
Abstract
Accumulating evidence shows callous–unemotional (CU) traits to delineate a subgroup of youth with unique etiological underpinnings to their conduct problems. Due to its inclusion as a conduct disorder specifier in Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), research that evaluates the psychometric properties of measures used to assess this construct is essential. The present study contributes to this area of investigation by examining two recently developed brief versions (10- and 12-item) of the Inventory of Callous–Unemotional Traits (ICU) among a Portuguese sample of incarcerated male juvenile offenders (N = 221). Each of these shortened versions demonstrated evidence in terms of factor structure, internal consistency, and convergent/discriminant validity with theoretically meaningful constructs. In line with prior research, there was evidence of unique correlations between separate ICU subscales and several outcomes of interest. Study findings indicate that the two shortened versions of the ICU, and particularly the ICU-12, may offer researchers and clinicians a relatively brief and psychometrically sound means of assessing CU traits.
Research demonstrates that psychopathy is a higher order construct comprised of several underlying facets (e.g., interpersonal, affective, behavioral). Callous–unemotional (CU) traits (e.g., lack of guilt, inability to show emotions, and affective empathy) represent a set of characteristics that are analogous to the affective features of adult psychopathy. A growing body of research indicates that CU traits delineate a subgroup of conduct problem youth having a particularly recalcitrant form of disruptive and antisocial behaviors (Feilhauer & Cima, 2013; Frick & White, 2008; Pechorro, Jiménez, Nunes, & Hidalgo, 2016). This subgroup of youth engages in more severe and persistent disruptive behaviors, shows differences in primary caregiver and teacher attachment quality, and has poorer treatment response compared with conduct disordered youth with normative levels of CU traits (Crum, Waschbusch, & Willoughby, 2016; Edens, Campbell, & Weir, 2007; Frick, 2009; Frick & White, 2008; Salekin & Lynam, 2010; Waschbusch, Graziano, Willoughby, & Pelham, 2015). Furthermore, research increasingly suggests that distinct etiologies may underlie the notably recalcitrant maladaptive behaviors recognized among these youth (Frick, Ray, Thornton, & Kahn, 2014; Frick & White, 2008).
Highlighting the growing importance of research into CU traits, the latest version of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) includes a severity specifier for diagnosing conduct disorder (CD) based on conceptualizations of CU traits (i.e., “With Limited Prosocial Emotions”), requiring that two or more of the following characteristics be present across multiple settings for at least the past 12 months: lack of remorse or guilt, callousness–lack of empathy, lack of concern about performance in important activities, and shallow or deficient affect. One measure that has become widely used for assessing these characteristics in youth is the Inventory of Callous–Unemotional Traits (ICU; Kimonis et al., 2008). The ICU was originally developed to address the limitations of existing instruments, namely, the Psychopathy Checklist: Youth Version (PCL:YV; Forth, Kosson, & Hare, 2003) and the Antisocial Process Screening Device (APSD; Frick & Hare, 2001), by providing a more comprehensive and precise assessment of CU traits (Kimonis et al., 2008). This measure includes four items directly referenced in the “Limited Prosocial Emotions” DSM-5 specifier (“I care about how well I do at school,” “I feel guilty when I do something wrong,” “I do not show emotions,” and “I am concerned about the feelings of others”). Although the ICU has demonstrated important advancements in our understanding of CU traits in youth, concerns remain regarding the measure’s psychometric properties and the manner by which the construct of CU is conceptualized (Lahey, 2014).
Essau, Sasagawa, and Frick (2006) conducted the first confirmatory factor analysis (CFA) of the ICU among a large (N = 1,443) community sample of youth (age range = 13–18 years) using a self-report version of the ICU. These authors found that ICU items best fit a bifactor model composed of three underlying dimensions (Callous, Uncaring, and Unemotional) and an overarching CU factor. Several studies since then have supported the bifactor structure of the ICU as the best option across culturally distinct samples and varying informant versions (i.e., self, parent, and teacher) of the measure (i.e., Byrd, Kahn, & Pardini, 2013; Ciucci, Baroncelli, Franchi, Golmaryami, & Frick, 2014; Fanti, Frick, & Georgiou, 2009; Kimonis et al., 2008; Roose, Bijttbier, Decoene, Claes, & Frick, 2010). However, across these studies, model fit has typically ranged from poor to acceptable, often only being achieved subsequent to a number of post hoc adjustments to the model. In addition, other studies have not supported a bifactor model, and have suggested that alternative two- (Houghton, Hunter, & Crow, 2013) and five-factor (Feilhauer, Cima, & Arntz, 2012) solutions were the best fitting models.
The lack of a consistently well-fitting factor structure for the ICU indicates that some items are likely not tapping into the underlying CU construct as intended by the measure. Several studies have provided evidence indicating that a number of these poorly functioning items may be those that are often considered to tap into the “unemotional” facet of the construct. These studies have shown the Unemotional factor to demonstrate less robust associations with theoretically relevant outcomes (e.g., CD, aggression, and antisocial outcomes) and other existing measures of CU traits in comparison with the Callous and Uncaring factors (Ciucci et al., 2014; Essau et al., 2006; Fanti et al., 2009; Fink, Tant, Tremba, & Kiehl, 2012; Kimonis et al., 2008; Latzman, Lilienfeld, Latzman, & Clark, 2013; Roose et al., 2010). These issues have led several research groups to develop projects focused on refining the ICU with the goal of enhancing the measure’s ability to tap into the CU construct as intended, and as a result improve the psychometric properties of the instrument.
Recently, Hawes, Byrd et al. (2014) conducted a series of analyses intended to aid in refining the parent-report ICU measure. This study employed CFA and item response theory (IRT) techniques to investigate the functioning of the ICU among a sample of 250 boys (age range = 6–12 years) with conduct problems. Results of this study led to a shortened 12-item version of the ICU, consisting of a “Callous” and an “Uncaring” factor, with the majority of the items from the original “Unemotional” factor being removed. This shortened 12-item version of the ICU demonstrated good model fit, high levels of internal consistency and test–retest reliability, and expected associations with relevant outcomes (e.g., dimensions of oppositional defiant disorder (ODD), conduct problems, social competence) that were nearly identical to that of the full measure. In addition, the factor structure for this 12-item ICU maintained good fit when replicated using a self-report version of the measure among an independent sample of adult males (n = 425).
