
Abstract
The authors tested the efficacy of an integrated approach to improving patient experience and physician burnout using a 24-week online training program coupled with a physician engagement strategy. Physicians from different disciplines were randomized to intervention (n = 30) and control (n = 33) groups. Patient experience, physician burnout, and satisfaction data were assessed using patient and provider surveys. Comparisons were made pre and post intervention, and between the groups. Intervention group mean scores increased (+1.40 points) while control group scores dropped (−0.11 points; P = .039). Scores on physician burnout surveys for the intervention group improved in all areas and changes in 2 domains were statistically significant. In all, 73.5% of physicians felt the program was effective. This integrated intervention enhanced patient experience scores and positively affected physicians’ level of burnout, and physicians believed this exercise was useful.
Physicians need to communicate effectively to provide high-quality care and to have a positive influence on patient experience. In a survey of orthopedic surgeons, 75% believed they were communicating satisfactorily with their patients while only 21% of their patients reported a satisfactory level of communication with that physician. 1 When a patient is included in his/her health care decision, research demonstrates superior outcomes and a reduction in cost of care, and a weakness in communication acts as a hindrance to the patient experience. 2 Prior studies also reveal that effective communication improves the patient experience and potentially reduces physician burnout.3,4
Physicians around the world are experiencing higher rates of burnout—a common syndrome that includes emotional exhaustion, depersonalization (detachment from patients), and low personal accomplishment, which can have a negative impact on patient care. 5 Burnout commonly leads to suicidal ideation, marital and family problems, exhaustion and insomnia, and increased use of drugs and alcohol. 6 According to the 2016 Survey of America’s Physicians, 54% of physicians rate their morale as somewhat or very negative and 49% of physicians often or always experience feelings of burnout. 7 Reasons for burnout cited include changes in the health care landscape, increased paperwork (decreasing allotted physician time in patient encounters), other time constraints, decreases in reimbursements, and adherence to an increased number of quality metrics, all of which interfere with physicians’ ability to practice in ways they find fulfilling. 8 Physician burnout increases medical errors, decreases patient satisfaction scores, increases staff turnover, and raises the cost of care delivered.9-11 Research suggests that an improvement in physician burnout will improve the patient and physician experience. 12
The investigator team conducted a study using an online physician training program, called The Clinician Experience Project (Practicing Excellence.com, San Diego, California). This tool combines a set of web-based learning modules with coaching tips to promote a patient-centered experience and emphasizes the importance of physician skill sharing with a strong focus on physicians’ use of empathy, superior nonverbal communication, teach-back, and improving patient adherence. Lessons, reminders, tips, and inspirational videos aimed at physician behavior and attitude are grouped together into bundles referred to as “projects,” each with its own focus, such as building patient confidence, explaining a diagnosis, and the power of touch. Each video bundle contains a module video paired with tip videos. Videos provide a general overview of a topic including its relevance, insightful information from scientific studies, tactics for addressing an issue, key takeaway information, and suggestions for how to implement best practices during patient encounters. Modules are paired with quizzes to evaluate physicians’ comprehension of the material in the video, and each quiz is linked to continuing medical education credit. After completing the module portion of the project, users are encouraged to continue watching tip videos pertaining to the same focus. Tips videos review the main points and guidelines mentioned in the modules. Included in each project is a supplementary pdf file containing a summary and templates of conversations for physicians to have with their patients. This platform encourages utilization through gamification and assignment of points for participation, module completion, and commenting, in order to foster an online community.
The investigator team undertook a randomized controlled trial to evaluate the efficacy of integrating this online physician training program with a social physician engagement strategy to improve patient experience and physician well-being.
Methods
Participants
Physicians were selected from Northwell Health Physician Partners—the employed medical group of Northwell Health, a large integrated health care system in the New York City metropolitan area. Volunteers from 4 clinical disciplines (medicine, cardiology, obstetrics/gynecology, and surgery), whose patient experience scores were in the middle tertile for their discipline at the study institution based on their national rank, relative to a benchmark established by the survey vendor, were included. Volunteers were placed into 2 groups by stratified randomization—stratified based on sex, age group, and medical specialty. Those in the intervention group were asked to complete a pre-participation survey, the Maslach Burnout Inventory (MBI).
