
Abstract
The Harvard Fellowship in Patient Safety and Quality is a 2-year physician-oriented training program with a strong operational orientation, embedding trainees in the quality departments of participating hospitals. It also integrates didactic and experiential learning and offers the option of obtaining a master’s degree in public health. The program focuses on methodologically rigorous improvement and measurement, with an emphasis on the development and implementation of innovative practice. The operational orientation is intended to foster the professional development of future quality and safety leaders. The purpose of this article is to describe the design and development of the fellowship.
Over the past decade, efforts to improve the quality and safety of health care have become an urgent national priority. This endeavor continues to shape clinical practice, health care management, clinical and health services research, education, and policy. In turn, it generates demand for physicians who are prepared both to participate in these activities and to lead them.
Across most medical institutions, physicians who play leadership roles in quality improvement and patient safety have arrived at those positions through a variety of career trajectories, often beginning in research and later transitioning to operational responsibilities. Many developed important skills without the benefit of formal training. Increasingly, however, resident physicians, at the beginning of their careers, are seeking advice about career paths in quality and safety. Unfortunately, there are limited formal opportunities for young physicians to prepare themselves to work in these areas. Although residency and fellowship training must satisfy Accreditation Council for Graduate Medical Education requirements to incorporate quality and safety, 1 residency curricula generally do not provide sufficient training to prepare residents for careers in these fields. As a result, junior clinicians who wish to pursue operational, educational, or research opportunities may be disadvantaged. Concurrently, hospitals and other health employers may find it challenging to identify and recruit health professionals who are adequately prepared to lead organizational initiatives that address quality and patient safety challenges.
A handful of quality and patient safety fellowship programs have been developed nationally to address this need, such as the 2-year VA National Quality Scholars Fellowship 2 and 1-year fellowships such as the American Hospital Association Patient Safety Leadership Fellowship, the Institute for Healthcare Improvement Fellowship, and quality/safety fellowships at individual hospitals (eg, Baystate Medical Center in Massachusetts, Beth Israel Hospital in New York). In addition, several master’s degree programs in quality and safety have emerged (eg, Jefferson School of Population Health, University of Pennsylvania—both in Philadelphia, Pennsylvania).
The Harvard Fellowship in Patient Safety and Quality is a 2-year physician-oriented training program that is based on adult learning models. 3 This fellowship differs from existing initiatives in its strong operational orientation, embedding trainees in the quality departments of participating hospitals. It also integrates didactics and offers the option of obtaining a master’s degree in public health (MPH). It draws on faculty and administrative leaders from across the system of Harvard-affiliated hospitals and is open to physicians from all specialties. The program focuses on methodologically rigorous improvement and measurement, with an emphasis on the development and implementation of innovative practice. This operational orientation is intended to foster the professional development of future quality and safety leaders. The purpose of this article is to describe the design and development of the Harvard Fellowship in Patient Safety and Quality.
Objectives
The primary goal of the Harvard Fellowship in Patient Safety and Quality is to train a cadre of physician scholars who are prepared to lead operational improvement efforts within the Harvard system and across the nation. In addition, the program is designed to create scholars who can rigorously measure quality in clinics and health systems, measure the impact of demonstration studies and intervention trials, and perform effective implementation and dissemination. The fellowship has received seed funding from CRICO (Risk Management Foundation of the Harvard Medical Institutions), the captive malpractice insurer for the Harvard hospitals, with the intention of recruiting 5 fellows per year for 3 cycles. CRICO has a long history of efforts in loss prevention and patient safety to reduce physician risk of malpractice, and has significant expertise in physician education about patient safety and risk management. CRICO has a grant program to fund patient safety projects, and CRICO’s vision in funding this fellowship was to expose clinicians to the nuances between risk, quality, and safety through the lens of malpractice.
