
Abstract
Effective quality improvement is a key factor in optimizing the care of hospitalized patients. Unfortunately, the US health care system has a poor safety record when compared to other major industries. For example, at 250 000 per year, medical errors are the third leading cause of death in the United States. Safety barrier management, a widely used methodology in high-risk industries such as commercial airline transportation and oil drilling, has not been widely used in traditional quality improvement efforts in health care, which rely more on standard lean Six Sigma quality approaches. The authors describe a quality improvement project that uses safety barrier analysis to help inform solutions to improve venous thromboembolism prophylaxis in hospitalized patients. This study found that safety barrier analysis helped inform solutions to improve venous thromboembolism prophylaxis at the study institution and can be a useful adjunct to standard lean Six Sigma methodologies for quality improvement in health care.
Safety barrier management, a widely used methodology in high-risk industries such as commercial airline transportation and oil drilling, has not been widely used in traditional quality improvement efforts in health care, which rely more on standard lean Six Sigma quality approaches. The strength of safety barrier management lies in its focus on a degree of formality and rigor in designing and implementing improvements in care processes that mitigate downstream effects of predictable human error on patient safety. A common method used to assess risk and optimize protective safety barriers is bow-tie analysis (BTA).1-5 The current study describes the use of safety barrier analysis, specifically BTA, combined with lean Six Sigma methodologies to develop interventions to reduce hospital-acquired venous thromboembolism (VTE).
VTE, including deep vein thrombosis and pulmonary embolism, is a significant contributor to morbidity and mortality in hospitalized medical and surgical patients. Of the approximately 900 000 people afflicted and 100 000 who die from VTE each year in the United States, more than half are hospital-associated (HA) VTEs that are potentially preventable with appropriate prophylaxis.6-8 The Centers for Medicare & Medicaid Services has identified HA-VTEs as potentially preventable “never events” and significant financial penalties exist for hospitals if patients experience HA-VTEs. Despite much attention paid to reducing HA-VTEs at the study institution, it still remains one of the highest hospital-acquired conditions.
This article describes a quality improvement project that uses safety barrier analysis to help inform solutions to improve VTE prophylaxis at the study institution. Specifically, BTA is used to identify and analyze key clinical risks (or safety threats) to appropriate VTE prophylaxis, as well as protective safety barriers preventing or mitigating the effects of safety threats on patient outcomes. The overall objective is to show how BTA can be used as an adjunct to standard lean Six Sigma methods for quality improvement in health care.
Methods
Study Setting
The University of North Carolina (UNC) Hospitals is an 803-bed tertiary academic medical center. UNC Hospital Medicine division is staffed by 29 physicians and 3 advanced practice providers (APPs). During the study period, there were 3 hospital medicine services at UNC Hospitals with a combined average daily census of approximately 40 patients, and each was staffed by 1 attending physician every day of the week and 1 APP Monday through Friday.
Study Design
Description of Bow-Tie Methodology
BTA covers all steps of a care process in which process failures can occur and lead to adverse patient outcomes. The strength of BTA is that it provides both a conceptual and visual representation of how threats to patient safety and quality of care are prevented and/or mitigated by existing safety barriers.
The first step in BTA is defining the top-level process failure (center of Figure 1). When the top-level process failure occurs no patient harm has yet transpired, but 1 or more key care processes has broken down that can directly result in an adverse patient outcome (eg, pulmonary embolism). In the case of VTE prophylaxis, the top-level process failure occurs when a patient at high risk of VTE, with no contraindications to VTE prophylaxis, is not receiving appropriate VTE prophylaxis. The top-level event can be triggered by 1 or more threats (left side of Figure 1). Threats are events that, if not prevented by safety barriers, are likely to lead to the top-level process failure. Preventive safety barriers are defenses against threats and reduce the likelihood that the threat will result in the top-level process failure. Mitigating barriers (right side of Figure 1) are defenses against the top-level process failure leading to adverse patient outcomes. Safety barriers are not always foolproof and their performance can be degraded (via degradation factors). Safeguards are intended to prevent degradation factors from interfering with the effectiveness of safety barriers. The efficacy of safety barriers can range from 0% to 100%; they are influenced by provider (eg, human error), patient, and system factors.