In addition to the 12-item ICU, a recent study by Ray, Frick, Thornton, Steinberg, and Cauffman (2016) adopted similar procedures focused on refining the self-report ICU measure. This study included 1,190 male juveniles (ages ~13–17) processed for first-time offenses. The main purpose of the study was to examine if item wording (i.e., positive and negative) contributed to a possible method effect as suggested by prior research (e.g., Hawes, Byrd et al., 2014). Findings from this study suggested that a method effect did appear to influence the underlying structure of the ICU measure. Subsequently, these authors investigated a 10-item short version (ICU-10) of the ICU, and reported similar estimates of reliability and validity among the 10-item, 12-item, and full measures of the ICU.
It is important to mention that although both short forms resolved various problems that have been reported previously regarding the ICU, they do not include all items that have been selected to assess the DSM-5 Limited Prosocial Emotions specifier criterion (Colins, Andershed, Hawes, Bijttebier, & Pardini, 2016; Kimonis et al., 2015). For example, the ICU-12 does not include the “Unconcerned about performance” characteristic, and the ICU-10 does not include “Shallow or deficient affect” characteristic.
Convergent/Discriminant Validity
Juveniles involved in the justice system exhibit high rates of mental health problems, and CU traits identify a particularly impaired group among these youth (Colins et al., 2016). Theory and prior research suggest that CU traits demonstrate a unique relationship with internalizing and externalizing forms of psychopathology, as well as criminal behaviors. With regard to convergent validity, high levels of CU are associated with an earlier onset of CD and engagement in more severe antisocial behaviors and criminal acts (Frick, 2006; Pardini & Frick, 2013). Alternatively, in terms of discriminant validity, CU traits have also been linked to deficits in affective responsivity (Blair, Colledge, Murray, & Mitchell, 2001; Frick et al., 2003). In particular, research indicates that increased levels of CU are related to a diminished, and in some cases negative relationship with internalizing facets of psychopathology (e.g., anxiety; Frick, Lilienfeld, Ellis, Loney, & Silverthorn, 1999; Hofmann, Korte, & Suvak, 2009; Kimonis, Branch, Hagman, Graham, & Miller, 2013; Pardini, 2006). To date, however, the vast majority of research has examined these associations among community-based samples, with few studies investigating these relationships among justice-involved youth.
Current Study
The development of brief measurement instruments that maintain a high level of diagnostic precision is particularly important in real-world settings, where time and resources are often limited. The ICU-12 and the ICU-10 represent important steps toward refining the ICU measure in this regard. However, to date, there has been no reported examination of these shortened instruments among forensic samples of detained youth offenders. Given the important clinical and judicial implications that accompany the assessment of these characteristics among individuals in a forensic setting, it is essential that such measures accurately reflect their intended construct. The present study is intended to address this gap in the current literature by evaluating the psychometric properties of Portuguese versions of the ICU-12 and the ICU-10 among detained youth. It was hypothesized that (a) the factor structures of the ICU-12 and the ICU-10 would show acceptable fit using CFA methods, (b) the ICU-12 and the ICU-10 would exhibit expected associations with theoretically relevant outcomes used to assess aspects of convergent validity (i.e., psychopathic traits, aggression) and discriminant validity (i.e., anxiety), and (c) the ICU-12 and the ICU-10 scores would be significantly associated with relevant variables used to assess aspects of criterion validity, such as CD, Limited Prosocial Emotions specifier, age of crime onset, increased crime seriousness, use of physical violence, alcohol abuse, and drug use. With regard to our first hypothesis, we based the CFA and item loadings for the ICU-12 on those identified by Hawes, Byrd et al. (2014). However, because Ray et al. (2016) did not conduct a factor analysis of the ICU-10, we based the item loadings for the CFA on those established in previous studies for the full version of the ICU (e.g., Kimonis et al., 2008).
Method
Participants
Male inmates from the eight, nation-wide juvenile detention centers managed by the Portuguese Ministry of Justice voluntarily agreed to participate in the current study (N = 221). Incarceration into juvenile detention centers is the most severe measure that can be taken by Portuguese courts. Seven of the detention centers are considered low to medium security, and one is considered maximum security. The maximum security facility is exclusively used for youth tried as adults (12.7% of participants came from this facility). Participants ranged in age from 13 to 20 years (M = 16.75; SD = 1.41), were primarily from an urban background (92.8%), and were comprised of White Europeans (54.3%), Black Africans (20.5%), mixed-race South Americans (18.6%), and members of other ethnic minorities (6.8%). The participants, on average, became involved in crime at an early age (M = 11.33 years, SD = 2.24 years), were detained prior to the age of 16 (M = 15.46 years, SD = 1.31 years), and had been convicted to an average of 21 months in detention (M = 20.67 months, SD = 6.69 months). The majority (87.6%) of the sample were convicted of having committed serious and/or violent crimes (e.g., homicide, robbery, assault, rape).
Measures
ICU
The ICU (Essau et al., 2006; Kimonis et al., 2008) is a 24-item self-report scale designed to assess CU traits in youth. The measure was developed based on the four items from the APSD (Frick & Hare, 2001) that have most consistently loaded on the CU factor in previous studies (i.e., “Concerned about the feelings of others,” “Feels bad or guilty when he or she does something wrong,” “Cares about how well he/she does at schoolwork,” and “Does not show emotions to others”). For each of these four items, three positively worded and three negatively worded items were created to index similar behaviors, leading to a total of 24 items. Each item is scored on a 4-point ordinal scale ranging from “Not at all true” to “Definitely true.” Essau et al. (2006) using CFA identified three independent factors: Callousness, Unemotional, and Uncaring. All items also loaded onto a general CU factor. Higher scores indicate an increased presence of CU traits. The Portuguese validation of the ICU was used in the present study (Pechorro, Hawes, Gonçalves, & Ray, 2017; Pechorro, Ray, Barroso, Maroco, & Gonçalves, 2016). The internal consistency for the current study, estimated by Cronbach’s alpha, was ICU total = .90, ICU Callousness dimension = .88, ICU Uncaring dimension = .86, and ICU Unemotional dimension = .87.
APSD
The Antisocial Process Screening Device–Self-Report (APSD-SR; Caputo, Frick, & Brodsky, 1999; Frick & Hare, 2001) is a multidimensional 20-item measure designed to assess psychopathic traits in adolescents. It was modeled after the Psychopathy Checklist (Forth et al., 2003; Hare, 2003; Pechorro, Barroso, Maroco, Vieira, & Gonçalves, 2015). Each item is scored on a 3-point ordinal scale ranging from “Never” to “Often” where higher scores are indicative of increased psychopathic features. Prior studies (e.g., Frick, Barry, & Bodin, 2000) have identified three main factors: Callous–Unemotional (six items), Narcissism (seven items), and Impulsivity (five items). To assess convergent validity of the ICU short forms, we used the APSD Callous–Unemotional scale based on a Portuguese version of the APSD-SR (Pechorro, Hidalgo, Nunes, & Jiménez, 2016; Pechorro, Maroco, Poiares, & Vieira, 2013), but it is worth mentioning it was not designed to be a specific refined and improved measure of CU traits. The internal consistency for the current study, estimated by Cronbach’s alpha, was APSD-SR total = .81 and APSD Callous–Unemotional dimension = .68.
