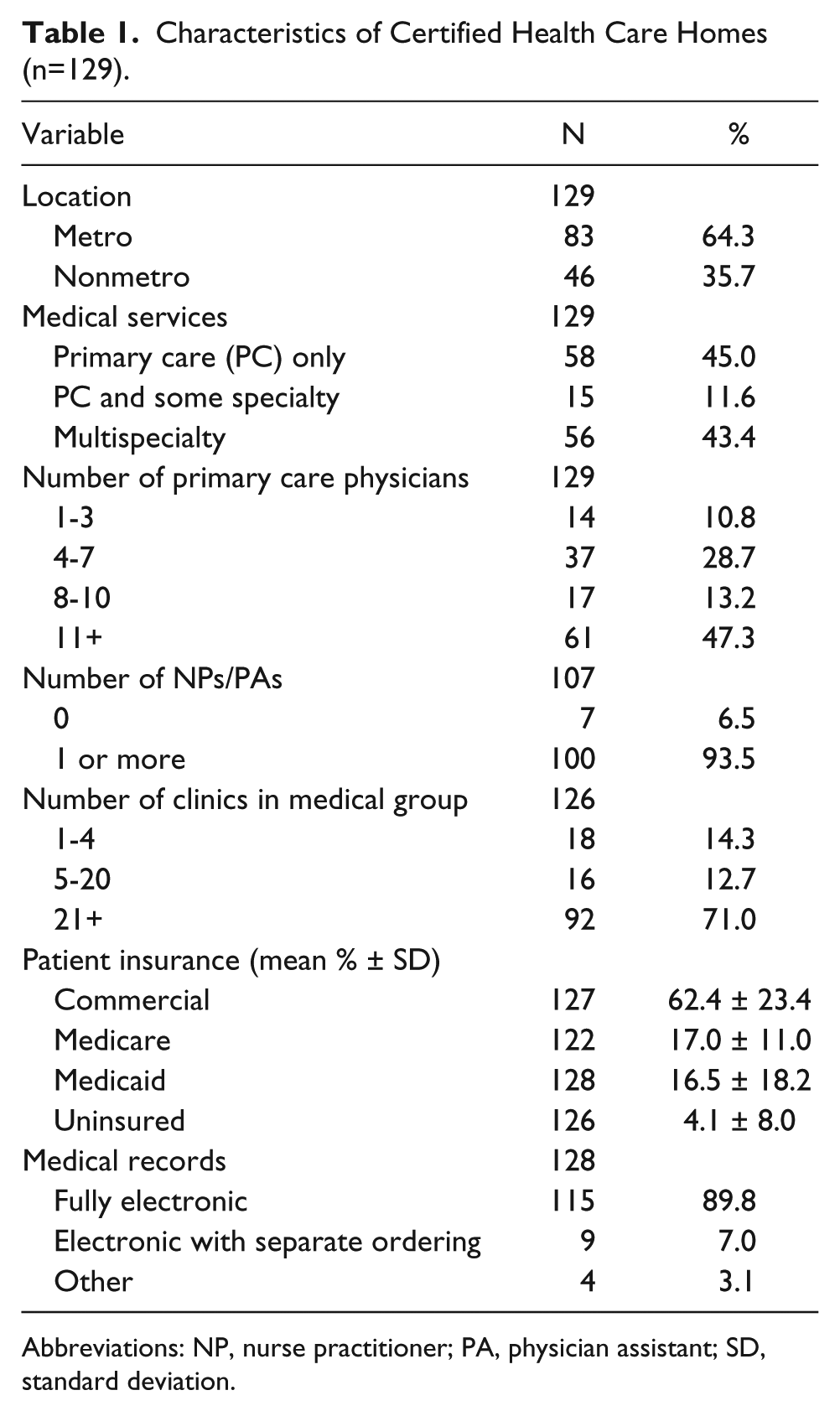
Abbreviations: NP, nurse practitioner; PA, physician assistant; SD, standard deviation.
