
Abstract
Youth in residential treatment settings often present with a complex combination of mental and physical health problems. Despite an emerging literature documenting significant associations between mental health and physical health, the relationship between these two areas of functioning has not been systematically examined in youth presenting to residential treatment. This study examines the association between youth psychopathology and physical health problems in a sample of 606 youth entering a large residential treatment program between 2003 and 2010. As a part of the intake process, youth psychopathology symptoms were assessed using the parent-report form of the Child Behavior Checklist, and youth physical health problems were assessed in a medical evaluation by a licensed child health professional. Results indicated that higher levels of youth psychopathology, particularly internalizing problems, were associated with greater risk for physical health problems and more prescription medications. Psychopathology comorbidity was also associated with physical health problems. These findings suggest an interplay between physical and mental health among youth entering residential treatment, highlighting the need for integrated assessment and intervention services that address psychological and medical needs within this population.
The physical health of youth with mental health problems is often overlooked. However, growing evidence suggests that these youth are at increased risk for not only mental health issues but also physical health problems (Nelson et al., 2011; Spady, Schopflocher, Svenson, & Thompson, 2005). Despite an emerging consensus that mental and physical health are associated, research exploring the relationship between mental and physical health among youth is limited. Although much is known about the psychological functioning of youth with serious chronic illnesses (Bennett, 1994; Katon et al., 2007; Lavigne & Faier-Routman, 1992; LeBovidge, Lavigne, Donenberg, & Miller, 2003), less is known about the physical well-being of youth with significant psychopathology. In particular, youth in residential treatment settings have high rates of mental health problems (Duppong Hurley et al., 2009); however, the association between mental health and physical health among this population remains largely unexplored. For example, questions remain about the health implications associated with the presence of pediatric psychopathology, the severity of the symptoms, the type of psychopathology, and the presence of psychological comorbidity. Better understanding of these relationships among youth in residential care—a population with considerable and diverse service needs—could be helpful in identifying youth in need of targeted assessment and intervention to promote overall well-being.
Presence and Severity of Psychopathology and Association With Physical Health
Considerable research among adult and pediatric populations suggests that individuals with significant psychopathology are also at risk for physical health problems. Among adults, multiple studies have linked mental health problems with poor physical health (Felker, Yazel, & Short, 1996; Hays, Marshall, Wang, & Sherbourne, 1994; Holahan et al., 2010; Smith & Ruiz, 2002; Zorrilla et al., 2001). In a review of the literature examining the relationship between mental health and physical health outcomes, Felker and colleagues (1996) found that adults with psychiatric diagnoses had higher rates of medical comorbidity and mortality than those found in the general population. More recently, specific aspects of mental health, such as psychological stress, negative emotions (e.g., anger, hostility), and emotional disorders (e.g., depression, anxiety), have consistently been associated with negative health outcomes in adults such as the development and progression of coronary artery disease (Smith & Ruiz, 2002). Research has also indicated that poor mental health is associated with protracted wound healing in adults (Bosch, Engeland, Cacioppo, & Marucha, 2007; Contrada et al., 2008), potentially due to the decreased immune functioning that has been related to stress and psychiatric diagnoses such as depression (Kiecolt-Glaser & Glaser, 2002; Zorrilla et al., 2001).
A smaller body of literature has also linked the presence of psychopathology with medical problems in youth. For example, in a large-scale Canadian study, Spady and colleagues (2005) found that youth with a variety of behavioral and emotional disorders (e.g., psychotic conditions, depression, hyperactivity) had higher levels of medical comorbidity than comparison youth with no mental health diagnosis. Similarly, studies have reported that the presence of a mental health diagnosis (Spady et al., 2005) and the severity of psychopathology symptoms (Angel & Angel, 1996; Lavigne et al., 1998) are associated with higher levels of medical service utilization among youth. The link between psychopathology and physical health problems might be especially relevant in adolescence, which is a developmental stage frequently characterized by an increase in risky behaviors (e.g., substance use, risky sexual behavior; Steinberg, 2007) and a decrease in key healthy behaviors (e.g., physical activity; Troiano et al., 2008). Along these lines, Brooks, Harris, Thrall, and Woods (2002) found that adolescent mental health symptoms were associated with increased health-risk behaviors such as tobacco use, involvement in physical fights, and sexual activity without using birth control.
Beyond literature establishing a link between psychopathology in general and physical health problems, research has demonstrated a relationship between specific youth mental health diagnoses and medical problems. Studies have found that youth with mental health disorders such as attention-deficit/hyperactivity disorder (ADHD; Cuffe, Moore, & McKeown, 2009), conduct disorder (CD; Pajer, Kazmi, Gardner, & Wang, 2007), depression (Bennett, 1994), and anxiety (Bardone et al., 1998) tend to have worse physical health outcomes than youth without a diagnosed condition. One study revealed that children with ADHD were two times more likely to have asthma and three times more likely to experience headaches than children without ADHD (Cuffe et al., 2009), whereas another study found that adolescent females with CD have significantly worse physical health and fewer healthy behaviors than young females without a mental health diagnosis (Pajer et al., 2007). In a longitudinal study by Bardone and colleagues (1998), diagnoses of CD, depression, and anxiety at age 15 were all independently associated with at least twice as many medical problems at age 21 compared with a group of healthy females, even after controlling for potentially confounding variables (e.g., childhood health, socioeconomic status). These studies highlight the relationship between specific mental health disorders and physical well-being in youth as well as the potential for negative health outcomes to continue into early adulthood if not addressed. Research directly comparing the differences in health status among youth with varying types of psychopathology is needed to identify which types are most strongly associated with physical health.