Youth Psychopathic Traits Inventory (YPI)
Psychopathy was assessed using the YPI (Andershed, Kerr, Stattin, & Levander, 2002), a 50-item self-report measure designed to assess the core personality traits of the psychopathic personality constellation in youth aged 12 years and above. Each item is scored on a 4-point ordinal scale ranging from “Does not apply at all” to “Applies very well.” The YPI consists of 10 subscales (with 5 items each) designed in line with Cooke and Michie’s (2001) three-dimensional conceptualization of the psychopathy construct, namely, the Grandiose–Manipulative (G-M) dimension, the Callous–Unemotional (C-U) dimension, and the Impulsive–Irresponsible (I-I) dimension. More specifically, the G-M dimension consists of the Dishonest Charm, Grandiosity, Lying, and Manipulation subscales; the C-U dimension consists of the Callousness, Unemotionality, and Remorselessness subscales; the I-I dimension consists of the Impulsivity, Thrill-Seeking, and Irresponsibility subscales. Higher scores reflect an increased presence of the characteristics associated, namely, psychopathic features. To assess convergent validity, we used the YPI-CU subscale based on a Portuguese version of the YPI (Pechorro, Andershed, Ray, Maroco, & Gonçalves, 2015; Pechorro, Ribeiro da Silva, Rijo, Gonçalves, & Andershed, 2017), but it is worth mentioning it was not designed to be a specific refined and improved measure of CU traits. The internal consistency for the current study, estimated by Cronbach’s alpha, was YPI total = .90 and YPI C-U dimension = .70.
Reactive–Proactive Aggression Questionnaire (RPQ)
The RPQ (Raine et al., 2006) is a self-report measure that distinguishes between reactive and proactive aggression. The RPQ consists of 23 items rated on a 3-point ordinal scale ranging from “Never” to “Often.” The reactive aggression scale consists of a summed score across 11 total items (e.g., “Reacted angrily when provoked by others”), while a summed total across 12 items is used for the proactive aggression scale (e.g., “Hurt others to win a game”). Higher scores indicate higher levels of aggression. The RPQ is appropriate for use with youth and young adults. The Portuguese validation of the RPQ was used (Pechorro, Kahn, Ray, Raine, & Goncalves, 2017; Pechorro, Ray, Raine, Maroco, & Goncalves, 2017). Internal consistency for the present study, estimated by Cronbach’s alpha, was RPQ Reactive dimension = .86 and RPQ Proactive dimension = .91.
Social Anxiety Scale for Adolescents (SAS-A)
The SAS-A (La Greca & Lopez, 1998) is an 18-item self-report scale designed to assess subjective experience of social anxiety in adolescents. Each item is rated on a 5-point ordinal scale ranging from “Not at all” to “All the time.” Scores are obtained by summing the ratings for the items comprising each subscale. The Portuguese adaptation of the SAS-A was used (Pechorro, Ayala-Nunes, Nunes, Maroco, & Gonçalves, 2016). Internal consistency for the present study, estimated by Cronbach’s alpha, was SAS-A total = .91.
Sellin–Wolfgang Index of Crime Seriousness (ICS)
Delinquency was assessed in the current study using the ICS (Wolfgang et al., as cited in White et al., 1994). This measure guided the delinquency seriousness classification of the official court reports. Level 0 consists of no delinquency. Level 1 consists of minor delinquency committed at home such as stealing minor amounts of money from mother’s purse. Level 2 consists of minor delinquency outside the home including shoplifting something worth less than 5 euros, vandalism, and minor fraud (e.g., not paying bus fare). Level 3 consists of moderately serious delinquency such as any theft over 5 euros, gang fighting, carrying weapons, and joyriding. Level 4 consists of serious delinquency such as car theft and breaking and entering. Level 5 consists of having performed at least two of each of the behaviors in Level 4.
A CD scale (see, for example, Skilling, Quinsey, & Craig, 2001) based on the DSM-5’s (American Psychiatric Association, 2013) criteria employed to assess CD (e.g., 1. Often bullies, threatens, or intimidates others) was created and utilized by the researchers. The 15 dichotomous items (coded 0 = No; 1 = Yes) were summated to obtain a total continuous score. Thus, higher scores indicate a higher number of positively endorsed indicators of CD. Based on the Kuder–Richardson coefficient, the internal consistency of the CD scale was satisfactory (.77).
A questionnaire was constructed to describe the sociodemographic and criminal characteristics of the participants, to offer a descriptive account of the sample, and to explore the association of some variables (e.g., age of onset) with the ICU-12 and ICU-10. This questionnaire, completed by the researchers, included the following variables: participants’ age, ethnic group, age of crime onset, use of physical violence in committing crimes (coded 0 = No; 1 = Yes), number of officially registered criminal charges, alcohol use (coded as a 5-point ordinal scale), and cannabis use (coded as a 5-point ordinal scale). DSM-5’s CD diagnostic (American Psychiatric Association, 2013), including the “Limited Prosocial Emotions” specifier, was made by the first and second authors of this article using the current official diagnostic criteria (i.e., the standard method described in the DSM-5).
Procedures
Authorization to adapt the ICU and its short versions among Portuguese youth was previously obtained from the measure’s authors. Appropriate procedures (e.g., avoiding item bias or differential item functioning) were followed during the translation and retroversion (Hambleton, Merenda, & Spielberger, 2005). The initial translation of the ICU from English into Portuguese was completed by Pechorro, Ray, et al. (2016). The questionnaire was independently translated back into English by a native English speaker with considerable professional experience in translating psychology-related scientific texts. No significant differences were found between the back-translation and the original version, providing evidence indicating that the translated items had the same or very similar meanings as the original English items.
