
Abstract
This project was designed to improve the colposcopy rate in an urban patient population with known abnormal Pap smears within 75 days of the test to rapidly identify and treat premalignant lesions. Using Plan-Do-Study-Act cycles, Lean techniques, and the electronic health record, the authors created a protocol to verify all Pap smears, then created a process whereby a phone-triage team contacted patients with abnormal Pap smears to educate them and schedule colposcopy. As a result, 100% of Pap smears were verified, compared with 95% prior to plan implementation. The mean time from Pap to colposcopy was 38.5 days, with 85% of patients having colposcopy performed after plan implementation, compared with 50% prior—a 70% improvement. If patients with medical contraindications were excluded, the percentage rose to 91%—an 82% improvement. Patient and provider satisfaction improved, staff and provider workload did not increase, and there was the potential for substantial economic savings.
The setting of this performance improvement project was the Department of Obstetrics and Gynecology at Thomas Jefferson University, which serves an urban female population. This project was undertaken after an established patient with vaginal bleeding saw a Thomas Jefferson University physician who, on reviewing the chart, noted that colposcopy was not performed based on the patient’s abnormal Pap smear results from 18 months prior because no one had verified the results or contacted the patient to schedule colposcopy. The patient underwent colposcopy, with biopsies revealing cervical carcinoma in situ; the patient received definitive treatment of a hysterectomy by a gynecological oncologist.
The incidence of cervical cancer has decreased by more than 50% over the past 30 years because of the widespread use of cervical cytology. Currently, approximately 60% of the diagnoses of cervical cancer are a result of women who were never screened (had no Pap smear) or inadequately screened (either the specimen was not satisfactory for evaluation or the patient never returned for follow-up on abnormalities, as in the case of the aforementioned patient). 1 Appropriate follow-up of abnormal Pap smears that show a risk of developing cervical cancer 2 should include colposcopy with directed biopsy to identify those patients with lesions that may progress to cervical cancer. 3
Those patients who lack a regular source of health care and the uninsured are at high risk for developing cervical cancer, presenting a population health challenge. The characteristics of patients who did not follow up for colposcopy included those whose primary language was not English, who were referred from an outside institution, 4 and/or who had long travel times to the physician’s office. 5 Additionally, 15% to 42% of women did not follow up on abnormal Pap smears because of poor social support, fear that the finding was serious, and lack of understanding of their condition. 6 Women with higher degrees of dysplasia were more likely to be compliant with follow-up than those with lesser degrees because of the fear that the more severe the dysplasia, the more likely they would have cervical cancer. 7 Additionally, “compliance” with colposcopy was defined as the patient returning for treatment within 14 months (but longer than 2.5 months because this was the smallest amount of time from Pap smear to verification to colposcopy) of their initial appointment, and noncompliance was defined as no follow-up visit within 2.5 to 14 months from initial Pap smear. 4 Additionally, the American Congress of Obstetricians and Gynecologists has recommended that offices have tracking systems in place to follow up on Pap smear abnormalities. 8
To assess the current state, the authors performed a chart review of Pap smears done in the department from January to March 2013, inclusive, which revealed that only 15 out of 30 patients (50%) with abnormal Pap smears who required colposcopy had had the procedure. The goal of this project was to perform colposcopy within 2.5 months of the initial Pap smear in 100% of patients with known abnormal Pap smears, within 3 months of plan implementation to identify and treat precancerous lesions. The goal of 2.5 months was chosen because it was felt that a tertiary care center should be able to perform colposcopy at the lowest end of the range.
Methods
The authors formed a multidisciplinary team of physicians, nurses, medical assistants (MAs), office managers, and patients who met weekly to evaluate the current state of performance using Lean process mapping and to perform a root cause analysis (RCA) through interviews with providers and patients to determine the causes of poor follow-up. From this information, the workgroup developed a future state process to improve the rate of follow-up for colposcopy and then piloted this process. The group then studied the pilot to determine if any modifications were needed based on feedback from stakeholders and analyzed the results of the revised pilot project.