To increase physician engagement, “physician champions” (PCs) were selected by the investigators prior to the implementation of the intervention. PCs were physicians in the top tertile of their respective clinical discipline who were chosen to lead biweekly discussions via conference calls about the online tool with their respective specialty participants in order to provide an interactive component and foster community. PCs were given a guide to lead sessions and were taught facilitation techniques, including the importance of the “learn-do-share” model.
This study was reviewed and approved by the North-well Health institutional review board.
Learn-Do-Share Intervention
The investigator team tailored a curriculum, called a “learning path,” to serve as a continuum of education for the 24-week program. The majority of projects came from the learning tracks titled “Outpatient Patient-Centeredness” and “Clinician Well-Being.” Each week, for the duration of the intervention, new bundles were assigned and participants were alerted to their newly assigned bundles through weekly emails. Although projects were assigned weekly, users had access to the entire stock of projects and were able to engage at their own pace.
Throughout the study, participants and PCs had biweekly conference calls. Discussions included opinions on the topics of the videos and a review of the tips and lessons taught in the set previously assigned. Participants also were encouraged to share stories about their implementation of the tips and tricks suggested by the videos.
To promote socialization, interest, and as part of an engagement strategy, investigators incentivized participants from each specialty who earned the most points from the online tool every 2 weeks with a complimentary breakfast for them and their office staff. Social gatherings on a monthly basis allowed physicians to discuss their thoughts in an informal setting, and at the completion of the 24-week program, a graduation celebration took place for all of the participants and PCs.
A “learn-do-share” approach was used whereby physicians were to learn from engaging in the module and tips videos, do by integrating the suggested tips into clinical encounters, and share their discoveries and integration success stories during the biweekly conference calls, on the comment section of the web-based tool, and at the in-person sessions.
Physicians’ patient experience scores were measured throughout the study period and an MBI was readministered to the intervention group to assess for improvement. The investigators had the ability to review the participants’ log-on activity to confirm active participation throughout the 24 weeks.
Data Collection
Baseline patient experience data were retrieved from surveys administered by a third-party vendor (Press Ganey Associates, Inc., South Bend, Indiana) from January 1 through December 31, 2015. Surveys were sent via a multimodal approach—email and US Postal Service (USPS) mail. Twenty-five surveys were sent at random by USPS mail per month, and all patients who had an email address on file received a survey via email. Internally, surveys were examined to ensure there were no duplicates. Patients were not asked to complete a survey more than once per 3 months. 13 The survey asked the patient to rate the physician on 10 care provider measures (see supplementary Appendix A) using a 5-point Likert-type scale (1 = very poor, 5 = very good). 13 Patient experience was summarized as the care provider section mean score (Patient Experience Score) and external rank (Patient Experience Rank), which was based on comparison against the vendor’s national database. Because of the nature of the learn-do-share model used, post patient experience data were examined from service dates during the 6-month period while the investigation was taking place to see how the study physicians were evolving in their practice as a result of participation in the intervention (May 8 through November 8, 2017).
MBI is a validated tool that determines specific measures of burnout—emotional exhaustion, burnout, depersonalization, and personal achievement. 6 Each measure uses a combination of different questions on a 7-point Likert-type scale, from 0 to 6, that results in a score that can be interpreted into one of 3 categories: low-level burnout, moderate burnout, or high-level burnout. Lower scores in the emotional exhaustion, burnout, and depersonalization categories correspond with lower levels of burnout, and a low score in the personal achievement category corresponds with a higher level of burnout. MBI scores were calculated for the intervention group before the intervention was introduced and after the intervention was complete.
A qualitative survey consisting of 5 questions was administered to the intervention group to establish participant self-efficacy, perceived effectiveness of the project, as well as their potentially enhanced connection to each other and their patients.
Statistical Method
Physicians’ care provider (CP) mean scores and external ranks were collected using patient experience surveys at baseline and during the 6-month intervention.
The Mann-Whitney test was utilized for mean differences in patient experience score comparisons between the intervention and control group before and after the intervention. The Wilcoxon signed-rank test was utilized for paired analysis for CP mean and rank differences in the intervention group, as well as for each MBI section. The differences were computed as measurements taken before and after the intervention. Results were considered statistically significant if P < .05. Analysis was conducted using SAS version 9.4 (SAS Institute, Inc., Cary, North Carolina). The participants and PCs involved in the intervention also completed a 5-question survey about their perceptions of the effectiveness of the program.