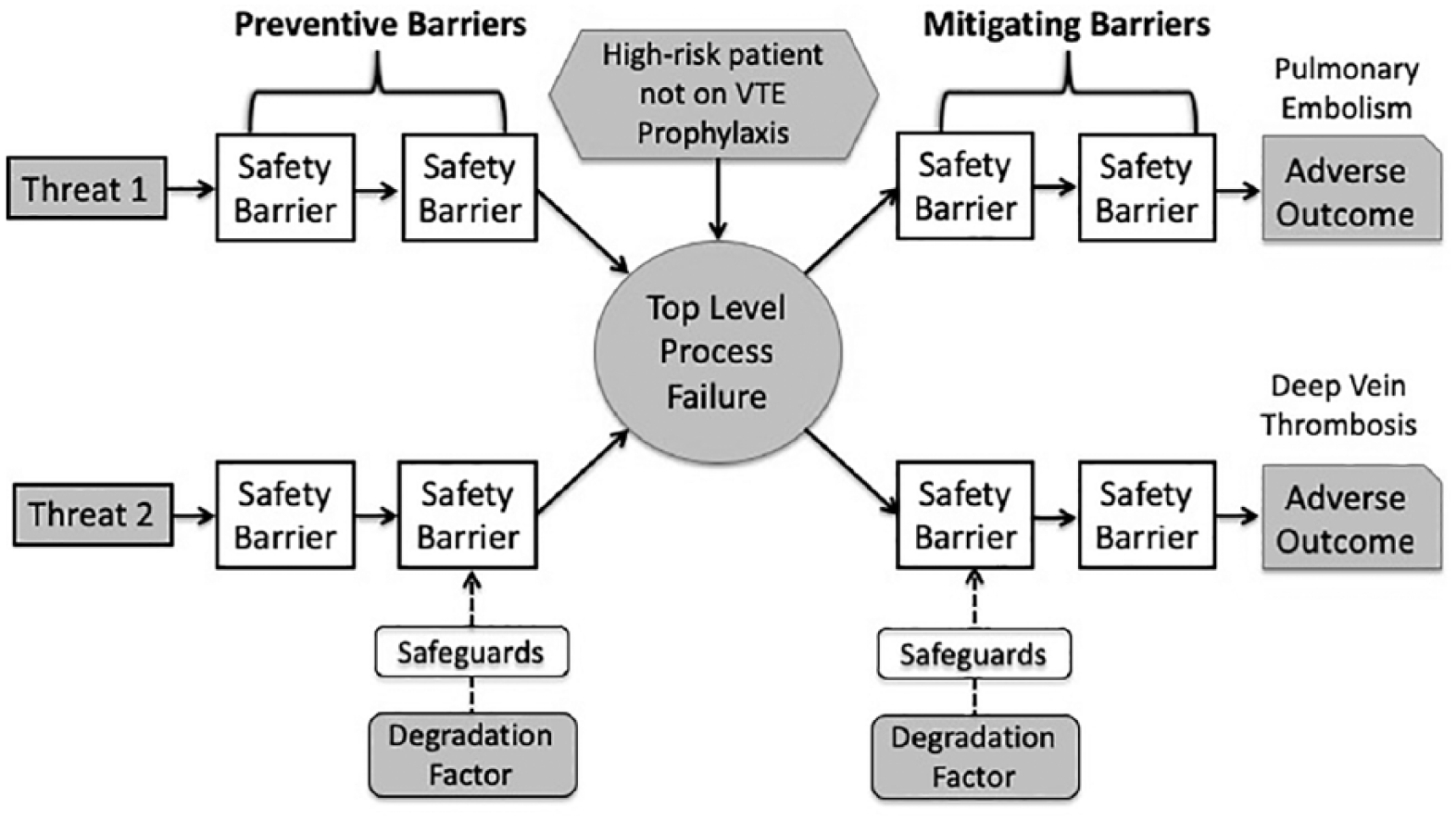
Bow-tie analysis components.
The next step in BTA is defining the threats, safety barriers, safeguards, and degradation factors in more detail. In order to accomplish this task, the current state of the system must be described; in the current case this is VTE prophylaxis.
Mapping the Current State of VTE Prophylaxis
To understand the current state of VTE prophylaxis at the study institution, a high-level process map was created to model all clinical workflow related to VTE prophylaxis, beginning from hospital admission to hospital discharge. The goal was to conceptualize the sequence of events related to VTE prophylaxis that occurred for most patients admitted to the study hospital. A team-based approach was used to create this process map and included both subject matter experts (frontline clinicians [eg, physicians, nurses]) and specialists trained in lean quality improvement methodologies. Multiple brainstorming meetings were held to develop the high-level process map collaboratively.
