
Abstract
Disagreement between parents and adolescents on the internalizing problems of adolescents poses a threat to diagnoses based on both parent- and adolescent-reported internalizing problems. In this article, we analyze ethnic differences in parent–adolescent agreement on internalizing disorders as reported in a diagnostic interview. A two-phase study design was used. In the first phase, a large sample of adolescents was screened for internalizing disorders using the Youth Self-Report. In the second phase, adolescents from each ethnic group (native Dutch, Surinamese Dutch, Turkish Dutch, Moroccan Dutch) were selected, with half scoring in the borderline/clinical range and half in the normal range. Diagnostic interviews were subsequently conducted with 348 parents and adolescents. Moroccan Dutch parents reported fewer internalizing disorders compared with native Dutch parents. Combining parent and adolescent reports therefore resulted in a lower amount of internalizing disorders among Moroccan Dutch adolescents. Results furthermore showed that (parent- and adolescent-reported) internalizing diagnoses were related to mental health service use in all ethnic groups. Professionals in the field should be sensitive to possible discrepancies between parents and adolescents when diagnosing adolescents’ internalizing disorders, in particular, because underreports of internalizing disorders among parents might contribute to lower levels of mental health service use among adolescents belonging to certain ethnic groups.
Most studies gather diagnostic information from both parents and children to decide whether children or adolescents suffer from internalizing psychiatric disorders (such as anxiety and depression; Mash & Hunsley, 2005; Schniering, Hudson, & Rapee, 2000; Silverman & Ollendick, 2005). During early childhood, parents are generally perceived as the most reliable informants of their child’s internalizing psychiatric disorders. As children grow older, clinicians tend to attach an increasing value to children’s own perceptions of their internalizing problems due to, for instance, increases in cognitive abilities to report on their own behavior or feelings (Grills & Ollendick, 2002, 2003; Jensen et al., 1999). As a result, in adolescence, both parent and child reports are used to establish diagnoses. However, several studies have shown large discrepancies between parents and adolescents in diagnostic information they provide (e.g., Grills & Ollendick, 2002, 2003; Verhulst, Van der Ende, Ferdinand, & Kasius, 1997). So far, discrepant diagnostic information has usually been considered complementary as opposed to unreliable (Jensen et al., 1999). It is assumed that parents’ and adolescents’ views should be considered equally important, because both are able to provide valid information concerning adolescents’ anxiety and depression.
In line with the foregoing, most studies that focused on prevalence rates of psychiatric disorders among adolescents combined parent and adolescent reports to obtain a diagnosis. Several methods have been applied to combine these different reports into one diagnosis. In some studies, children were considered to have a disorder if the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for a specific disorder were met as reported by either the parent or the child (e.g., Canino et al., 2004; Verhulst et al., 1997); other studies regarded a symptom to be present if either parent or child reported it (Angold et al., 2002; Costello, Farmer, Angold, Burns, & Erkanli, 1997); and finally, some studies used best-estimate diagnoses, which were attributed when at least two informants indicated a diagnosis to be present (i.e., parent–child, parent–teacher, or child–teacher; Zwirs et al., 2007). Regardless of the specific method used, a central component found in all previous study methodologies is that both parents and (adolescent) children are given equal weight in determining whether a child suffers from a disorder.
If parent and adolescent reports contribute evenly to the final diagnosis, it is of importance to gain more insights into the factors that influence levels of possible (dis)agreement between parent and adolescent reports of internalizing disorders, as these may considerably affect the pertinent diagnostic conclusions. Previous research has identified some factors that may affect the extent to which parents and their adolescent children agree about the presence of internalizing disorders, in particular, characteristics of the child (type of disorder and age) or family (parental psychopathology, lack of communication, family conflict; Grills & Ollendick, 2002).
Until now, ethnic differences have rarely been considered in research examining agreement on the outcome of parent and adolescent diagnostic interviews. In the Netherlands, the largest non-Dutch ethnic groups consist of immigrant groups, and because international migrations are currently of unprecedented volume, it may be important to examine possible differences between immigrant and non-immigrant groups (Bhugra, 2004). Children of immigrants may be at increased risk of internalizing problems because of various disadvantages related to the migration of their parents, such as their limited socioeconomic resources within the family, their low social status, and their position as newcomer in a new and sometimes unwelcoming society (Guarnaccia & Lopez, 1998; Stevens & Vollebergh, 2008). Moreover, because one’s cultural background has been supposed to influence one’s interpretation of problem symptoms (Weisz et al., 1988), and immigrant adolescents may more strongly adhere to the receiving culture than their parents (Le & Stockdale, 2008), immigrant parents and their adolescent children may relatively often disagree about the child’s level of internalizing problems or disorders. Therefore, in the current study, we will examine differences in parent–adolescent agreement on internalizing problems between four ethnic groups in the Netherlands (i.e., native Dutch, Surinamese Dutch, Turkish Dutch, and Moroccan Dutch). Indeed, research comparing different ethnic groups, either ethnic minority and majority or immigrant and non-immigrant populations, suggests that ethnicity might influence parent–adolescent agreement (De Los Reyes & Kazdin, 2005; Roberts, Alegria, Roberts, & Chen, 2005). In addition, in research using questionnaires to assess internalizing problems, parents and adolescents from ethnic minority/immigrant groups have been found to disagree more about the problems of their child than did ethnic majority/non-immigrant dyads (Lau et al., 2004; Van de Looij-Jansen, Jansen, De Wilde, Donker, & Verhulst, 2011). In a U.S.-based study, all ethnic minority parents reported fewer internalizing problems than did their children (Lau et al., 2004), whereas in a study conducted in the Netherlands, Turkish immigrant parents were found to report more internalizing problems, and Surinamese/Antillean parents were found to report fewer internalizing problems compared with their children (Van de Looij-Jansen et al., 2011). Although several studies showed differences between ethnic groups, no consistent patterns were found. Furthermore, ethnic differences in parent–adolescent agreement regarding internalizing problems have not been examined using diagnostic interviews. Such research is needed, because this might not only influence ethnic differences in the extent to which adolescents are diagnosed with an internalizing disorder but may also influence the decision to seek mental health care.