Results
Demographics
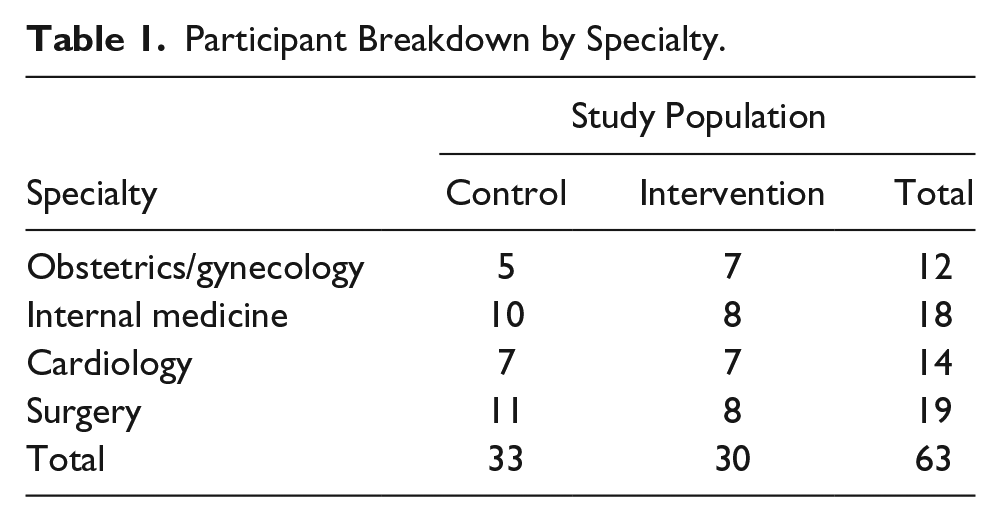
There were a total of 63 participants: 30 in the intervention group and 33 in the control group (Table 1). Participants were randomized based on sex, age group, and medical specialty (Table 2).
Participant Breakdown by Specialty.
Randomized Participants.
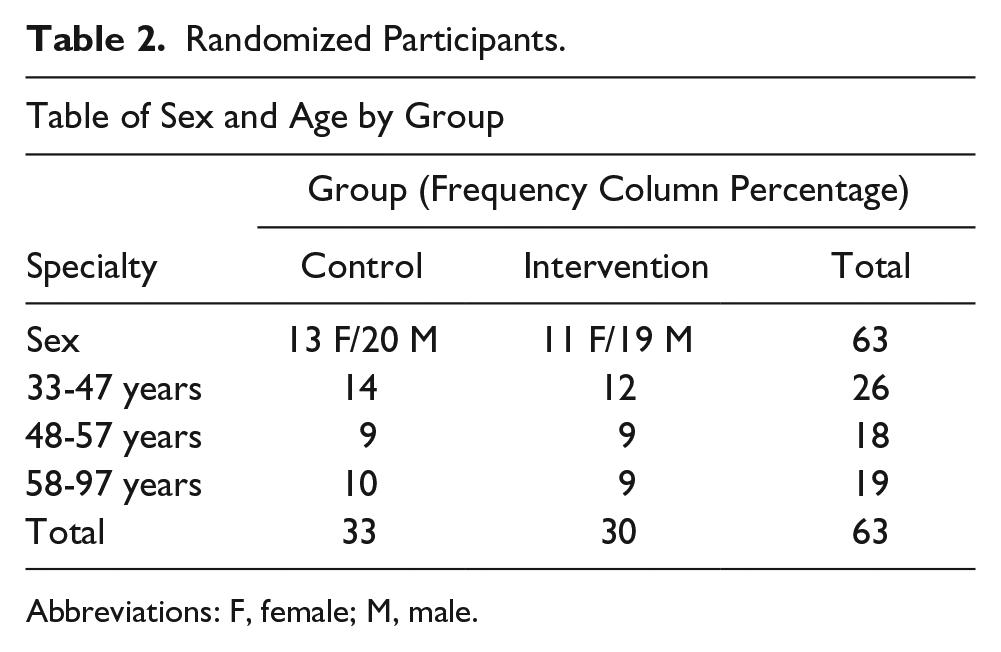
Abbreviations: F, female; M, male.