Figure 2 shows a high-level driver diagram of the current state of VTE prophylaxis at the study institution. During the hospital admission process (P1 in Figure 2), VTE risk and bleeding risk are assessed and a judgment is made of whether or not to prescribe VTE prophylaxis based on physicians’ risk-benefit analysis. During the hospitalization (P2 and P3 in Figure 2), patients’ VTE and/or bleeding risks may change (eg, patient scheduled for surgical procedure with high bleeding risk). Ideally, treating physicians are cognizant of changes in VTE prophylaxis risk and benefit and make appropriate adjustments in prophylaxis; however, this does not always occur. Additionally, patients prescribed VTE prophylaxis may refuse treatment because of discomfort from daily subcutaneous injections. Finally, during the discharge process (P4 in Figure 2), patients may require post-discharge VTE prophylaxis (eg, hip fracture patients). This may or may not occur during transitions from inpatient to outpatient care.
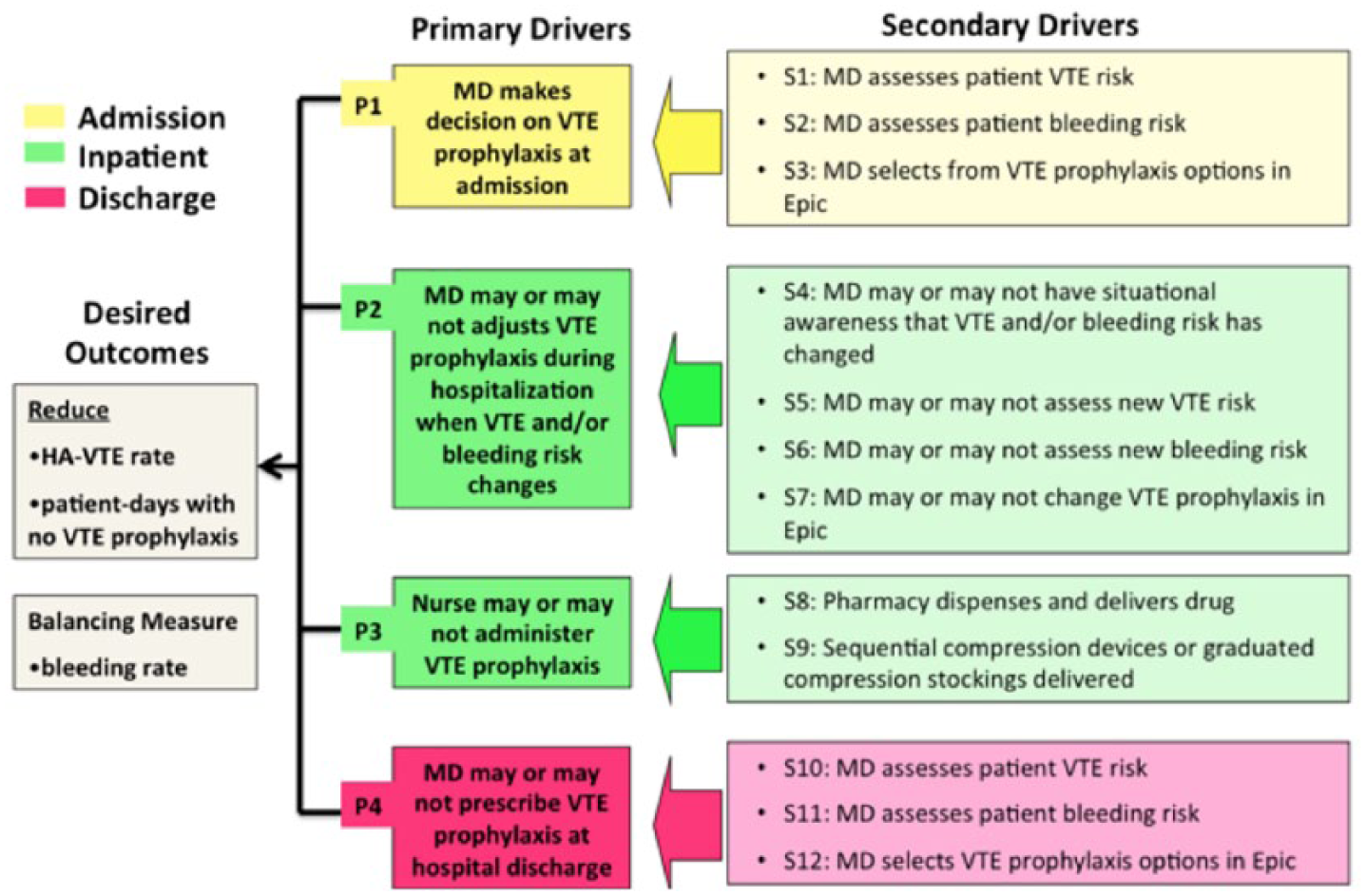
VTE prophylaxis: current state.
The next step after defining the VTE prophylaxis current state was to translate the high-level map into a more detailed process map.