Psychopathology Comorbidity and Physical Health
In addition to the presence and severity of psychopathology, it is possible that psychopathology comorbidity is an important factor influencing risk for physical health problems. In a review of 12 studies examining medical service utilization in terms of length of stay, cost of care, or resource utilization for adults, it was found that patients with psychiatric comorbidity have an increased risk for nonpsychiatric service utilization when compared with those without comorbid disorders (Zolnierek, 2009). This suggests that psychopathology comorbidity may contribute to physical health risk in adults (or vice versa); however, fewer studies have examined this relationship in youth. One longitudinal study examining children over a period of 20 years suggests that psychiatric comorbidity in youth may be associated with worse physical health in adulthood (Chen et al., 2009). Youth who endorsed comorbid psychiatric symptoms (i.e., Axis I and Axis II disorders) at baseline had significantly worse physical health 20 years later than those who endorsed symptoms from only one disorder and those with no diagnosable symptoms (Chen et al., 2009). The issue of psychopathology comorbidity is particularly relevant to youth in residential treatment settings, where comorbidity is a common challenge; however, the relationship between comorbidity and physical health functioning within this uniquely vulnerable population has not been examined.
The Present Study
Despite a significant literature linking psychopathology and physical health problems, this relationship remains unstudied in the pediatric residential care population. Youth in residential care are an important population to study for several reasons. First, a significant number of youth (approximately 200,000; Child Welfare League of America, 2010) are placed in residential treatment settings in the United States at any given time. Second, this population has high rates of psychopathology and related psychosocial risk factors that could affect physical health risk (Duppong Hurley et al., 2009). Third, youth in residential care settings may have particularly high service needs, for mental health and medical issues (Nelson et al., 2011). Consequently, efforts to better understand the factors associated with health among this population could have a significant impact on long-term health and health service trajectories. Therefore, the present study aims to examine the association between psychopathology and physical health status in a large sample of youth entering residential treatment.
The present study is guided by a conceptual framework proposing that multiple factors may affect the physical health status of youth in residential care (see Nelson et al., 2011, for discussion). Within this framework, demographic factors, the residential placement history of the youth, and psychopathology are all considered possible contributors to youth health status within this population. Demographic factors (such as age, sex) may correlate with psychopathology and physical health status. Similarly, an individual history of residential placement instability (in the form of numerous out-of-home placements or placements with nonparent caregivers) could disrupt appropriate medical care and the establishment of a consistent medical home, increasing the risk for physical health problems. Given the potential contributions of demographic and placement history factors, it is important to control for these variables to better isolate and evaluate the association between psychopathology and health status.
Building on the broader youth mental health–physical health literature, this study focused on three related issues concerning the relationship between psychopathology and physical health status. First, we examined the association between the severity of youth psychopathology symptoms and risk for physical health problems. We hypothesized that the overall severity level of youth psychopathology symptoms would be related to medical status such that higher levels of psychopathology would be associated with higher risk for medical problems and more prescribed medications. Second, we investigated the relationship between different types of psychopathology symptoms (e.g., internalizing vs. externalizing) and physical health status. Based on recent research examining psychopathology and service utilization in a residential sample (Nelson et al., under review), we expected that internalizing problems would be associated with greater risk for medical problems. Third, we examined the association between psychopathology comorbidity and physical health status. We hypothesized that comorbidity would be associated with increased risk for medical problems and more prescription medications. For each hypothesis, we expected that the psychopathology construct of interest would be significant even after controlling for other relevant demographic and placement history factors. Overall, the results of this study are expected to provide insight into the relationship between mental health and physical health among a particularly high-risk and high-need population. These results should be valuable in identifying youth at risk of significant health problems and for targeting assessment and treatment services to youth at high risk.
Method
Participants and Procedures
The participants were 606 youth aged 8 to 18 years (M = 14.6 years) who entered the Boys Town Nebraska Treatment Family Home Program between 2003 and 2010. The Boys Town Nebraska Treatment Family Home Program is a large residential treatment program for youth with a variety of behavioral and emotional issues. Youth are referred to Boys Town from the surrounding areas and from across the country, resulting in a diverse population. The sample was 60.2% male and ethnically diverse (52.6% European American, 19.2% African American, 11.8% Hispanic American, 6.6% Native American, 0.8% Asian/Pacific Islander, and 8.9% multiracial). Data on family income were available for a subset of the sample (n = 146; 24% of the total sample), with 23.3% reporting annual income of less than US$15,000, 46.6% reporting between US$15,000 and US$40,000, and 30.1% reporting more than US$40,000. Approximately, 51% of the sample entered Boys Town directly from the home of their natural parent(s), 10.5% came from an adoptive home or the home of a relative, and the remaining youth came from other out-of-home placements (e.g., detention centers, group homes and shelters, other residential programs).
Data were drawn from a review of electronic records contained in the Boys Town National Database. At the time of intake into the residential treatment program, each youth received a psychological and medical evaluation. As a part of the psychological evaluation, youth caregivers completed the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) as a broadband measure of youth psychopathology symptoms. Only youth whose parent or legal guardian completed the CBCL were included in the current study. Although some youth had CBCL data provided by other relevant adults (e.g., teacher, noncustodial relative, case worker), we did not include these cases because the validity and reliability of these reports are often questionable due to limited contact between the reporter and the youth. Youth included in this study did not differ from those who were excluded on age, t(1,733) = .54, p > .05; sex, χ2(1) = .26, p > .05; ethnicity, χ2(5) = 9.65, p > .05; or the presence of a diagnosed medical condition at intake, χ2(1) = .61, p > .05, suggesting that the current sample is a representative subset of the larger Boys Town population. In addition to the psychological evaluation, youth received a comprehensive medical evaluation by a licensed child health professional (either a physician or a nurse practitioner) at the time of intake. The medical evaluation consisted of a detailed medical history, review of available records, and a physical examination of the youth. Medical information, such as medical diagnoses and medications taken, were recorded at this time. All procedures were approved by the Boys Town Institutional Review Board.
