
Abstract
Veterans are increasingly eligible for non-VA care through the Veteran Health Administration (VA) Maintaining Internal Systems and Strengthening Integrated Outside Networks Act while maintaining care in the VA. Continuity of care is challenging when delivered across multiple systems resulting in avoidable complications. The Community Hospital Transitions Program (CHTP) intervention was developed to address challenges veterans face post non-VA hospitalization. Propensity score–matched analysis was used to compare outcomes between 334 intervention and matched control patients who were discharged from non-VA hospitals. Veterans in CHTP were more likely than matched controls to receive a follow-up appointment within 14 days (mean: 0.43 vs 0.34, P < .05) and 30 days (mean: 0.62 vs 0.50, P < .05). There were no significant differences in 30-day readmissions or 30-day emergency department visits. CHTP veterans received timely follow-up care post discharge in VA facilities. Providing quality care to dual-use veterans is dependent on coordinated transitional care.
The Veteran Health Administration (VA) is committed to providing access to high-quality care in a timely and efficient manner for the 9 million veterans enrolled in the VA health system. However, the VA experienced challenges because of an increase in demand for care and inadequate provider networks. 1 In an effort to improve access to care, Congress passed the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks Act (MISSION Act) in 2018 to allow veterans more choices for approved non-VA care. 2 It is expected that 40% of veterans will be eligible for non-VA care compared to the 8% who were eligible before the MISSION Act. 2
Expanded access to non-VA care presents care coordination challenges for both VA and non-VA hospitals. Research has shown that postdischarge transitional care is especially challenging for dual-use veterans because of a lack of standardized processes for identifying them, transferring medical records, obtaining medications at a non-VA pharmacy, and reestablishing VA care. 3 Strategies for effectively coordinating care in this population have not kept pace, resulting in adverse events for dual-use veterans.4-10
Moreover, prior research showed that establishing a primary care medical home is linked to improved health outcomes. 11 Interventions that facilitated the transition of patients from hospitals to home found that patients had improved health outcomes and reduced service utilization.12-14 Patients had fewer adverse events when they received comprehensive postdischarge care such as instructions on medication use and self-care, as well as symptom recognition and management, and reminders to attend follow-up appointments.14,15
Although researchers identified the components of effective transitional care, 16 barriers to coordinated care still exist. The communication and collaboration needed to provide coordinated care across health care delivery systems are difficult because of the lack of standardized approaches between systems.17,18 Consequently, follow-up care may be delayed or missed altogether.
Earlier research showed that VA and non-VA clinicians, staff, and veteran patients experienced care coordination challenges post non-VA hospital discharge because of a fragmented process. For example, VA primary care providers (PCPs) mentioned not having a complete picture of the care provided to patients in the non-VA hospital because of delayed receipt of medical records. 3 This previous work resulted in suggestions to improve the current transition process for veterans post non-VA hospital discharge, which informed the development of the Community Hospital Transitions Program (CHTP)—a quality improvement intervention. CHTP was designed to improve transitions of care and address barriers to transitional care when veterans were discharged from non-VA hospitals and returned to VA primary care, their medical home, for follow-up care.
The purpose of this pilot study was to evaluate the impact of the nurse-led CHTP relative to matched controls on veterans’ receipt of 14- and 30-day VA primary care follow-up, as well as 30-day readmission rate and 30-day ED utilization, post non-VA hospital discharge.
Methods
During the pre-implementation phase, the research team identified barriers and facilitators to transitioning patients from non-VA hospitals to VA primary care. Guided by the Practical, Robust, Implementation and Sustainability Model, the team conducted a qualitative assessment with VA and non-VA stakeholders as well as veterans. The protocol is described elsewhere.19,20 This pre-implementation assessment of the transition process showed that transitions of care for veterans were challenging and fragmented. Stakeholders provided suggestions to improve the current process, which were incorporated into findings 3 from the pre-implementation assessment and existing best practices, 16 to develop a transitional care intervention.