Authorization to assess youths was obtained from the General Directorate of Reintegration and Prison Services–Ministry of Justice (Direção-Geral de Reinserção e Serviços Prisionais – Ministério da Justiça). The detainees, from the eight existing Portuguese Juvenile Detention Centers that admit male youths, were informed about the nature of the study and asked to voluntarily participate. The participation rate was approximately 92%. Not all young people agreed or were able to participate; reasons for this included refusal to participate (5%), inability to participate due to not understanding the Portuguese language (2%), and inability to participate due to security issues (1%). The measures were administered by means of individual face-to-face interviews in each juvenile facility. Institutional files were also used to complement the information obtained (e.g., prior criminal activity and detentions, psychiatric diagnosis). Some information (e.g., sociodemographic variables) was obtained from self-reports. The first and second authors made the diagnosis of CD (American Psychiatric Association, 2013), after interviewing each youth and taking into consideration the institutional files (which also included the official psychiatric and psychological assessments of each youth).
Data Analytical Strategy
The data were analyzed using SPSS version 24 (IBM SPSS, 2016) and EQS 6.2 (Bentler & Wu, 2015). Factor structures were assessed with CFA performed in EQS 6.3 (Bentler & Wu, 2015) using the maximum likelihood (ML) method with robust estimation. The scaled chi-square and robust standard errors using ML estimation is the typical default method used by the EQS software as it has been shown to provide a good general approach to dealing with nonnormality (Byrne, 2006). Goodness-of-fit indices were calculated, including chi-square/degrees of freedom or Satorra–Bentler chi-square/degrees of freedom, comparative fit index (CFI), incremental fit index (IFI), and root mean square error of approximation (RMSEA). A chi-square/degrees of freedom value <5 is considered acceptable, a value ≤2 is considered good, and =1 very good (Maroco, 2014; West, Taylor, & Wu, 2012). A CFI ≥.90 and RMSEA ≤.08 indicate adequate fit, whereas a CFI ≥.95 and RMSEA ≤.06 indicate good model fit (Byrne, 2006; West et al., 2012). The IFI, also known as Bollen’s IFI, is relatively insensitive to sample size; values that exceed .90 are regarded as acceptable and above .95 are regarded as good (Maroco, 2014). In terms of the Akaike information criterion (AIC), which measures the expected discrepancy between the true model and the hypothesized model, the model with the smallest AIC should be selected (West et al., 2012). It is important to mention that the AIC cannot be used to compare models composed of different items (i.e., the 12-item measure with the 10-item measure). The CFA was performed on the original scale items. The minimum value considered for an adequate loading was a standardized loading above .30 (Nunnally & Bernstein, 1994). Polychoric correlations were used with robust methodologies to perform the CFAs on the ordinal items as they tend to provide more accurate estimates (Byrne, 2006). No modification indexes were used to improve the fit.
To test convergent and discriminant validity with other psychometric measures, Pearson correlations were used (associations between scale variables). To test criterion-related validity with other variables, Spearman and point-biserial correlations were used (associations with ordinal variables and nominal dichotomous variables; Leech, Barrett, & Morgan, 2015). Cronbach’s alpha values >.70 were considered to be good, mean interitem correlations were considered good if between .15 and .50, and corrected item-total correlations were considered adequate if above .20 (Clark & Watson, 1995; Nunnally & Bernstein, 1994).
Results
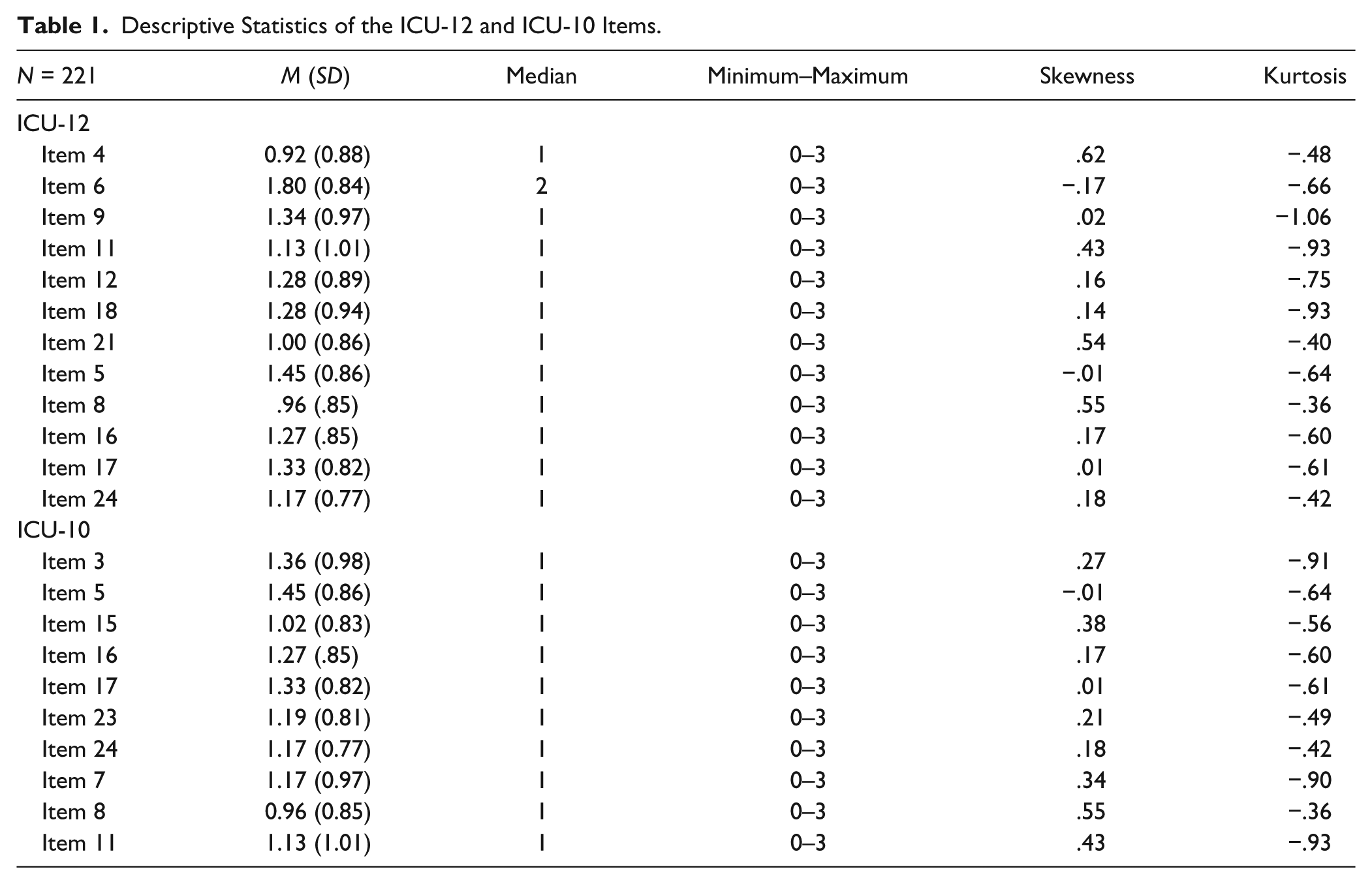
Our first step in examining the psychometric properties of the two short versions of the ICU was to examine descriptive information about the items (see Table 1).