Translating the High-Level Process Map Into a Detailed Process Map (Care Path) in GoodCatch
The high-level process map created was then translated into a detailed process map or care path for use in GoodCatch. GoodCatch is a quality improvement software package developed at the study institution that integrates detailed process mapping, adverse event reporting, and mapping of the location of failures onto the process map. The team worked in close collaboration with a team from the Division of Healthcare Engineering, ultimately categorizing each step in the care path as one of the following: task, safeguard, or safety barrier. Safety barriers were further stratified as engineering, human operational, or human organizational. This classification system reflects health and safety methodologies in industries such as manufacturing, informed by key principles from human factors. The team recognized the importance of including a range of “events” on the process map: physical events (eg, the physician evaluates the patient), cognitive events (eg, the physician mentally risk stratifies the patient’s risk for VTE or bleeding), digital events (eg, the physician places an order for subcutaneous heparin), and task execution events (eg, the nurse receives the order and administers the medication).
Collecting Data on VTE Prophylaxis Process Failures
After developing a detailed process map and implementing this as a care path in GoodCatch, the team began collecting patient-level data to better characterize VTE process failures. The team was interested in identifying cases of either
(1) Suboptimal VTE prophylaxis (eg, a patient at high risk for VTE, with no contraindications for VTE prophylaxis, for whom no prophylaxis was ordered), or
(2) Acute VTE events among hospitalized patients at the study institution.
To better understand the nature of all VTE events—not just perioperative events—and the variability thereof, the team sought to identify VTE events in near real time to perform root cause analysis while the patient was still admitted to the hospital. Data were collected over a 3-month period in near real time (see supplemental Appendix A for details of data collection).
Results
BTA for VTE Prophylaxis
The BTA for VTE prophylaxis is shown in Figure 3. Three distinct threats to optimal VTE prophylaxis were identified (Figure 3). Three preventive safety barriers designed to prevent the threats from propagating and resulting in the top-level event (suboptimal VTE prophylaxis) also were found. Finally, a mitigating safety barrier was identified to block suboptimal VTE prophylaxis from resulting in an adverse patient outcome.
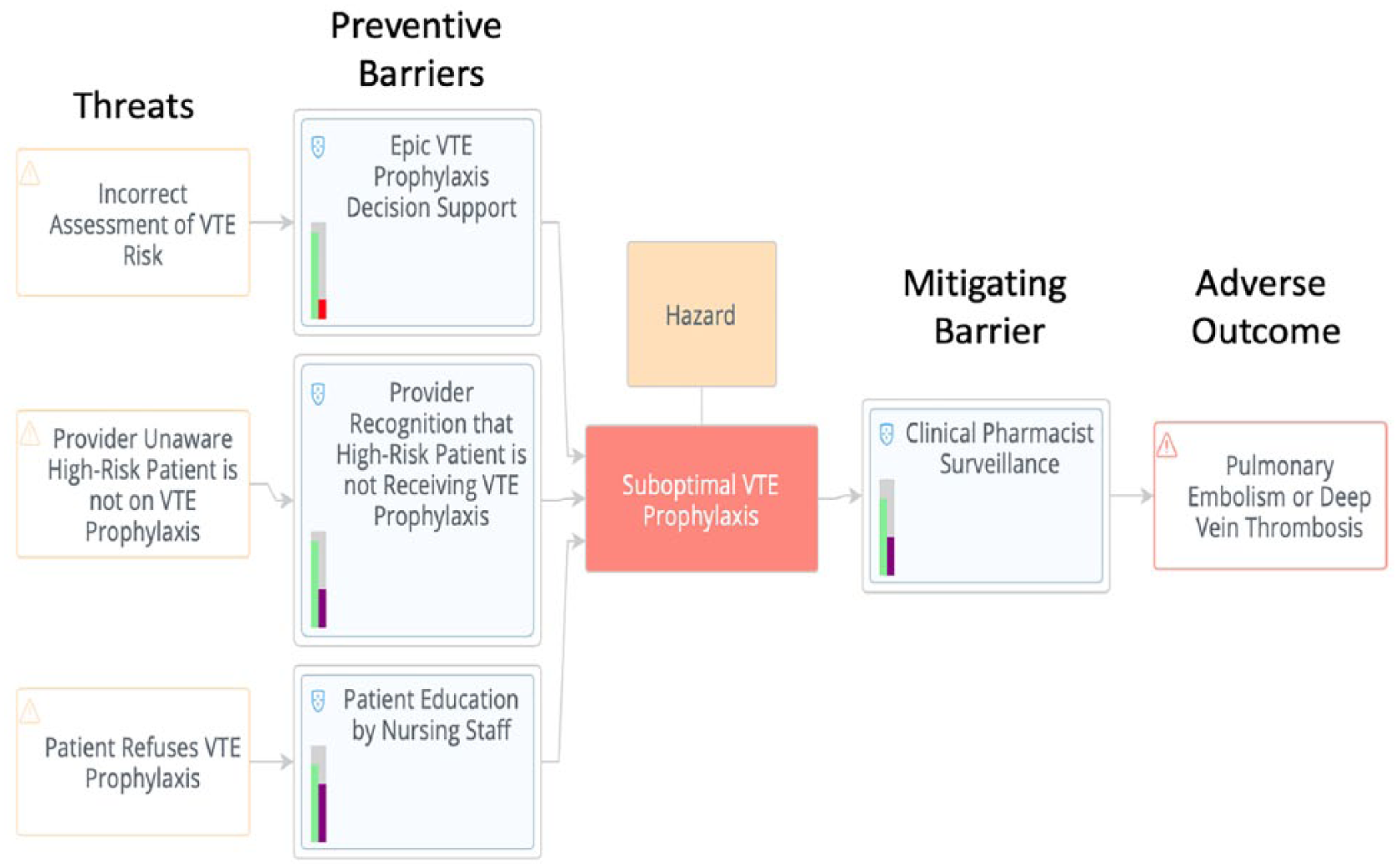
Bow-tie analysis of VTE prophylaxis.
Threat 1: Incorrect Assessment of VTE Risk on Admission
The first threat to optimal VTE prophylaxis is providers incorrectly assessing patient VTE risk at the time of hospital admission. The preventive protective safety barrier against this threat was found to be VTE prophylaxis clinical decision support embedded in standardized admission order sets in the electronic health record (EHR). It was reasoned that effective EHR decision support should guide most providers to appropriately risk stratify their patients at admission. To better understand these dynamics in the current state, a retrospective chart audit was performed of consecutive patients admitted to the hospitalist service (n = 100). Findings suggested risk discordance in 17% of cases; that is, VTE risk assessment made by the provider (high risk/low risk for VTE) did not align with the patient’s actual VTE risk as calculated using a validated clinical scoring system. 