Setting
The Rocky Mountain Regional VA Medical Center (RMR VAMC) is in Aurora, Colorado, and is one of the 2 tertiary VA hospital facilities in Veterans Integrated Service Network (VISN) 19. VISN 19 is one of the largest geographic VISNs in the country, serving veterans in Wyoming, Montana, Utah, and Colorado. In 2017/2018, approximately 3968 veterans with established VA primary care at RMR VAMC were hospitalized in a non-VA hospital setting.
Patients
Veterans who were discharged from non-VA hospitals between October 1, 2017, and July 31, 2018, were referred to the CHTP nurse for episodic transitional care. Patients were asked verbally by the CHTP nurse to participate in the program. Patients were excluded if they were discharged to another inpatient facility (eg, post-acute care, hospice, skilled nursing facility), had confirmed case management elsewhere (eg, had an oncology social worker), lived out of the state of Colorado, were homeless, died, and were observation-only patients (no discharge report). Most patients were discharged to another facility with a clinical setting and were followed by clinicians. For CHTP, focusing on patients discharged home allowed the potential to assist patients with higher care coordination needs immediately following hospital discharge while narrowing the reach for the CHTP pilot intervention to be feasible. Some patients were lost to follow-up post enrollment in the intervention. The Colorado Multiple Institutional Review Board (COMIRB Protocol 15-1321) and the Veterans Affairs Health Services Research and Development ethics review board deemed this a quality improvement project on October 21, 2015.
Intervention
CHTP is a nurse-led care coordination intervention that includes pre and post non-VA hospital discharge components. 19 Non-VA hospitals in the Denver Metro area, Pueblo, Colorado, and VA primary care teams were informed about the implementation of this program. A full-time CHTP registered nurse enrolled veterans who were referred to CHTP from the non-VA hospitals when they were hospitalized or recently discharged. Non-VA hospitals were asked to notify the CHTP nurse as soon as possible when a veteran was admitted to their hospitals to ensure patients had coordinated care post discharge. If the CHTP nurse was not notified of the veteran admission, the veteran would not be enrolled in the program because there is no timely way for the CHTP nurse to learn about this patient’s non-VA care. Timeliness of notification was an essential component of implementation.
Once the CHTP nurse was notified of a veteran admission, medical records were requested to ensure that VA PCPs were aware of their patient’s community hospitalization. The CHTP nurse delivered VA providers a structured discharge summary by directly uploading the discharge summary and the structured summary to the VA electronic medical record system. Finally, the CHTP nurse reached out to the patient who was still hospitalized or within 72 hours of discharge. 16 This was to assess the patient’s symptoms, discuss any medication changes, discuss and verify the discharge follow-up plan, and provide comprehensive self-management education. The CHTP nurse scheduled follow-up appointments for recently discharged veterans with the goal of having patients seen within 14 days of community hospital discharge.
The CHTP nurse remained a point of contact for community hospital providers, veterans, and the VA primary care team until the point of handoff. All intervention components and any additional notes were thoroughly recorded in the CHTP database. Figure 1 describes the CHTP intervention core components. The research team developed a unique database with interactive interfaces, along with visual dashboards, to capture specific inputs related to the intervention core components. The database visual dashboards provide quick access to a program participant’s information for the CHTP nurse, help assess intervention fidelity among non-VA hospitals, and inform communication with stakeholders.