Patient Experience Mean Changes
The number of surveys received differed by physician and ranged from 6 to 210, with a mean of 74 for the entire group, and the number of surveys received for the intervention group differed by physician and ranged from 8 to 113, with a mean of 51. The mean CP score for the intervention group increased by 1.40 (P = .0009) between pre and post intervention (Table 3). The mean CP score for the control group dropped −0.11 over the same time period. The intervention group had a significantly greater improvement in CP patient experience scores compared to control group (median [Q1, Q3] = 1.60 [0.40, 2.40] vs 0.60 [−1.30, 1.90], P < .039). However, there was no statistically significant difference in change in Patient Experience Ranks between the 2 groups (median [Q1, Q3] = 4.0 [−27.0, 13.0] vs −13.0 [−36.0, 12.0], P < .346). For the intervention group, the average CP score after 6 months was significantly higher than baseline (median [Q1, Q3] = 96.5 [94.6, 97.3] vs 94.8 [94.2, 95.3], P < .0009). However, there was no statistically significant difference in change in rank between baseline and 6 months (median [Q1, Q3] = 75.0 [43.0, 94.0] vs 76.5 [60.0, 85.0], P < .800; Table 3).
Care Provider Patient Experience Mean Score and Rank Compared Pre and Post Intervention, Compared with Control.
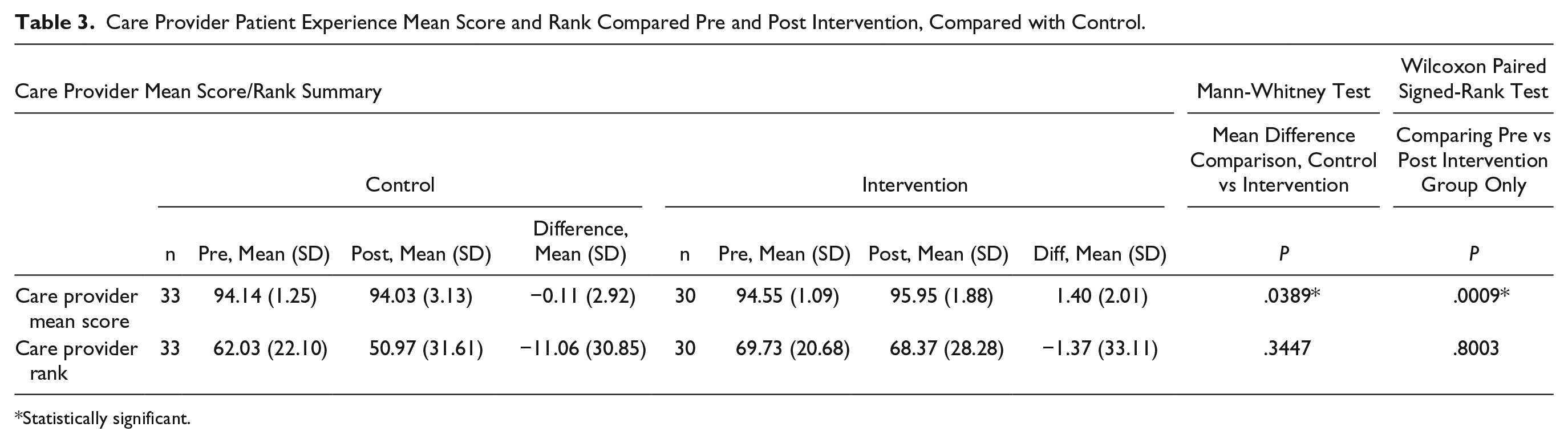
Statistically significant.
MBI
Four measures on the MBI were compared, 2 of which were statistically significant. Depersonalization score went from 11.24 to 8.81, and the mean depersonalization score measured after 6 months was significantly lower than baseline (median [Q1, Q3] = 7.5 [2.5, 13.5] vs 12.0 [7.0, 16.0], P < .023). Personal Achievement score increased (P = .0007), and Burnout score decreased (P = .0504; Table 4).
Maslach Burnout Inventory (MBI) per Section Compared Pre and Post Intervention.