9 This risk discordance was equally split: half of cases involved providers assigning high risk to a patient deemed low risk by VTE guidelines and the other half involved providers assigning low risk to a patient deemed high risk by VTE guidelines. This suggested that the existing EHR decision support was performing weakly as a protective barrier. This analysis of the EHR decision support in the VTE order set revealed language that was ambiguous and not evidence based. Specifically, the existing decision support risk stratifies patients as high versus low risk based primarily on patient mobility. If a patient is fully mobile then he/she is stratified as low risk. This recommendation is not consistent with evidence-based guidelines (eg, Padua score) that consider patient immobility as only one of several risk factors (eg, malignancy, obesity, history of VTE) that should go into calculating the patient’s overall VTE risk.
Additionally, it was found that the only safeguard that might improve the effectiveness of the safety barrier was provider knowledge of evidence-based guidelines on VTE prophylaxis. However, a potential degradation factor is high provider workload, which might prevent admitting providers from taking time to calculate patient VTE risk if it requires increased time demands or temporarily exiting the EHR interface/workflow to view external web-based guidelines or risk calculators.
Threat 2: Provider Unaware High-Risk Patient Is Not on VTE Prophylaxis
Poor situational awareness was identified as a second threat to suboptimal VTE prophylaxis. Often, individual providers or provider teams failed to recognize situations in which patients’ VTE risk status and/or bleeding risk changed during the course of a hospitalization. For example, multiple instances were found in which patients undergoing procedures had chemical VTE prophylaxis stopped because of transiently increased perioperative bleeding risk. However, postoperatively these patients inappropriately remained off chemical VTE prophylaxis for many days, even when their bleeding risk returned to baseline, because providers failed to restart prophylactic medications. Similarly, some patients who were at low risk for VTE on admission were found to experience clinical deterioration after admission and thus transitioned into a high VTE risk category, but providers did not modify orders for VTE prophylaxis to reflect the clinical change in risk.
Threat 3: Patient Refuses VTE Prophylaxis
The analysis identified patient refusal of VTE prophylaxis as a third threat to the system. Internal medication audit data from the EHR supported this finding: on some hospital units, rates of patient refusal of chemical VTE prophylaxis exceeded 11%. Patient education by the clinical staff, primarily bedside nurses, was identified to represent a protective safety barrier at the system level. However, a degradation factor reducing the effectiveness of this safety barrier was the lack of standardized workflow for nurses to educate patients, and in general the team observed large variation in the extent to which nurses educated patients about the importance of VTE prophylaxis. Additionally, nurses complained that high workload was often an impediment to taking the time required to properly educate patients on the importance of VTE prophylaxis.