The implications of this parent–adolescent disagreement for mental health service use of the adolescents may be considerable. In general, parents have been found to play a pivotal role in the pathways toward mental health care for their adolescent children (Logan & King, 2001; Zwaanswijk, Verhaak, Bensing, Van der Ende, & Verhulst, 2003). For instance, if parents do not identify any problems in their child, their child’s chances to receive mental health care reduce considerably (Teagle, 2002; Verhulst & Van der Ende, 1997). Thus, low levels of parent-reported internalizing disorders may prevent their (adolescent) children from receiving help for their problems. In fact, in a previous study, Moroccan Dutch, Turkish Dutch, and Surinamese Dutch parents, as well as Moroccan Dutch adolescents, were found to report significantly lower levels of mental health service use for adolescents’ internalizing problems (Verhulp, Stevens, Van de Schoot, & Vollebergh, 2013).
In sum, the present study adds to the current literature by examining ethnic differences in parent–adolescent agreement on internalizing disorders as measured by a diagnostic interview, by comparing three immigrant groups in the Netherlands with a non-immigrant reference group. In addition to testing ethnic differences in the percentages of parent- and adolescent-reported internalizing disorders, the present study assessed ethnic differences in the agreement about the presence of internalizing disorders. In line with the foregoing, we expected less parent–adolescent agreement with regard to internalizing disorders in the immigrant groups. These discrepancies may be primarily due to immigrant parents reporting fewer internalizing disorders as compared with native Dutch parents, although differences between immigrant groups could also be present (Van de Looij-Jansen et al., 2011). In addition, parent and adolescent reports of internalizing disorders were examined in relation to mental health service use (as reported by parents and adolescents). Reports of internalizing disorders were expected to be positively related to mental health service use, with strongest associations among parent reports.
Method
Sample
The present study used data from the second phase of a two-phase study. In the first phase of the study, a screening was performed at 16 schools selected, because their population consisted of more than 40% non-Western immigrant adolescents (N = 3,331; Mage = 14.1). The response rate of the adolescents in the first phase of the study was 95%. In the second phase, we selected random samples of adolescents and their parents with either a native Dutch, Surinamese Dutch, Turkish Dutch, or Moroccan Dutch background (the latter three ethnic groups belong to the largest immigrant groups in the Netherlands; De Valk, 2010). For all four groups of adolescents, 50% of the adolescents scored in the borderline/clinical range and 50% scored in the normal range on internalizing problems on the Youth Self-Report (YSR) as assessed in the first phase of the study (Achenbach & Rescorla, 2001).
In the second phase of the study, diagnostic interviews were performed with both parents and adolescents. Parents, mostly biological mothers (91%), were interviewed first (n = 381; response rate 64%; ranging from 57% among Surinamese Dutch to 70% among Moroccan Dutch parents). They provided permission to interview their adolescent child (96% of the parents provided informed consent, which varied from 92% among Moroccan Dutch parents to 100% among native Dutch parents). Of the adolescents with parental consent, 96% agreed to participate (ranging from 92% among Surinamese Dutch to 98% among Turkish Dutch and native Dutch adolescents), which resulted in a sample of 349 parents and adolescents. Because one adolescent did not complete the diagnostic interview, the total study sample was 348 (native Dutch n = 95, Surinamese Dutch n = 85, Turkish Dutch n = 86, and Moroccan Dutch n = 82). The mean age of the adolescents in the study sample was 15.2 years, ranging from 13.1 to 18.0 years. An overview of the sample characteristics is provided in Table 1. As shown in Table 1, the selection procedure was successful, as the percentage of adolescents scoring in the borderline/clinical range in the first phase of the study was around 50 in all ethnic groups. Significant differences were only found in education level of parents. Native Dutch and Surinamese Dutch parents did not differ with regard to mean education level, whereas Turkish Dutch and Moroccan Dutch parents had a significantly lower mean education level compared with parents of native Dutch origin. No differences in the mean education level were found between Turkish Dutch and Moroccan Dutch parents. The local medical ethical committee approved the study, and all participants provided written informed consent for data use.
Background Characteristics of the Study Sample.