Measures
Youth psychopathology
Youth psychopathology symptoms were assessed using the parent-report version of the CBCL (Achenbach & Rescorla, 2001). The CBCL is a commonly used measure of youth psychopathology with strong reliability and validity data (Nakamura, Ebesutani, Bernstein, & Chorpita, 2009). The CBCL yields a broad Total Problems Scale, as well as the Internalizing Problems Scale, Externalizing Problems Scale, and numerous specific subscales. To correspond more closely with diagnostic categories, the CBCL also yields Diagnostic and Statistical Manual of Mental Disorders (DSM)-related subscale scores, including Affective, Anxiety, ADHD, Oppositional Defiant, and Conduct Problems scores (see Table 1 for means and standard deviations; see Table 2 for correlations between CBCL subscales). As discussed in the results section, CBCL raw scores (with a z score transformation) were used in logistic regression analyses to maximize the interpretability of results.
Means and Descriptive Statistics for CBCL Scales and Subscales.
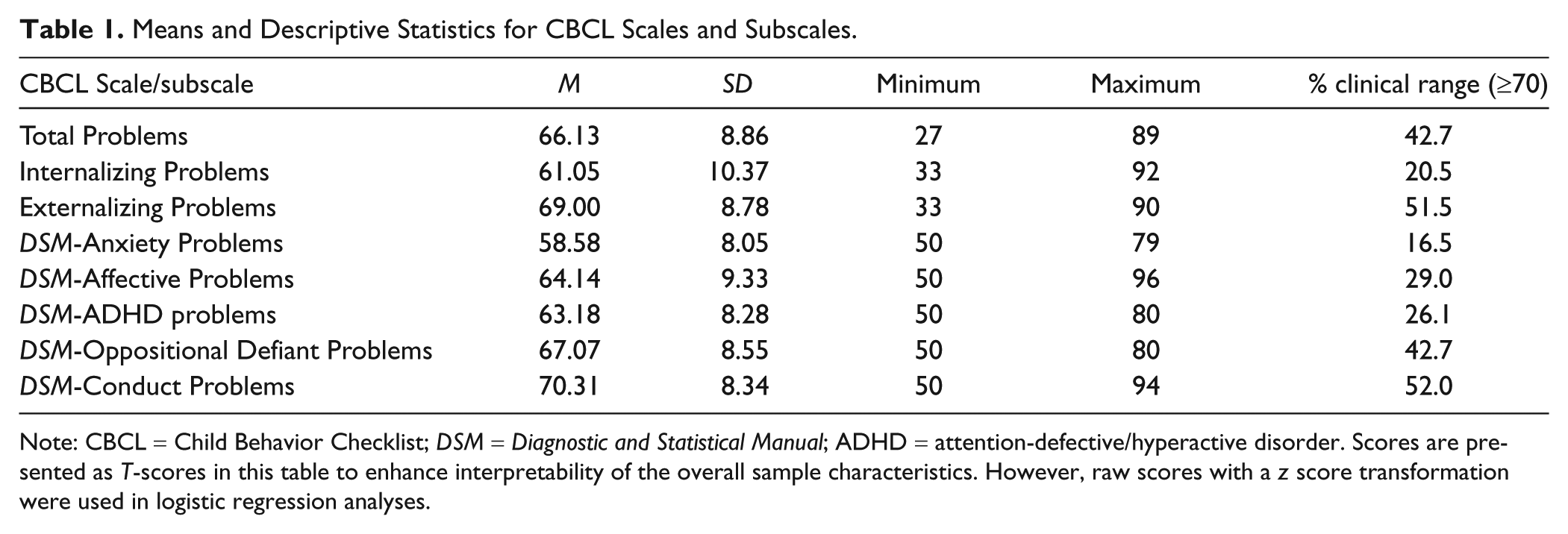
Note: CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual; ADHD = attention-defective/hyperactive disorder. Scores are presented as T-scores in this table to enhance interpretability of the overall sample characteristics. However, raw scores with a z score transformation were used in logistic regression analyses.
Correlations Among CBCL DSM Subscales.
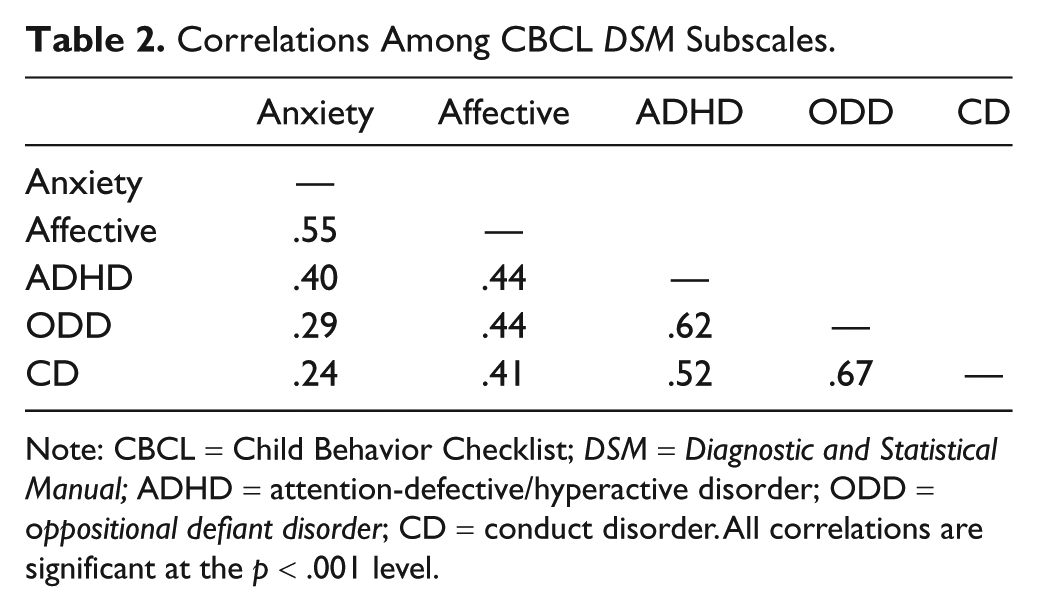
Note: CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual; ADHD = attention-defective/hyperactive disorder; ODD = oppositional defiant disorder; CD = conduct disorder. All correlations are significant at the p < .001 level.
