
Abstract
Positive behavioral interventions and supports (PBIS) and school mental health (SMH) are prominent initiatives in the United States to improve student behavior and promote mental health and wellness, led by education and mental health systems, respectively. Unfortunately, PBIS and SMH often operate separately in districts and schools, resulting in a number of missed opportunities for interconnecting programs and services and increasing their depth and quality within multi-tiered frameworks of prevention, support, and intervention. The current article details a necessary first step in the process of improved interconnection of these two frameworks by describing the development of a process and tool for schools/districts to assess readiness for connecting PBIS and SMH through a blended system. Relevant literature, pilot data, and methodology are discussed, in addition to psychometric properties of the survey and future applications of this instrument for practice, research, and policy.
Keywords
Although federal and state education laws have historically focused on academic proficiency, more recent legislation has included provisions for addressing students’ behavior and mental health and well-being. The 2004 reauthorization of the Individuals With Disabilities in Education Improvement Act (IDEA; 2004) required use of positive behavioral interventions and supports (PBIS) for students receiving special education, and teachers’ professional development to include PBIS training. The No Child Left Behind Act of 2001 (NCLB; 2002) incorporated promotion of students’ behavioral/mental health. In 2003, a major report of the U.S. President evaluated the nation’s mental health system, including a major recommendation to “improve and expand school mental health programs” (President’s New Freedom Commission on Mental Health, 2003). A more recent report from the U.S. President called for improvement of school climate and school mental health (SMH) services in a broader plan to improve student safety, following yet another tragic incident of school violence (U.S. White House, 2013). Thus, PBIS and SMH have become cornerstones in the nation’s systems to promote student learning, health, and wellness. Because these two systems have typically operated separately, this is a significant missed opportunity for complementarity and synergy in program development and implementation in multi-tiered frameworks aimed at enhancing student well-being and school success (Barrett, Eber, & Weist, 2013). In the following article, we provide background on the two systems, document benefits for interconnection, and describe the development of an initial measure now available in the public domain to assess school/district readiness for such interconnection.
School-wide PBIS is a framework for teaching, promoting, and reinforcing positive behaviors, as opposed to relying on reactive and punitive discipline strategies when students exhibit inappropriate behavior (Sugai & Horner, 2002). PBIS is not an intervention, but a multi-tiered system for applying positive behavior strategies to minimize problem behaviors and increase adaptive behaviors (Sugai, Horner, et al., 2000). Once PBIS is in place, appropriate programming can be implemented according to the needs of the students and the community. School staff cannot design, fund, and implement separate programs for each federal and state education initiative; thus, a school-wide PBIS framework can meet students’ needs and satisfy federal and state requirements (Lewis-Palmer & Barrett, 2007).
PBIS operates as a layered system of prevention-based interventions. Tier I, primary prevention strategies to support positive behavior, are implemented for the entire student population. For the 15% to 20% of students who do not respond to primary interventions, Tier II or secondary interventions are implemented to assist in early identification and focused prevention and intervention for students who are contending with conditions of risk or showing beginning levels of behavioral issues. Tier III or tertiary interventions are for the remaining 1% to 5% students who do not respond to Tier II strategies. These interventions are reserved for students with more challenging behavior problems, and focus on reducing the level and frequency of these behaviors. By promoting population-wide positive behavior in students, PBIS can have dramatic impacts in schools by reducing problem behaviors, improving the school climate, and giving teachers and school administrators increased time to focus more on learning (Eber, Sugai, Smith, & Scott, 2002; Sugai, Sprague, Horner, & Walker, 2000).
Data suggest that PBIS is an effective framework for improving behavioral issues and promoting academic success (see Bradshaw, Mitchell, & Leaf, 2010; Lassen, Steele, & Sailor, 2006; McIntosh, Campbell, Carter, & Dickey, 2009; Todd, Campbell, Meyer, & Horner, 2008, regarding effectiveness of Tier I and Tier II interventions). By reinforcing appropriate and adaptive behaviors, PBIS can “render problem behavior irrelevant, inefficient, and ineffective by helping an individual achieve his or her goals in a socially acceptable manner, thus reducing, or eliminating altogether, episodes of problem behavior” (Carr et al., 2002, p. 5). Thus, a system of services and supports can be developed to maximize strengths and minimize deficits (Eber et al., 2002). The PBIS framework also emphasizes data-based decision making and use of evidence-based interventions (EBIs; Sugai, Horner, et al., 2000), which parallels directives in IDEA 2004 and NCLB.
Although the utility and effectiveness of PBIS have been established, implementation varies widely. According to Pas and Bradshaw (2012), 44 states had district- or state-level supports for school-wide PBIS (Tier I). However, previous research indicated that 47 states reported using PBIS, but the number of schools implementing PBIS ranged from zero to 804 (Spaulding, Horner, May, & Vincent, 2008). Furthermore, implementation of the three PBIS tiers is inconsistent. Tier I is the most commonly implemented intervention (Lane, 2007), whereas Tier II and Tier III interventions are often partially implemented or not at all. Because Tier II and Tier III interventions are implemented less frequently and with varying degrees of fidelity, students in need of more intensive support may not receive the necessary academic or behavioral assistance.
SMH
Between 12% and 32% of youth contend with serious emotional/behavioral problems (Burnett-Zeigler & Lyons, 2012; Merikangas et al., 2010). Less than one third of youth receive mental health services (Gaskin, Kouzis, & Richard, 2008; National Research Council, 2006), and if they do receive them, they are likely to receive them in schools (Rones & Hoagwood, 2000), the most universal natural environment for children apart from their homes. Socioemotional skills in children are unique predictors of academic performance and share a reciprocal relationship with academic performance (Guzman et al., 2011; Nadeem, Maslak, Chacko, & Hoagwood, 2010). Students’ mental health has been associated with increases in prosocial behavior and family engagement in school activities, as well as decreases in discipline referrals, special education referrals, and behavior problems (Stephan, Weist, Kataoka, Adelsheim, & Mills, 2007). Interventions promoting socioemotional learning are linked with improved attitudes and school functioning and decreases in depression (Merrell, 2010).