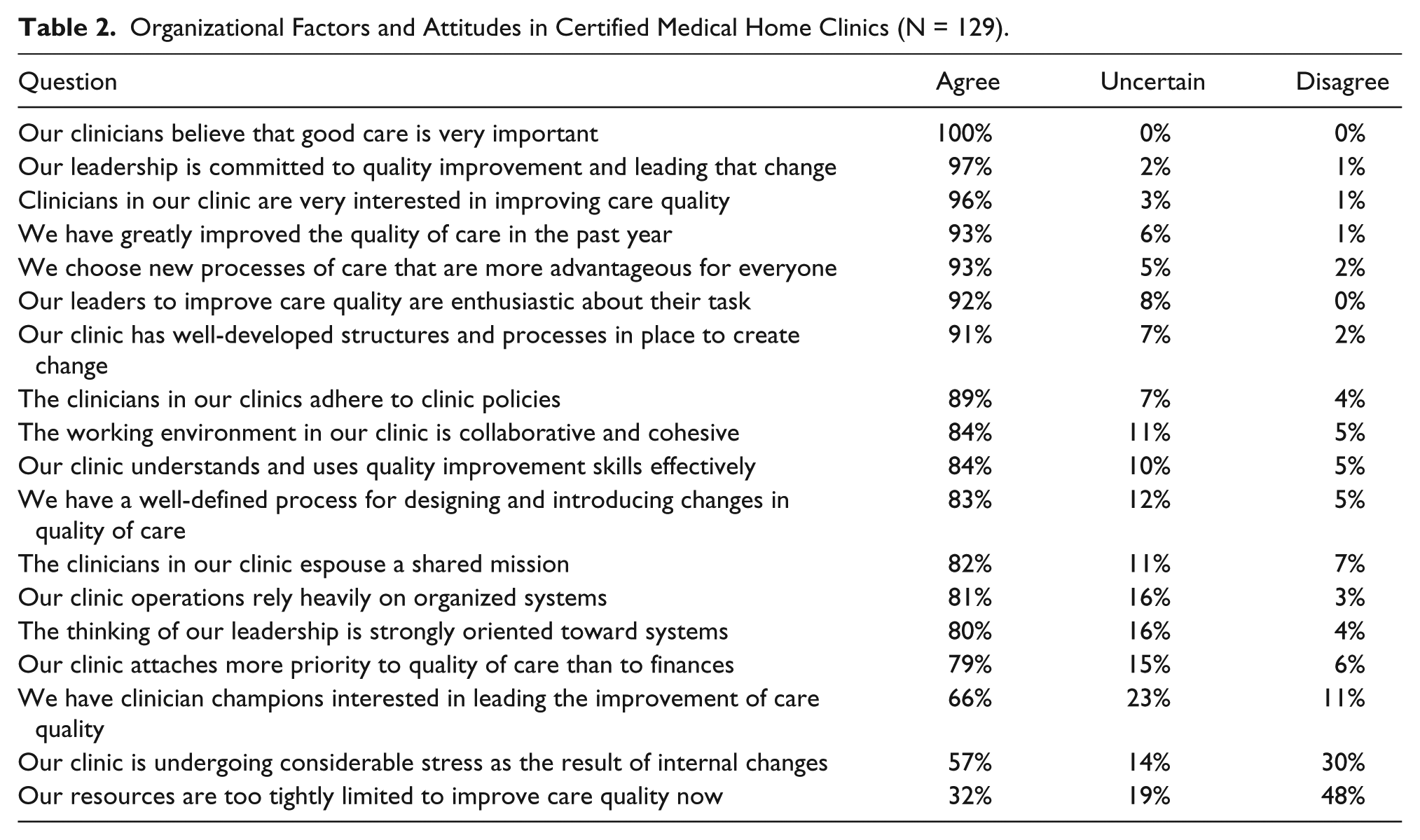
Table 2 shows the proportion of the 129 clinic managers reporting the presence of each of the organizational factors and attitudes related to the ability to improve from the CPCQ survey. All but 3 of the 18 items in this scale were reportedly present in at least 79% of the certified clinics. The 3 items with lower frequencies were having clinician champions for improving quality, adequate resources, and lack of considerable stress. With a potential range from −2 to +2, the mean clinic score for organizational factors among these clinics was +1.11 with a SD of 0.43.
Organizational Factors and Attitudes in Certified Medical Home Clinics (N = 129).