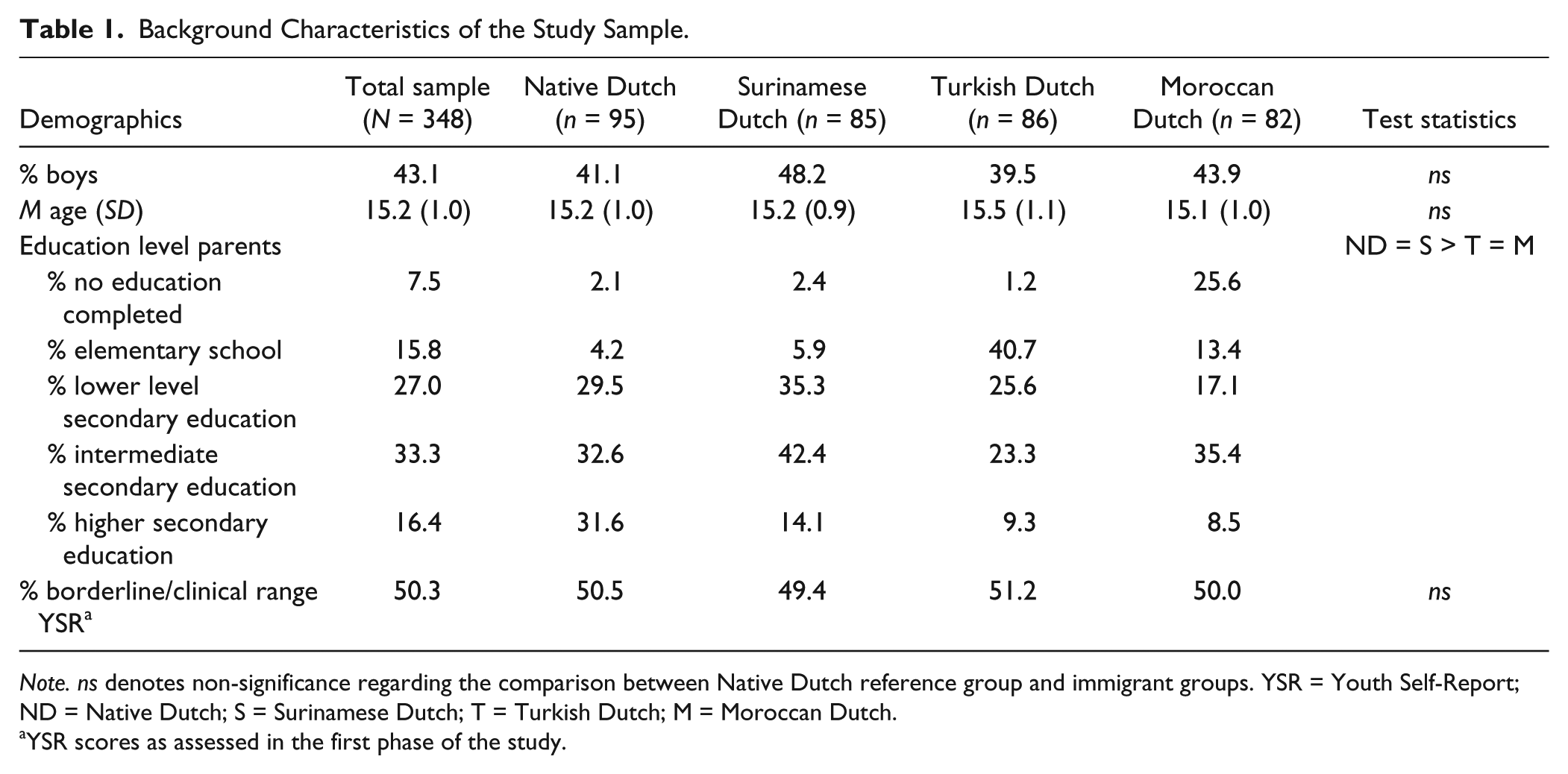
Note. ns denotes non-significance regarding the comparison between Native Dutch reference group and immigrant groups. YSR = Youth Self-Report; ND = Native Dutch; S = Surinamese Dutch; T = Turkish Dutch; M = Moroccan Dutch.
YSR scores as assessed in the first phase of the study.
Instruments
Internalizing disorders
The Dutch translation of the Anxiety Disorders Interview Schedule for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) Child Version (ADIS-C; Siebelink & Treffers, 2001; Silverman & Albano, 1996) was used to assess internalizing disorders. The instrument consists of semi-structured interviews, with different versions for parents and adolescents. Both versions are quite similar and in the present study, parents and adolescents were assessed for separation anxiety, social phobia, specific phobia, panic disorder, agoraphobia, generalized anxiety disorder, obsessive–compulsive disorder, posttraumatic stress disorder, dysthymic disorder, and depressive disorder. Due to the limited amount of several of the internalizing disorders in the present study, a distinction was made only between anxiety and affective disorders. To determine the diagnostic status of the adolescents, we followed the guidelines provided in the manual (Siebelink & Treffers, 2001; Silverman & Albano, 1996). To receive a diagnosis, the adolescent needed to meet the criteria prescribed by the DSM-IV, and the severity should be rated by the interviewer as 4 or higher on a scale from 0 (not severe) to 8 (really severe). Previous studies have shown acceptable to good test–retest reliabilities for this parent and child interview (Silverman, Saavedra, & Pina, 2001).
Mental health service use
Parents and adolescents were asked whether the adolescents received formal mental health care for their internalizing problems from any of several different professionals in the past year. To make sure that all parents and adolescents with different ethnic backgrounds agreed on the meaning of internalizing problems, a definition of internalizing problems was provided based on the items of the Emotional Problem Scale of the Strengths and Difficulties Questionnaire (Goodman, 1997). Both parents and adolescents were given a list of possible professional caregivers, such as psychiatrists, (school) psychologists, or social workers. For both parents and adolescents separately, a dichotomous variable was created with 0 indicating that the adolescent did not receive care in the past year and 1 indicating that the adolescent received care in the past year (see also Verhulp et al., 2013).
Ethnicity
Ethnicity of the adolescent was determined by the country of birth of the parents. If at least one parent was born in the Netherlands, Suriname, Turkey, or Morocco, adolescents were defined as having a native Dutch, Surinamese Dutch, Turkish Dutch, or Moroccan Dutch background. The majority of the parent dyads were born in the same country (i.e., 95% of the families). Whenever one of the parents was born in, for instance, Morocco while the other parent was born in Turkey, the country of birth of the mother was used as an indication of ethnicity. Although at least one of the parents of the immigrant adolescents was born in Morocco, Turkey, or Suriname, the vast majority of the immigrant adolescents were born in the Netherlands (82%; see Note 1).