Youth medical diagnosis
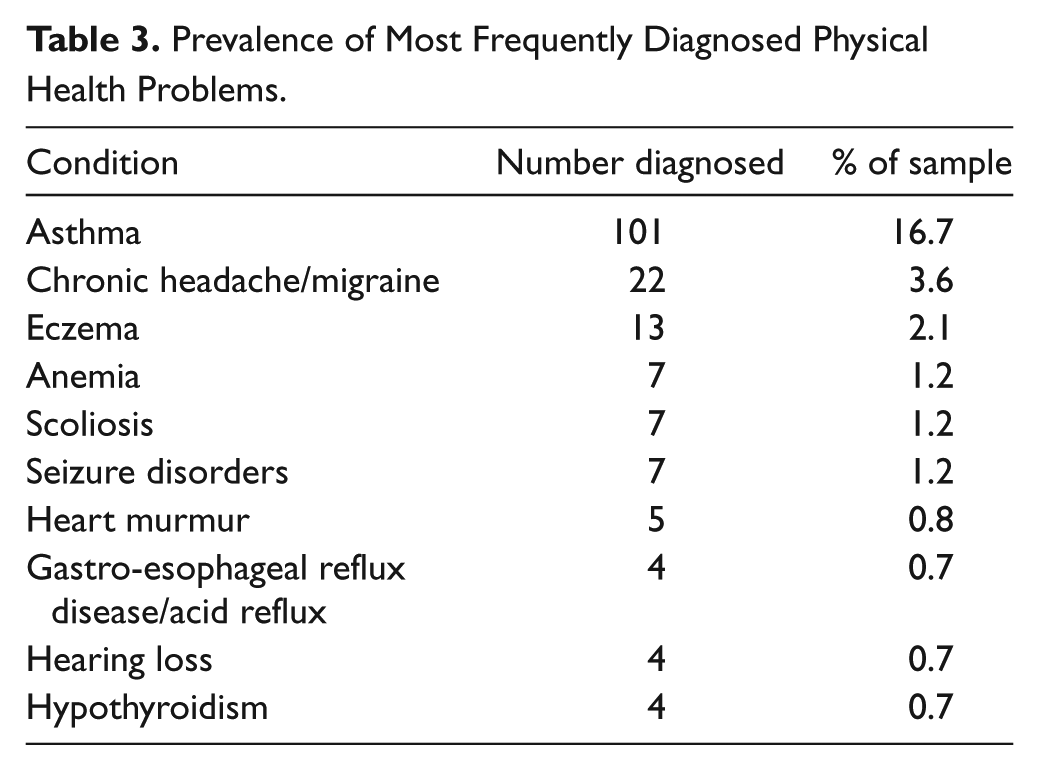
At the conclusion of the intake medical evaluation, the licensed child health professionals recorded any medical diagnoses deemed appropriate at the time. These diagnoses were then routinely entered verbatim into the Boys Town National Database by Boys Town staff. If no conditions were diagnosed at the time of the intake evaluation, then “none” was entered in the database. When data were extracted for the current study, they were checked by a research assistant so that only medical conditions represented in the International Classification of Diseases-10 (ICD-10; World Health Organization, 2006), excluding mental health diagnoses (found on Axis I or II of the Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV]; American Psychiatric Association [APA], 1994), were included. Obesity, allergies, and acne were also excluded due to their high prevalence rates in the general population but inconsistent recording during the intake evaluation. Approximately 35% of the sample had at least one medical diagnosis at the time of intake, which is considerably higher than estimates of prevalences among the general pediatric population from large national health surveys (e.g., 8.6% from National Center for Health Statistics, 2007; 9.3% from National Longitudinal Survey of Youth; Van Cleave, Gortmaker, & Perrin, 2010). Approximately 6.9% of the sample had multiple medical diagnoses. The most frequent diagnoses were asthma (16.7% of the sample), chronic headache/migraine (3.6%), eczema (2.1%), anemia (1.2%), scoliosis (1.2%), and seizure disorders (1.2%; see Table 3 for list of 10 most frequent diagnoses). The diagnostic patterns in this sample were similar to those reported in previous research using the entire Boys Town population (Nelson et al., 2011).
Prevalence of Most Frequently Diagnosed Physical Health Problems.