In reaction to this increased recognition of the links between mental health and student learning, as well as the realization that students’ mental health needs are largely met within the school setting (Eiraldi, Wolk, Locke, & Beidas, 2015), expanded SMH services have been developing around the nation (Evans, Weist, & Serpell, 2007; Weist, Evans, & Lever, 2003). These programs emphasize school–community system partnerships to implement a full continuum of promotion, prevention, early intervention, and treatment for youth in schools. Growth of SMH has been promoted through federal investments for national centers (e.g., University of Maryland, Center for School Mental Health) focused on advancing this field, and by evidence of improved access, reduced burden of care, and improved behavioral and school outcomes when these programs are done well (Adelman et al., 1999; Weist et al., 2007).
SMH services are delivered by a variety of professionals, including school psychologists, counselors, social workers, and community mental health staff, as well as others with backgrounds in clinical child psychology (Nabors, Weist, Tashman, & Meyers, 1999; Weist et al., 2009). Bringing community mental health staff into schools to augment the work of school-employed mental health staff increases the ability of schools to respond to student mental health needs. In addition, this would address the problem of too few school-employed staff and the fact that many of them contend with position constraints, such as psychologists in roles that emphasize evaluation (Weist, Lever, Bradshaw, & Owens, 2014). However, SMH services typically lack an implementation structure and, as a result, are implemented with high variability within schools and school districts, with many different arrangements, and often are not connected to PBIS. Failing to connect to PBIS also compromises SMH in relation to missed opportunities for effective teamwork and data-based decision making, two core features of PBIS (Barrett et al., 2013).
It is also imperative that professionals in the school and community receive adequate and ongoing training in mental health promotion and SMH service delivery (Weist, 2005). Massey, Armstrong, Boroughs, Henson, and McCash (2005) recommended that teachers receive ongoing training to increase understanding of the intervention process and how interventions function with the academic curriculum. This training also promotes intervention fidelity and consistency.
Mellin and Weist (2011) suggested conceptualizing collaboration among SMH professionals using a social capital framework. By viewing these interconnected relationships from a perspective of mutual support and trust, SMH services and outcomes for students can be enhanced by sharing resources and information. For instance, mental health practitioners in the community can learn about the unique logistical, cultural, and legal issues regarding delivery of mental health services in the schools. Thus, increasing knowledge in this organic fashion can increase the effectiveness of interventions and streamline SMH service delivery.
Toward the Interconnection of PBIS and SMH
Interconnecting SMH with PBIS is a logical next step for adding depth and quality to PBIS and improving team functioning and data-based decision making for SMH. More than 18,000 schools across the U.S. use the PBIS framework and are familiar with its operation (Barrett et al., 2013). Although national data are less clear for SMH programs, at least 5,000 schools have formal connections with community mental health services in the national survey of SMH conducted by the Substance Abuse and Mental Health Services Administration (Foster et al., 2005). Thus, interconnection of PBIS and SMH has the potential to enhance quality of programming in many U.S. schools and create synergies and economies of scale in a collaborative approach that capitalizes on the respective strengths of each approach (Barrett et al., 2013).
Another factor integral to successful PBIS–SMH interconnection is buy-in and support of school administrators, teachers, and key stakeholders. “Buy-in among school professionals” was one of the top five essential factors impacting SMH collaboration (Mellin & Weist, 2011). According to Langley, Nadeem, Katoaka, Stein, and Jaycox (2010), lack of teacher buy-in was a major barrier for implementing SMH services. Buy-in from administrators tends to diffuse toward teachers and other staff (Massey et al., 2005).
Data suggest that PBIS and SMH initiatives are effective in ameliorating behavioral issues and promoting academic success. Bradshaw et al.’s (2010) examination of Tier I PBIS indicated that over 5 years in 37 Maryland public schools, both the number of student discipline referrals and suspensions decreased significantly. Check-In/Check-Out (Tier II) resulted in significant decreases in student discipline referrals and teacher ratings of student problem behaviors (McIntosh et al., 2009), as well as decreases in the frequency and severity of problem behaviors (Todd et al., 2008). Positive effects of standardized test scores and reductions in office discipline referrals and suspensions were also observed (Lassen et al., 2006). Similarly, promotion of SMH has been linked to increases in school performance. By improving students’ overall well-being, other peripheral concerns that are detrimental to academic achievement (e.g., discipline referrals, truancy, drop outs, and lack of school engagement) are ameliorated (Stephan et al., 2007).
Unfortunately, bringing PBIS and SMH together can be difficult for school district personnel. Many schools and districts, even those presently using PBIS in any capacity, may be unprepared to integrate SMH services into their current programming. A central barrier to PBIS–SMH interconnection is the lack of a measure to evaluate the readiness of schools and districts for undertaking this process. Evaluating readiness is the first part of PBIS–SMH interconnection, which is a multistep process. Without such a measure, program implementers and school leaders do not have a formal method by which to gauge the level of preparedness for PBIS–SMH interconnection. When stakeholders perceive an intervention as unnecessary, too expensive, or incompatible with their values and beliefs, the intervention is likely to fail (Fixsen, Naoom, Blase, Friedman, & Wallace, 2005). Thus, evaluating readiness for intervention implementation allows interventionists to identify sites in which stakeholders are likely to endorse the plan.
Prior to interconnecting PBIS and SMH, it is imperative to consider issues surrounding readiness to adopt change. This is an especially critical step, as PBIS–SMH interconnection is likely an unfamiliar concept. Readiness for integrating PBIS and SMH can be conceptualized using the science of implementation framework by Fixsen and colleagues (2005). This framework includes the steps of exploration and adoption, program installation, initial implementation, full operation, innovation, and sustainability. The first phase of this framework is exploration and adoption, in which a program is investigated to determine its goodness of fit with current issues, needs and resources of the community, and needs regarding evidence-based practice and programming. Based on the information gathered during exploration, a choice is made regarding whether to adopt and implement the intervention or continue use of current programming. If the intervention will be adopted, a plan for implementation is developed, with ideas for facilitating operations and reducing any barriers that would hinder implementation. Readiness is a critically important construct on whether a school or program moves through initial steps of embracing and beginning to implement an innovation as reviewed here.