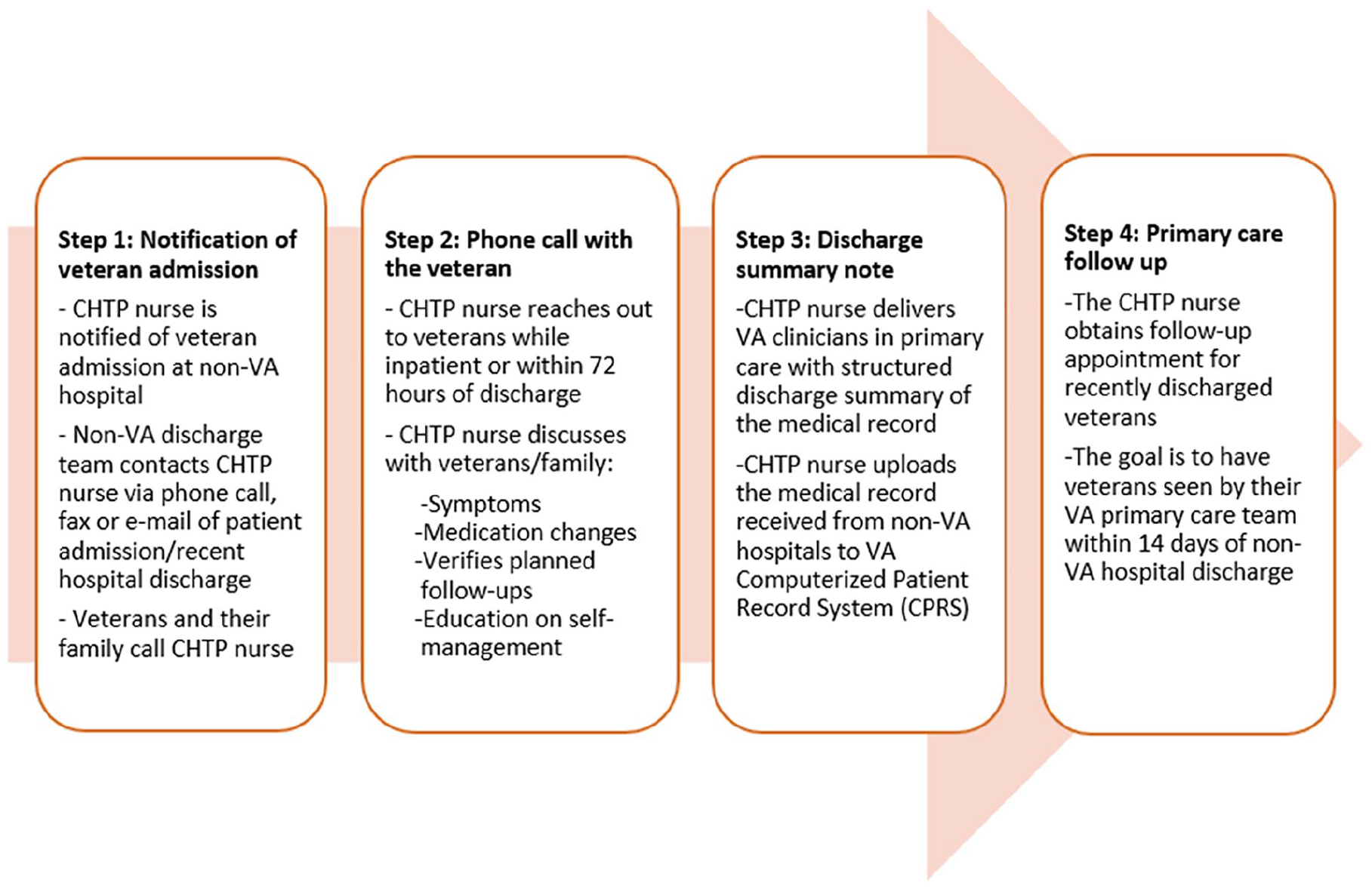
Community Hospital Transitions Program core components.
The team also instituted health system changes to support the CHTP nurse role and to improve communication between health care systems in delivering the 4 core components. The system changes included (1) a secure phone line for community hospitals to notify the CHTP nurse when a veteran was admitted so that early discharge planning could begin, (2) a secure fax line for community providers to submit discharge summaries/electronic medical records, and (3) a letter to the veteran introducing CHTP along with a Veteran Care card. The Veteran Care card identified the Veteran’s VA care team, provided CHTP nurse contact information, and a process for VA notification information of emergency and nonemergency visits. These systems streamlined the notification process for non-VA hospitals, veterans, and the CHTP nurse.