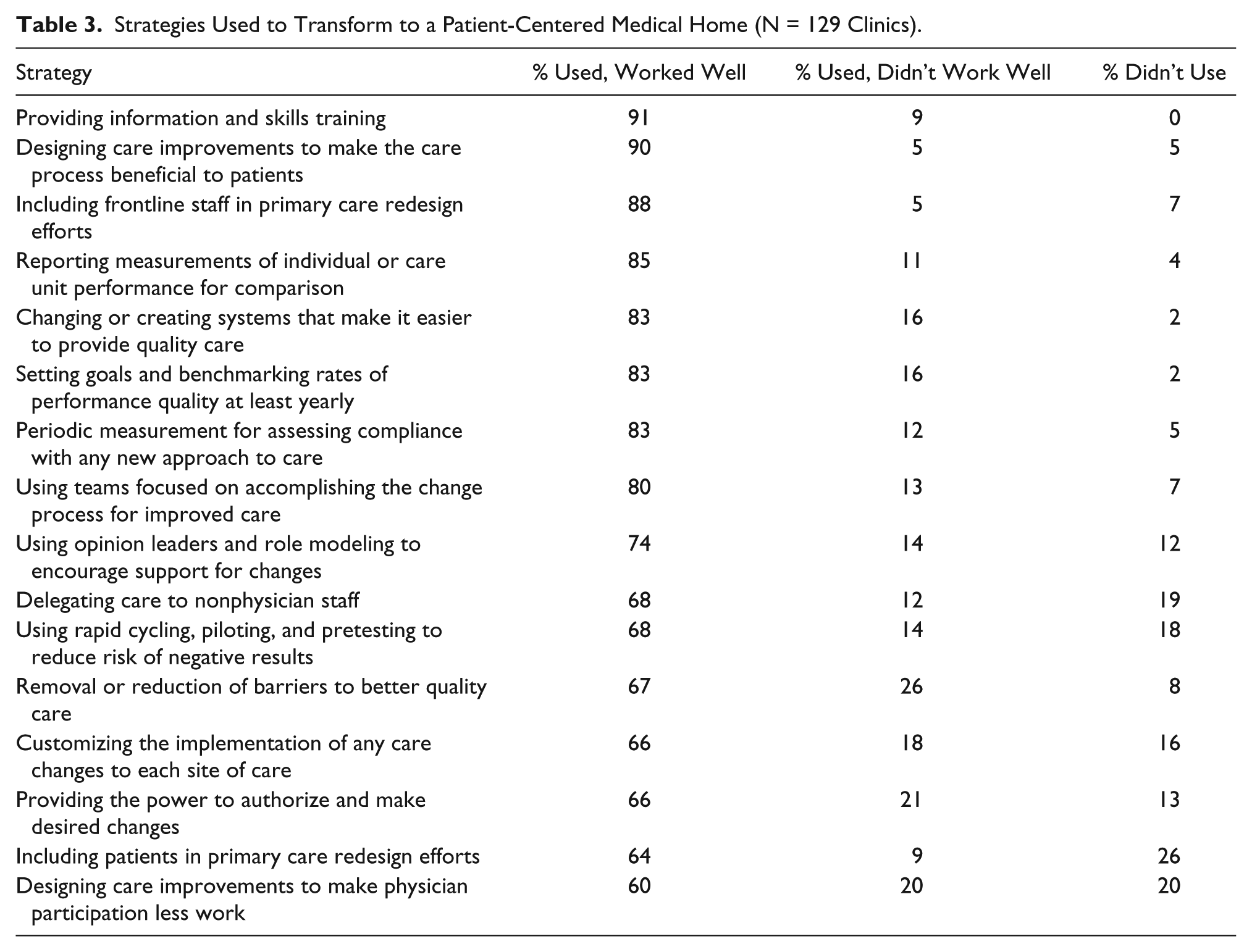
In Table 3, 60% to 91% of these clinic managers reported that their clinic had used each of 16 important strategies successfully for transformation to medical homes and another 5% to 26% reported using them but without success. The mean clinic score for strategies used in transformation was 84.2 ± 14.5%, because half credit is given for trying a strategy even though it did not work well. There were no significant differences between pediatrics and family/internal medicine clinics in either organizational factors or strategies scores.