The literature is somewhat limited regarding readiness to implement PBIS and SMH. In a qualitative study, Savage, Lewis, and Colless (2011) found that school readiness for school-wide PBIS implementation is necessary prior to adopting the intervention, as well as after for sustainability purposes. Initial implementation was also facilitated due to the involvement of all school personnel, from administrators to teachers to support and custodial staff. The authors also indicated that readiness consists of perceiving a need for change, being open to acquiring new skills, and having sufficient preparation to implement the intervention. Tools to promote a systematic readiness process are now available on various websites connected to PBIS implementation, including www.pbis.org, www.istac.net, and http://flpbs.fmhi.usf.edu.
Handler et al. (2007) noted several systemic issues germane to readiness for PBIS implementation. For instance, a leadership team consisting of school and community stakeholders should be in place to guide adoption and implementation. Consistent communication between administrators and school staff can encourage adoption and early implementation. In addition, support from the school district is imperative. Specifically, the district must realize that systemic change requires some time, but the benefits of prevention and early intervention will reveal themselves later with improved academic performance and graduation rates and fewer discipline referrals and behavioral problems (Sugai & Horner, 2008).
The Interconnected Systems Framework (ISF) highlights SMH service delivery within a multi-tier PBIS framework (Eber, Weist, & Barrett, 2013). By combining the two systems, the ISF can ameliorate issues with each system (e.g., inconsistent implementation of Tiers II and III in PBIS, lack of data-based decision making in SMH services). Key features of the ISF include utilizing existing education and mental health systems, EBIs, and collaboration among professionals and stakeholders at the state, district, community, and school levels. Furthermore, fidelity and efficacy are assessed regularly, with changes implemented as needed to improve quality of service delivery and outcomes.
According to Paternite and Butts (2013), the ISF is operating in 16 states through each state’s Community of Practice (CoP) in School Behavioral Health, in collaboration with the IDEA Partnership. Paternite and Butts discussed examples from Pennsylvania, Utah, and Montana. These states deliver comprehensive SMH services within the PBIS framework that are child-centered, evidence-based, and data-driven. There is also emphasis on multidisciplinary collaboration and feedback from community stakeholders, families, and youth.
With this limited literature base on readiness for PBIS and SMH implementation, measures for PBIS–SMH readiness are even scarcer. There is also no measure to evaluate readiness to integrate PBIS and SMH, despite calls for development of such a measure (Kincaid, Childs, Blase, & Wallace, 2007). Some measures assess similar constructs such as practitioners’ perceptions of PBIS implementation and attitudes regarding PBIS facilitators and barriers (see Bambara, Nonnemacher, & Kern, 2009; Michaels, Brown, & Mirabella, 2005; Lewis-Palmer, Horner, Todd, & Sugai, 2001), but none directly pinpoint readiness for PBIS–SMH interconnection. Thus, existing measures appear to focus on implementation and fidelity, barriers and facilitators to implementation, and service utilization. The current research aims to remedy this with the preliminary development of a readiness for PBIS–SMH interconnection measure.
Methods
This study involved a mixed method design of qualitative analyses (survey of relevant stakeholders, consultation with key informants) and quantitative analyses (survey development, psychometric analyses) to develop a survey for readiness to integrate PBIS and SMH. Therefore, the study and subsequent analyses are exploratory in nature.
This study was carried out in four phases. The first phase was a pilot study, conducted in September of 2011. A sample of key stakeholders with interests in PBIS and SMH were asked to complete an open-ended survey to determine fundamental factors for satisfactory implementation and interconnection of PBIS and SMH. Following the pilot study, Phase II involved aggregating and qualitatively analyzing these data to develop common themes relevant to PBIS–SMH interconnection. In addition, the principal investigator (PI) consulted with experts in PBIS, SMH, and related fields and reviewed the applicable literature. This information was used to develop a 35-item readiness for PBIS–SMH interconnection survey.
In Phase III of the study, the 35-item survey was revised further through additional literature review and consultation with experts in PBIS and SMH and survey construction. Based on these consultations, survey items were revised, added, or discarded accordingly. New items were added to capture constructs identified through the literature review and consultations, resulting in a 98-item survey. Lastly, Phase IV included converting the survey to an online format, disseminating the survey to potential participants via email, and collecting and analyzing the data. All four phases of the study were reviewed and approved by the Institutional Review Board of the sponsoring university. Each phase of the study is discussed further below.
Procedure
Phase I: Pilot study
A pilot study was conducted in September 2011 at a national SMH conference. Key PBIS and SMH stakeholders in attendance were asked to complete a brief, open-ended survey regarding barriers and facilitators of PBIS, SMH, and readiness for PBIS–SMH interconnection. The survey is based on work by Horner et al. (2004) and Levesque, Prochaska, and Prochaska (1999). Items on this survey addressed PBIS and SMH implementation (derived from Horner et al.’s survey), as well as the construct of readiness from Levesque and colleagues. Sample items included “What are the top five factors promoting effective expanded school mental health services?” and “What are the top five factors that would facilitate PBIS and school mental health integration?”
Participants included 25 key PBIS/SMH stakeholders (72% female) who, on average, have been working in their respective fields for 22 years and included disciplines of government official (n = 5), family member/advocate (n = 5), director of state PBIS center/state-wide PBIS projects (n = 3), and technical assistance provider/coordinator (n = 3). The latter part of the survey asked participants to rate the current status and priority level of 10 features of PBIS and SMH services in their school. Of nine raters, 65.56% indicated that these features were currently in place, 26.67% stated the features were partially in place, and 7.78% reported that they are not in place. Regarding priority level, 35.71% noted the features were of high priority, whereas 34.29% and 30.00% indicated medium and low priority, respectively. Participants were also asked to indicate the top five factors in each of the following categories: promoting effective PBIS, hindering implementation of PBIS, promoting effective expanded school mental health (ESMH) services, challenges to providing effective ESMH services, and facilitating PBIS–SMH interconnection.
Phase II: Development of preliminary survey
Responses to the pilot survey were compiled, summarized, and distilled into 20 themes. The PI and second author listed all responses and cataloged similar responses into groups. As responses were cataloged, 20 themes emerged from the data. A complete listing of the themes is found in the appendix. Bambara et al.’s (2009) study regarding barriers and enablers of positive behavior supports for individual students revealed many similar themes. Following the development of the 20 themes based on the pilot study data, as well as literature review of PBIS and SMH adoption and implementation, a 35-item preliminary survey was distributed via email to key informants with expertise in PBIS, SMH, and related fields. Information regarding the survey content, wording of each item, length of the survey, and other thoughts was solicited from this group. Participants in this phase included 12 key informants, all members of the IDEA Partnership’s (n.d.) National Community of Practice (CoP) on Collaborative School Behavioral Health. This group, which is co-sponsored by the IDEA Partnership (led by the National Association of State Directors of Special Education) and the Center for School Mental Health at the University of Maryland, includes stakeholders interested in promoting positive mental health and behavior for youth in their schools and communities.