Measures and Statistical Analysis
In descriptive analyses, demographic and clinical characteristics were compared between the CHTP intervention group and the propensity-matched control group created for this pilot study. Using VA claim data, a control group was selected from veterans who had an inpatient visit in a non-VA hospital in the RMR VAMC area between October 1, 2017, and July 31, 2018, and were discharged to home or self-care but did not receive the CHTP intervention. Patient characteristics and Elixhauser comorbidity variables between the 2 groups were compared using χ2 tests for categorical variables and Mann-Whitney-Wilcoxon nonparametric tests for continuous variables. There were no significant differences between the 2 groups for most of the variables. Propensity score matching was used to reduce the difference between CHTP and control group patients prior to outcome comparisons. Propensity score matching also helped reduce selection bias given that patients were not randomly selected to receive the intervention. The 2 groups were matched on age, sex, Elixhauser comorbidity index, and number of hospitalizations and primary care visits in the past year.
Propensity matching was conducted using the nearest neighbor method. The matched cohort was checked by assessing the propensity score balance between control and intervention groups, as well as the standardized differences of the matched variables. The absolute standardized difference was <10%, commonly considered adequate balance. After matching, all covariates showed adequate balance except for age, pulmonary circulation disorder, and number of VA primary care visits in the past year. The team included age, Elixhauser comorbidity score, and number of VA primary care visits in the past year in the outcome model. Race and urban/rural location were not used to estimate the propensity to receive CHTP care because of missingness. These 2 variables also were included in the outcome model. This was a non–intention-to-treat analysis and controlling for confounders using propensity score matching is an appropriate approach.
The primary outcomes of interest were (1) completed follow-up appointment within 14 and 30 days of discharge; (2) rate of 30-day hospital readmission; and (3) rate of 30-day emergency department (ED) admission. To account for correlations between outcomes, the research team fit joint survival models with shared frailty simultaneously for ED visit, rehospitalization, and VA primary care visit. To deal with the missing values for race and urban/rural locations, the joint models were fitted using the Markov chain Monte Carlo method. Survival models were assumed to have proportional hazard, with baseline risk function of Weibull distribution for all outcomes. Covariates included in the outcome model were race (white/nonwhite), urban (urban, rural/high rural), Elixhauser comorbidity score, age, and number of VA primary care visits in the past year. The joint model was fit separately for VA primary care visits within 14 days and 30 days of discharge. The secondary outcome of interest was to describe all-cause mortality outcomes between the intervention and control groups within 30, 60, and 90 days following hospital discharge. Unfortunately, there were not enough mortality events to fit a survival model.
Results
A total of 334 Veterans completed the CHTP intervention core components from October 1, 2017, to July 31, 2018. The average age of the intervention cohort was 66.6 years. The majority of participants were white (94%). Baseline demographic, health care utilization, and comorbidities of the intervention and control groups were comparable (Table 1). A total of 1264 referrals were received from non-VA hospitals. Of those, 68% were excluded for the following reasons: 35% were discharged to another inpatient facility (eg, post-acute care, hospice, skilled nursing facility), 12% died, 9% lived out of the state of Colorado, 7% had confirmed case management elsewhere (eg, had an oncology social worker), 7% were homeless, and 6% were observation-only patients (no discharge report). Eighteen percent of veterans were lost to follow-up post enrollment in the CHTP intervention. Supplementary online Appendix 1 shows a flow diagram of enrolled and excluded veterans in CHTP program.
Baseline Characteristics of Community Hospital Transitions Program Participants and Matched Reference Hospitalizations.
