
Abstract
Adverse drug events (ADEs) have been highlighted as a national patient safety and public health challenge by the National Action Plan for Adverse Drug Event Prevention (ADE Action Plan), which was released by the Office of Disease Prevention and Health Promotion in August 2014. The following October, the ADE Prevention: 2014 Action Plan Conference provided an opportunity for federal agencies, national experts, and stakeholders to coordinate and collaborate in the initiative to reduce preventable ADEs. The single-day conference included morning plenary sessions focused on the surveillance, evidence-based prevention, incentives and oversights, and additional research needs of the drug classes highlighted in the ADE Action Plan: anticoagulants, diabetes agents, and opioids. Afternoon breakout sessions allowed for facilitated discussions on measures for tracking national progress in ADE prevention and the identification of opportunities to ensure safe and high-quality health care and medication use.
Adverse drug events (ADEs) are among the largest contributors to health care–related harms and are a significant cause of morbidity and mortality for both outpatients and inpatients within the United States. An ADE is defined by the Institute of Medicine as “an injury resulting from medical intervention related to a drug,” 1 and these events include but are not limited to medication errors, adverse drug reactions, allergic reactions, and overdoses. In outpatient settings, national surveillance data indicate that ADEs account for more than 3.5 million physician office visits 2 and an estimated 1 million emergency department (ED) visits each year. 3 In inpatient settings, ADEs account for an estimated one third of all hospital adverse events 4 and affect nearly 2 million hospitalizations annually. 5 Given the large and ever-increasing magnitude of medication exposure in the US population, ADEs represent a major patient safety and public health challenge.
To reduce the patient harms from ADEs, the Office of Disease Prevention and Health Promotion (ODPHP), in conjunction with the Federal Interagency Steering Committee and Workgroups for ADEs, developed the National Action Plan for Adverse Drug Event Prevention (ADE Action Plan). The ADE Action Plan seeks to identify, coordinate, and communicate opportunities and gaps within public and private sectors in order to promote safe use of prescription medications and high-quality patient care.
The Steering Committee identified 3 drug classes as being associated with common, clinically significant, preventable, and measurable ADEs: anticoagulants, diabetes agents, and opioids. These 3 drug classes, all of which require careful monitoring, were implicated in one third of ADEs in a national inpatient sample of Medicare beneficiaries. 4 To address each of the unique challenges that these medication classes present, the Steering Committee established 3 Federal Interagency Workgroups with representation from across federal agencies working in conjunction with subject matter experts. The workgroups focused on each of these drug classes and agreed to target their efforts to address 4 critical areas: surveillance, evidence-based prevention, incentives and oversights, and additional research needs. These 3 drug classes and 4 areas of focus helped define the framework of the ADE Action Plan.
On October 30, 2014, ODPHP, on behalf of the Office of the Assistant Secretary for Health and the Department of Health and Human Services, held the ADE Prevention: 2014 Action Plan Conference in Washington, DC. This conference provided an opportunity for more than 200 in-person and webcast participants to (1) coordinate and collaborate in the initiative to reduce preventable ADEs and (2) discuss potential measures to track national progress in ADE prevention as highlighted in the ADE Action Plan. 3 The conference drew participants from the private and public sectors and included academicians, health policy leaders, clinicians, and pharmacists. The ongoing momentum of ADE prevention, however, will require continued engagement and collaboration within and beyond the clinical quality improvement community.
Opening Remarks and Conference Agenda
Morning plenary sessions provided an overview of the surveillance, evidence-based prevention, incentives and oversights, and additional research needs of 3 drug classes. Afternoon breakout sessions allowed for facilitated dialogue among conference participants in order to discuss measures for tracking national progress in ADE prevention and to identify opportunities to ensure safe and high-quality care for patients who are prescribed the high-priority medications outlined in the ADE Action Plan.
Morning Plenary Session 1: Preventing Anticoagulant ADEs and Monitoring Progress
Dr Shehab provided an overview of the tremendous national burden of anticoagulant-related ADEs and presented strategies for population-based prevention of these events. She outlined the capabilities and challenges of existing anticoagulant-related ADE surveillance systems. For example, at the national level, administrative claims data can be useful for capturing bleeding events, but the accuracy of diagnostic coding (International Classification of Diseases, Ninth Revision [ICD-9]) for identifying these events is not well-established. The impact of the transition to ICD-10 is unknown. Current systems developed for the monitoring and prevention of health care–associated infections, such as the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network, might serve as a good example for benchmarking progress and gaps in ADE prevention efforts.