Just as the clinic and hospital are laboratories for the practice of clinical medicine, the clinic, hospital, and health system are the laboratory for scientifically based improvement work. And just as mentorship at the bedside is critical to the development of clinical skills, fellows need to learn about the complexities of health care operations and change management via in situ experiences under the mentorship of senior hospital physician-leaders. Contributions from adult learning theory advocate for adult learners to participate in goal-oriented learning, activity-oriented learning, and learning-oriented learning 3 ; the experiential nature of this fellowship combined with rigorous didactics support this rich and effective adult learning process.4,5 At the conclusion of the fellowship, the intent is for fellows to have developed the skills, knowledge, and experience to succeed as clinical and operational leaders in health care.
The main competencies that the fellowship program seeks to cultivate are the following:
understand the scientific basis of quality improvement and patient safety, including the epidemiology and nature of medical error, quality measurement and data analysis, evaluation design, improvement tools and techniques, and best practices;
develop competence in designing, conducting, and evaluating quality improvement projects using rigorous methods, the results of which can be communicated through publication;
learn to facilitate and lead health care professionals in multidisciplinary teams; and
understand and navigate the complex dynamics of hospital/clinical operations.
Operations Projects
Fellows are based in the quality department of one of the Harvard-affiliated teaching hospitals. Each fellow is paired with at least one mentor who is a faculty member with expertise and experience in quality and safety. Each institution’s director/vice president of quality and patient safety (or equivalent title) along with CRICO faculty provide program oversight and assist with developing mentor-mentee relationships and with selecting projects. Project selection is informed by local organizational priorities and projects as well as data from CRICO on high-risk areas at the organization. Mentoring is a critical part of the program. Mentors assist each fellow in career development, with the goal of a career in quality improvement practice as well as hands-on mentoring of specific improvement initiatives. Fellows also participate in a number of hospital quality and safety committees to better understand and participate in local hospital operations. Fellows participate in projects and on committees and task forces that enable them to develop competency in understanding the complexity of health care delivery and how to effect change.