Descriptive Statistics of the ICU-12 and ICU-10 Items.
Our next step was to use CFA to examine the fit of previously reported factor structures for these instruments, focusing primarily on the factor structures suggested by the two original development studies of the 10- and 12-item scales (Hawes, Byrd et al., 2014; Ray et al., 2016). 1 As seen in Table 2, the correlated two-factor model for both the ICU-12 and ICU-10 fit the data better than either the unidimensional model or the higher order two-factor model (i.e., first-order factors subsumed by a single higher order factor). No modifications (e.g., correlated residuals) were used to improve the fit of these models. When comparing the two-factor first-order structures of the ICU-12 and the ICU-10, results mostly indicate the ICU-12 obtained an adequate model fit (e.g., RMSEA = .08), and the ICU-10 failed to reach an adequate fit (e.g., RMSEA = .10).
Goodness-of-Fit Indices for the Different Models of the ICU-12 and ICU-10.
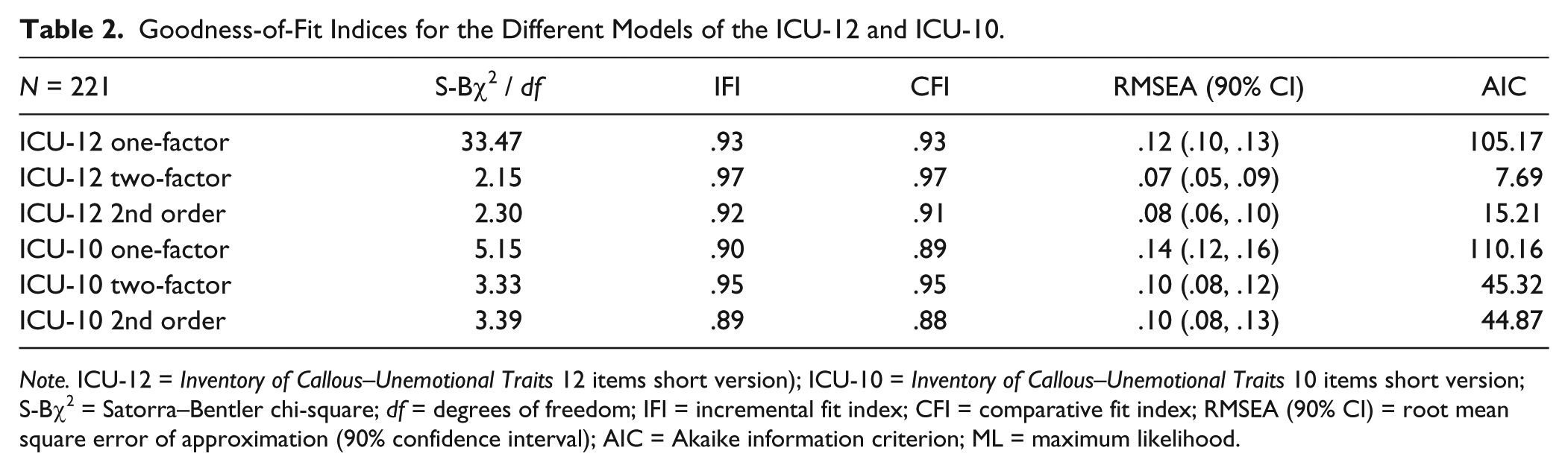
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version); ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version; S-Bχ2 = Satorra–Bentler chi-square; df = degrees of freedom; IFI = incremental fit index; CFI = comparative fit index; RMSEA (90% CI) = root mean square error of approximation (90% confidence interval); AIC = Akaike information criterion; ML = maximum likelihood.
Presented in Table 3 are the loadings of the ICU-12 and ICU-10 for the two-factor model. The CFA for the ICU-12 was based on the factor structure identified by Hawes, Byrd et al.(2014). Alternatively, the ICU-10 items and their respective specified scale loadings were based on the original bifactor structure identified by Kimonis et al. (2008). Thus, the items on each of the subscales differ across the two ICU scales. For example, Item 8 loaded on a different factor in the two scales because the rationale for the factor structure of each scale was different. Because Ray et al. (2016) did not conduct a factor analysis of the ICU-10, we decided to use findings from previous research with the original ICU to guide which factors the items would load on while Hawes, Byrd et al. (2014) provided direct guidance in this regard for the ICU-12. As seen in the table, all loadings were above the minimum recommended value (i.e., .30). It is perhaps worth noting that Item 24 (“I do things to make others feel good”) on the Uncaring subscale exhibited the highest loading on both the ICU-12 and ICU-10.
Item Loadings for the Confirmatory Two-Factor First-Order Intercorrelated Structure of the ICU-12 and ICU-10.