Youth medications
As a part of the intake medical evaluation, the medical team recorded any medications that the child was taking regularly at the time of intake. This information was routinely entered into the Boys Town National Database by Boys Town staff, and medications were coded by Boys Town staff as psychotropic or nonpsychotropic based on the reason they were prescribed and common usage. When data were extracted from the Boys Town National Database for this study, the number of psychotropic and nonpsychotropic medications listed were tallied separately, yielding a total count for each. To provide another measure of youth physical health, we included only nonpsychotropic medications in our analyses. The nonpsychotropic medication variable was then coded into a dichotomous yes/no variable with youth taking one or more nonpsychotropic medications coded as “yes” and youth taking zero nonpsychotropic medications coded as “no.” Approximately 31.5% of the sample was taking at least one such medication at the time of intake, and the number of medications ranged from 0 to 14 (M = 10.67; SD = 1.32). Consistent with data for youth medical diagnoses, the most frequently prescribed medications were for asthma and pain management (see Table 4 for details).
Prevalence of Most Frequently Prescribed Medications.
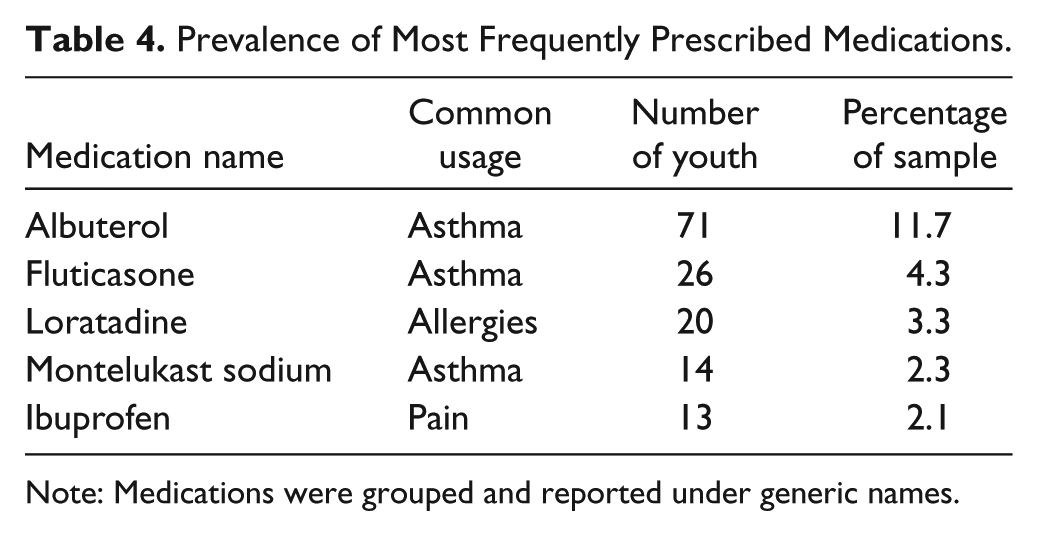
Note: Medications were grouped and reported under generic names.
Results
Preliminary Analyses
Preliminary analyses were conducted to determine the relationship between demographic factors (i.e., age, sex, ethnicity), placement history factors (i.e., last placement with biological parents vs. alternative placement, number of previous out-of-home placements), and the presence of physical health problems. None of the demographic or placement history factors were significantly related to the presence of a physical health problem in bivariate analyses, r = −.02, p > .05, for age; χ2(1) = 1.79, p > .05, for sex; χ2(5) = 2.44, p > .05, for ethnicity; χ2(1) = 0.76, p > .05, for last placement; and r = .06, p > .05, for number of previous placements). However, to provide a more comprehensive and rigorous analysis of the relationship between psychopathology and physical health problems, we controlled for age, sex, last placement with biological parents versus alternative placement, and number of previous out-of-home placements in subsequent regression analyses.
Youth Psychopathology and Physical Health Problems
To examine the association between parent-reported youth psychopathology symptoms and risk for physical health problems, we conducted a series of hierarchical binary logistic regressions with the presence of a diagnosed medical condition (represented dichotomously as either “yes” or “no”) as the dependent variable. For each analysis, demographic (age, sex) and placement factors (last placement with biological parents, number of previous out-of-home placements) were entered together on the first step to control for these factors, then the psychopathology variable of interest was entered on the second step, and the unique variance associated with this variable was examined. Consistent with recommendations by Achenbach (1991), we used raw scores rather than T-scores for CBCL variables because age and gender were already controlled for on the first step of the analyses. To aid in interpretation of odds ratios, raw scores from the CBCL were then transformed into z scores for logistic regression analyses. Therefore, the resulting odds ratios can be interpreted as the increase in likelihood of being in a certain group (e.g., having a medical condition) for every one standard deviation increase in the CBCL score.
In the first analysis, the demographic and placement factors entered on the first step did not significantly predict the presence of a medical condition (step χ2[4] = 3.66, p > .05; all individual variable statistics >.05). We then included CBCL Total Problems as the predictor variable of interest on the second step to determine whether the overall level of psychopathology symptoms reported was associated with risk for a medical diagnosis. The CBCL Total Problems score was significantly associated with having a diagnosed medical condition, β = .22, Wald χ2(1) = 5.94, p < .05, odds ratio = 1.24, such that higher psychopathology scores were associated with greater risk for having a medical condition. In the second analysis, after entering demographic and placement factors on the first step, we entered CBCL Internalizing Problems and CBCL Externalizing Problems scores simultaneously on the second step (instead of Total Problems) to determine which type of psychopathology symptoms was more associated with physical health risk. Although internalizing and externalizing problems were significantly associated with physical health problems in bivariate relationships, r = .12, p = .01 for internalizing and r = .08, p < .05 for externalizing, only internalizing problems was associated with physical health risk when both variables were entered together and allowed to compete for variance, β = .25, Wald χ2(1) = 5.81, p < .05, odds ratio = 1.28. To further probe the relationship between different types of psychopathology symptoms and physical health problems, the third analysis included CBCL DSM subscale scores (i.e., Affective Problems, Anxiety Problems, ADHD Problems, Oppositional Defiant Problems, Conduct Problems) as the predictors of the dichotomous medical diagnosis variable, entered on the second step after demographic and placement factors. Of the CBCL DSM subscales entered simultaneously, only Anxiety Problems was a significant predictor of having a medical diagnosis, β = .35, Wald χ2(1) = 9.73, p < .01, odds ratio = 1.41. A similar pattern of results was found using the presence of multiple medical conditions (yes/no) as the dependent variable; that is, total problems, β = .40, Wald χ2(1) = 5.86, p < .05, odds ratio = 1.49; internalizing problems, β = .61, Wald χ2(1) = 12.99, p < .001, odds ratio = 1.85; and anxiety, β = .61, Wald χ2(1) = 10.12, p = .001, odds ratio = 1.83, were all associated with greater risk for having multiple medical conditions (see Table 5).