The current state analysis and the RCA demonstrated 3 reasons for the low colposcopy rate. (1) The abnormal Pap smear result was not verified by the provider because of issues with the electronic health record (EHR). The current state was for the Pap smear result to be filed electronically in the EHR, at which time a reminder was sent to the provider to verify it. Because of interface errors, some results were filed in the patient’s chart, but a reminder was not sent to the provider who, therefore, would be unaware of the abnormal result. As part of the current state, the MAs kept a written logbook of all Pap smears performed on a daily basis. A 4-week review demonstrated that out of 405 Pap smears done over a 4-week period, only 387 had results that were electronically verified by the provider, for a rate of 96%. (2) The providers found it challenging to contact the patients and “too time consuming on the phone” to explain abnormal results and the importance of colposcopy. (3) Patients did not call to schedule an appointment because they were anxious about colposcopy and did not understand its importance. Patients who called were put on hold for a long time, causing them to hang up.
The workgroup decided that because there were 3 equally important system issues that needed to be addressed, they needed to apply the IHI Model for Improvement using Plan-Do-Study-Act (PDSA) cycles. The goal of the initial PDSA would be to ensure that 100% of Pap smears were verified by the provider. The workgroup created the following protocol:
Weekly, the MAs would cross-check the Pap smears performed 3 weeks prior that were recorded in the logbook with the results filed in the EHR to ensure that the Pap smear result was filed and verified by the provider.
If the Pap smear was filed but not verified, the MA would send an electronic reminder to the provider to verify the result. The provider would then make further treatment recommendations.
The workgroup would study the protocol after 4 weeks to determine (1) the amount of time it took the MAs to evaluate the Pap smears, (2) if the added responsibilities had an impact on the workflow of the other MAs, and (3) the rate of verification of all Pap smears after being reviewed by the MA, with a goal of 100% verification.
Once 100% verification was reached, the workgroup applied additional PDSA cycles to the remaining systems issues: challenges in contacting patients and patient reluctance or inability to schedule an appointment. The plan was to transfer responsibility for contacting patients from providers with direct patient care responsibility to other qualified medical professionals, to educate patients about the importance of colposcopy without alarming them, and to create a patient-centered process for scheduling a colposcopy appointment.
To implement the plan, the group created a list within the EHR onto which providers could place the names of patients needing colposcopy and utilized an existing triage team (nurse practitioner [NP] and registered nurse) to answer patient phone calls. The workgroup devised the following protocol:
the provider would place the names of patients with abnormal Pap smears requiring colposcopy on the list;
a triage team member would call the patients to explain the abnormal results and the importance of colposcopy and answer any questions;
this caller would schedule the patient’s colposcopy while they were on the line for the first available appointment with any provider;
the caller would send an electronic reminder to the provider to inform him or her of this scheduled appointment, completing the communication loop;
the caller would create a personal electronic reminder that would be activated the day of the colposcopy appointment to verify that the patient arrived;
after the patient completed the colposcopy, a triage team member would make a notation in the chart; and
if the patient did not keep the colposcopy appointment, the triage team member would call the patient to reschedule; if the patient could not be reached after 3 weekly attempts, the patient would be sent a certified letter to contact the office.
This protocol was piloted with the general gynecology division (8 physicians and 4 NPs). The working group assessed the implemented plan after 4 weeks for the following: (1) compliance of providers placing names of patients with abnormal Pap smears on the list, with the goal being 100% for each provider; (2) the increase in the workload of the triage team; (3) patient complaints because their provider did not explain the results; and (4) provider assessment as to whether the new protocol saved them time.
After 12 weeks, the workgroup studied the plan for the aforementioned items as well as the elapsed time from performing the Pap smear to the colposcopy appointment, the number of patients who had colposcopy performed at the first appointment scheduled and the number who rescheduled, the reasons why patients did not keep their appointments or rescheduled, and the percentage of patients with low- and high-grade lesions who kept their appointments.