In addition to highlighting the need for improved surveillance systems, Dr Shehab outlined health policy strategies that might be effective in preventing anticoagulant-related ADEs. She recommended that 2 key areas be addressed: minimizing payment or coverage barriers to delivering evidence-based anticoagulant management and expanding nationally recognized health care quality measures to address safe use of anticoagulants.
Dr Shehab noted that current nationally recognized health care quality measures generally focus on whether anticoagulants are being used, but do not include adequate metrics for whether anticoagulants are used safely. For example, the National Quality Forum (NQF) has endorsed a number of measures related to venous thromboembolism prophylaxis but far fewer that relate to bleeding risk mitigation.
Dr Shehab concluded by summarizing that the surveillance of anticoagulant-related ADEs is currently conducted through a variety of national and local data sources (Table 1). For example, the Medicare Patient Safety Monitoring System (MPSMS) collects national data on inpatient bleeding events within selected patient populations via retrospective chart review, and a number of local process metrics support appropriate monitoring of patients on warfarin. Moving forward, the ADE Action Plan suggests that existing quality measures should be expanded to address (1) safe use of anticoagulants, (2) use of new oral anticoagulants, (3) high-risk populations and settings (eg, long-term care), and (4) clinical outcomes versus surrogate indicators.
Inventory of Potential Measures for Identifying Anticoagulant ADEs.
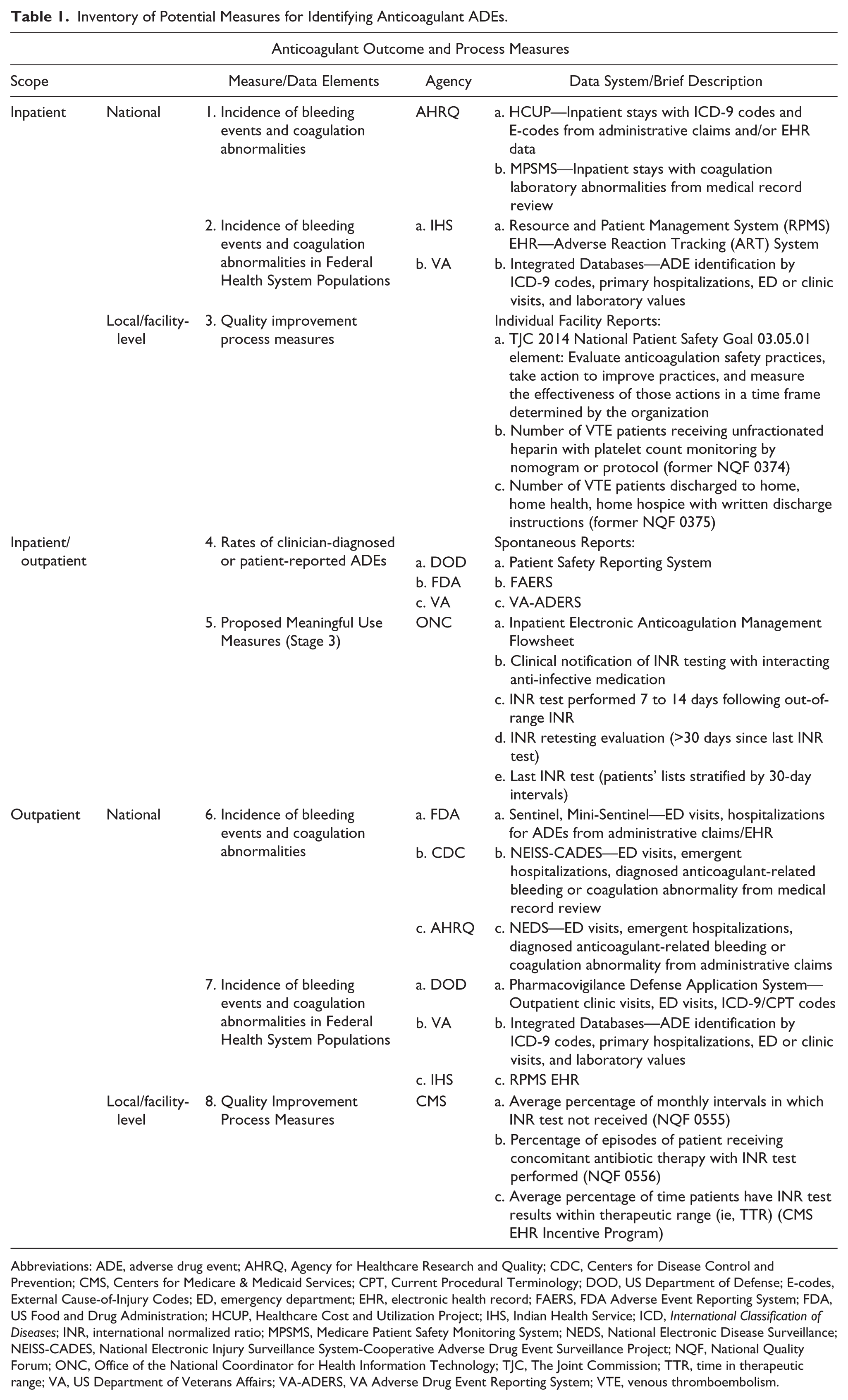
Abbreviations: ADE, adverse drug event; AHRQ, Agency for Healthcare Research and Quality; CDC, Centers for Disease Control and Prevention; CMS, Centers for Medicare & Medicaid Services; CPT, Current Procedural Terminology; DOD, US Department of Defense; E-codes, External Cause-of-Injury Codes; ED, emergency department; EHR, electronic health record; FAERS, FDA Adverse Event Reporting System; FDA, US Food and Drug Administration; HCUP, Healthcare Cost and Utilization Project; IHS, Indian Health Service; ICD, International Classification of Diseases; INR, international normalized ratio; MPSMS, Medicare Patient Safety Monitoring System; NEDS, National Electronic Disease Surveillance; NEISS-CADES, National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance Project; NQF, National Quality Forum; ONC, Office of the National Coordinator for Health Information Technology; TJC, The Joint Commission; TTR, time in therapeutic range; VA, US Department of Veterans Affairs; VA-ADERS, VA Adverse Drug Event Reporting System; VTE, venous thromboembolism.
Dr Thomas provided additional background on strategies for the prevention of anticoagulant-related ADEs. The ADE Action Plan highlights improved communication, patient engagement, and care coordination as a key strategy for anticoagulant-related ADE prevention. Medication reconciliation and appropriate simplification of medication regimens are also areas for improvement. She further emphasized that although evidence-based practices are optimal, it is also critical to engage communities to identify local best practices.