Summary of Logistic Regression Analyses.
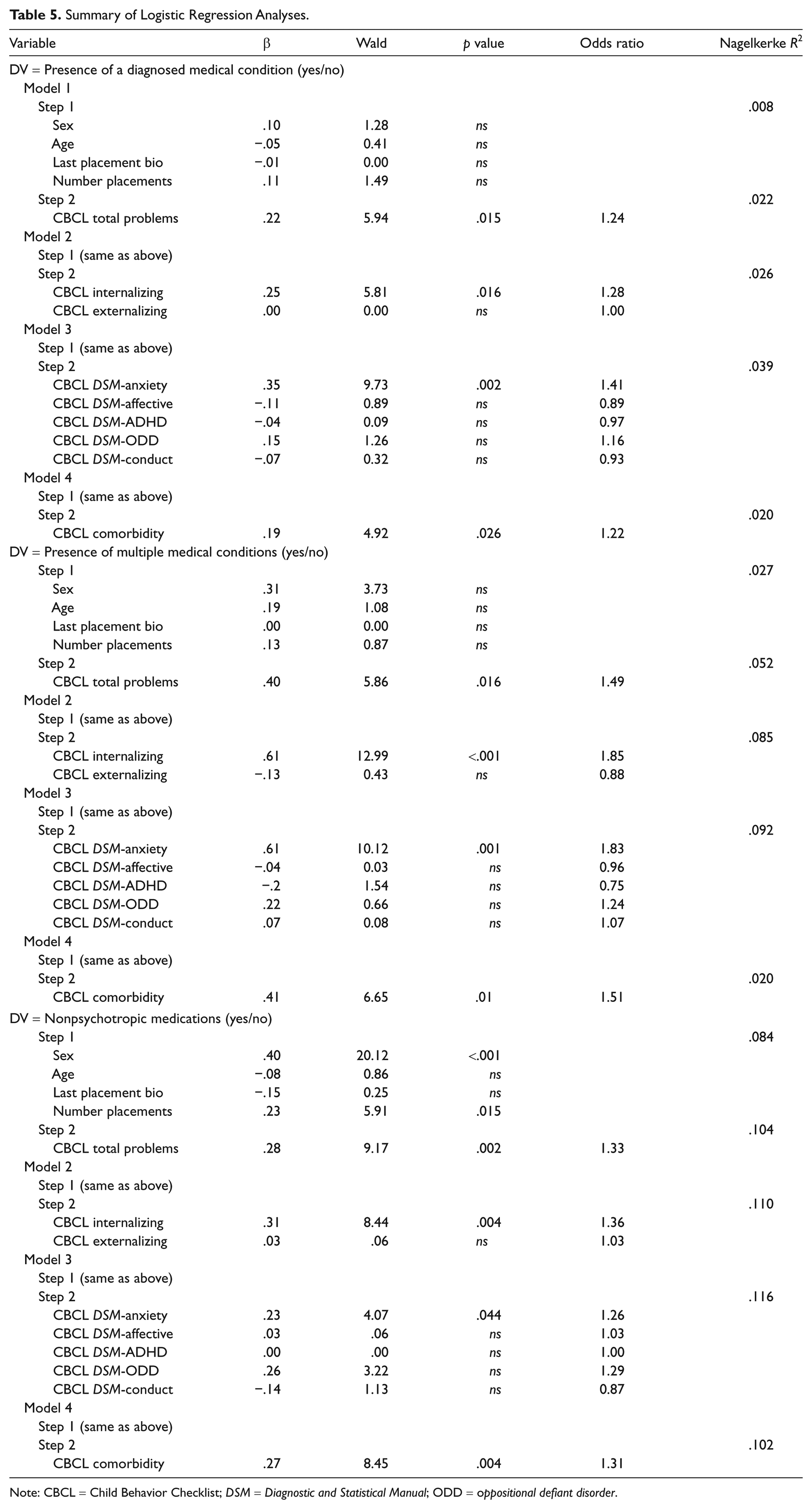
Note: CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual; ODD = oppositional defiant disorder.
In addition to analyses predicting diagnosed medical conditions, we examined the relationship between youth psychopathology and medication status. Specifically, we conducted a series of hierarchical logistic regressions, similar to those presented above, using the nonpsychotropic medications variable (yes/no) as the dependent variable of interest controlling for demographic and placement history variables. A similar pattern emerged, with CBCL Total Problems, β = .28, Wald χ2(1) = 9.17, p < .01, odds ratio = 1.33; Internalizing Problems, β = .31, Wald χ2(1) = 8.44, p < .01, odds ratio = 1.36; and Anxiety Problems, β = .23, Wald χ2(1) = 4.07, p < .05, odds ratio = 1.26, associated with greater risk for being on a medication (see Table 5).