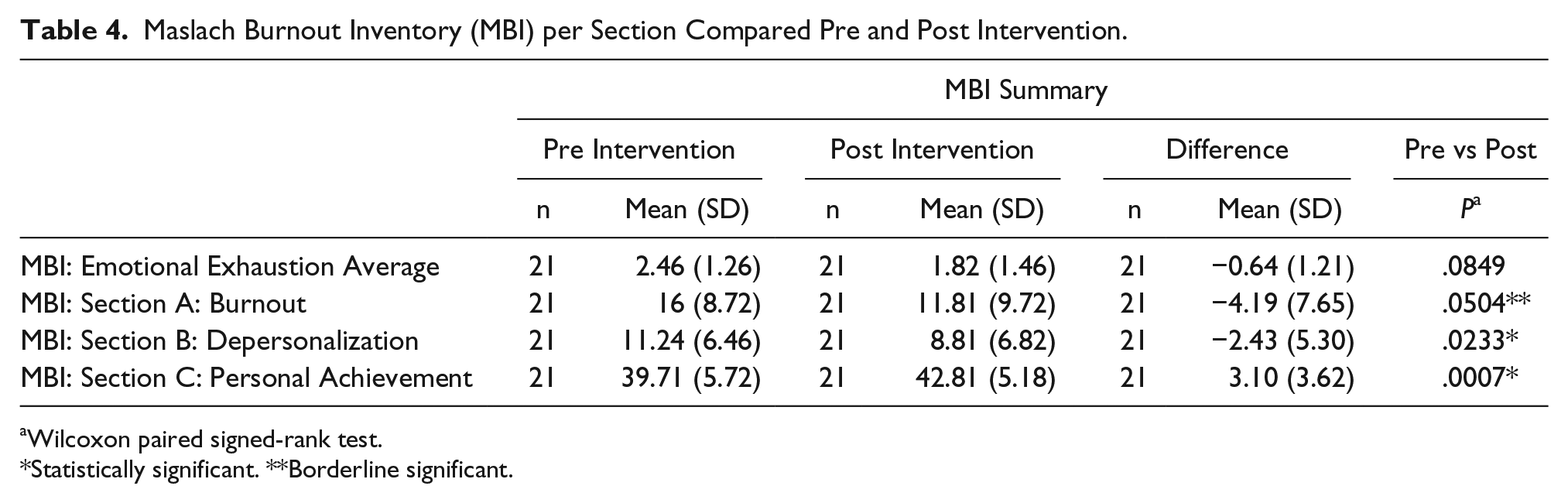
Wilcoxon paired signed-rank test.
Statistically significant. **Borderline significant.
Qualitative Survey
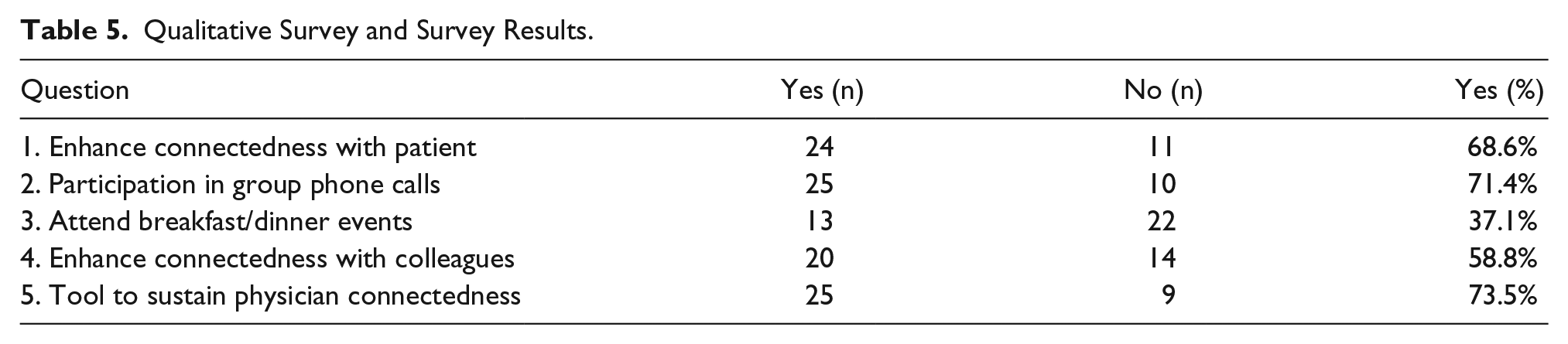
The survey had 35 respondents—33 respondents answered every question and 2 abstained from one question each (Table 5).
Qualitative Survey and Survey Results.