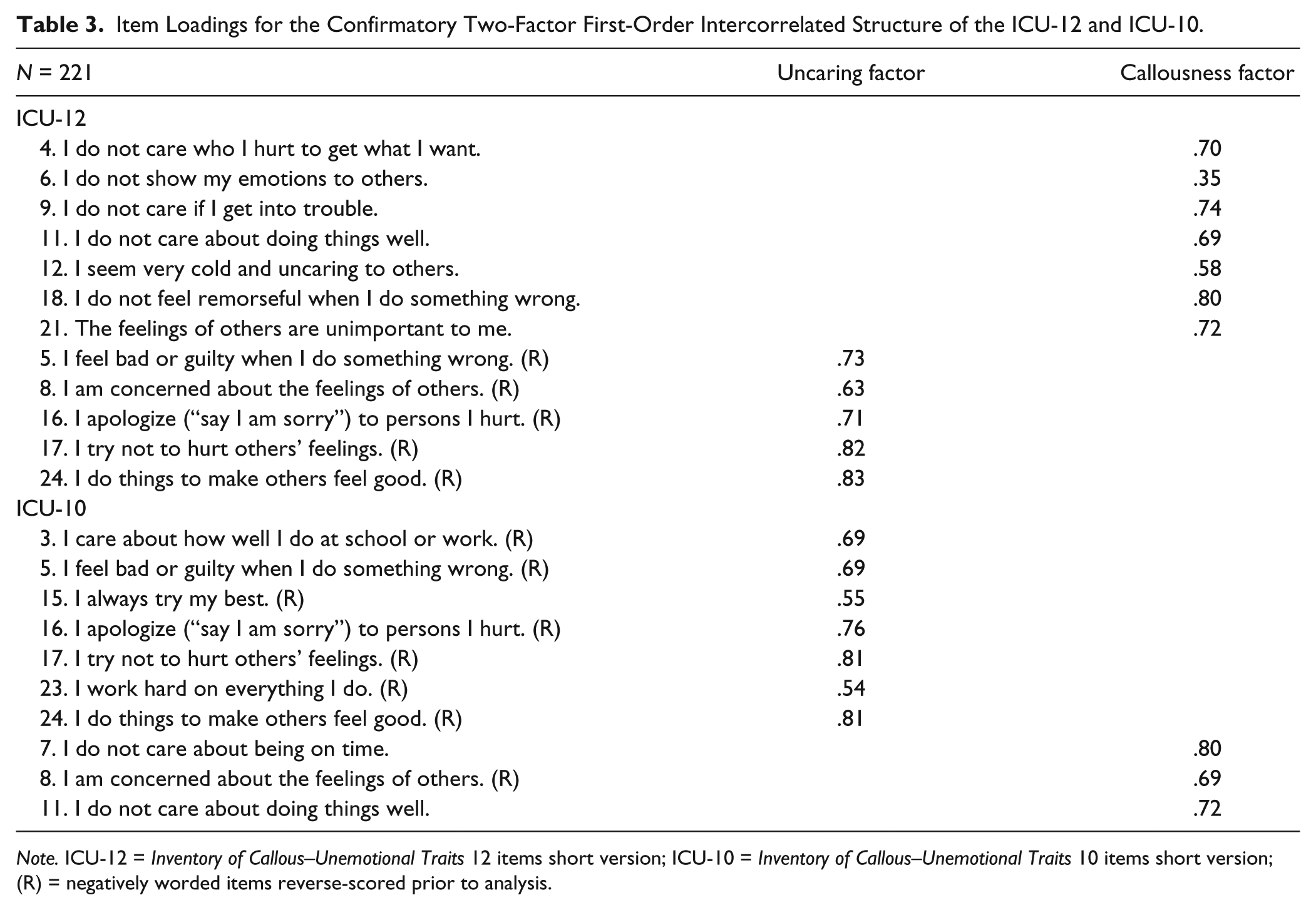
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version; ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version; (R) = negatively worded items reverse-scored prior to analysis.
Presented in Table 4 are the correlations between the ICU-12 (total and its dimensions) and the ICU-10 (total and its dimensions). These correlations ranged from moderate to high as expected, as these measures are both intended to tap into the same underlying constructs. Specifically, the analogous subscales across the two versions (e.g., ICU-10 callousness with ICU-12 callousness) showed the strongest correlations while the Callousness subscale of the ICU-10 showed the weakest correlation with the Uncaring subscales of both the ICU-12 and ICU-10.
Pearson Correlations Matrix for the ICU-12 and ICU-10.
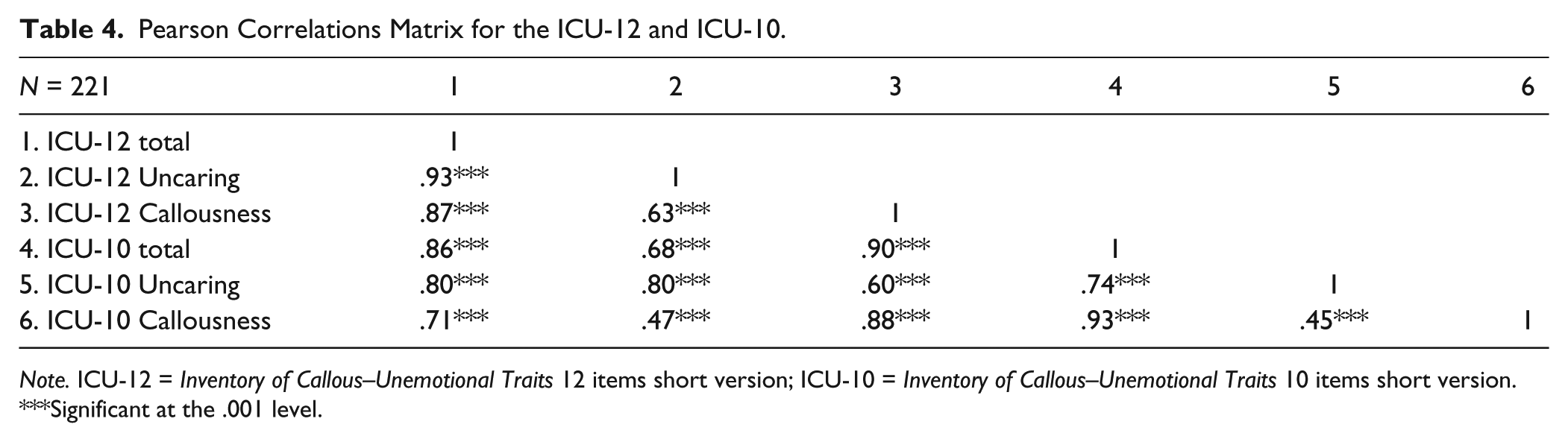
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version; ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version.
Significant at the .001 level.
Estimates of Cronbach’s alpha, mean interitem correlations, and corrected item-total correlations for the ICU-12 and the ICU-10 indicate that each of these measures exhibit good internal consistency (see Table 5). In terms of Cronbach’s alpha, the ICU-12 total obtained the highest value and the ICU-10 Callousness subscale obtained the lowest. This is not too surprising given that the ICU-10 Callousness subscale consisted of only three items.
Cronbach’s Alpha, Mean Interitem Correlation, and Corrected Item-Total Correlation Range for the ICU-12 and ICU-10.