The Phase II participant sample consisted of eight females and four males working in the fields of clinical psychology, special education, public health, student support services, education administration, and social work, with years of experience ranging from 5 years to more than 25 years. Participants were asked to rate each survey item on its importance to PBIS–SMH interconnection using a 6-point scale, with 1 being “not at all important” and 6 being “essential.” In addition, participants were asked to comment on the items or edit the wording as they saw fit.
Based on these ratings, items regarding communication between schools and communities, participation in school activities, and school teams’ awareness of community data were removed. These items fell below a threshold of 4.70 based on a scatter plot. The language of the survey was edited according to participants’ suggestions to increase clarity and specificity of meaning (per suggestions from four participants). Items containing multiple ideas were broken into separate questions. Some items included a stem with sub-items for respondents to rate. Items were rewritten to reflect a single idea, so as to facilitate data interpretation later (Saris & Gallhofer, 2007). Furthermore, key terms used in the survey (e.g., PBIS and SMH) were defined prior to the survey items (Fink & Kosecoff, 1998; Fowler, 1995). Survey items were further revised through consultation with a nationally recognized survey expert.
Phase III: Consultation and final revisions
Following modifications to the preliminary survey based on input from key informants in Phase II, the revised survey was then distributed via email to several members of the National CoP for School Behavioral Health. These individuals are all experienced in SMH, and have interest in joining SMH with the PBIS framework. After discussing the survey items and intended future use of the survey on a conference call, conference call participants were invited to email their survey comments to the PI. Two participants provided feedback, and the survey was revised to reflect their suggestions. This draft of the survey was forwarded to the study’s co-authors. Following a final edit based on their comments, the survey was formatted and finalized for dissemination. The final survey included 98 items. On a second conference call, the authors and National CoP for School Behavioral Health members discussed the final draft and survey dissemination strategies.
Phase IV: Dissemination of major survey and data collection
In this final phase of the study, a link to the major survey on SurveyMonkey.com was distributed to potential participants via email and postings on websites of relevant professional organizations. A list of email addresses was assembled with listservs from Center for School Mental Health (CSMH), the National CoP on School Behavioral Health, and other related organizations and individuals. The 98-item survey took about 15 min to complete. Participation was anonymous, and only basic demographics were collected in addition to the survey responses. As an incentive for participation, participants could provide their contact information and be entered into a drawing to receive a $100, $75, or $50 gift card. This information was stored separately from survey responses.
Participants
Participants included 346 individuals from a national sample. The National CoP for School Behavioral Health played an integral role in guiding and promoting interest in the survey. The major survey was discussed on several of their regularly scheduled conference calls. Furthermore, the survey and corresponding link were advertised through postings on National CoP listserv announcements, as well as websites of affiliated organizations. The target population for the study was school and community stakeholders, teachers, administrators, family members, mental health practitioners, and other professionals working with PBIS and SMH. Inclusion criteria for participants were individuals who are currently working in a setting using PBIS and SMH (e.g., a school or school district), delivering mental health services to youth enrolled in school, and/or community members who support PBIS and SMH services.
Of the 346 participants, 273 (78%) completed the major survey. This sample more than satisfies recommendations from Everitt (1975), Kline (2010), and Loehlin (2004) to ensure valid factor analyses. The following demographics describe those who completed the survey in its entirety (also refer to Table 1). Most participants were female (n = 214, 78.4%). The majority identified as school social workers (n = 56, 20.5%). Other highly represented professions included general education teachers, school psychologists, and school administrators. Participants also worked at the state, district, and building levels, with most indicating the latter (n = 172). (Refer to Table 2 for further information.) Practitioners with 25 or more years experience in their field comprised 20.9% of the sample. In terms of school level, 38.5% of participants worked in elementary (K–5) schools. Most participants worked in non-metropolitan urban settings, defined as areas having more than 2,500 but less than 250,000 residents (50.9%). Also, 15.4% of participants worked in settings where 41% to 50% of students received free or reduced lunch.
Major Survey Participant Demographics.