Psychopathology Comorbidity and Physical Health Problems
To examine the association between psychopathology comorbidity and physical health problems, we created a comorbidity variable by calculating the number of DSM-related subscale T-scores (including Affective Problems, Anxiety Problems, ADHD Problems, Oppositional Defiant Problems, and Conduct Problems) that were at or above 70 (a common and conservative clinical cutoff; Ebesutani et al., 2010), resulting in a variable with higher scores representing greater psychopathology comorbidity. Scores on this variable ranged from 0 to 5 with a mean of 1.66 (SD = 1.50). In separate binary logistic regression analyses, after controlling for demographic and placement history factors, this comorbidity variable was a significant predictor of having a medical diagnosis, β = .19, Wald χ2(1) = 4.92, p < .05, odds ratio = 1.22; having multiple medical diagnoses, β = .41, Wald χ2(1) = 6.65, p = .01, odds ratio = 1.51; and being on a nonpsychotropic medication, β = 27, Wald χ2(1) = 8.45, p < .01, odds ratio = 1.31 (see Table 5).
Discussion
The present study examined the relationship between psychopathology and medical status among youth in a large residential care setting. Results indicated that higher levels of youth psychopathology were associated with greater risk for a comorbid medical problem at intake into residential care. Internalizing problems, particularly anxiety symptoms, were most strongly associated with medical status. Furthermore, psychopathology comorbidity was associated with medical problems, with greater comorbidity associated with greater medical risk. The results were consistent across a variety of physical health indicators, including the presence of a medical diagnosis, multiple diagnoses, and nonpsychotropic medications.
These findings contribute to the literature in important ways. First, this study extends previous research on the relationship between psychopathology and health status to the high-risk clinical population of youth in residential treatment. Given the tremendous mental health (Duppong Hurley et al., 2009) and physical health (Nelson et al., 2011) needs of this population, understanding the interplay between the two is crucial for effective assessment and intervention. Second, the current study expands the conceptualization of physical health status to include not only medical diagnosis but also prescription medications. Third, this study examined the associations of different types of psychopathology symptoms (e.g., internalizing vs. externalizing) with risk for physical health issues. Finally, the current study improved on some methodological issues in previous research, employing systematic medical evaluations by licensed child health professionals instead of subjective reports of health problems. Although our study did not examine possible mechanisms for the observed association between psychopathology and physical health, several potential explanations merit discussion. One possibility is that psychopathology, and the stress associated with youth psychopathology (Grant, Compas, Thurm, McMahon, & Gipson, 2004), can lead to the development of physical health problems. Previous research has found that chronic stress can compromise healthy immune functioning (Segerstrom & Miller, 2004), increasing susceptibility to chronic medical conditions. Alternatively, youth with significant psychopathology are often prescribed psychotropic medications, the side effects of which might compromise physical health over the long term. In particular, medications that increase the risk for obesity could trigger or exacerbate other physical health problems, such as asthma and chronic headache. Another related explanation could be that some environmental factors associated with psychopathology risk—including poverty, trauma, family stress, and dysfunction—might also contribute to medical risk. This cluster of risk factors, which may be common among youth referred for residential treatment, could undermine well-being in general, mental and physical, and contribute to high service needs. Finally, caregivers may sometimes overlook the physical health problems of youth with significant mental health issues. Severe psychopathology, including disruptive behavior and risk for self-harm, typically requires intensive intervention efforts on the part of professionals and parents, and this attention to mental health may distract caregivers from less obvious physical health problems. Furthermore, youth requiring out-of-home placement for mental health treatment may experience disruptions in their regular medical care, particularly for routine and preventive services. Taken together, numerous aspects of youth psychopathology, its correlates and its consequences, may contribute to physical health risk across development for youth in residential care.
The finding that internalizing problems, and anxiety specifically, were most associated with physical health problems offers further opportunity to speculate about the possible mechanisms at work. Anxiety is often characterized by frequent, intrusive, and chronic worry, which could undermine immune functioning and physical well-being. In addition to potentially developing new chronic medical conditions because of stress and worry, these phenomena could also exacerbate existing conditions. Chronic headaches and stomachaches, for example, might be triggered by anxiety and worsened by a process of somatosensory amplification (Nakao & Barsky, 2007). Furthermore, clinical anxiety symptoms could interfere with effective coping and prevention strategies, increasing the negative impact on youth functioning. Chronic physical health problems, in turn, could be a source of frustration and worry for the youth, exacerbating psychopathology in a vicious cycle that could result in problems that are overwhelming for caregivers. With such potential mental–physical interactions at work, effective mental health and medical intervention in the residential care population may be crucial.
Clinical and Research Implications
The current study has important implications for clinical practice. The results suggest that many youth with significant psychopathology also have significant physical health problems. Furthermore, they suggest that the more severe the psychopathology, the greater the risk for comorbid medical issues. This association between psychopathology and medical risk highlights the reality that youth presenting with serious mental health problems (such as those referred for intensive residential treatment) are often characterized by complex clinical presentations, including physical and mental health concerns. Recognizing this complexity, as well as the interplay between physical and mental symptoms, is crucial for mental health providers, particularly those working in settings such as residential care. Furthermore, the possibility that physical health symptoms and psychopathology interact with each other suggests that effective assessment and intervention with these youth must address not only the mental health issues but also physical health. Integration of pediatric primary care and behavioral health services has the potential to improve outcomes and, in some cases, may even prevent the need for more costly and restrictive placements. As previously suggested (Nelson et al., 2011), child-focused professionals with expertise in mental and physical health might be particularly well positioned to implement such services as a part of integrated multidisciplinary teams.