Strategies Used to Transform to a Patient-Centered Medical Home (N = 129 Clinics).
Finally, the mean PPC-RS (systems) score for these clinics rose from 38.5 ± 16% 3 years ago to 66.4 ± 15%, a relative increase in systems of 72% and an absolute increase of 28.0%. The 12 pediatrics clinics had scores 3 years ago that were similar to family/internal medicine clinics, but their increase was less (18.0% vs 29.1%, P = .005). The practice systems with both the greatest improvement and the strongest association with higher performance measures for diabetes and cardiovascular outcomes were the following:
Reminders for clinicians during care about services needed for chronic conditions
Registries for tracking care for patients with chronic conditions
Designated primary care teams that collaborate in the care of a defined group of patients
Routine use of secure e-mail to support self-management for patients and their families
Routine exchange of data with patients with access to their own electronic health record
A systematic process to screen patients for dementia and depression
In bivariate analyses, urban/rural location and number of primary care physicians or nurse practitioners had no relation to either component of the CPCQ, but if the clinic was limited to primary care clinicians, there was a slightly higher score for organizational factors (1.2 vs 1.0, P = .02). Clinics that were part of medical groups with more than 5 clinic sites had higher scores for both organizational factors (1.2 vs 0.8, P = .001) and strategies (4.3 vs 3.8, P ≤ .0001). Clinics that had a larger proportion of patients with commercial insurance and a correspondingly smaller proportion of patients with Medicare or Medicaid also were more likely to use more change strategies (Spearman correlations were +0.32, −0.27, and −0.26, respectively, P = .0003, .002, and .003). Finally, the few clinics without electronic medical records had much lower CPCQ factors and strategies scores than those with them.
The number of strategies used was significantly correlated with the PPC-RS change in practice systems (ie, extent of transformation over the past 3 years) at 0.21 (P = .03), but not with the final score on current systems in place (P = .23). In contrast, the clinic’s priority for medical home transformation was significantly correlated with both organizational factors and strategies on the CPCQ as well as the change in systems over the past 3 years (0.2-0.3, P ≤ .05).
Although the CPCQ strategies score among the 120 adult clinics was correlated with change in quality outcomes performance for cardiovascular disease (0.24, P = .02), it was not for diabetes (0.17, P = .08). Both the change in systems scores over 3 years and the current level of systems were correlated with change in cardiovascular disease outcome performance at the level of 0.30 and 0.36 (P ≤ .001).
Accounting for all other variables in the multivariate model demonstrated in Table 4, on average, clinics with only primary care clinicians experienced an absolute 7.3% greater increase in PPC-RS systems over 3 years than did those with any specialists. Similarly, those clinics in small medical groups (0-5 sites) had an 8.8% greater increase than those in larger groups and there was a 1.1% increase in systems for every 5% increase in the percent of clinic patients on commercial insurance. The greatest changes, however, were associated with a clinic’s priority for medical home changes and the number of strategies used to implement those changes. A priority score over 5 on a 10-point scale and use of more than 60% of surveyed strategies were both associated with increases in systems changes. The CPCQ organizational factors score was inversely related to systems change, however.
Multivariate Relationship a Between Change in Systems and Other Variables (N = 102).