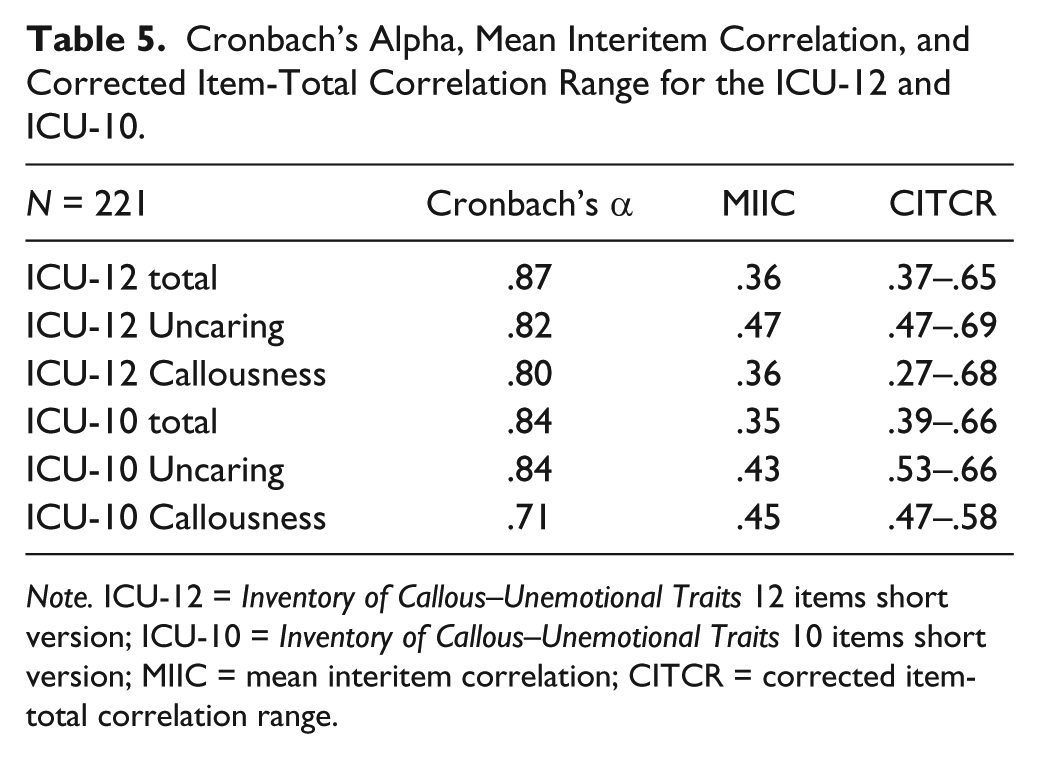
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version; ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version; MIIC = mean interitem correlation; CITCR = corrected item-total correlation range.
Convergent validity (showing that psychometric variables that are supposed to be measuring the same construct and to be related are in fact, related) and discriminant validity (showing that psychometric variables that are not supposed to be related are in fact, unrelated) of the ICU scale scores were examined by calculating bivariate correlations between the total and subscale scores of the ICU-12 and ICU-10 measures with several theoretically relevant criterion variables (see Table 6). 2 Partial correlations were also calculated to examine the unique convergent and discriminant associations with other study measures while controlling/adjusting the effect of subscale overlap separately for the ICU-12 and ICU-10. As shown in the table, the positive correlations with the full ICU, the APSD-SR CU subscale, and the YPI C-U subscale support the convergent validity of both short forms. When examining the correlations between the ICU-10 and ICU-12 with the RPQ Reactive and Proactive subscales, there is also evidence for convergent validity. In general, the correlations with the SAS-A revealed the expected negative (or nonsignificant) correlations.
Correlations and Partial Correlations of the ICU-12 and ICU-10 With Other Psychometric Measures.
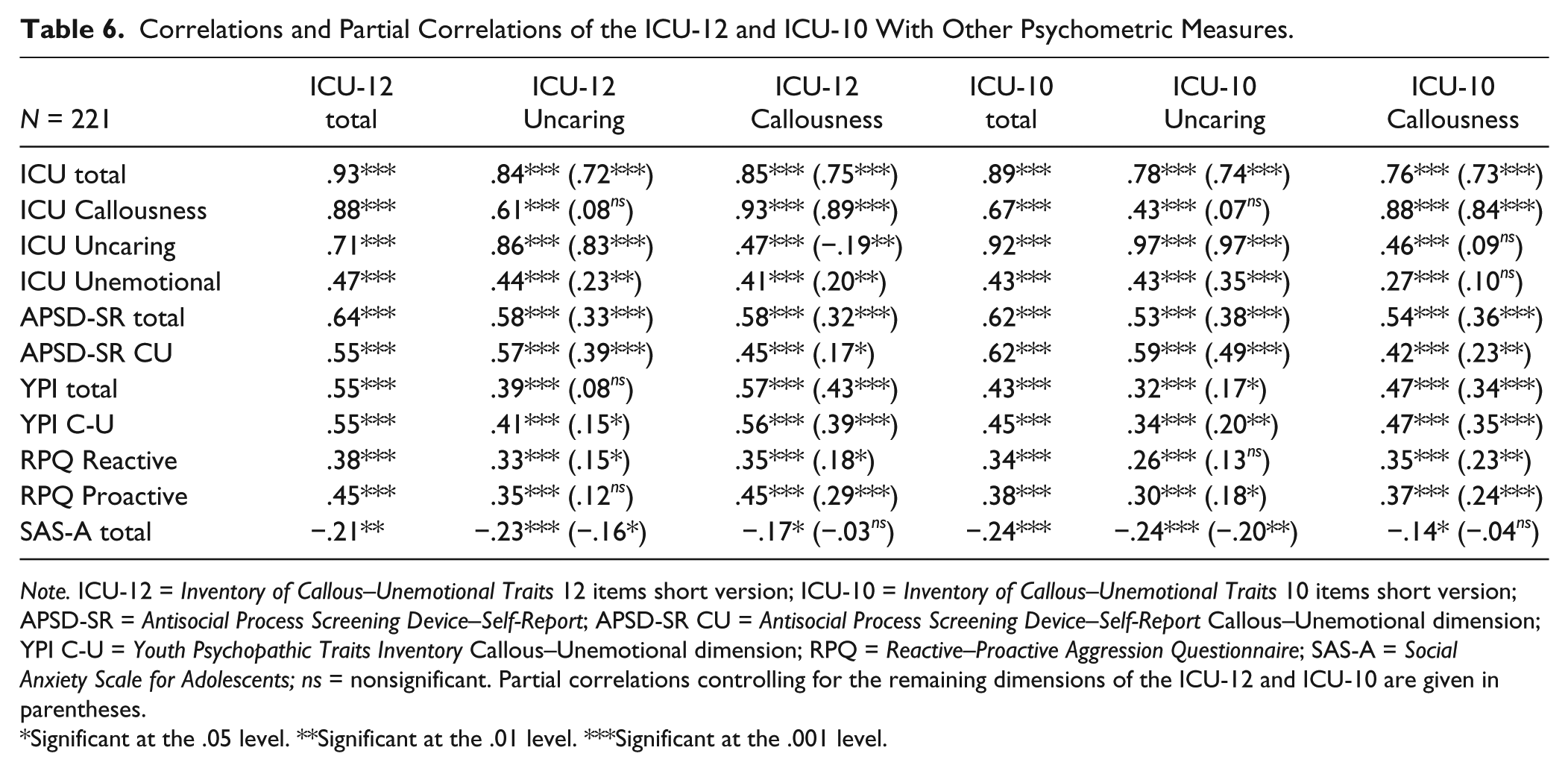
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version; ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version; APSD-SR = Antisocial Process Screening Device–Self-Report; APSD-SR CU = Antisocial Process Screening Device–Self-Report Callous–Unemotional dimension; YPI C-U = Youth Psychopathic Traits Inventory Callous–Unemotional dimension; RPQ = Reactive–Proactive Aggression Questionnaire; SAS-A = Social Anxiety Scale for Adolescents; ns = nonsignificant. Partial correlations controlling for the remaining dimensions of the ICU-12 and ICU-10 are given in parentheses.