Dr Thomas then highlighted the role of the CMS Quality Improvement Organization (QIO) in decreasing ADEs. The QIO is an integral part of national quality strategies to improve care for individuals, improve health for populations, and reduce health care costs. Within the QIO, the Quality Innovation Network champions local-level, results-oriented change while facilitating learning and action networks as well as providing technical assistance for ADE prevention.
Dr Kaatz provided a clinical perspective on opportunities for improvement in anticoagulation use. He recognized that fiscal constraints can limit the ability of health care systems to implement inpatient anticoagulation services, and that the lack of reimbursement for outpatient anticoagulation clinics limits their widespread utilization. Dr Kaatz emphasized, however, that large integrated health care systems can successfully implement systems-based strategies to manage anticoagulation, as exemplified by the US Department of Veterans Affairs (VA). Resources for a systems-based approach to improving anticoagulation safety are readily available through the Anticoagulation Forum’s Anticoagulation Centers of Excellence, the National Certification Board for Anticoagulation Providers, and the Indian Health Service’s 3-day training program, among other training programs.
Dr Kaatz concluded the anticoagulation session with an emphasis on the proposed incentives and oversight opportunities for preventing anticoagulant-related ADEs across health care settings. Within the inpatient environment, quality incentives robust enough to effect change are needed. Moving forward, the outpatient side will require modifications in the reimbursement structure for anticoagulation clinic care. Furthermore, there must be a mechanism for anticoagulation clinics to manage extended care.
Afternoon Breakout Session Summary: Preventing Anticoagulant ADEs and Monitoring Progress
Morning Plenary Session 2: Preventing Diabetes Agents ADEs and Monitoring Progress
Dr Pogach provided an overview of serious hypoglycemic events in outpatient settings and highlighted the contribution of hypoglycemia to the burden of ADEs. Insulin is the most common drug implicated in ADE-related ED visits, 6 and insulin and oral diabetes agents are implicated in 25% of emergent hospitalizations for ADEs in older adults. 7
Opportunities for advancing the prevention of hypoglycemia include safer care, patient and family engagement, effective communication and coordination of care, and science-driven prevention and treatment. Dr Pogach described the VA’s leadership role in preventing hypoglycemia and emphasized strategies such as individualized glycemic targets and shared decision making, as well as universal health literacy and health numeracy.