Mitigating Safety Barrier
By identifying high-risk patients not on VTE prophylaxis, clinical pharmacist surveillance was found to be a mitigating protective barrier. At the study institution clinical pharmacists review medications orders for appropriateness of dose and contraindications. The analysis found that some clinical pharmacists, but not all, reviewed their patient lists to determine if VTE prophylaxis was being ordered for high-risk patients. If high-risk patients were not on VTE prophylaxis and there was no obvious contraindication, they contacted providers to discuss the possibility of starting chemical prophylaxis. Two degradation factors were found that limited the effectiveness of this safety barrier. First, high workload was seen as an impediment to conducting surveillance on patients; second, VTE prophylaxis surveillance was not a standard part of pharmacist workflow and therefore varied from individual to individual.
Effect of Interventions on VTE Events
Preliminary results of the interventions are promising. Data were collected on the effects on patient outcomes by conducting a 3-month pre–post intervention study comparing fiscal year (FY) 2017 and 2018 perioperative VTE events (Figure 4). In the 3-month period prior to the interventions (August, September, and October), there were 4 cumulative events in FY17 versus 10 cumulative events in FY18. In the 3-month period after the interventions (November, December, and January), there were 15 versus 9 cumulative events in FY18 and FY17, respectively, thus showing a reduction in the perioperative HA-VTE event rate during the same time periods between FY18 and FY17.
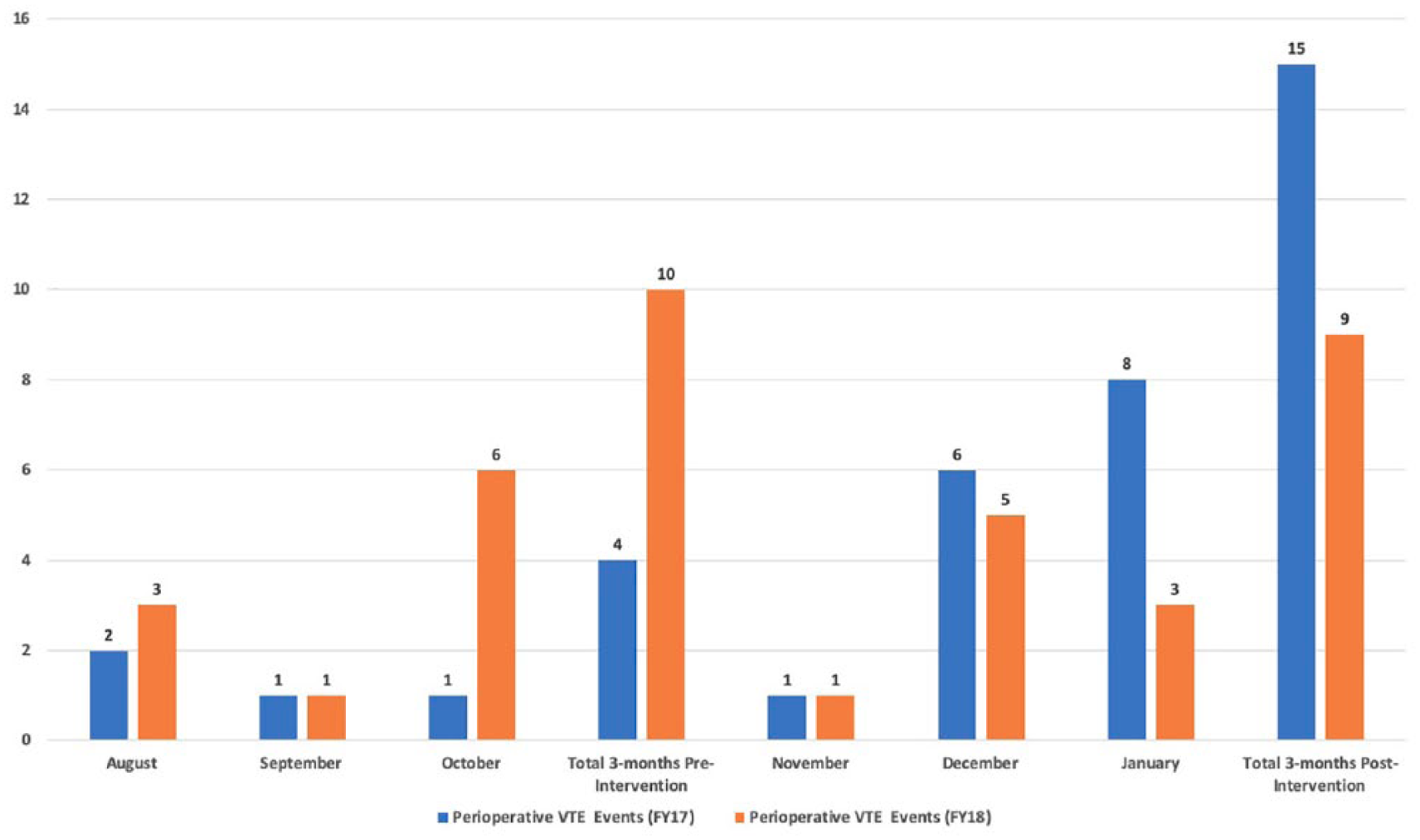
Perioperative VTE events (pre vs post interventions).