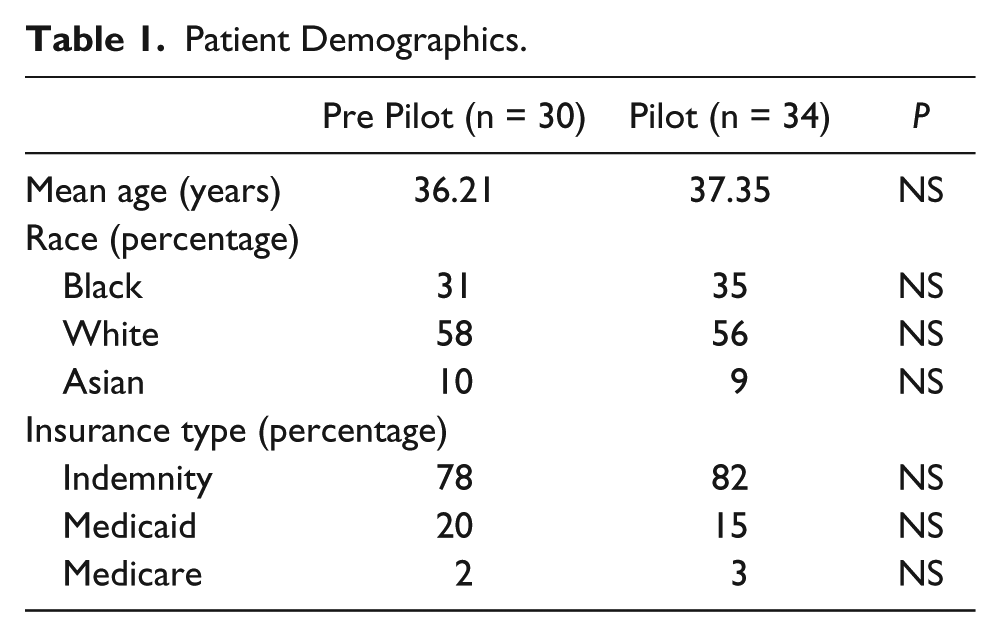
Patient demographics, including age, race, and insurance status were analyzed in pre-pilot and post-pilot groups. SPSS Statistics 22.0 software (IBM Corporation, Armonk, New York) was used to analyze the data, using the χ2 test for categorical data and the Student t test for numerical data.
Results
In all, 34 patients needing colposcopy were identified in the pilot period of November 17, 2013, to February 18, 2014. They were compared with the historical control group of 30 patients in the original chart review. There was no significant difference in age, race, or type of insurance between the 2 groups (Table 1). The majority of patients in both groups were white and had indemnity insurance.
Patient Demographics.
After 4 weeks of having the MAs check the logbook, the working group found that the time it took to verify 1 week of Pap smears averaged 45 minutes and that all unverified Pap smears were sent to the provider, resulting in 100% verification.
After 2 days of implementing the pilot project, the workgroup discovered that neither member of the triage team was trained to schedule appointments. The workgroup reassessed the plan and modified the protocol so that there would be 2 designated call center personnel to whom the triage team member would transfer the patient call. The designated call center personnel would schedule the appointment while the patient was still on the line to ensure correct appointment scheduling because the call center personnel were familiar with the providers’ scheduling idiosyncrasies.
After 4 weeks of the revised protocol, the workgroup found that:
six of 8 physicians and 4 nurse practitioners (83%) were 100% compliant with the protocol; 2 physicians were 92% and 95% compliant. These 2 physicians explained that the reason for less than 100% compliance was that they “forgot to adhere to the protocol”; future patients’ names with abnormal Pap smears were sent correctly to the team, and the physicians re-sent the names of patients they had missed to the triage team for colposcopy;
the triage team members did not find that the work detracted from their other responsibilities; they encountered no resistance from patients to whom they were explaining the abnormal results;
there was no insistence by patients to speak with the provider who performed the Pap smear;
providers found that they did save time by not having to call patients with results;
providers found that although the patients were coming in quickly for colposcopy, they were not seeing their own patients, and appointments took longer, taking them away from other duties.