Dr Pogach concluded his portion of the presentation with a discussion of health information technology including recommendations for more robust electronic health records (EHRs) that link pharmacy and laboratory data, include data elements that record comorbid conditions, and are able to create patient lists stratified by specific lab values and certain risk factors.
Dr Andrawis gave an overview of the impact of diabetes agents–related ADEs and then focused on the prevention of serious hypoglycemic events in inpatient settings. She noted that challenges to inpatient glycemic control include the lack of a standard definition for serious, severe, or clinically significant hypoglycemia; conflicting evidence regarding ideal glycemic targets; a lack of systematic identification of patients at risk for hypoglycemia; and barriers to multidisciplinary coordination.
Dr Andrawis discussed 2 significant challenges that underscore the need to systematically identify inpatients at risk for hypoglycemia: (1) failure to adjust insulin/diabetes regimens in response to decreases in oral intake such as an unexpected interruption of tube feedings or other sources of nutrition and (2) failure to respond appropriately to an initial hypoglycemic event. To address these challenges and help prevent hypoglycemia in the inpatient setting, Dr Andrawis recommended adopting basal/bolus insulin protocols instead of sliding-scale insulin, instituting a nurse-driven protocol for hypoglycemia management, and coordinating blood glucose testing with meals and insulin administration.
LCDR Geller highlighted key considerations in surveillance, such as selecting data sources and metrics for monitoring ADEs, and the relative importance of quantifying known ADEs rather than signal detection of rare or unrecognized ADEs. Accurate quantification requires active surveillance as opposed to relying on passive or voluntary reporting systems, and when possible, actual patient harms should be measured rather than surrogate markers.
LCDR Geller focused on data sources that can be leveraged to monitor diabetes agents–related ADEs in both the inpatient and ambulatory settings. The discussion included an overview of sources such as the Agency for Healthcare Research and Quality’s MPSMS, which has been used to measure the percentage of patients administered hypoglycemic agents with an episode of hypoglycemia requiring intervention in the inpatient setting. For ambulatory patients, the National Health Interview Survey, a household survey that quantifies the number of Americans self-reporting a diabetes diagnosis and treatment with insulin or oral diabetes agents, can be leveraged to derive denominator data.