Education level
Education level was measured as the highest education level achieved by either of the parents (either within the Netherlands or in their country of origin). Response categories were 0 (no education completed), 1 (elementary school), 2 (lower level of secondary/vocational training), 3 (intermediate level of secondary/vocational training), or 4 (university education or higher level of vocational training).
Procedure
Intensively trained lay interviewers with a Turkish Dutch or Moroccan Dutch background performed the diagnostic interviews with Turkish Dutch and Moroccan Dutch parents to be able to perform interviews in their first language if necessary. These lay interviewers were experienced interviewers who also worked with adolescents professionally. Developmental psychologists (who were also trained to perform the interview) conducted the interviews with the Surinamese Dutch and native Dutch parents and with all adolescents. The training for both lay interviewers and developmental psychologists consisted of 2 days, with sessions on internalizing problems, the ADIS-C, and more general interview techniques. Furthermore, interviewers practiced using the ADIS-C by rating two previously conducted ADIS-C interviews, which were subsequently discussed during one of the sessions. Next, all interviewers videotaped one of their own first interviews with parents and adolescents (i.e., both a parent and an adolescent interview) and received feedback from a developmental psychologist with multiple years of experience using the ADIS-C. Next to this clinician, two other developmental psychologists rated these videotaped interviews (i.e., for each interviewer a parent and a child interview was rated, or in case interviewers only interviewed parents or adolescents, then only a parent or a child interview was rated), and the inter-rater agreement about the presence and severity of a certain diagnosis between the interviewer and this rater was found to be good. The average kappa for the presence of internalizing disorders was .93 for parent-reported diagnoses and .91 for adolescent-reported diagnoses. The inter-rater agreement about the severity ratings of the disorders was examined using Pearson’s correlations, showing average correlations of .91 for parents and .96 for adolescents. Note that only the final diagnostic status was used in our analyses (the severity rating was, next to the presence of sufficient symptoms, necessary to receive a diagnosis).
Statistical Analyses
Cross-tabulations were used to indicate ethnic differences in the total percentage of adolescents with internalizing disorders (i.e., reported by parents and adolescents separately) split between anxiety and affective disorders. In addition, for each ethnic group, gender differences in adolescent- and parent-reported internalizing problems were examined. Logistic regression analyses were used to test ethnic differences using dummy variables of ethnicity.
Furthermore, cross-tabulations were used to calculate ethnic differences in total percentages of adolescents with internalizing diagnoses (reported by either parent, child, or both), in percentages of parents and adolescents who agreed on the presence of an internalizing diagnosis (i.e., agreement on the dyadic level), in percentages of cases for which only parents indicated a diagnosis, and in percentages of cases for which only adolescents indicated a diagnosis. Logistic regression analyses were used to test these ethnic differences. All analyses including parent reports were also performed using educational level of parents as a covariate.
Finally, Mplus (Version 7; Muthén & Muthén, 1998–2012) was used to examine the associations between parent- and adolescent-reported internalizing disorders and mental health service use while controlling for gender and age of the child and educational level of the parents. Multiple group analyses were used to test whether the associations differed between different ethnic groups.
Results
Parent and Adolescent Reports of Internalizing Disorders
Table 2 shows the total amount of parent- and adolescent-reported diagnoses separately as well as anxiety and affective disorders separately. Surinamese Dutch, Turkish Dutch, and Moroccan Dutch adolescents did not report significantly fewer internalizing disorders compared with native Dutch adolescents (Surinamese Dutch: odds ratio [OR] = 0.80, 95% confidence interval [CI] = [0.44, 1.45]; Turkish Dutch: OR = 0.90, 95% CI = [0.50, 1.63]; Moroccan Dutch: OR = 0.68, 95% CI = [0.37, 1.26]). Moroccan Dutch parents, however, reported fewer internalizing disorders compared with native Dutch parents (OR = 0.37, 95% CI = [0.18, 0.77]), whereas Surinamese Dutch and Turkish Dutch parents reported similar amounts of internalizing disorders for their children compared with native Dutch parents (OR = 0.73, 95% CI = [0.39, 1.39] and OR = 1.17, 95% CI = [0.63, 2.15], respectively). Table 2 further presents the gender distribution of adolescents with an internalizing disorder. At least two thirds of the adolescents with an internalizing disorder were girls across all ethnic groups. When differentiating between anxiety and affective disorders, Moroccan Dutch parents reported significantly fewer anxiety disorders (Surinamese Dutch: OR= 0.77, 95% CI = [0.40, 1.46]; Turkish Dutch: OR = 1.22, 95% CI = [0.66, 2.26]; Moroccan Dutch: OR = 0.32, 95% CI = [0.15, 0.69]), but did not report fewer affective disorders (Surinamese Dutch: OR = 0.74, 95% CI = [0.12, 4.53]; Turkish Dutch: OR = 1.11, 95% CI = [0.22, 5.64]; Moroccan Dutch: OR = 1.17, 95% CI = [0.23, 5.93]) compared with native Dutch parents. Again, no ethnic differences were found among adolescents regarding both anxiety and affective disorders (Anxiety: Surinamese Dutch OR = 0.76, 95% CI = [0.42, 1.38]; Turkish Dutch OR = 0.90, 95% CI = [0.50, 1.63]; Moroccan Dutch OR = 0.61, 95% CI = [0.33, 1.13]; Affective: Surinamese Dutch OR = 0.40, 95% CI = [0.10, 1.55]; Turkish Dutch OR = 0.39, 95% CI = [0.10, 1.53]; Moroccan Dutch OR = 0.41, 95% CI = [0.11, 1.61]). Finally, Table 2 shows the ethnic differences in mental health service use for internalizing problems. Surinamese Dutch, Turkish Dutch, and Moroccan Dutch parents reported that their children used mental health services for internalizing problems significantly less compared with native Dutch parents. Among adolescents, only Moroccan Dutch adolescents reported significantly lower levels of mental health service use compared with their native Dutch peers (for test statistics, see Verhulp et al., 2013).