To address provider dissatisfaction with not seeing their own patients, the workgroup changed the protocol and instructed the call center personnel to ensure that attempts were made to place patients on the schedule of the provider who performed the Pap smear.
After 12 weeks, 29 of 34 patients (85%) had colposcopy performed compared with 15 of 30 patients (50%) in the original chart review—a 70% improvement. Of the 34 patients who had abnormal Pap smears, 9 (26%) had high-grade lesions, and all had colposcopy within 2.5 months; 25 (74%) had low-grade lesions, and 20 (80%) of these patients completed the appointment in 2.5 months. Of the 5 patients with low-grade lesions who did not have colposcopy, 2 were 8 weeks pregnant, and the plan was to perform colposcopy after their delivery; 2 patients were scheduled to have colposcopy after the close of data collection, and 1 patient refused to come in after phone contact and registered letters. If the patients who were pregnant and had the colposcopy deferred for medical indications were excluded, the percentage of patients having the procedure rose to 91%, which was an 82% improvement from pre-project levels. Only 3 (9%) patients did not arrive within 2.5 months. Of the 34 patients, 11 (32%) did not keep their original appointment because of inclement weather and not because of inability to schedule an appointment or anxiety about the procedure; all 11 were rescheduled, and 9 of the 11 arrived after being rescheduled once. Two patients were rescheduled twice because of inclement weather; their appointments would occur after the close of data collection. The mean number of days from Pap smear to colposcopy was 38.5, with a range of 11 to 66 days (Figure 1).
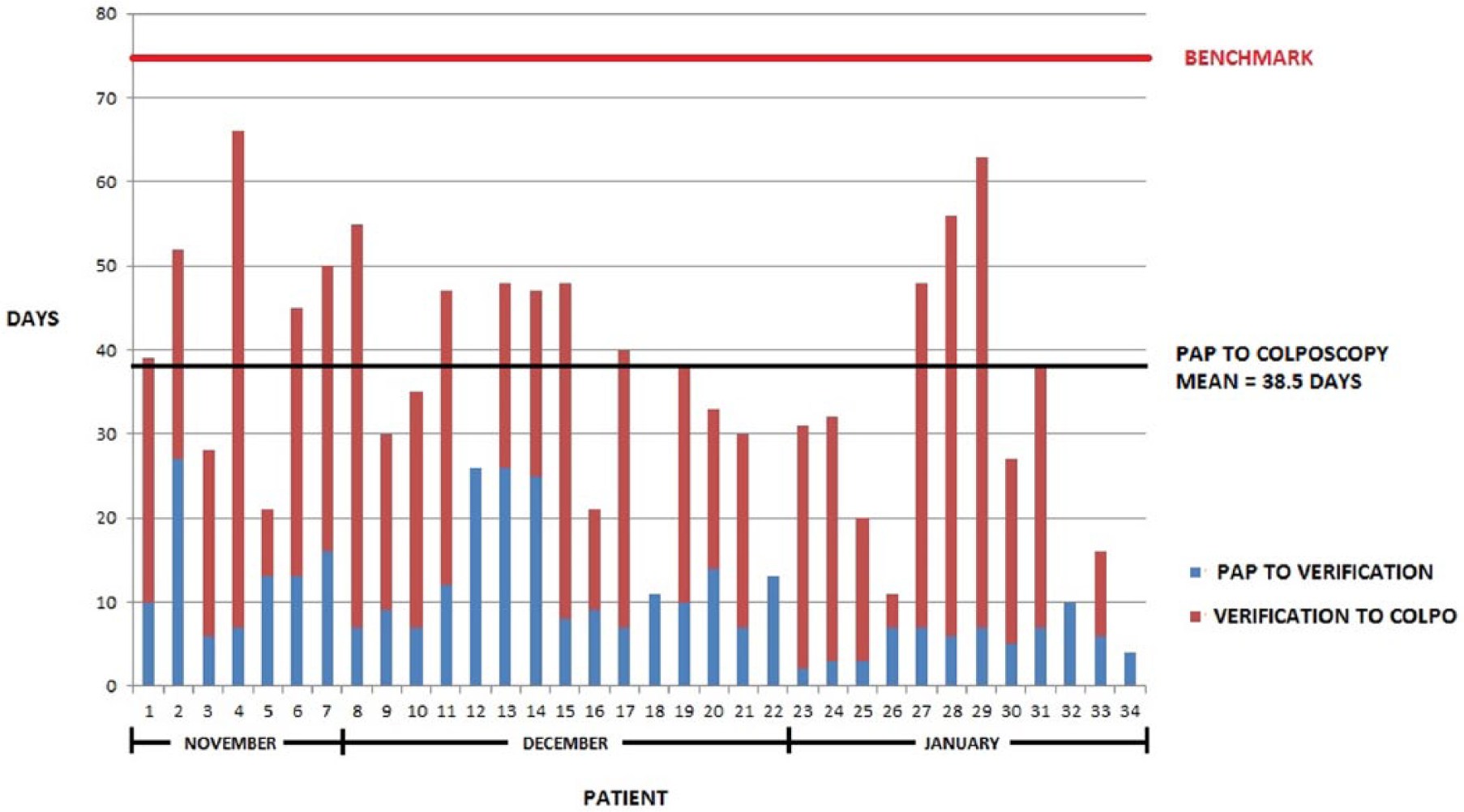
Days from Pap smear to colposcopy by patient.
At 4 weeks, 83% of providers were 100% compliant, and by 12 weeks, all providers were 100% compliant with the protocol. At 12 weeks, similar to the 4-week evaluation, the triage team and the MAs did not feel the work burdensome, 100% of providers felt that they were saving time, and interviews with a sample of 5 patients who arrived for colposcopy showed that they did not mind speaking with the triage team about their colposcopy; all felt that their questions were answered without provoking undue anxiety.