Discussion
This study adds to the growing literature showing how BTA can be applied in health care to improve patient safety.1-5 For example, Abdi and colleagues 5 used BTA to identify and control hazards to patient safety in an intensive care unit setting. Similarly, Culwick and colleagues 4 used BTA for risk management in anesthesia. This is the first study to use BTA to address threats to optimal VTE prophylaxis in the hospital setting.
More broadly, this study shows how BTA, a methodology used effectively in high-risk industries outside of health care, can be used to conceptualize and visualize weaknesses in patient care processes. In this way BTA can serve as an important adjunct to standard lean Six Sigma methodologies for quality improvement. A table of the side-by-side comparison of lean Six Sigma versus BTA methodology is shown in supplemental Appendix B. Importantly, BTA can help inform quality improvement solutions that prevent and/or mitigate patient harm. For example, based on the BTA, the team implemented 3 targeted interventions to improve VTE prophylaxis at the study institution.
Intervention 1: Revised EHR Order Sets to Improve VTE Risk Stratification by Providers
The analysis of EHR decision support for VTE prophylaxis revealed language that was ambiguous and not evidence based (top of Figure 5). To remedy this, the EHR decision support was modified to include a concise, free-text, evidence-based risk tool based on the Padua risk score 10 (bottom of Figure 5). To evaluate the revised EHR decision support, 5 hospitalist physicians were recruited to pilot the new tool in a live observational setting. Qualitative feedback was collected on layout and wording, and this feedback was used to iteratively improve the order set. Quantitative data were collected via chart audit (n = 27) on multiple physicians using the new tool, which showed agreement between provider-assigned VTE risk and actual risk (as calculated by Padua risk scoring) in 96% of cases—a 13% improvement in risk discordance compared to the old VTE order set. This experience with a simple EHR-based change aligns with a growing body of work utilizing the concept of electronic “nudges” to improve patient care.11-13
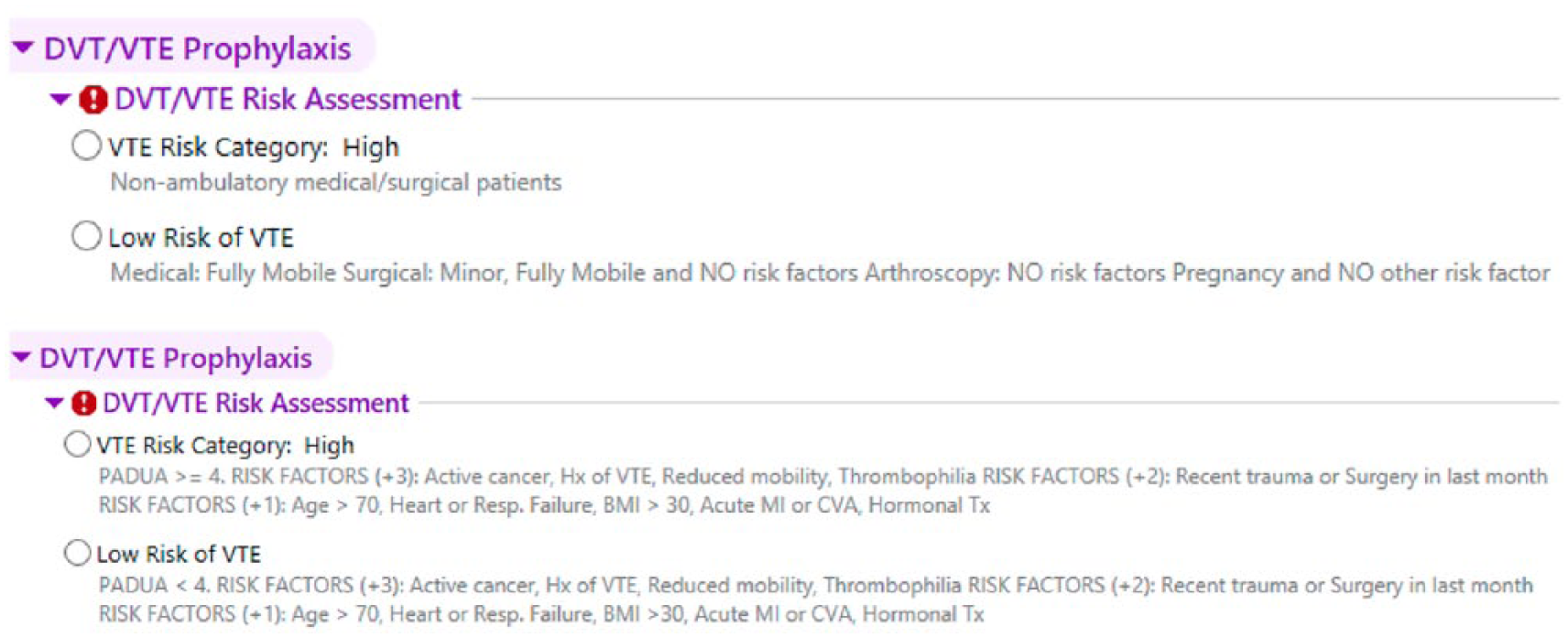
Old (top) versus new (bottom) electronic health record support for VTE stratification.