Social Discussions
Discussions maintained an educational direction, but offered a community component—increasing social interactions among physicians. Physicians commented that a tool that included a socialization component would be conducive to sustaining physician connectedness and can counter the isolation of a physician residing in an office. During these sessions, physicians remarked that this tool refueled their passion in medicine and, after completing the intervention, physicians commented that they remembered why they were interested in medicine in the first place.
Discussion
This study demonstrated a statistically significant difference in improvement of patient experience scores between the intervention and control groups. Increased patient experience scores may be a product of physician satisfaction and improved communication likely increased as a byproduct of participation in the intervention.3,12,14 Previous research demonstrates that communication skills training courses improve patient satisfaction, similarly to the present study. 3 Studies confirm that good provider communication is associated with better outcomes. In a study that assessed a communication course, similar to the present study model, increased scores for physician communication and improvements in self-perceptions of empathy and burnout were all associated with physicians who enrolled in a course compared to physicians who did not.3,4 Programs aimed at improving physician burnout have shown improvements in patient satisfaction. 12 The present study also shows the generalizability of an intervention across 4 clinical disciplines—medicine, cardiology, obstetrics/gynecology, and surgery.
Patient experience data were collected during the intervention period, not after completion of the program. As a result, changes in patient or provider experience that took time to develop would have been underestimated. There were not a minimum number of responses to surveys per physician used in the study; however, 85% of physicians had more than 30 surveys returned. Results were not weighted based on the number of surveys returned; each physician’s scores contributed equally, and the median is reported instead of the mean of the group to minimize the potential impact of large changes in the scores of any one physician.
MBI scores among the intervention group improved in all areas, and 2 areas were statistically significant—depersonalization and personal achievement. Deper-sonalization occurs when physicians become indifferent, unmoved, and unsympathetic to patients or colleagues. Personal achievement relates to the innate feeling of success that physicians feel during memorable moments of practicing the art of medicine. Studies suggest that a physician experiencing burnout may deliver a poorer quality of care and have difficulty when relating to patients, which is why programs aimed at improving burnout are so important. 8 When improvements in burnout occur, the quality of care delivered improves. 12 Multidisciplinary approaches, including courses focused on patient communication and stress management, likely will help manage burnout while improving the patient experience.
This study included group sessions. Group sessions that review material with providers on the patient-centered approach and programs that develop a work-related social support are an effective strategy to reduce stress and burnout symptoms.5,12 The results of the qualitative survey suggest that physicians felt this tool enhanced relationships and connectedness with patients, colleagues, and physicians, likely contributing to the improved MBI. The comment section in the online tool provided a means to review the material in the modules and a method to connect physicians and spark conversation. As seen in the literature and observed in this study, decreased professional isolation through discussion groups decreases the mental burden felt by physicians. 15
Increased time constraints force decreased communication, which ultimately decreases patient satisfaction, which may lead to increases in physician burnout.12,14 The intervention has the potential to craft a community of learning and sustain practice by allowing users to return to modules over time. The learn-do-share approach coupled with the ability to communicate, connect, and engage with a group of physicians may contribute to an increase in positive patient experience, as well as the physician experience. The online nature of the tool allows for convenience and flexibility.
Limitations and Considerations
There were several limitations to the study. The sample size was only 63 participants, but large enough to yield statistically significant results. The size of the sample did not allow the investigator team to assess all specialties. The MBI was not assessed or reassessed in the control group. The team did not trend the patient experience scores and MBI scores to assess if this program offers sustainable results over time. Because of the integrated model used—the online tool with a physician socialization engagement strategy—the team is unable to assess which portion affected the results more strongly.
Conclusions
The online intervention, coupled with the learn-do-share collaborative effort, enhanced care provider patient experience scores of physicians who participated in the projects and also had a positive impact on MBI measures of depersonalization and personal achievement. Participating physicians reported a high level of self-efficacy and belief in the effectiveness of this integrated intervention to improve physician–patient connectedness and to sustain inter-physician connectedness across all specialties.
Supplemental Material
Appendix_A – Supplemental material for The Use of Online Physician Training Can Improve Patient Experience and Physician Burnout
Supplemental material, Appendix_A for The Use of Online Physician Training Can Improve Patient Experience and Physician Burnout by Susan Congiusta, Eric M. Ascher, Seungjun Ahn and Ira S. Nash in American Journal of Medical Quality
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.