Each fellow is required to participate in and lead a portfolio of improvement efforts. These efforts align with the hospital’s strategic initiatives and allow the fellows to utilize various skills they are developing. Fellows work on a variety of projects in the course of their training. It is important that each individual develop a portfolio of projects for which he or she has assumed significant responsibility and for which he or she can take credit. This can be part of a larger project or a stand-alone effort. Fellows identify at least one project in each year of the fellowship that they will be able to describe as major projects that comprise a key part of their portfolio.
There is a great deal of flexibility in the selection of projects. Fellows and their site directors consider several dimensions in developing their project portfolio (Table 1).
Dimensions for Operations Project Selection.
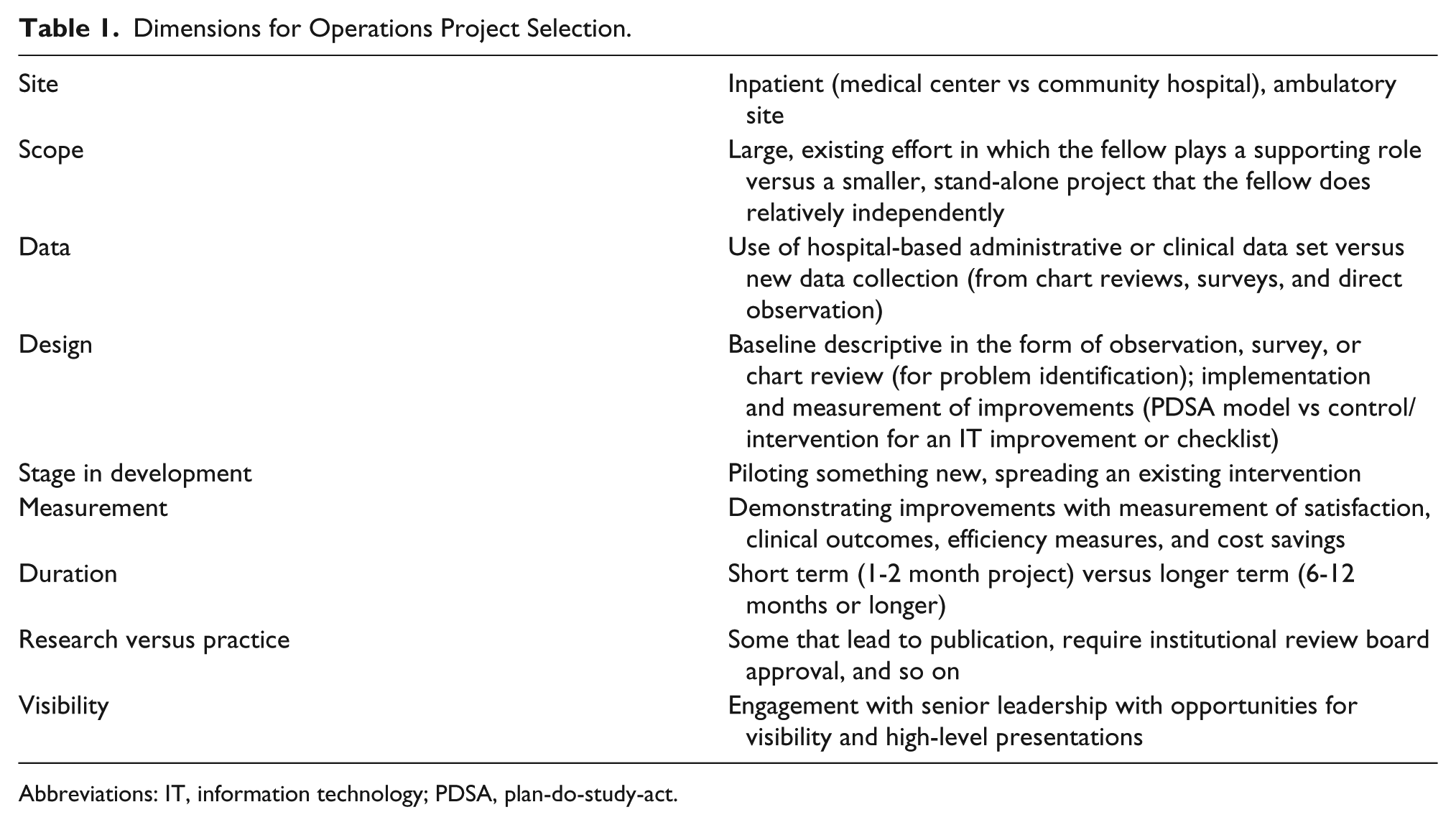
Abbreviations: IT, information technology; PDSA, plan-do-study-act.
Ideally, each project addresses a different quality or patient safety problem (to build the fellow’s breadth of expertise), demonstrates the use of various data analytic tools, and draws on a set of tools relevant to quality improvement and patient safety. Different projects may focus on a single clinical area (eg, surgery, pathology) or practice site (eg, hospital-based, ambulatory), reflecting the fellow’s area of interest and expertise. Examples of projects include an effort to improve preoperative anticoagulation management, improve timing of antibiotic-level blood draws, and redesign the pathology specimen process.
Each fellow is expected, with the help of his/her site director or designee, to identify a major project early in each year of the fellowship. The fellow is expected to present the proposed project to the other fellows and site directors in a structured presentation on a quarterly basis, outlining the major features of the project and inviting feedback and advice. It is expected that most projects will be suitable for and submitted as an abstract at a quality improvement, patient safety, or specialty-oriented professional meeting each year and that most fellows will write up and submit their major projects as academic manuscripts. Although site directors or their designees assume primary responsibility for supporting the fellow’s project and ensuring its success, members of the fellowship faculty are available to provide additional mentorship and to coordinate formal presentations and review final reports.