Discussion
Implementation of this quality improvement project using a modified PDSA approach was successful in improving the colposcopy rate among an urban population of women with known abnormal Pap smears. This project improved provider satisfaction by decreasing their workload and improved patients’ satisfaction by providing them with an improved understanding of their condition, all without increasing ancillary staff workload. Although the goal of having 100% of patients receiving this test in 2.5 months was not achieved, there was a 70% improvement from pre-project levels.
One reason for project success was that the workgroup applied the principles of the shared quality agenda described by Reinertsen et al. 9 These principles included involving physicians and NPs early and focusing on their desire to improve patient access to colposcopy, communicating the plan succinctly during the planning and implementation phases, discovering the common purpose of saving time and demonstrating how the plan would reduce the workload, and standardizing an easy-to-follow protocol to evaluate abnormal Pap smears.
Equally important to project success was that the team maximized its potential by focusing on a just culture 10 and applying the principles described by Ovretveit to promote psychological safety among junior members. 11 This allowed all team members, regardless of role, to express ideas on process improvement without fear of repercussion. These principles included supporting each member’s efforts to deliver the best possible care without blame for error; promoting interdisciplinary, open discussion about system failures; implementing change based on the analysis of data; and disseminating information about the improvement. An example of how this just culture was successfully manifested occurred when the MAs were assured that they would not be chastised by providers for sending them reminders to verify labs; the workgroup reinforced this with providers at meetings. Having patients on the team provided a unique perspective for the group and a clearer understanding of the barriers they faced in obtaining appointments.