LCDR Geller then reviewed several of the existing measure concepts for hypoglycemia (Table 2). For ambulatory patients, Healthy People 2020’s Medical Product Safety (MPS) topic area currently has an objective (MPS-5.2) to reduce ED visits for overdoses from injectable antidiabetic agents. For hospitalized patients, NQF Endocrine Measure 2363 looks at the rate of severe hypoglycemic events following the administration of an antidiabetic agent. LCDR Geller’s discussion of data sources and metrics laid the groundwork for the afternoon breakout sessions.
Inventory of Potential Measures for Identifying Diabetes Agents ADEs.
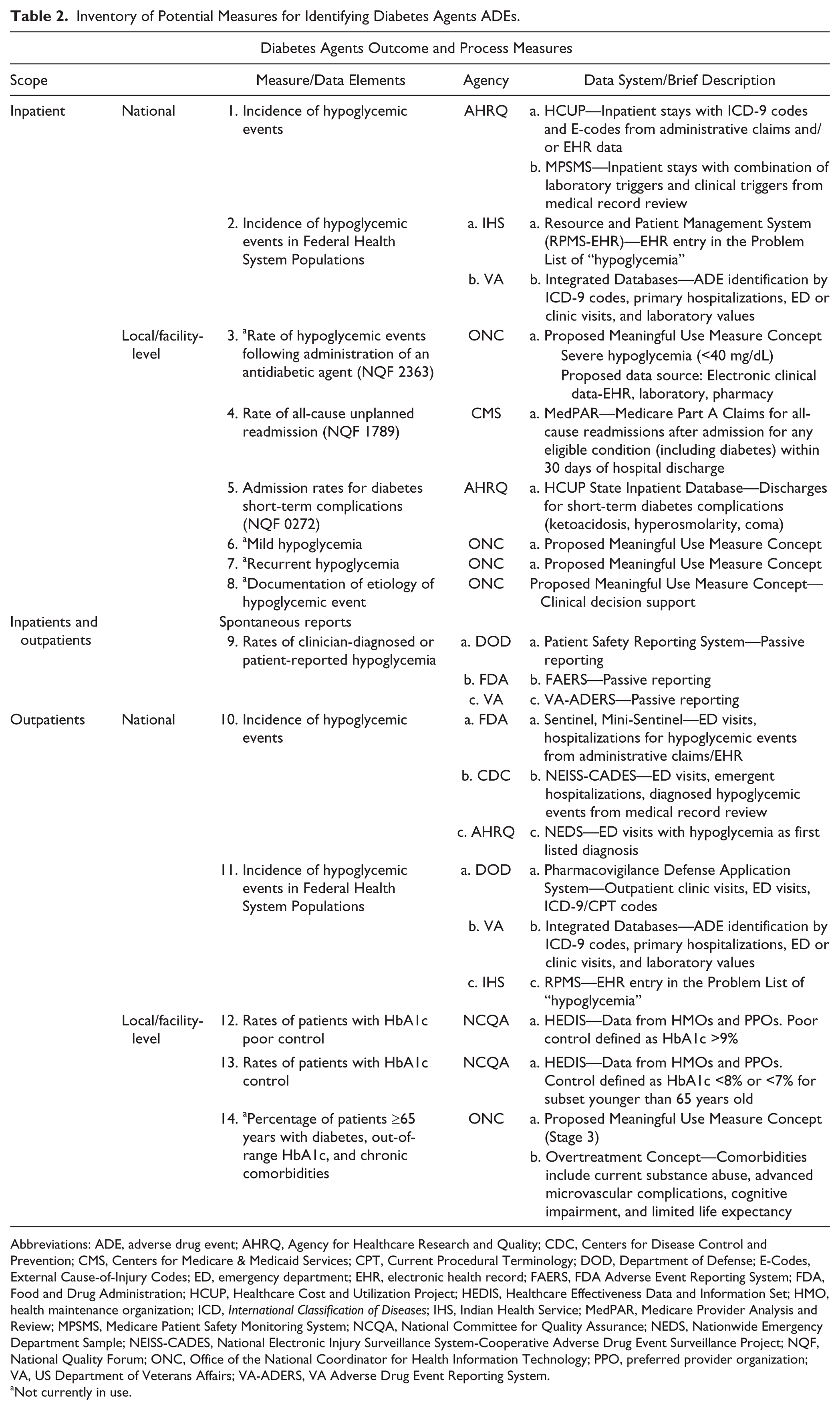
Abbreviations: ADE, adverse drug event; AHRQ, Agency for Healthcare Research and Quality; CDC, Centers for Disease Control and Prevention; CMS, Centers for Medicare & Medicaid Services; CPT, Current Procedural Terminology; DOD, Department of Defense; E-Codes, External Cause-of-Injury Codes; ED, emergency department; EHR, electronic health record; FAERS, FDA Adverse Event Reporting System; FDA, Food and Drug Administration; HCUP, Healthcare Cost and Utilization Project; HEDIS, Healthcare Effectiveness Data and Information Set; HMO, health maintenance organization; ICD, International Classification of Diseases; IHS, Indian Health Service; MedPAR, Medicare Provider Analysis and Review; MPSMS, Medicare Patient Safety Monitoring System; NCQA, National Committee for Quality Assurance; NEDS, Nationwide Emergency Department Sample; NEISS-CADES, National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance Project; NQF, National Quality Forum; ONC, Office of the National Coordinator for Health Information Technology; PPO, preferred provider organization; VA, US Department of Veterans Affairs; VA-ADERS, VA Adverse Drug Event Reporting System.
Not currently in use.
Afternoon Breakout Session Summary: Preventing Diabetes Agents ADEs and Monitoring Progress
Dr Pogach summarized key themes discussed in the diabetes agents–related ADE measures breakout session where the potential measures for tracking national progress in diabetes agents ADE prevention were discussed (Table 2). First, the breakout participants agreed that it was important to meet meaningful use criteria in order to improve and monitor patient care; however, it is essential to carefully consider unintended consequences of these systems. Dr Pogach also emphasized the need for a consistent definition of hypoglycemia and consistent glucose thresholds within the hospital systems. Participants also discussed general issues associated with patient reporting of hypoglycemia. For example, when reporting about a hypoglycemic event, additional qualitative details about the impact of the event on the patient’s quality of life can provide a wealth of information. There are not easy mechanisms for incorporating this narrative into the EHR, however. Furthermore, it may be necessary to stratify populations in order to address the specific needs of patients based on their age or comorbidities.