Curriculum
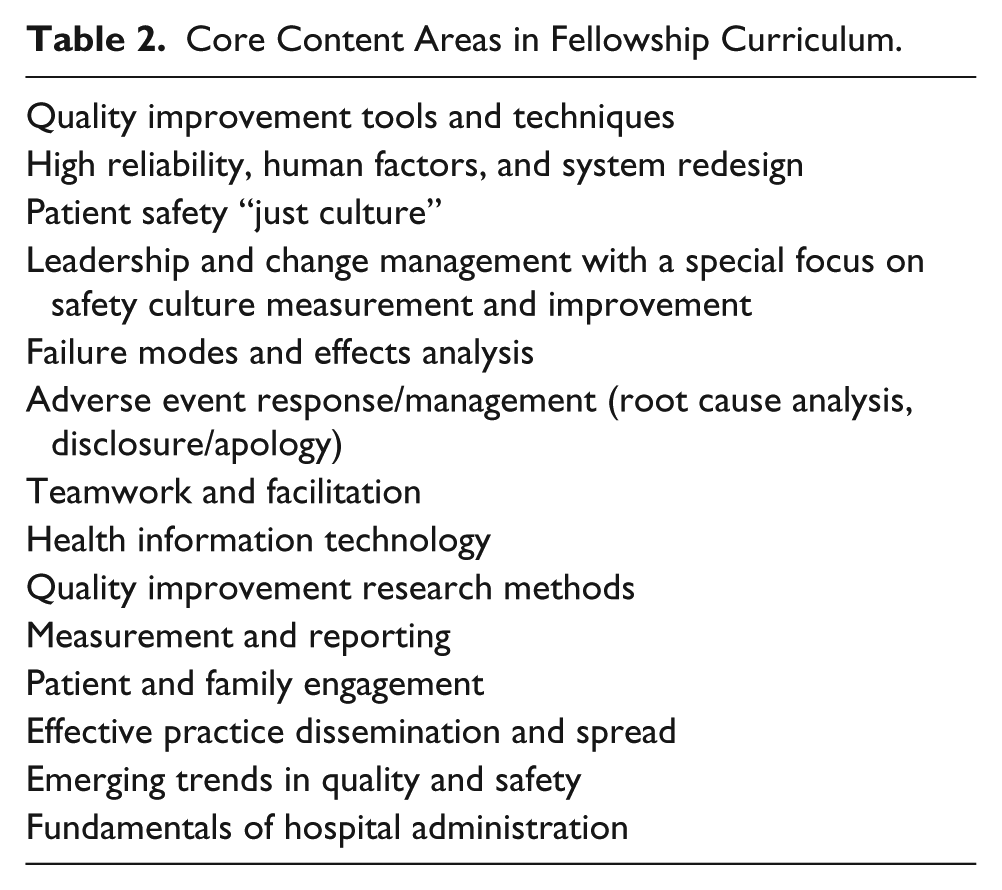
The fellowship curriculum and the process to develop it are described in the companion article, “Creating a Fellowship Curriculum in Patient Safety and Quality.” The broad domains of quality and patient safety were derived based on a consensus among experts, and individual milestones were developed. Table 2 shows the core content areas included in the fellowship’s quality and safety curriculum. A strategy to achieve the milestones was developed as well as tools to evaluate fellows’ achievement and the overall success of the fellowship.
Core Content Areas in Fellowship Curriculum.
Rotations
Although each fellow is based at one of the Harvard teaching hospitals, fellows rotate to the quality program or department of affiliated community hospitals, office practices, and clinics during the course of the program to gain exposure to quality and safety issues in a variety of settings. Rotations include participation in hospital quality and safety committees and shadowing key quality and safety leaders at the organization.
Fellows are required to rotate to at least 2 different sites—1 academic medical center and 1 community hospital—away from their home site. In addition, elective rotation opportunities based on fellows’ interests are available at various sites (eg, the Harvard Simulation Center, international locations, National Patient Safety Foundation). Fellows also are funded to attend a national quality/safety meeting each year.
Clinical Time
To maintain their clinical skills and to have insight into practical health care operations, fellows are encouraged, but not required, to maintain a small clinical practice equivalent to 10% to 20% effort. They are expected to dedicate at least 80% of their time to fellowship activities.
Applicants
Applicants are generally residents or fellows in training, though midcareer professionals also have participated. In the fellowship’s first year (2012-2013), 4 fellows were selected from diverse backgrounds, including pediatric endocrinology (fellow), pediatric rheumatology (fellow), pathology (junior faculty), and anesthesiology (midcareer). In the second cycle (2013-2014), 6 fellows were selected, with backgrounds that included general surgery (resident), nephrology (fellow), infectious disease (fellow), and general pediatrics hospitalist (junior faculty) as well as 2 general internists (junior faculty).