The selection of the RCA, the PDSA cycle, and Lean process mapping as tools added to project success. RCAs are successful in discovering systems breakdowns rather than individual failings as the causes of errors, 12 as was demonstrated by the 3 causes of poor follow-up in the study population being related to systems issues and not human error. The PDSA was originally described by Shewhart and modified by Deming. 13 It is designed to test changes in the real work setting and to promote rapid-cycle improvement, 14 as was shown by the improvement in this study in just 12 weeks. Lean process engineering allowed the workgroup to define all required tasks, the person responsible, and the time it took to complete the task. 15
The workgroup felt that the improved communication between providers, standardization of protocols, telephone education of patients, and immediate appointment scheduling were all essential to the 70% improvement and the low noncompliance rate of 15%, which was more than twice that of the 18% to 30% improvement and similar to the lower end of the noncompliance rate of 15% to 42% reported by Abercrombie. 6 The present study also supports the work of Abercrombie, who used nursing support staff to increase compliance, and that of Miller et al, 16 who demonstrated that telephone counseling helped improve follow-up. The workgroup felt that patient education by the nurses was essential for the equal follow-up rate between patients with low-grade lesions and those with high-grade lesions, which contradicts the findings by Kola and Walsh, 7 who reported that women with lower degrees of dysplasia were less likely to follow up. This patient education also reduced patient anxiety about the test because no patient failed to keep their first appointment because of anxiety but rather because of inclement weather. The ability to leverage the EHR to improve provider communication and generate reminders to reschedule patients supports the work of White and Kenton, 17 who wrote how using embedded EHR prompts was useful to remind providers to order Pap smear follow-up.
One limitation of this project was that the majority of patients had indemnity insurance and were seen in the urban offices of the attending providers rather than in the resident clinic. However, the project population was not significantly different from the index population. Although employment status was not examined, the patients in this study who had indemnity plans obtained them through work; therefore, one limitation could be that these results may not be applicable to the unemployed, underemployed, or nonurban setting. Another limitation is that educational status was not assessed, and so no comment can be made on whether literacy had an effect on patients’ understanding of their condition, which could affect compliance. The limitation of the EHR used in this study was that it was not 100% effective in sending completed Pap smears for the providers to track; this increased the possibility of human error because providers may “forget” to track their tests. As further functionality improves, the workgroup anticipates relying less on manual verification.
Strategies to sustain success include monitoring compliance by providers with placing patient names on the list, reporting the names of patients who did not arrive for colposcopy after repeated contact attempts, collecting data weekly on the Pap smear to colposcopy time interval, and monitoring patient wait time to see their own provider (given that the success of the project was directly related to the scheduling of the appointment within 2 to 4 weeks of the phone call explaining the results). The plan is to present this information at monthly faculty and staff meetings to illustrate progress and to publicly recognize outstanding performers. The workgroup plans to extend this project to other departmental divisions and the resident clinic to provide a similar improvement in colposcopy rate.
The economic return could be substantial. The fixed cost of the existing triage team and the EHR system were maximized to implement this project with no additional expenses. The opportunity cost savings included increased provider satisfaction and time savings that allowed them to focus on other academic duties or to increase patient visits, demonstrating that in order to improve physician buy-in, a quality improvement project must provide a tangible gain to those involved in addition to the goal of improving patient care. Notably, 2 patients with high-grade lesions had their Pap smear results filed electronically in the chart without being verified by the provider; if these abnormal results had not been acted on by using the verification protocol, these patients would not have been identified, and their lesions possibly would have progressed to cervical cancer, similar to the patient who prompted the original project. The estimated cost of treating a patient with cervical cancer 1 year after diagnosis ranged from $14 000 for in situ cancer to $36 000 for cancers with distant spread.18,19 This would represent a cost savings of at least $28 000, not accounting for inflation, because these patients with high-grade lesions were treated and did not progress to cervical cancer. If one assumes that the rate of undetected lesions remains the same, then one can anticipate avoiding cervical cancer in 8 patients per year. The average 5-year survival rate for cervical cancer is 68%; therefore, 3 lives per year would be saved by this protocol. In areas with a higher rate of cervical cancer, the number of lives saved would be greater. Additional costs for treating cervical cancer would be lost patient work productivity, the psychological cost of having preventable cancer, and the cost of litigation from a missed diagnosis.
In conclusion, by using a modified PDSA approach and Lean process mapping, creating a multidisciplinary team to problem solve, and leveraging the functionality of the EHR, providers improved the rate of colposcopy by 70% within 3 months of plan implementation while improving patient and provider satisfaction and providing an economic benefit without increasing provider workload.
Footnotes
Acknowledgements
The authors would like to thank Susan Freeman, MD, MS, for her assistance in reviewing this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.