Percentage of Adolescents (Girls and Boys) With Internalizing Diagnoses (Based on Parent and Adolescent Reports Presented Separately by Anxiety and Affective Disorders) and Mental Health Service Use for Internalizing Problems (Reported by Parents and Adolescents).
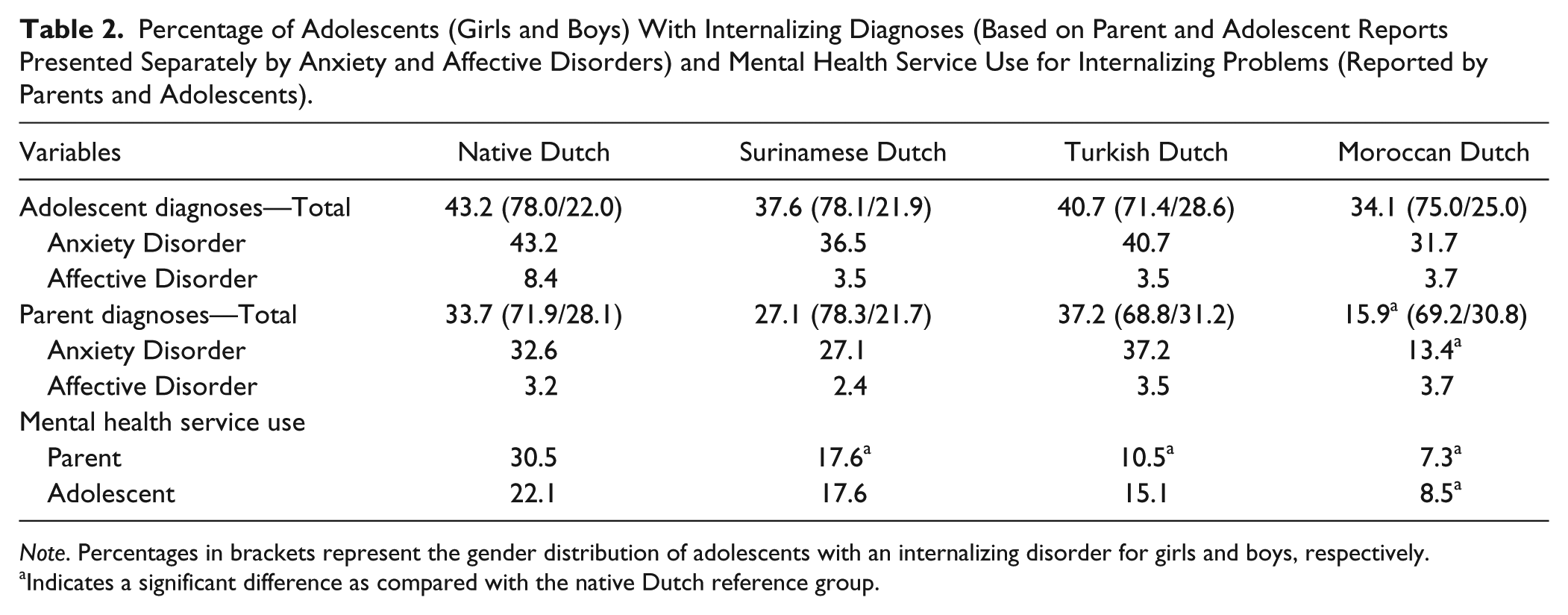
Note. Percentages in brackets represent the gender distribution of adolescents with an internalizing disorder for girls and boys, respectively.
Indicates a significant difference as compared with the native Dutch reference group.
Agreement on Parent and Adolescent Reports of Internalizing Disorders
Combining the parent- and adolescent-reported internalizing disorders into a single diagnosis resulted in fewer internalizing disorders among Moroccan Dutch adolescents compared with native Dutch adolescents (see Table 3; Surinamese Dutch: OR = 0.61, 95% CI = [0.34, 1.11]; Turkish Dutch: OR = 1.22, 95% CI = [0.67, 2.21]; Moroccan Dutch: OR = 0.51, 95% CI = [0.28, 0.93]). To further illustrate the (dis)agreement between parents and adolescents on internalizing diagnosis, the amount of internalizing disorders reported by both parents and adolescents (i.e., cases in which parents and adolescents agreed on the presence of a disorder) and the disorders reported only by the parent or the adolescent (i.e., cases in which parents and adolescents disagreed on the presence of a disorder) are presented in Table 3.
Total Percentage of Adolescents With Internalizing Diagnoses (Reported by Either Parent, Adolescent, or Both) and Percentages of Cases in Which Both Parents and Adolescents Reported a Diagnosis (i.e., Agreement) and Cases in Which Only the Adolescent or Only the Parent Reported a Diagnosis (i.e., Disagreement).