Morning Plenary Session 3: Preventing Opioid ADEs and Monitoring Progress
Dr Kerns introduced and highlighted several important themes present in the ADE Action Plan regarding both the problem posed by the need for opioids to treat patient pain and subsequent possible ADEs and their prevention. For example, the available literature examining opioids versus placebo or nonopioids for chronic low-back pain is scarce and does not provide clear support for opioid use. Opioids can be essential tools to manage pain in both the acute and palliative care settings, but the widespread and growing controversy regarding opioid therapy for chronic pain needs to be addressed. The ADE Action Plan should be considered within the context of published guidelines for the management of acute postoperative pain, pain in the palliative care setting, and management of chronic noncancer pain—calling for judicious use of opioids in appropriately selected and monitored patients. Dr Kerns reiterated that the ADE Action Plan focuses only on the therapeutic use of opioids, not illicit and/or recreational use, medication withdrawal, intentional harm, and medication nonadherence.
CDR Jones reviewed surveillance methods outlined in the opioids section of the ADE Action Plan, reemphasizing that disentangling use and abuse remains a challenge. There are a variety of opioid-related adverse outcomes to track, including clinical (primary) outcomes such as ED visits or deaths and intermediate (surrogate) outcomes such as clinical or laboratory values, (eg, toxicity screens) that precede or lead to clinical outcomes. The section also provides process measures that are indicators of actions aimed at mitigating risk for primary or surrogate outcomes. Recently, there have been advances in surveillance capabilities including more specific diagnostic and procedural coding, improved process measures across inpatient and outpatient settings, EHR integration, and Prescription Drug Monitoring Programs (PDMPs).
CDR Jones emphasized surveillance as the cornerstone of understanding the problem of opioid-related ADEs and of tracking progress to improve opioid safety. Current systems are not optimal for opioid-related ADE surveillance, but opportunities exist to develop clinical outcome and process measures, standardize definitions for opioid-related ADEs, create new agency collaborations, and conduct research to validate candidate metrics. First, federal agencies should explore ways to improve uptake of evidence-based strategies for safe opioid prescribing through the increased use of opioid-prescribing guidelines and through the development of appropriate provider training programs. Second, federal agencies should promote patient-centered, multimodal, team-based care to personalize pain management; properly manage patients with high-risk medical and mental comorbidities; and intensively manage patients at high risk for opioid overdose. Third, federal agencies should develop and encourage the use of patient education materials and tools. Such materials should be developed using health literacy principles and engage the patient to use opioids safely. Finally, federal agencies can leverage and learn from other federal partners’ individual initiatives related to patient care.
COL Coster gave an overview of the incentives and oversight involved in preventing opioid-related ADEs. She emphasized drug utilization reviews with administrative and/or point-of-sale data for better oversight with flags on the accounts of possible at-risk patients. The sharing of such data among pharmacies and physician practices also can assist in preventing unsafe opioid prescribing and dispensing.
In the inpatient setting, health care quality reporting measures can be expanded to include multidisciplinary models of pain management and metrics can be validated for the monitoring of patient-controlled analgesia. Meanwhile, outpatient strategies for improved opioid safety include defining metrics for process measures that identify high-risk patients; addressing financial barriers to using evidence-based prevention strategies; using multidisciplinary teams and multimodal treatments for pain management, especially in transitions of care; and developing metrics for identifying high-risk patients and high-risk prescribers using administrative data and PDMPs that lead to abuse or misuse.
Dr Perfetto concluded the plenary session on opioids by focusing on some of the specific measures and metrics that CDR Jones summarized earlier. Currently, data are collected on national opioid-related ADE outcomes measures by a number of systems that capture inpatient and outpatient events, ED visits, and prescribing patterns (Table 3).
Inventory of Potential Measures for Identifying Opioid ADEs.