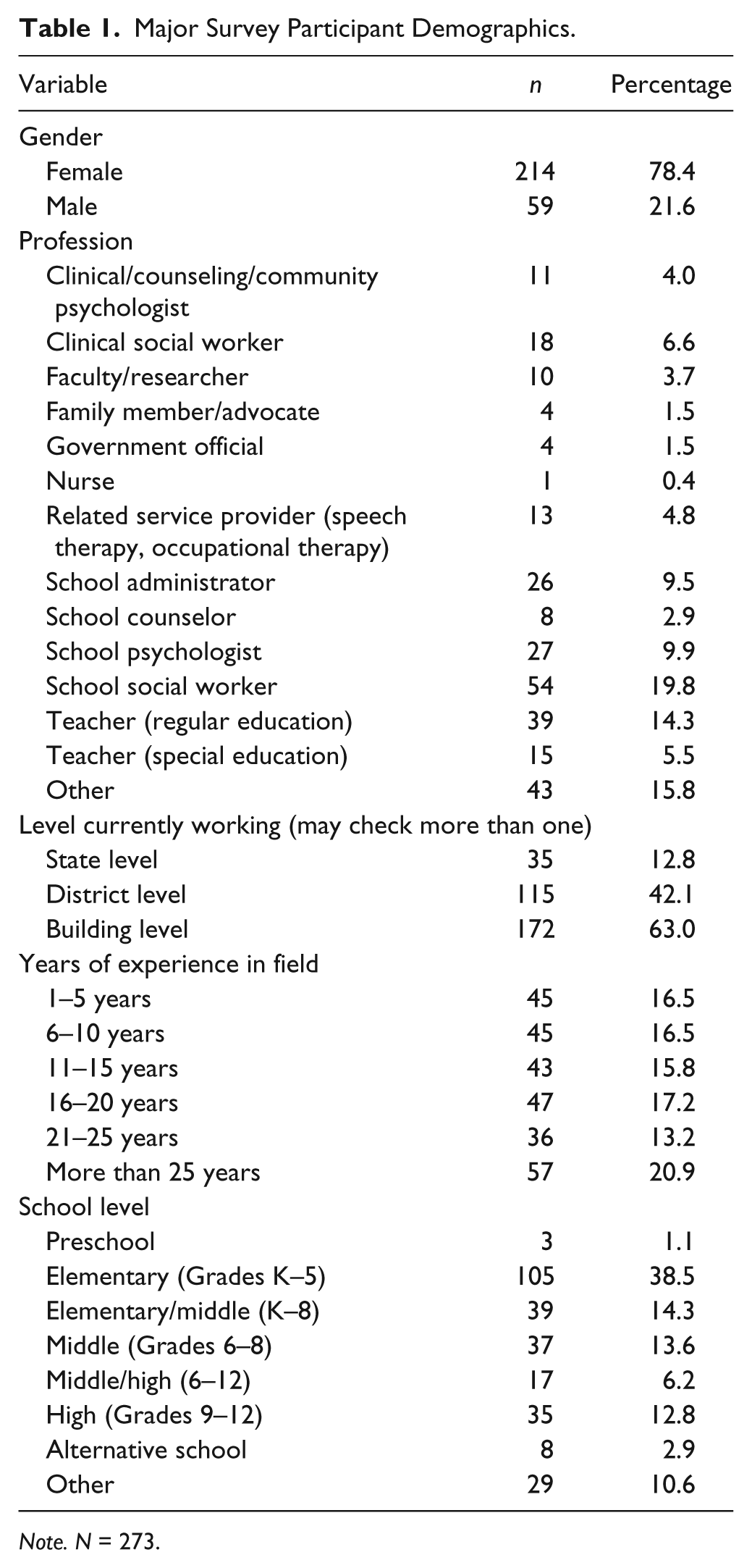
Note. N = 273.
Demographics by Profession and State/District/Building Level.
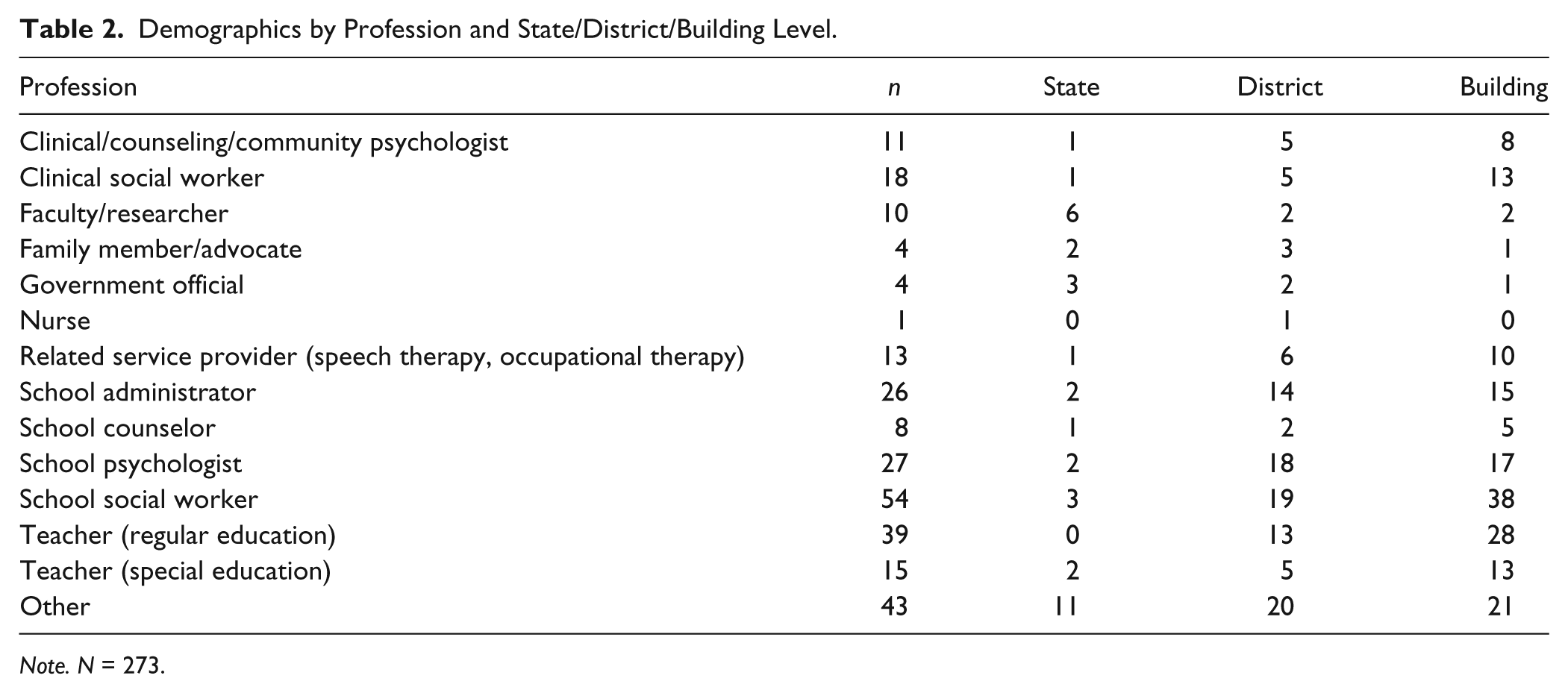
Note. N = 273.
Results
According to descriptive analyses, all responses were normally distributed. Skew and kurtosis index scores were within normal limits. Item means ranged from 2.01 (SD = 0.72) to 3.16 (SD = 0.76). Spearman’s rho correlations ranged from –.19 to .89. Cronbach’s α of .98 indicated a high level of internal consistency. A priori between-group analyses were planned to evaluate differences in responding by profession; however, due to the small n per each group, there was insufficient power to detect meaningful group differences (Cohen, 1988).