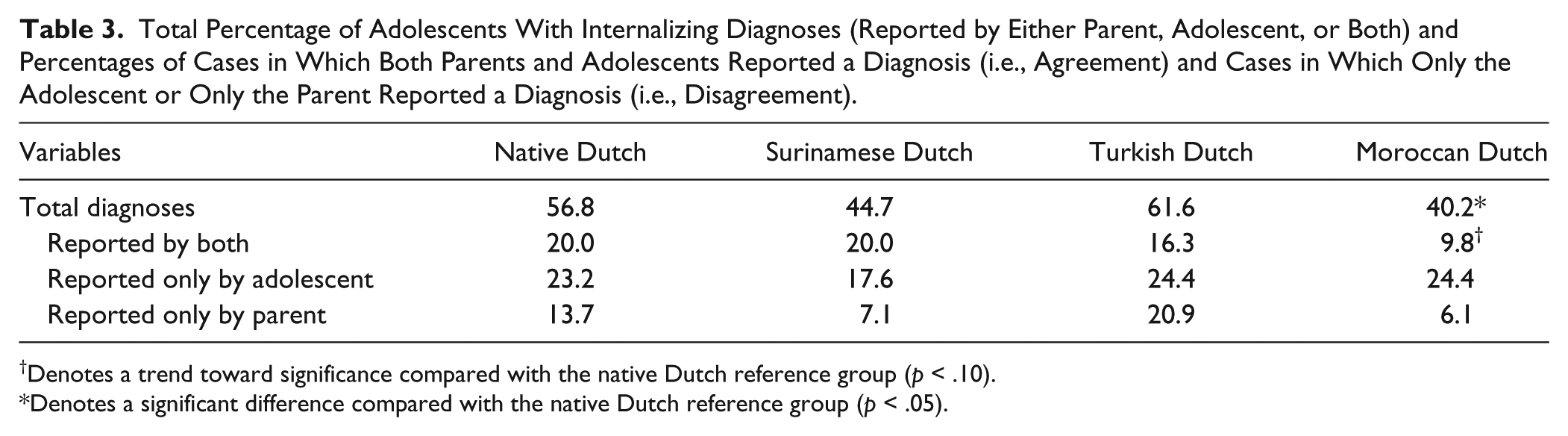
Denotes a trend toward significance compared with the native Dutch reference group (p < .10).
Denotes a significant difference compared with the native Dutch reference group (p < .05).
Table 3 indicates that the percentage of parent–adolescent agreement about the presence of an internalizing disorder (i.e., diagnoses reported by both parent and adolescent) was lower only for the Moroccan Dutch adolescents relative to the native Dutch reference group, although this difference only showed a trend toward significance (OR = 0.43, 95% CI = [0.18, 1.05]). Considering parent-only reported internalizing disorders, differences in percentages between ethnic groups seem to indicate fewer internalizing disorders reported by Surinamese Dutch and Moroccan Dutch parents compared with native Dutch parents, although these differences were non-significant.
Parental Education Level
Table 1 shows clear ethnic differences in education level of the parents, with Turkish Dutch and Moroccan Dutch parents having lower education levels than native Dutch and Surinamese Dutch parents. Therefore, analyses concerning parent reports were rerun using parental education level as a covariate. First, ethnic differences in parent-reported internalizing disorders were tested again. After controlling for education level, for Moroccan Dutch parents, only a trend toward significance was found (OR = 0.50, 95% CI = [0.23, 1.06]). Second, the total amount of internalizing disorders (reported by either parents and/or adolescents) among Moroccan Dutch adolescents did not significantly differ from the native Dutch adolescents, after controlling for parental education level (OR = 0.60, 95% CI = [0.32, 1.13]). Furthermore, regarding agreement between parents and adolescents on the presence of an internalizing disorder, the previously found difference between Moroccan Dutch and native Dutch adolescents was non-significant after controlling for education level of parents (OR = 0.49, 95% CI = [0.19, 1.22]). Finally, ethnic differences in parent-only reported disorders were also reexamined. Again, the effect remained non-significant for Moroccan Dutch parents (OR = 0.61, 95% CI = [0.20, 1.86]). However, a non-significant effect became significant for Turkish Dutch parents, indicating that after controlling for education level, Turkish Dutch parents reported significantly more internalizing disorders for their adolescent children than native Dutch parents (OR = 2.67, 95% CI = [1.13, 6.28]).
Associations With Mental Health Service Use
To examine the possible consequences of the lower number of parental reports of internalizing disorders among Moroccan Dutch compared with Dutch native adolescents, associations of parent and adolescent reports of internalizing disorders with parent- and adolescent-reported mental health service use were investigated. The effects of age, gender, and education level of parents were controlled for but deleted from the model, because they did not contribute significantly to the model.
The results of the analysis are shown in Figure 1, indicating that in the total sample, parent-reported internalizing disorders related to parent-reported mental health service use, whereas adolescent-reported internalizing disorders related to adolescent-reported mental health service use. Cross paths of parent-reported internalizing disorders with adolescent-reported mental health service use and of adolescent-reported internalizing disorders with parent-reported mental health service use were not significant. Multi-group analyses were used to examine whether the associations between reports of internalizing disorders and mental health service use differed between ethnic groups. Wald tests revealed that all associations were similar across ethnic groups (the path from parent-reported internalizing disorder to parent-reported mental health service use: Wald = 1.77, p = .621 and from adolescent-reported disorder to adolescent-reported service use: Wald = 1.89, p = .596).
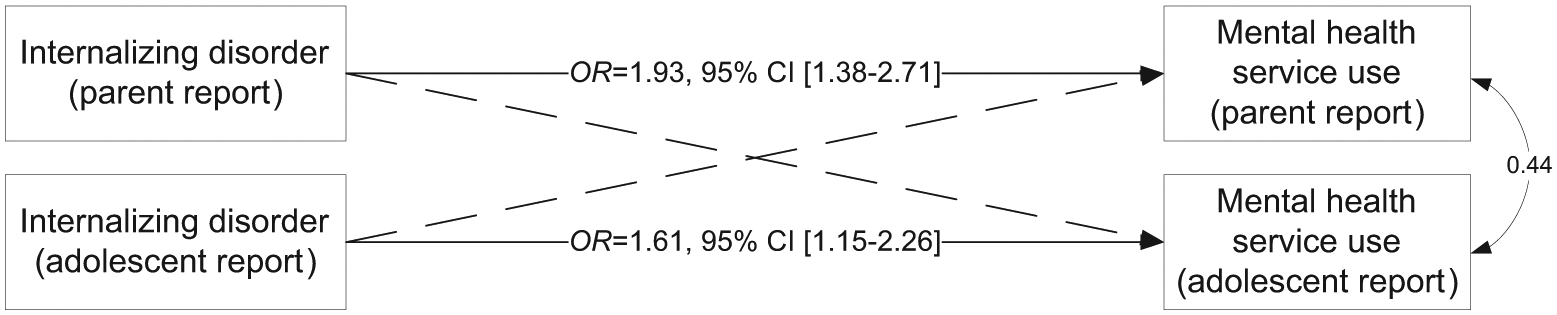
Logistic regression model testing the associations between internalizing disorders (reported by parents and adolescents) and mental health service use (reported by parents and adolescents).