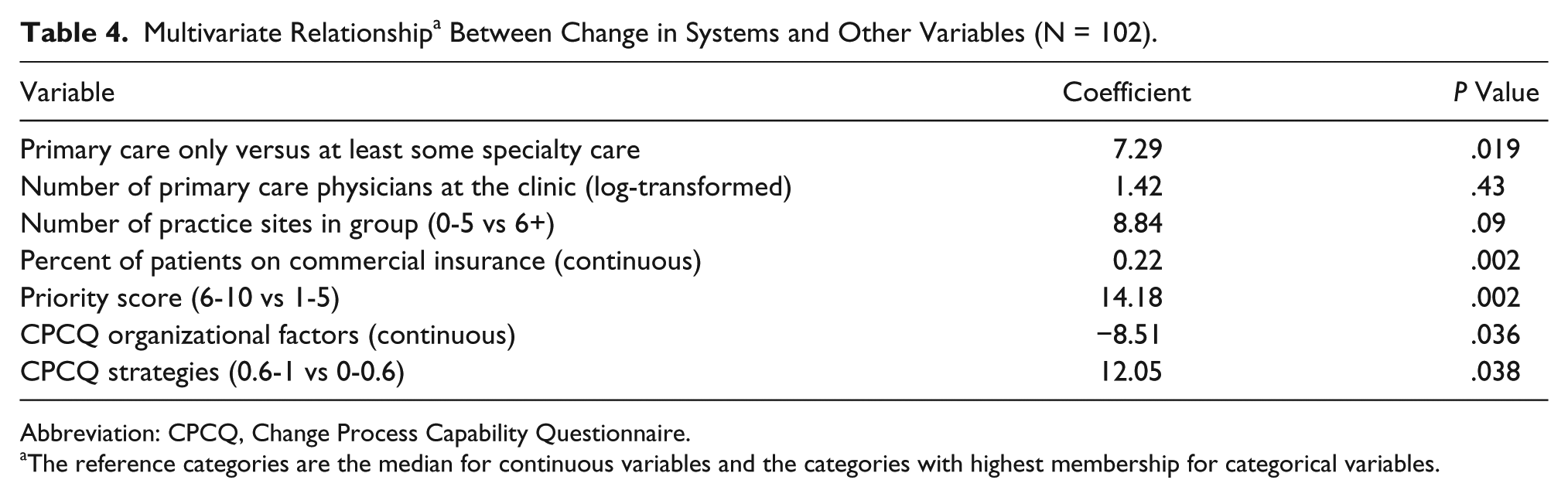
Abbreviation: CPCQ, Change Process Capability Questionnaire.
The reference categories are the median for continuous variables and the categories with highest membership for categorical variables.
Discussion
The great majority of these early-adopting primary care clinics that had been certified as health care homes reported having nearly all of the organizational factors on the CPCQ believed to be important for successful implementation. Most of them also reported having used nearly all of the change strategies recommended by experienced implementers, mostly successfully. The 7 strategies that were used less frequently by these early-adopting clinics also tended to be used less successfully, so perhaps those working on or facilitating medical home transformation should focus more attention on making better use of them. Although greater use of these strategies was associated with better outcomes for their patients with cardiovascular disease (but not diabetes), the research team has shown previously that these outcomes measures are slow to change (and there was little overall increase in mean performance scores for either condition during these 3 years). 13 Therefore, a more proximate measure of improvement in medical home function may be a clinic’s increase in medical home practice systems to provide more consistent care to its patients with these conditions. Targeting especially the systems with the greatest change and the greatest relation to performance and monitoring change in systems scores may provide both more focus and a more immediate way to know whether transformation is going well.
In that regard, these data show that only a few practice characteristics predict change in systems (primary care only, part of larger systems, and fewer Medicare or Medicaid patients), and those characteristics are not easily changeable. On the other hand, the largest systems changes are associated with clinics that had a high priority for making medical home changes and those that used more of the identified strategies for doing so. Those are factors that are almost completely under the control of most clinics. The one puzzling finding was that an increase in the CPCQ organizational factors score was associated with a decrease in the amount of systems change. Possibly that is because clinics with more favorable organizational factors already had more systems 3 years earlier, so they had less room to improve.