Following these analyses, a confirmatory factor analysis (CFA) was conducted to ascertain if the survey items load onto the following factors: support/buy-in/resources, collaboration and teamwork, positive student outcomes, and use, understanding, and applications of PBIS. These factors were selected based on the pilot survey data and subsequent key themes, as well as Bambara et al. (2009) and Handler et al. (2007). Factor analyses were carried out using MPlus software (Muthén & Muthén, 1998–2011), whereas all other analyses were calculated with SPSS software (IBM, 2011). The CFA was conducted using the specified model and the weighted least squares parameter estimation (WLSMV), with various model fit estimates examined. The root mean square error of approximation (RMSEA) estimate was .082. According to Hu and Bentler (1999) and MacCallum, Browne, and Sugawara (1996), an RMSEA estimate of .05 is indicative of good model fit, whereas .08 suggests a “mediocre” model fit. The comparative fit index (CFI) of .83 was below the recommended cutoff of .95 (Brown, 2006; Hu & Bentler, 1999). Although the CFI for this sample approached the cutoff, this suggested that the hypothesized model is not an optimal representation of the data. Similarly, the Tucker–Lewis index (TLI) of .83 was below the suggested cutoff of 1.00 (Brown, 2006). Based on the current sample, these estimates did not support the hypothesized factor structure as a strong model.
Thus, an exploratory factor analysis (EFA) with WLSMV was conducted to develop a factor structure from the data. WLSMV is robust to variation in model complexity, sample size, and non-normality (Brown, 2006; Muthén & Muthén, 1998–2011). To promote a theoretically strong factor structure, the number of factors was limited to four. Eigenvalues from the EFA were examined using the scree test. In Figure 1, the line drops sharply at one, indicating a one-factor solution for the survey. Because the data suggested a one-factor solution as opposed to the originally hypothesized four-factor structure, readiness to interconnect PBIS and SMH may be a unitary construct. This is examined further in the Discussion section.
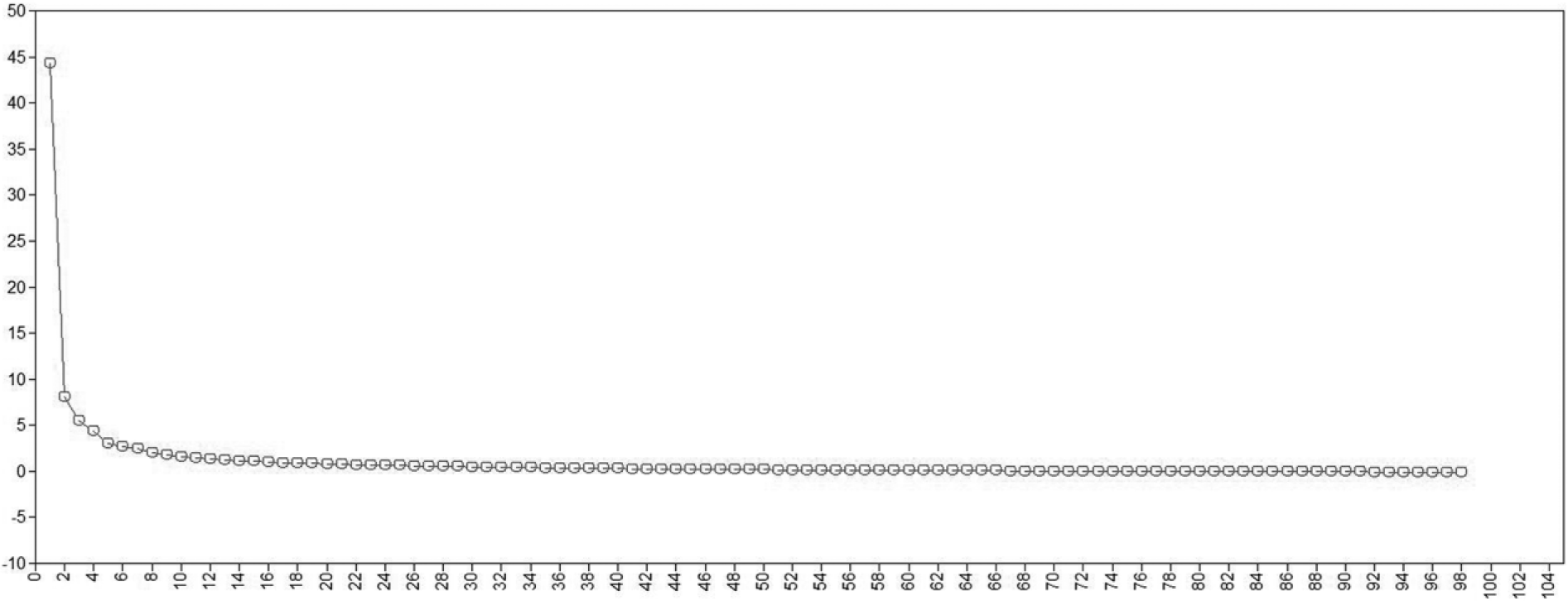
Scree plot for exploratory factor analysis.
The EFA data were evaluated further to determine which items should be removed from the survey to promote survey use and utility. Eigenvalues for each item under the single-factor structure ranged from .436 to .895. Recommendations for eigenvalue cutpoints vary; Kline (2010) suggested .50, whereas Sterba (2011) reported using eigenvalues of .70 or greater for high indicator loadings, per Nunnally and Bernstein’s (1994) recommendation. For this study, a rigorous cutoff score of .70 was used. Thus, 62 items of the original 98 remained. The additional item “PBIS and SMH teams meet together” was also retained, as communication between these two groups is essential to PBIS–SMH interconnection. Thus, the final survey has 63 items, including 34 major items with some items having sub-responses. Some items were slightly reworded through consultation with PBIS–SMH experts to increase clarity. An α of .98 suggested excellent internal consistency, and was the same α calculated for the original survey.
Discussion
Although pairing PBIS and SMH is advantageous to students, schools, families, and communities, it can be a large undertaking. To ensure that PBIS–SMH interconnection is productive and useful to the school and community, it is imperative to evaluate readiness prior to installation and implementation (Fixsen et al., 2005). To support the successful adoption and installation of the intervention, stakeholders and school staff must view the intervention as a potential solution to problems identified within the school community. If they are not prepared to take action to address these problems, the intervention has a small chance of success.