Discussion
The aim of the present study was to examine ethnic differences in the agreement between parents and adolescents regarding adolescents’ internalizing disorders and possible consequences for mental health care. The results only revealed significant differences in parent–adolescent agreement between native Dutch and the Moroccan Dutch groups. Moroccan Dutch parents reported lower levels of internalizing disorders for their children compared with native Dutch parents, whereas Moroccan Dutch adolescents themselves reported as many internalizing disorders as their native Dutch peers, providing preliminary evidence for a lower level of parent–adolescent agreement in the Moroccan Dutch population. More specifically, by testing ethnic differences in percentages of cases for which both parents and their child reported an internalizing disorder, the results indeed showed that the degree of parent–child agreement on the presence of an internalizing disorder in the child was much lower in the Moroccan Dutch compared with the native Dutch ethnic group. The consequences of Moroccan Dutch parents’ reports for pertinent diagnostic conclusions were clear. When combining reports of both informants—a method frequently used to assess adolescent diagnoses—Moroccan Dutch adolescents were considerably less often diagnosed with an internalizing disorder compared with native Dutch adolescents. The results furthermore suggested that this lower level of parent-reported internalizing disorders among the Moroccan Dutch group negatively affects Moroccan Dutch children’s access to mental health care, because there is a clear relationship between parental reports of adolescents’ internalizing disorders and parent-reported mental health service use by the child.
The results further showed that the relatively low levels of parent-reported internalizing disorders by Moroccan Dutch parents and the resulting low levels of parent–adolescent agreement in Moroccan Dutch families could be partly explained by the lower education level of Moroccan Dutch compared with native Dutch parents. Possibly, both their low level of education and their cultural background may have influenced these parents’ perceptions of their child’s internalizing problems. More specifically, compared with their children and other parents, lowly educated Moroccan Dutch parents may be less likely to define their children’s problems psychologically (De Swaan, 1990; Knipscheer & Kleber, 2005) and may have higher thresholds for considering child behaviors as abnormal (Weisz et al., 1988). Furthermore, it has become clear that, in general, it might be difficult for parents to detect internalizing problems, as adolescents have to share their internal states with their parents (Grills & Ollendick, 2002; Jensen et al., 1999). In this sense, it is not strange that a previous study has indicated that a lack of communication between parents and adolescents results in larger discrepancies between parent and adolescent reports (Grills & Ollendick, 2002). Combining our findings with research showing greater cultural differences between Moroccan Dutch adolescents and their parents compared with Turkish adolescents and their parents (Verkuyten, 2003) may indicate that Moroccan Dutch adolescents in the Netherlands might not share feelings and emotions with their parents as other adolescents do (Pels & De Haan, 2003). This might explain why Moroccan Dutch parents seem to be relatively unaware of their children’s problems and subsequently report relatively few internalizing disorders.
In contrast, when compared with native Dutch parents, Turkish Dutch parents were found to report relatively high levels of internalizing disorders in their children after controlling for education level of the parents. These findings are in line with several studies conducted in several Turkish Dutch samples and in Turkish children in Turkey. Parents of Turkish Dutch children have been found to report more internalizing problems than non-immigrant parents, but comparing Turkish Dutch children with Turkish children in Turkey revealed no differences between these groups with regard to internalizing problems (Bengi-Arslan, Verhulst, Van der Ende, & Erol, 1997; Van de Looij-Jansen et al., 2011). Together, these studies might be suggestive of an effect of Turkish culture on parental perceptions of children’s internalizing disorders or symptoms. In studies performed 10 years ago, Turkish Dutch adolescents were also found to report more internalizing problems than native Dutch adolescents (Janssen et al., 2004). However, these differences were already less pronounced than the differences found among parents (Bengi-Arslan et al., 1997). Findings in different generations and at different time points suggest that Turkish Dutch adolescents have become more similar to non-immigrant adolescents in reporting about problem behavior, which has been suggested to be influenced by the fact that adolescents are more strongly integrated in the new society than their parents (Janssen et al., 2004).
Although reports of internalizing disorders may be more comparable between Surinamese Dutch, Turkish Dutch, and native Dutch parents and adolescents, Surinamese Dutch and Turkish Dutch parents reported lower levels of mental health service use in our study. However, in a previous study, we found that Surinamese Dutch and Turkish Dutch parents did not identify emotional problems to a similar extent compared with native Dutch parents, and we showed that this subjective identification of emotional problems is more strongly related with mental health service use than their reports of problem symptoms (Verhulp et al., 2013). In fact, these ethnic differences in subjective emotional problem identification mediated the association between ethnicity and mental health service use. These findings suggest that Turkish Dutch and Surinamese Dutch parents are less likely to seek help for their children’s internalizing problems, because they tend to subjectively identify fewer emotional problems. Furthermore, Surinamese Dutch and Turkish Dutch adolescents did not report lower levels of mental health service use themselves compared with native Dutch adolescents, which may indicate that these adolescents also seek help for their internalizing problems without informing their parents (e.g., in the school context).