The extensive recent literature on the PCMH has had relatively little to say about the transformation process. Most of it consists of commentaries, descriptions, and recent studies of the impact of PCMH on quality, cost, and patient experience. As summarized in recent systematic literature reviews by Jackson et al, Peikes et al, and Hoff et al, the PCMH is a promising concept with as yet inconclusive or insufficient evidence about its impacts.3-5,17 While we await better evidence, so many practices are engaged in transformation efforts with so little guidance on where to focus and how to change that the Agency for Healthcare Research and Quality funded 14 grantees in 2010 to study the transformation process as well as associated outcomes. McNellis et al summarized the key lessons learned from these studies about the transformation process. 18 Those key lessons were the following:
A strong foundation is needed for successful redesign
The process of transformation can be a long and difficult journey
[Successful] approaches to transformation vary
Visionary leadership and a supportive culture ease the way for change
Contextual factors are inextricably linked to outcome
Further details about these important general themes are available in a special issue of Annals of Family Medicine, which was devoted entirely to reports from and about these 14 projects. 19 However, it is not clear that transforming a medical practice to a PCMH is fundamentally different from any other medical practice implementation, except perhaps in scope. Implementation researchers are likely to agree with the importance of the aforementioned general themes, but they also have much to say about practice implementation. Lee et al recently published a systematic review of empirical research on organizational transformation in health care and other industries. 20 Unfortunately, as concluded in this review, “Available research documents the multiplicity of factors affecting change and the complexity of their interaction, but less information is available about the processes of transformational change than about its antecedents and consequences.” The other problem with the work of implementation scientists was noted by Knapp and Anaya: “Principles of implementation science provide key theories to guide these [QI] processes, however, such theories tend to be highly technical in nature and do not provide pragmatic or streamlined approaches to real-world implementation.” 21 The research team hopes that this study’s results overcome some of these problems by focusing on identifying what relatively successful practices have done and the factors and strategies they used to do it.
The main limitation for these findings is the absence of comparable information about noncertified clinics or those that have become certified after these early adopter clinics. The clinical significance of the findings also is limited by the very small changes in performance measures for patients with diabetes or cardiovascular disease, either among certified or uncertified clinics in Minnesota. The mean diabetes all-or-none performance measure with 5 components only increased among certified clinics by an average of 2.4% (from 22.0% to 24.4%) from 2008 to 2010. Similarly, the cardiovascular outcomes measure with 4 components only increased from 37.5% to 41.6% over that time. Thus, there is limited ability to correlate the variables in this analysis with some of the all-important outcomes expected from medical home transformation. Cardiovascular and diabetes measures are difficult to change and have been the main targets for quality improvement in this community for the past 10 years, so all of the easy improvements have already been made for these conditions. Relying on the leadership memory of practice system presence 3 years ago also may be inaccurate, although there is no reason to believe this would selectively affect some clinics. Finally, medical care in Minnesota is different than in many states in that there are very few independent small practices, many physicians are employees, and most clinics have electronic medical records. Also, most of these certified clinics have more experience with quality improvement methodologies than most elsewhere because of their involvement with the Institute for Clinical Systems Improvement, Minnesota’s highly rated quality improvement collaborative.
Nevertheless, this explication of the system changes and the factors and strategies associated with these PCMH clinics should be helpful to primary care clinics everywhere that are interested in transforming themselves, as well as to those who are sponsoring or facilitating medical home changes. The system changes that were associated with higher performance mostly concerned information and communication—reminders for physicians, registries, secure e-mail and Internet access for patients. It also appears that the specific practical aspects of clinic culture and change management that were highlighted by successful leaders of clinic implementation of quality improvements 15 years ago are as relevant for today’s interest in medical home transformation as they were then for implementation of evidence-based guidelines. 16 Physicians working to improve their care and work life would be well advised to focus their change efforts on the systems, factors, and strategies identified here.
Footnotes
Acknowledgements
We are very grateful for the cooperation of the Minnesota Department of Health throughout this study, especially for the opportunity to work together to use the lessons learned from these evaluations with all of the growing number of certified health care homes in Minnesota. We also are grateful for the way in which the leaders of the health care homes cooperated with the data collection for this study, especially those in the 9 clinics that participated in our interviews and clinic advisory board: Essentia Health Duluth Clinic Pediatric Department—Gordon Harvieux, MD; Park Nicollet in St. Louis Park Internal Medicine Department—Kristin Kopski, MD, and Jeanine Rosner, RN; CentraCare Becker Clinic—Paul Spinner, MD; UMP Phalen Village—Angela Smithson, MD, and Mary Beth Collins; Lakewood Health in Staples—John Halfen, MD; Mayo Northwest Clinic in Rochester—Steven Hagedorn, MD; United Hospital District Blue Earth Clinic—Terry Cahill, MD; HealthPartners St. Paul Clinic—Mary Jo Pechacek, RN; Fairview Maple Grove Clinic—Yeng Yang, MD, and Linda Zarns, RN.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality, the funding agency.
Declaration of Conflicting Interests
The authors declared no conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the Agency for Healthcare Research and Quality (Grant No. R18HS019161).