The results of the current study also suggest that youth with internalizing problems, particularly anxiety, might be at greatest risk of comorbid medical conditions. Although this finding might be unique to residential treatment and should be examined in other high-need populations, it highlights the importance of comprehensive psychological and medical evaluation of youth with internalizing problems. Early identification of internalizing problems might allow for early intervention that could prevent the development or exacerbation of medical problems. Conversely, early identification of chronic medical conditions among youth with significant psychopathology could allow for effective management of the condition, which could have a positive effect on overall well-being and treatment progress. At a minimum, comprehensive evaluation and the use of multidisciplinary electronic health records would give treatment teams a more complete picture of the youth’s functioning across physical and psychological domains, allowing for richer case conceptualizations and more appropriately tailored treatment plans.
In addition to integrated assessment and treatment services, the association between psychopathology and physical health problems suggests that health promotion interventions could be useful with youth presenting with significant psychopathology. For example, programs that foster awareness of health issues, as well as interventions specifically targeting key health behaviors (e.g., physical activity, diet, sleep) could be especially relevant within this population. Although promising health behavior change interventions for youth already exist (see Wilson & Lawman, 2009, for discussion), it will be crucial to tailor treatments to address the unique challenges of health promotion in a population of youth with significant psychopathology.
In terms of research, longitudinal studies explicating the relationship between psychopathology and physical health over time are needed. Specific mechanisms proposed to mediate the psychopathology–health association—including chronic stress, psychotropic medication side effects, and certain environmental risk factors—are excellent candidates for further exploration. The current study also suggests that it could be particularly salient to examine the impact of effective behavioral and emotional treatment on long-term health outcomes. Similarly, this study highlights the need for the development and validation of health promotion interventions specifically tailored for youth with significant psychopathology. Whether adaptations of existing programs or new treatments developed for this special population, the effectiveness of such interventions in improving short- and long-term health outcomes is an important area for future study. Residential care settings offering comprehensive services might be ideal settings for testing the potential value added by such programming.
Limitations and Future Directions
The current study has several limitations that should be noted. First, the study utilized a cross-sectional design, examining physical problems and psychopathology at the time of intake, limiting our ability to draw causal conclusions. As discussed above, psychopathology could be contributing to medical issues; however, the reverse relationship or a bidirectional model must also be considered. Instead of determining causality, our study only establishes cross-sectional associations between physical and mental health. We believe that these associations are useful because it is important to recognize the complex and co-occurring problems present in youth in residential care; however, longitudinal research is needed to further explicate these relationships. Similarly, longitudinal research is needed to examine whether effective mental health treatment can change medical risk. Recent research suggests that prevention programs for conduct problems can reduce future medical service utilization (Jones et al., 2010); however, similar research examining internalizing problems and residential care is needed.
Second, the current study was limited in its measurement of psychopathology and physical health problems. Although the CBCL is a well-validated and commonly used measure, it may not fully capture the range and severity of youth psychopathology. Similarly, the chart review design of the study is a limitation worth noting. However, unlike many chart review examinations, this study utilized standard procedures in how the medical data were initially collected and recorded (i.e., from standard comprehensive intake medical examinations with the medical team systematically recording key variables in an existing database at the time of the evaluation). These procedures likely helped to avoid many of the common pitfalls of medical chart reviews, including inconsistent procedures and variability in how data are recorded. Still, physician-generated medical diagnoses capture only identifiable health conditions, and they are far from a perfect measure of physical well-being. Despite these limitations in measurement, the use of multiple methods (i.e., parent report, physician evaluation) is a strength of the study because it avoids the problem of common-method variance that plagues studies using self-report for physical and mental health.
Third, although significant associations were found between psychopathology and physical health variables, the effect sizes were small. This could be attributable to imperfect measurement (see above) or to a somewhat restricted range in psychopathology scores in this population (i.e., given the residential treatment setting, scores on the CBCL tended to be high and had perhaps less variability than would be expected in the general population). In addition, it is possible that the relationship between mental and physical health is modest and that psychopathology is just one of many factors that can affect health status. Consequently, the clinical significance of this relationship should be explored in treatment studies that examine the effect of mental health symptom reduction on physical health functioning (see Jones et al., 2010, for an example). Even relatively small effects related to health risk can have important implications for long-term functioning and promotion of youth well-being.
Finally, the study was conducted in a single residential treatment setting. Boys Town’s size and referral base (which extends well beyond the immediate surrounding areas) makes it an ideal setting for conducting research that might be generalizable to youth across the country; however, other residential settings may be different based on the needs and referral patterns in surrounding areas. Therefore, future research should replicate these findings in other residential settings of varying sizes across the country. It is also worth noting that Boys Town has a well-developed comprehensive care model, providing youth with needed medical, behavioral, and educational services all within the Boys Town system. With the capacity to provide such services, it is possible that Boys Town is able to admit youth with a variety of physical health problems that other residential settings might not be able to accommodate. Again, this makes Boys Town an ideal setting for this kind of research, but the physical health of youth in smaller residential placements (and the health trajectories of those youth) still needs to be examined. Furthermore, research extending these findings to other at-risk samples is needed to determine whether the physical and mental health relationships found in this study are generalizable beyond youth in residential care.
Conclusions
Youth psychopathology, particularly internalizing problems, is associated with greater risk for comorbid physical health problems among youth in residential treatment. This means that youth with the most severe mental health symptoms may tend to represent the most complex cases, presenting with psychological and medical difficulties. Comprehensive assessment of physical and mental health status, combined with integrated multidisciplinary treatment, may be indicated for these youth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.