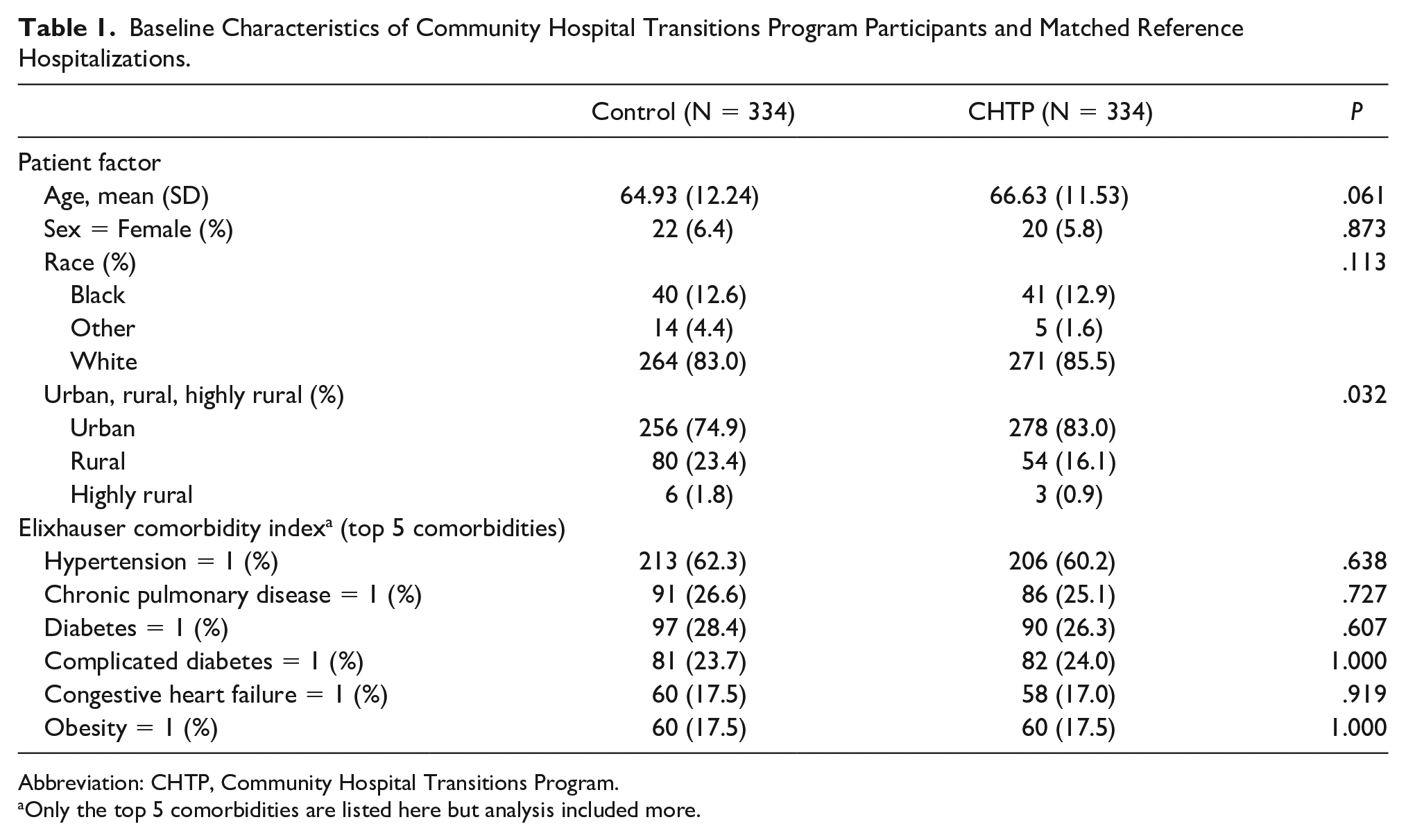
Abbreviation: CHTP, Community Hospital Transitions Program.
Only the top 5 comorbidities are listed here but analysis included more.
CHTP Intervention Implementation
The CHTP nurse received notifications from 27 non-VA hospitals about veterans’ admissions through the VA bed management list, a community hospital staff call or fax, or a veteran or family member call about a recent hospitalization. The CHTP nurse called 57% of patients within 72 hours of discharge from the hospital; the CHTP nurse contacted 36% of them before hospital discharge. On average, the CHTP nurse spoke with the majority of patients (82%) regarding postdischarge care within 14 days of discharge. This ranged from speaking to patients while they were still hospitalized to before the patient’s primary care appointment in the VA. All of these intervention activities were recorded in real time in the program database by the CHTP nurse.