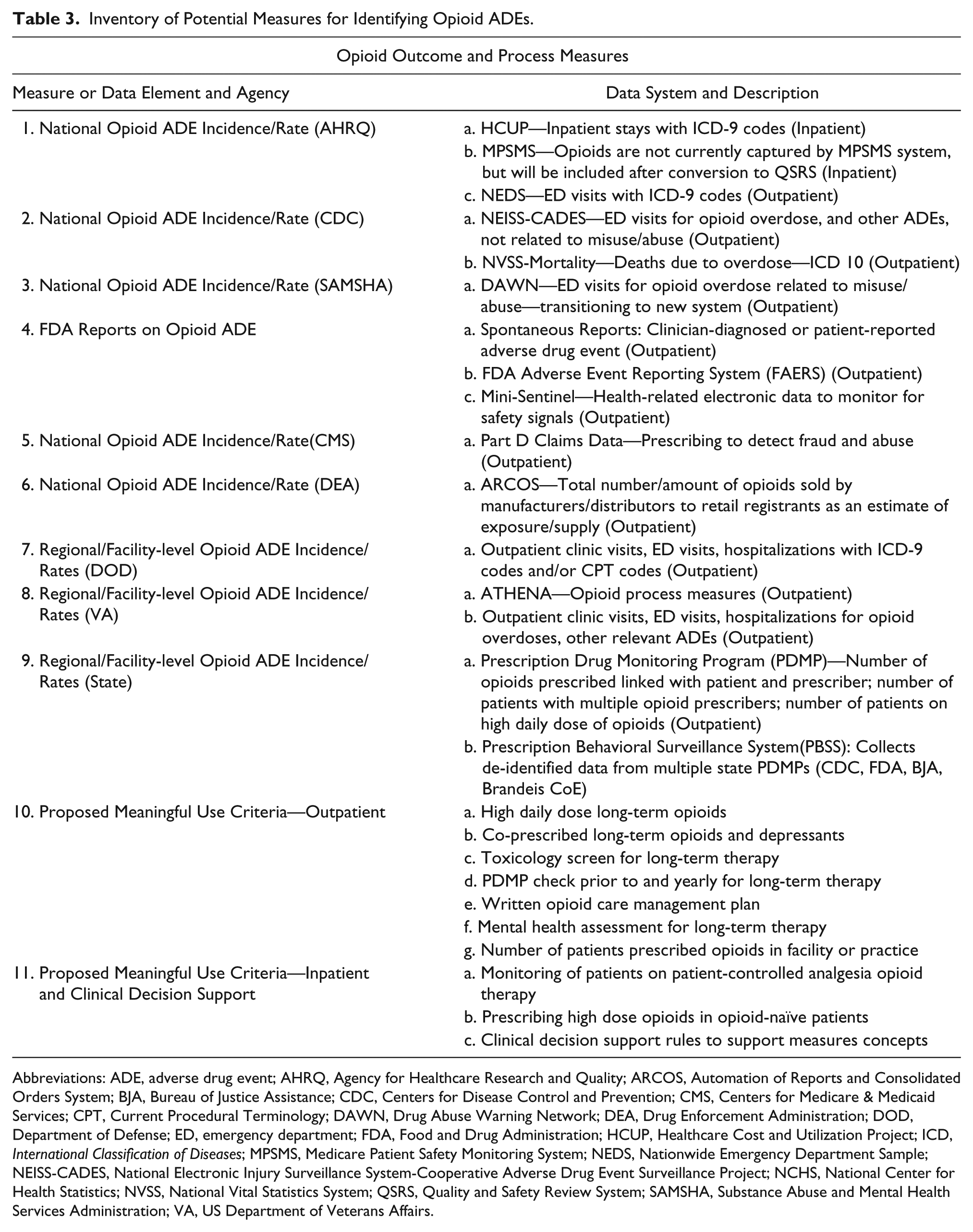
Abbreviations: ADE, adverse drug event; AHRQ, Agency for Healthcare Research and Quality; ARCOS, Automation of Reports and Consolidated Orders System; BJA, Bureau of Justice Assistance; CDC, Centers for Disease Control and Prevention; CMS, Centers for Medicare & Medicaid Services; CPT, Current Procedural Terminology; DAWN, Drug Abuse Warning Network; DEA, Drug Enforcement Administration; DOD, Department of Defense; ED, emergency department; FDA, Food and Drug Administration; HCUP, Healthcare Cost and Utilization Project; ICD, International Classification of Diseases; MPSMS, Medicare Patient Safety Monitoring System; NEDS, Nationwide Emergency Department Sample; NEISS-CADES, National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance Project; NCHS, National Center for Health Statistics; NVSS, National Vital Statistics System; QSRS, Quality and Safety Review System; SAMSHA, Substance Abuse and Mental Health Services Administration; VA, US Department of Veterans Affairs.
The Automation of Reports and Consolidated Orders System (ARCOS) provides current process measures on the national ADE incidence rate. The ARCOS system is an automated, comprehensive drug reporting system that monitors the flow of US Drug Enforcement Administration controlled substances from their point of manufacture through commercial distribution channels to point of sale or distribution at the dispensing/retail level.