Intervention 2: Standardizing VTE Risk Surveillance and Creating EHR-Based Visual Cues for Clinical Pharmacists
To strengthen the protective barrier of clinical pharmacist surveillance of VTE prophylaxis, the team engaged with clinical pharmacists to address deficiencies identified in the BTA. To better standardize and improve the ease of clinical pharmacist surveillance of high-risk patients not on VTE prophylaxis, their EHR screens were modified so that all information needed to assess adequacy of VTE prophylaxis for patients appears at a glance on a single EHR screen. This includes the following:
VTE risk status (high vs low)
VTE prophylaxis status (as indicated by the presence of specific medications on the active order list)
Scheduled procedures (as indicated by appointment times in the next 72 hours)
To assess the efficacy of the new pharmacist EHR screen, task-based usability testing was performed in a lab environment using screen capture software. These results suggested considerable improvements in efficiency with the new VTE screen; on average, an individual provider reviewing 10 patients in the EHR could see a time savings of almost 5 minutes while performing 27 fewer mouse clicks.
Intervention 3: Development of a Patient-Focused Script to Improve Patient Compliance
The analysis revealed patient refusal of VTE prophylactic medication as a third threat in the system. To better understand this phenomenon, the team convened a patient focus group that revealed opportunities to improve patient education and engagement concerning VTE risk mitigation. Working with a group of patients, the team developed standard language to support bedside conversations with nurses and other members of the care team. Initial pilot testing of this script indicated buy-in among nursing staff and a trend toward improved patient compliance.
Preliminary results 3 months after implementation of the interventions are promising and show a trend (not statistically significant) toward a reduction in perioperative VTE events compared to the previous year.
This study has several limitations. First, although quantitative and qualitative data were gathered to evaluate the impact of the interventions on VTE care processes, the long-term effects of the interventions on patient outcomes were not rigorously studied. Also, the pre–post analysis of perioperative VTE events did not account for secular trends that may have affected VTE rates. Second, the results of the BTA only apply to the study institution; however, the methodology used to derive the BTA can be used at any institution. Finally, a proprietary software package called GoodCatch was used to map process failures onto the VTE prophylaxis care path. This software may not be available to other institutions; however, the same process of failure mapping can be accomplished using other commonly available tools such as Excel spreadsheets.
Conclusion
This study used BTA, a methodology applied in other high-risk industries such as commercial airline transportation, to identify weaknesses in the study institution’s VTE prophylaxis care processes. BTA helped inform solutions to improve quality of care for hospitalized patients at high risk for VTE. BTA can be a useful adjunct to standard lean Six Sigma methodologies for quality improvement and patient safety in health care.
Supplemental Material
Supplemental_Material – Supplemental material for Using Safety Barrier Analysis to Facilitate Quality Improvement in Health Care: Improving Venous Thromboembolism Prophylaxis as a Proof of Concept
Supplemental material, Supplemental_Material for Using Safety Barrier Analysis to Facilitate Quality Improvement in Health Care: Improving Venous Thromboembolism Prophylaxis as a Proof of Concept by Carlton Moore, G. Cameron Coleman, Jamison Chang, Max Nagle and May-Britt Sten in American Journal of Medical Quality
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a grant from the University of North Carolina School of Medicine Institute for Healthcare Quality Improvement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.