The most frequent CHTP nurse intervention focused on veteran education about the program, what to do when hospitalized at non-VA hospitals, and identifying themselves as a veteran when receiving care in the community. The CHTP nurse educated patients about postdischarge self-management including medication management and the need for VA primary care follow-up appointments post non-VA hospital discharge (Table 2).
Intervention Education With Veterans by the Community Hospital Transitions Program Nurse.
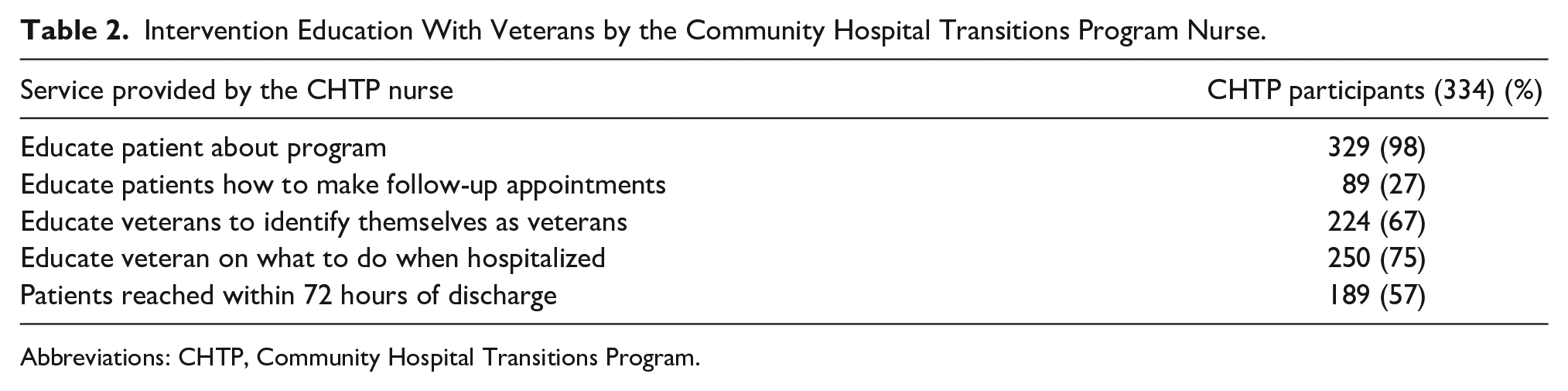
Abbreviations: CHTP, Community Hospital Transitions Program.
Outcomes
As shown in Table 3, event rates for the matched CHTP and control groups showed that veterans enrolled in CHTP were significantly more likely than matched controls to receive a follow-up appointment within 14 days (mean: intervention 0.43 vs control 0.34, P < .05) and 30 days (mean: intervention 0.62 vs control 0.50, P < .05) post discharge. There were no statistically significant differences between the 2 groups in 30-day readmission or 30-day ED visit rates post non-VA hospital discharge.
Community Hospital Transitions Program Outcomes.