In addition to outcome and process measures, there are a number of quality improvement measures in place to identify regional- or facility-level opioid-related ADE incidence rates. Organizations with key quality improvement measures include, but are not limited to, the DOD, the VA, PDMPs, and patient safety organizations. For example, PDMPs serve as networks to track patients with high daily doses of opioids, multiple prescribers, and connecting patients and their appropriate prescriber. One other group of measures discussed in detail included the Proposed Meaningful Use Criteria for both inpatient and outpatient safe opioid use. The purpose of these measures is to also act as a safety checkpoint with actions such as identifying opioid naïve patients or patients prescribed both opioids and central nervous system depressants such as benzodiazepines. These measures served as various focal points for discussion during the opioid breakout sessions in the afternoon.
Afternoon Breakout Session Summary: Preventing Opioid ADEs and Monitoring Progress
Dr Kerns provided highlights of key themes from the afternoon opioid-related ADE prevention breakout session where the potential measures for tracking national progress in opioid ADE prevention were discussed (Table 3). He noted that it would be essential to consider the ADE Action Plan within the context of the national imperative to improve pain care. The prevention of opioid-related ADEs will require patient-centered care in order to avoid the magnification of existing pain management stigma and disparities. The breakout participants agreed that attention to improved operationalization of existing strategies is necessary. For example, the urine drug screen depends on setting, patient population, context, and sensitivity of assay. Additionally, participants suggested the potential benefit of shortening the 90-day surveillance period in order to analyze the optimal follow-up threshold. The group expressed a similar concern about dosing thresholds and recommended the need for further research.
Closing Remarks
As part of closing remarks, CAPT Hu thanked participants for their attendance and thoughtful contributions to the important work of ADE prevention. He suggested that the diversity of backgrounds and expertise of participants greatly benefited the conference sessions. He commented that although a tremendous amount of work has been done to date, there is still a lot to be done. Over the coming year, the Federal Interagency Steering Committee will reconvene in order to discuss the potential measures for tracking national progress in ADE prevention. Ongoing federal efforts will target the 4 focus areas of the ADE Action Plan in order to improve surveillance, evidence-based prevention strategies, incentives and oversight, and further research.
Conclusions
In summary, the ADE Prevention: 2014 Action Plan Conference highlighted important ADE prevention strategies for anticoagulants, diabetes agents, and opioids as a national patient safety priority. The expert panel of plenary speakers illustrated broad-based federal support for this initiative. Conference participation from health care providers, advocacy groups, policy analysts, and industry representatives, among others, demonstrated substantial private sector interest in engaging with the challenge of ADE prevention. Echoed throughout the morning plenaries and afternoon breakout sessions was the sentiment that ongoing collaboration and innovative solutions will be needed in order to protect patients from ADE-related harms. The discussions held in the afternoon breakout sessions will serve as a basis for the reconvening of the Federal Interagency Workgroup for ADE Prevention. Under their guidance, and with input from public stakeholders and subject matter experts, national benchmarks will be established to measure progress in ADE prevention. Although a multitude of efforts, including those highlighted in this conference, continue toward this end on a day-to-day basis, the establishment of national measures and targets for reducing ADEs will help align efforts across the public and private sectors and coordinate targeted initiatives toward ADE prevention.
Footnotes
Acknowledgements
We would like to thank the lead speakers and facilitators for their contributions to the success of the ADE Prevention: 2014 Action Plan Conference. In addition to the speakers listed in the text, we would like to thank Dr Nadine Braunstein, Dr Kyle Campbell, Dr Simon Dagenais, Dr E. Robert Feroli, Dr Robert Hurley, Dr Brian Isetts, Meelee Kim, Dr Andrew Kolodny, Dr Christine Lee, Dr Mishale Mistry, CDR Sharon Saydah, Dr Maureen Schanck, Dr Samuel F. Stolpe, Dr Robert Twillman, and Dr Andrew York for facilitating the afternoon breakout sessions. We would also like to thank Dr Paul Hughes and the US Institute of Peace, Daniel Gallardo, Dr Philip Blanc, Connor Hughes, Dr Leith States, the American Institutes for Research, and Kayla Schuster for their support. This research was supported in part by an appointment to the Research Participation Program at the Department of Health and Human Services administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the US Department of Energy and the US Department of Health and Human Services.
Authors’ Note
The authors prepared this work within the scope of their employment with the US Department of Health and Human Services (DHHS). The views expressed herein are those of the authors and do not necessarily reflect the views of the DHHS.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.