The interconnection of PBIS and SMH is an essential next step in promoting improvements in children’s behavior and functioning across domains. As outlined by Eber et al. (2013) in the ISF, SMH services can be integrated within the multi-tiered framework of PBIS, allowing parents, teachers, mental health professionals, and others to tailor the intervention to the student’s unique needs. Furthermore, PBIS is an evidence-based framework (see Sugai, Horner, et al., 2000; Sugai, Sprague, et al., 2000), and is featured on the National Registry of Evidence-Based Programs and Practices (NREPP) of the Substance Abuse and Mental Health Services Administration (SAMHSA). Similarly, there are many evidence-based mental health interventions and prevention strategies available to meet a variety of needs (Browne, Gafni, Roberts, Byrne, & Majumdar, 2004; Splett & Maras, 2011), as well as studies examining strategies to overcome barriers to implementation (Langley et al., 2010; Reinke, Stormont, Herman, Puri, & Goel, 2011; Schaeffer et al., 2005). In addition to the variety of benefits of the ISF, this is a practical way to increase the availability of mental health services in the schools. PBIS and SMH fit together to promote better mental health, as well as academic and socioemotional competence.
The development of an initial survey to assess the readiness for PBIS–SMH interconnection survey is a timely addition to the field and the literature. This survey and the study of its psychometric properties can provide interventionists and researchers with a starting point for gauging preparedness of schools and communities to integrate PBIS and SMH. Prior to the current study, no such measure existed despite a critical need for this tool discussed in the literature to move this line of research and intervention forward (Kincaid et al., 2007).
Through a pilot study and consultation with experts in the fields of PBIS, SMH, and survey construction, the original 98-item survey was developed. A CFA indicated that the hypothesized four-factor structure (support/buy-in/resources, collaboration and teamwork, positive student outcomes, and use, understanding, and applications of PBIS) was not an optimal representation of readiness. An EFA revealed a single-factor structure, with item eigenvalues ranging from .436 to .895. Therefore, readiness for PBIS–SMH interconnection appears to be a unitary construct. To facilitate interpretability of results, items with eigenvalues below .70 were removed. The survey was revised through consultation with PBIS–SMH experts, resulting in a 63-item survey with 34 major questions and some sub-items for selected questions.
The single-factor structure has several important theoretical implications. The hypothesized four-factor structure was not supported by the data, despite research highlighting these factors as integral players in intervention adoption and implementation (Fixsen et al., 2005; Handler et al., 2007; Nastasi & Hitchcock, 2009). From a practical applications perspective, key elements must be in place to successfully adopt and implement any intervention (Fixsen, et al., 2005). However, the current study does not support discrete sub-factors of the overarching PBIS–SMH readiness construct, although several areas contribute to the single construct. Nevertheless, it is imperative that interventionists examine various areas for adequate buy-in and resources prior to adoption and installation. For example, a lack of teaming structures may undermine the success or, at the very least, attenuate the intervention’s success.
In addition to raising awareness of readiness issues in general, the Readiness for PBIS–SMH Interconnection Survey has utility on several fronts. First, being available online at no cost (see Anello & Weist, 2013) removes the barriers of accessibility that often influence intervention adoption and implementation in the schools. Because assessment and intervention are iterative processes, the survey can be used at multiple time points to evaluate readiness as schools and communities move toward full implementation of PBIS–SMH interconnection. Also, communities and school districts may use the survey to identify pilot schools for PBIS–SMH interconnection that may later serve as exemplars of the intervention.
Furthermore, the survey can guide school and community leaders as they invest in building PBIS–SMH interconnection. Because implementation of PBIS (Spaulding et al., 2008) and SMH (Splett & Maras, 2011) can vary so greatly, an examination of resources and fidelity can assist schools in carrying out PBIS and SMH interventions as designed by their developers. From that point, schools may evaluate their SMH delivery, available services, and partnerships with service providers in the community. Discussing these issues can lead to opportunities for building buy-in and support among administrators, school staff, and community members. The power of these working relationships should not be underestimated. Social capital can be quite influential when building support for new initiatives (Mellin & Weist, 2011).
In addition to identifying implementation supports, the survey also points to several paradigm shifts necessary to move ISF research and practice forward. Because PBIS and SMH focus on student needs and supporting their academic and socioemotional growth, merging these systems can emphasize person-centered approaches to service and intervention planning. The introduction of cross-systems problem solving teams also brings a multidisciplinary approach to ameliorating issues identified by key stakeholders (Eber et al., 2013). By evaluating readiness and the needs of the students and the community, schools and districts can introduce new services to address these issues, as well as modifying current services and delivery modalities accordingly. Similarly, decisions for intervention selection and service delivery are data- and evidence-based, which can facilitate decision making and determining next steps.
The availability of readiness data about PBIS/SMH integration may be useful to community and school leaders as they work together to resolve the fragmentation of youth mental health services. Unfortunately, there is still a lack of coordination and communication among the various professionals working with school-age youth experiencing mental health issues (Kerns et al., 2014). Communication among service providers, regardless of modality, is in the best interest of the populations served. By allowing for more communication among these service providers, some of whom may be unaware that they are serving the same students, consistency in service provision can be increased, while the redundancy of some services may be reduced. According to Eber et al. (2013), a key feature of ISF implementation is increasing communication and coordination of services among service providers. By having professionals from various disciplines lead and serve on teams at multiple points of intervention, providers are able to collaborate and streamline services, which can lead to maximizing resources and delivering effective EBIs. Furthermore, systematic progress monitoring and fidelity checks are built into the ISF, which is also crucial for intervention effectiveness. This collaboration is especially timely, in light of mental health care reform and corresponding changes in health care legislation.
The survey also fits with recent research on classroom management interventions. These interventions point to the need for measurement of readiness to implement interventions, as well as ongoing measurement of integrity and fidelity of implementation. Farmer, Reinke, and Brooks (2014) discussed classroom management strategies within the framework of linking behavioral and ecological perspectives via social-interactional considerations. Supporting students with emotional and behavioral problems requires addressing these concerns within the contexts of classroom, school, and community. Furthermore, there are several domains of classroom functioning, including learning, classroom procedures, and social interactions, to consider when selecting an appropriate intervention. Thus, the readiness survey can be used to bridge research and practice for implementation of EBIs in classrooms, as well as in identifying needs according to the various contexts discussed by Farmer and colleagues.