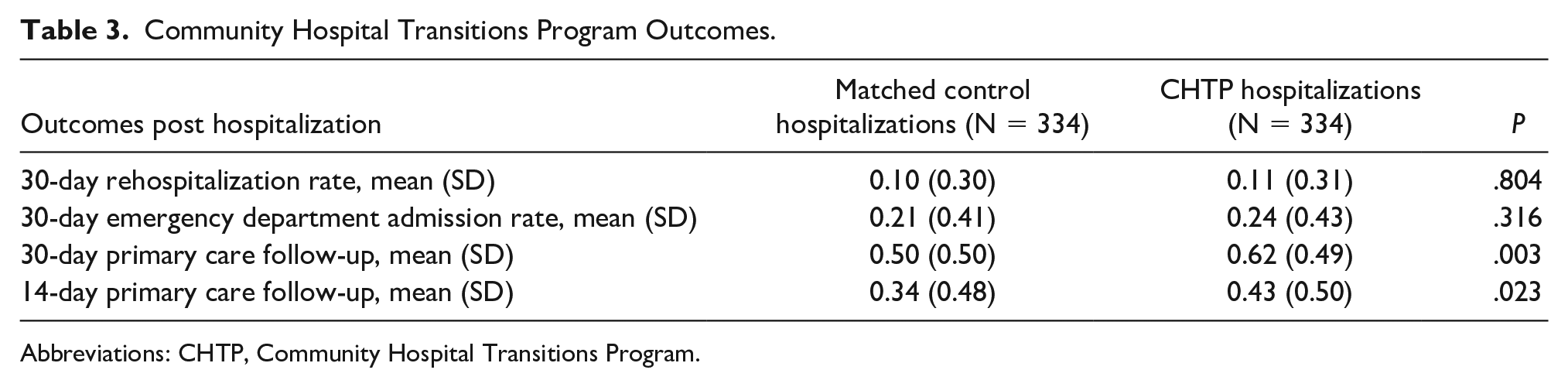
Abbreviations: CHTP, Community Hospital Transitions Program.
Based on the joint survival model, compared to the matched control group, veterans discharged from a non-VA hospital who received CHTP care had a significantly higher probability of follow-up with VA primary care within 30 days of discharge (Hazard ratio: 1.30; highest posterior density interval: 1.09-1.57). The CHTP intervention had no significant effect on ED visits, rehospitalization within 30 days of discharge, or on a PCP visit within 14 days of discharge (Table 3). Table 4 shows the estimates and intervals of the hazard ratio for CHTP outcomes.
Community Hospital Transitions Program Hazard Ratios and Intervals.

Discussion
Implementation of CHTP, a nurse-led care coordination intervention, resulted in a significant improvement in timely postdischarge follow-up with VA primary care for veterans recently discharged from non-VA hospitals. Outpatient follow-up with appropriate postdischarge providers is crucial for providing ideal transitions. 16 Because of the MISSION Act of 2018, 2 an increasing number of veterans are seeking care outside the VA while also maintaining their VA primary care home. Veterans are given more options to receive care in community settings, increasing dual-use veterans’ need for care coordination. Prior research showed that improved primary care follow-up reduced 30-day hospital readmission rates, cost of care, and reduced ED utilization among other benefits.21,22 To the research team’s knowledge, this pilot study is the first to implement and assess a care coordination program as it relates to multiple non-VA hospitals transitioning veterans back to VA primary care post discharge. Results from CHTP provided insights into intervention components needed to improve transitional care and it could be implemented on a larger scale.
No statistically significant outcome was observed in 30-day hospital readmission rate, 30-day ED utilization rate, or mortality rate. The team speculated that this may be because of 4 main reasons. First, analysis was of only 10 months of pilot data, and long-term outcomes were not assessed. Looking at program outcomes after a longer period of implementation would reflect a greater number of veterans and might allow the outcomes to be better powered. Care coordination programs and the patient-centered medical home literature described that a decrease in 30-day rehospitalizations and ED use were observed after program maturation.11,23 Second, this may have been in part because of the lack of hospitalization or ED utilization data in cases in which the VA did not pay for services. This eliminates a large group of veterans from the intervention and control cohorts. Hence, program impact might not have been captured fully for these veterans because both the intervention and control groups might have had non-VA health care utilization for which the VA did not pay. Third, the program did not stratify patients based on specific risk. CHTP benefits might be increased by focusing care coordination efforts on high-risk dual-use veterans. 24 Future studies will need to include analysis of critical subgroups such as older adults, individuals with history of ≥1 chronic illnesses, mental illness, substance use disorders, and those who reside in rural settings. Fourth, increasing intervention fidelity, such as education on follow-up appointments, might have improved the utilization outcomes observed. Some patient education intervention components were not delivered 100% of the time, possibly creating some gap in outcomes.