Evaluation
Evaluation of fellows is based on their performance relative to the aforementioned competencies as well as other aspects of professionalism and character that are integral to a successful career in quality and safety. Fellows receive regular feedback from their site program director on a quarterly basis. Formal written reviews occur at the end of 6 and 12 months during each year of the fellowship and are collected and assessed centrally. Career counseling and mentoring occurs on a continual basis during regular meetings between the fellow and site director and between the fellow and other faculty members.
Fellows’ feedback about the fellowship experience is elicited by the fellowship director during semiannual meetings. They also complete evaluations of the curriculum after each lecture and provide a formal written evaluation of the fellowship faculty and overall fellowship experience semiannually. Fellowship faculty meet monthly to review evaluations and discuss the status and future direction of the fellowship.
Early findings from the first-year class evaluations have consistently shown ratings of excellent on a 4-point scale for both the operations and didactic components of the fellowship. Fellows strongly value both the MPH and the fellowship-specific curriculum. Challenges do exist with finding the right time balance between the didactics, clinical work, and operational work, which the site directors are constantly evaluating. In addition, rotations can be challenging because fellows often are still working on projects at their home site during the rotation. However, based on strong positive feedback, there have been no major revisions to the structure of the fellowship after the first 2 years. The site directors will be reevaluating the curriculum to identify new topics or changes in an ongoing way.
The first graduating class of fellows was encouraged to take the exam to become Certified Professionals in Patient Safety (sponsored by the Certification Board for Professionals in Patient Safety), which is an evidence-based examination that provides candidates with a process by which they can demonstrate their competency in patient safety science and application. All 4 fellows passed the exam, validating the quality of the patient safety curriculum content and the level of competency achieved by the fellows.
A significant metric of success is the job placement of fellowship graduates. All 4 graduates of the first cycle of fellows have gone on to enter jobs with significant leadership roles in quality and safety (and dedicated time for quality and safety), which has been a very positive indication of the value of the fellowship.
Faculty
Each Harvard hospital has local, national, and international leaders in the field of quality and safety. This offers considerable depth with respect to content expertise. Faculty members meet regularly to share experiences, address challenges, and plan future aspects of the program. There is a central fellowship director, and each site has a local site director with senior operational responsibility for quality and safety.
Advisory Board
An advisory committee was created to meet every 12 to 18 months to provide guidance to fellowship leadership regarding the content, format, and organization of the fellowship itself; selection of fellows; curriculum design; preparation of graduates for professional positions; and future funding. The committee consists of national leaders in quality and safety from within and outside of the Harvard system, recent junior faculty with careers in quality/safety, medical school leadership, curriculum experts, and directors of other similar fellowship programs.
Challenges/Future Improvements
The fellowship faces several challenges. First, the program needs to identify long-term sustainable funding once the CRICO grant funding has ended. It is showing significant benefit to the participating hospitals, with fellows working on projects that often would have been left undone. Therefore, long-term options might include additional CRICO or hospital funding. Second, the program is composed primarily of physicians still in training or in early career. Potential modifications to facilitate participation of midcareer physicians (eg, an executive education version) are being discussed. Finally, the didactic program consumes significant faculty time; ways to consolidate certain aspects of the curriculum with MPH courses are a future possibility.
Other improvements to the program include ensuring more networking time between different classes of fellows, streamlining didactic sessions, and adding in new topics, such as how to conduct a job search or create a quality portfolio on a résumé, interviewing techniques (for when the fellows need to hire new employees in the future), and writing/publishing quality improvement projects. Finally, stronger methods for evaluation of the success of the program are being discussed, such as career trajectories of graduating fellows and success of operational projects (in terms of measurable improvements and published articles).
Summary/Conclusions
The Harvard Fellowship in Patient Safety and Quality is an innovative program to train the next generation of physician operational leaders in quality and safety. Through a rigorous curriculum and a focus on hands-on project design, implementation, and evaluation, we expect the fellows to learn essential skills to advance into quality and safety leadership positions. Further work is under way to make ongoing additions and improvements to the program based on evaluations from fellows and faculty and to evaluate the success of the program and the careers of the fellows who have made such a large commitment to quality and safety.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by a grant from CRICO, Boston, MA.