Similarly, Kern et al. (2015) discussed implementation of the Center for Adolescent Research in Schools (CARS) intervention with secondary students experiencing emotional/behavioral problems. The authors used an iterative process and data-based decision making to tailor the intervention to students’ needs, as well as implementing the minimally sufficient level of intervention necessary. Data were collected on a variety of outcomes, including student factors such as academic achievement scores, as well as measures of life satisfaction, anxiety, and depression. Observational data of teachers’ classroom practices was also collected, in addition to office discipline referrals, suspensions, absences, and students’ use of community mental health services. Perceptions of intervention feasibility and acceptability were also assessed. The authors’ focus on linking school and community mental health services, in addition to providing the level and type of intervention necessary according to student and school needs, is key for promoting buy-in and integrity of implementation.
Motoca et al. (2014) studied the directed consultation model within a professional development context and its effects on teachers’ classroom management. In this consultee-focused intervention, sixth-grade teachers participated in the Supporting Early Adolescent Learning and Social Supports (SEALS) program, with the aim of fostering supportive classroom environments for students transitioning to middle school. By using structured classroom observations, the authors evaluated teachers’ classroom management practices pre- and post-intervention. As compared with control classrooms, teachers who participated in the intervention were rated higher on positive feedback to students, behavior management, classroom structure, communication with students, instructional protocols, communication, and the use of groups and social dynamics. By integrating an evidence-based classroom management intervention within an ecological framework, teachers were given targeted strategies to embed in their instruction.
Limitations
The current study has several limitations. First, survey methodology is susceptible to influence by social desirability or personal biases. Although Heerwegh (2009) suggested that online surveys come with an inherent sense of mistrust for data security and confidentiality, it is unlikely that this affected responding to the current survey. Because the survey did not include any personal or sensitive questions, and asked for only general demographic information (e.g., gender, job title), there was a low risk of social desirability bias and concerns for confidentiality.
Another limitation concerns group analyses. For the major survey, the number of total participants exceeded minimum recommendations for conducting factor analyses. However, the ns for groups by discipline (e.g., clinical psychologist, teacher) were not large enough to conduct inter-group analyses due to insufficient power. Further studies may examine differential responding to this preliminary survey according to discipline or training.
The use of an online survey format is both a strength and a limitation. On a positive note, online surveys are relatively quick and inexpensive to administer. Because the majority of the target population has internet access, many participants can be reached via email. However, participants may receive many unsolicited emails, and may not wish to participate in yet another survey. Also, participants may “multitask” and complete other jobs (e.g., returning phone calls) while completing the survey (Heerwegh, 2009), which may result in inaccurate responding.
As this survey is a first step in interconnecting PBIS and SMH, there is still much work to be done to validate and strengthen the measure. Although schools and communities may wish to use the survey as part of a needs assessment before interconnecting PBIS and SMH, users of the survey are encouraged to use multiple sources of data in their needs assessment.
Future Research Needs and Practice Implications
Although the current survey provides a needed resource to PBIS–SMH interventionists and practitioners, this is an initial step in the PBIS–SMH interconnection. Further research is necessary in several related areas. First, future studies should focus on establishing the predictive validity of the measure. This would involve measuring readiness at multiple points in the intervention adoption and early implementation phases, and examining any correlations with readiness at these stages and the later degrees of success in interconnecting PBIS–SMH services.
Furthermore, subsequent research should examine methods to score the measure. Presently, schools and communities may qualitatively evaluate readiness by comparing areas where respondents indicated established areas of support, and where there are reported areas of weakness. In the future, establishing score ranges can provide users of the survey with a general idea of their level of readiness. For the final (short) version of the survey, scores would range from 63 to 252 (based on scoring of 1 to 4 per item). If a rating of 75% were indicative of readiness (i.e., an average rating of 3 or higher on survey items), then scores of 189 or higher would indicate strong readiness for PBIS–SMH interconnection. Scores of 126 to 188 would indicate that the school or community is somewhat ready (i.e., average ratings of 2 to 3), and scores of 125 or lower would suggest inadequate readiness (again note that these scores and this example are hypothetical). Item analyses would then be conducted. Empirical studies are needed to establish score cutpoints and predictive validity, and to further refine the survey.
Similarly, future research is needed to examine the factor structure of the survey. According to the current data, readiness for PBIS–SMH interconnection was a unitary construct. However, further study is needed to examine this single-factor structure and clarify any differential responding based on participants’ profession or other germane factors.
An established PBIS–SMH interconnection can provide a solid foundation for the organization and delivery of EBIs that are progress-monitored over time. An additional need is to examine the fidelity and impact of PBIS–SMH interconnection (several measures are available at www.pbis.org). In terms of ISF impact, such measures could assess several larger-scale issues, such as cases of social services involvement with families and cost-effectiveness of mental health service delivery in the schools. Mental health service utilization can also be monitored, as Kern et al. (2015) demonstrated, in addition to the number of severe behaviors observed (e.g., self-injurious behaviors). Although PBIS–SMH interconnection must be well-established in schools and communities, research on its larger influence could provide further support for this intervention.
The current study addresses a long-standing gap in the literature regarding the development of measures assessing readiness to implement interventions. Furthermore, in spite of the growing interest in PBIS–SMH interconnection, there was no measure to evaluate the readiness and motivation within schools and communities to do so. The current study is a beginning step in remedying this issue. By developing a psychometrically sound measure to evaluate readiness for PBIS–SMH interconnection, more attention is being drawn to ways to feasibly provide SMH services that are accessible, cost-effective, and driven by the needs of students, schools, and communities. Needs assessments conducted by Kern et al. (2015) and Motoca and colleagues (2014) in their respective studies show how consultee- and student-driven interventions are viewed as more acceptable and necessary to cope with behavioral and mental health issues. Moreover, PBIS–SMH interconnection fosters the collaboration of professionals from many backgrounds, fields, and work environments. By combining their efforts, these professionals can support students in a variety of ways to encourage academic achievement, social skill development, and coping skills. It is our hope that Readiness for PBIS–SMH Interconnection Survey helps to facilitate this progress.
Footnotes
Appendix
20 Themes of Positive Behavioral Interventions and Supports (PBIS) and School Mental Health (SMH) Interconnection From Pilot Study
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.