Several other nurse-led care coordination programs have established the value of care coordination in improving patient outcomes.23,25,26 The present intervention is unique in that it bridged a gap in care coordination by improving communication between VA and non-VA health care systems. These health care systems usually had different information systems and operating philosophies and required the CHTP nurse to use a multicomponent approach to establish and maintain relationships. Another quality improvement program in the VA, which implemented an intervention to coordinate care with one community hospital and VA primary care, found an increased amount of follow-up with the primary care clinic. 27 Expanding CHTP eligibility criteria for veterans hospitalized in other inpatient settings, such as those discharged to another inpatient facility (eg, post-acute care, hospice) as well as those discharged from psychiatric or substance abuse treatment centers, could help capture a high-risk cohort. Additionally, increasing veteran enrollment rate in the CHTP program by increasing non-VA hospital engagement would capture higher numbers of veterans and might show additional program value.
Limitations
Results from this study have limitations and should be interpreted with additional context. There are several unmeasured confounders in the analysis because of the lack of available data; for example, social determinants of health. Additionally, because of the lack of access to data, veteran patients’ non-VA utilization was not captured in the analysis unless the VA paid for those services. This intervention was conducted in the VA system and results might not be generalizable in non-VA settings. Additionally, this program enrolled veterans who were hospitalized primarily in the Denver metropolitan area hospitals. Expanding the program to include more rural hospitals could provide additional insight into the effectiveness of CHTP in improving patient outcomes. Furthermore, there was loss of follow-up among 18% of veterans following their initial enrollment in the program. This might be because of veterans’ perceptions of the value of CHTP to them, or it is possible that they established care in a non-VA setting and their VA care utilization is not captured in VA data. Last, propensity score matching was conducted to control for overt bias using observed covariates. However, there are hidden biases from confounders not observed in the data that cannot be controlled by propensity score adjustments. Future research should include these variables, non-VA care data (VA paid or otherwise), other approaches to control for hidden biases such as an instrumental variable approach, and use feasible, acceptable experiment designs such as stepped-wedge, cluster-randomized, and mixed-methods approaches to better understand the reasons for the results observed. Finally, having a dedicated nurse to coordinate care might seem costly, but the benefits associated with increased postdischarge follow-up care might offset such costs.
This study also had strengths, including the use of robust data analysis steps to ensure intervention patients were matched on available VA data. This study employed a multidisciplinary team experienced in quality improvement, implementation science, and outcomes evaluation who conducted, analyzed, and interpreted these improvement results.
Conclusion
CHTP holds promise for dual-use veterans who face common barriers to safe transitional care post discharge from a non-VA hospital to their primary care team. CHTP improved veterans’ follow-up with their primary care team. CHTP is being expanded to other VA hospitals with some adaptations for site-specific needs and the research team is actively making efforts to sustain program continuation and sustainability. In the current VA policy environment that allows for increased veteran access to non-VA care, implementing a dedicated program for care coordination should reduce barriers and improve patient outcomes.
Supplemental Material
AJMQ_Appendix_1 – Supplemental material for VA Care Coordination Program Increased Primary Care Visits and Improved Transitional Care for Veterans Post Non-VA Hospital Discharge
Supplemental material, AJMQ_Appendix_1 for VA Care Coordination Program Increased Primary Care Visits and Improved Transitional Care for Veterans Post Non-VA Hospital Discharge by Roman A. Ayele, Wenhui Liu, Carly Rohs, Marina McCreight, Ashlea Mayberry, Heidi Sjoberg, Lynette Kelley, Russell E. Glasgow, Borsika A. Rabin and Catherine Battaglia in American Journal of Medical Quality
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Veterans Affairs Health Services Research and Development—Quality Enhancement Research Initiative (QUE 15-268) grant. The funding body had no role in the design of the study; collection, analysis, and interpretation of the data; or writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.