The present study has provided more insights into the overlap between diagnoses based on parent and adolescent reports, showing that the agreement between parent and adolescent reports is rather limited in general and that the independent contribution of both the parent and child reports of internalizing disorders is substantial. More specifically, for all four ethnic groups, for more than 50% of the participants, their diagnosis was based on only one informant. Obviously, there is no “gold standard” to decide whether the parent or the adolescent report on internalizing disorders is right or wrong. However, when only one of the two informants reports lower levels of internalizing disorders, combining information provided by parents and adolescents by giving them similar weight might result in a lower number of diagnoses. In this study, this was the case for Moroccan Dutch adolescents. For the Moroccan Dutch adolescents in our sample, the lower number of internalizing diagnoses might not be an accurate estimate because Moroccan Dutch adolescents themselves reported similar amounts of internalizing disorders compared with the native Dutch adolescents. Studies reporting on prevalence rates among different ethnic groups might also suffer from this problem, and therefore, these prevalence rates should be interpreted with caution.
To solve the issue of low parent–adolescent agreement, previous studies have suggested using a more continuous approach by analyzing problems at the symptom level (Brown-Jacobsen, Wallace, & Whiteside, 2011; Comer & Kendall, 2004). Although this might enhance parent–adolescent agreement, it is unlikely to solve the ethnic differences in parent–adolescent agreement on internalizing disorders. Analyzing reports of psychiatric disorders at the symptom level will possibly result in higher parent–adolescent agreement among all ethnic groups and will not result in smaller ethnic differences. Therefore, when investigating the prevalence rates of psychiatric problems in different ethnic groups, parent and adolescent reports should be studied to examine whether underreports of parents in some ethnic groups influence these prevalence rates.
Several limitations of the present study should be considered. First, some apparent differences between ethnic groups were found to be non-significant, most likely due to insufficient group sizes and thus limited power. Second, the variation in the outcome variable was limited, which might have influenced the results. Future studies should replicate the findings of the current study using a larger sample and more variation in the outcome variable to assess whether non-significant differences found in the current study become significant. A larger sample size might also have provided the possibility to differentiate more consistently between anxiety and affective disorders. To disentangle the parent–adolescent discrepancies more thoroughly, such a differentiation may be worthwhile. Third, Moroccan Dutch and Turkish Dutch lay interviewers were used to interview the Moroccan Dutch and Turkish Dutch parents, respectively, to facilitate communication in participants’ first language. Although all lay interviewers were trained elaborately and did have some experience in working with children and/or adolescents, they were not psychologists. We cannot rule out that this procedure has had a negative impact on the validity of the diagnoses. However, the fact that these parents were interviewed by members of their own ethnic group and were able to communicate in their first language may also have had a positive influence on the validity of the diagnoses. Finally, another limitation of the present study was that it focused only on internalizing disorders. Studying parent–adolescent agreement regarding externalizing disorders would also be very interesting, because these types of behaviors are more visible for parents, and therefore, agreement is probably larger in general. Moreover, ethnic differences in parent–adolescent agreement might also differ with regard to different types of behavior. For example, compared with other ethnic groups, previous research showed that Turkish Dutch parents have more difficulties detecting attention deficit hyperactivity disorder (ADHD; Zwirs, Burger, Buitelaar, & Schulpen, 2006), whereas they seem to have no difficulties detecting internalizing problems in their children (Van de Looij-Jansen et al., 2011).
To our knowledge, the present study is the first to examine ethnic differences in parent and adolescent reports of internalizing disorders as well as the contributions of both informants to the final diagnosis. To enhance the generalizability of the present findings, other studies in other countries with different ethnic groups should examine the same research questions including the potential influence of parental education level. Even more importantly, research is necessary to explain why a lack of parent–adolescent agreement on internalizing disorders may be especially prevalent in certain immigrant groups. More specifically, more research is needed to understand why these immigrant populations, besides their low education level, experience difficulties reporting on their children’s problem behaviors. Do they actually proto-professionalize problems to a lesser extent, and/or do they have different thresholds in when to consider behavior as abnormal or problematic? For example, these parents may need mental health education on internalizing problems and on the possible benefits of mental health service use. Finally, it would also be interesting for future research to attempt to tap into variation within immigrant populations. For example, in the current study, we did not account for the amount of years immigrant parents resided in the Netherlands since their migration, being first- or second-generation immigrants, or for instance, the extent to which these parents are oriented toward the Dutch and their ethnic culture (i.e., parental acculturation orientations). These factors may also influence parents’ perceptions of their children’s behavior and as a consequence, have an impact on parent–adolescent agreement on internalizing disorders (e.g., Sood, Mendez, & Kendall, 2012).
Conclusion
Although discrepant diagnostic information is considered complementary as opposed to unreliable (Jensen et al., 1999), clinicians tend to base their final diagnostic conclusion on parent rather than child reports (Grills & Ollendick, 2003). As a result, clinicians should be aware of the fact that some immigrant parents might underreport internalizing disorders in their (adolescent) children. In other words, reports of internalizing disorders by adolescents should perhaps be taken more seriously particularly in some ethnic groups (Cantwell, Lewinsohn, Rohde, & Seeley, 1997). Another important issue to be aware of in some ethnic groups is that the pathway toward mental health care through parents may be used less often. To reach out to these adolescents and provide them with adequate mental health care, mental health education could be provided to these immigrant populations. In addition, other pathways may be considered toward mental health care. Schools, general practitioners, social workers, and other professionals should be aware of the possibility that in some ethnic groups, parents might experience more difficulties reporting on their children’s internalizing problems and therefore with entering mental health care for their children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Organization for Health Research and Development (Grant 15701.2005).