Significant at the .05 level. **Significant at the .01 level. ***Significant at the .001 level.
Presented in Table 7 are the correlations and partial correlations with behavioral measures. Statistically significant correlations were found between the ICU-12 and ICU-10 and criterion-related variables such as age of crime onset, CD symptoms (scored as a scale), CD diagnosis, Limited Prosocial Emotions specifier, crime seriousness, alcohol use, and cannabis use. In general, both measures show similar patterns in their correlations with these criteria, mainly in the expected direction. However, the most discrepant findings emerge when comparing their associations with previous violence and number of criminal charges. Specifically, the ICU-12 shows significant positive correlations with both, whereas the ICU-10 was unrelated to these measures. In terms of the DSM-5 CD diagnostic, we found a very high prevalence rate of 94.1% in our sample which may explain the relatively low correlations due to a lack of variance.
Correlations and Partial Correlations of the ICU-12 and ICU-10 With Behavioral Measures.
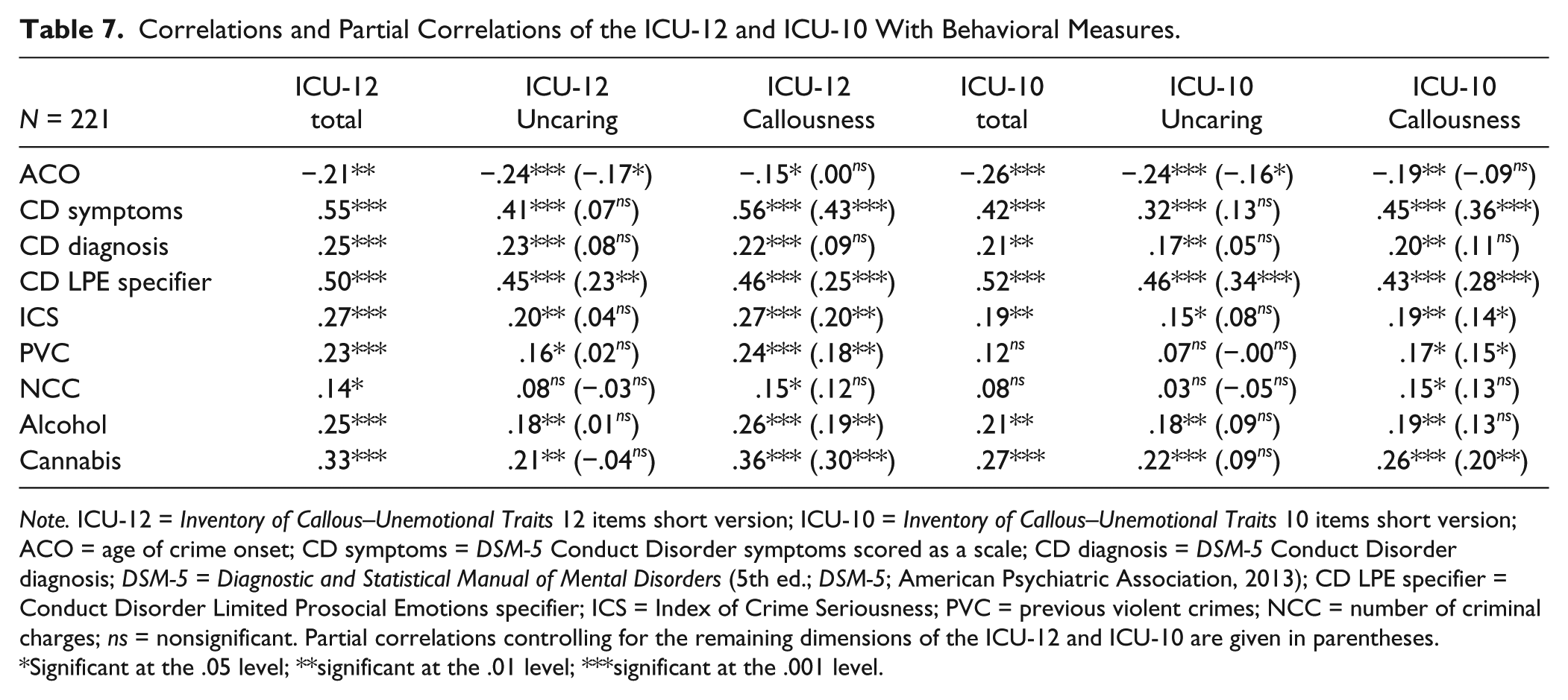
Note. ICU-12 = Inventory of Callous–Unemotional Traits 12 items short version; ICU-10 = Inventory of Callous–Unemotional Traits 10 items short version; ACO = age of crime onset; CD symptoms = DSM-5 Conduct Disorder symptoms scored as a scale; CD diagnosis = DSM-5 Conduct Disorder diagnosis; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013); CD LPE specifier = Conduct Disorder Limited Prosocial Emotions specifier; ICS = Index of Crime Seriousness; PVC = previous violent crimes; NCC = number of criminal charges; ns = nonsignificant. Partial correlations controlling for the remaining dimensions of the ICU-12 and ICU-10 are given in parentheses.
Significant at the .05 level; **significant at the .01 level; ***significant at the .001 level.
Discussion
Findings from this study represent the first investigation of two shortened versions of the self-report ICU among a sample of incarcerated male juvenile delinquents. In line with prior research (i.e., Hawes, Byrd et al., 2014; Waller et al., 2015), a correlated two-factor model was found to provide the best fit for both the 12- and 10-item versions of the measure. Results from CFA testing suggested a considerably better fit for the ICU-12 compared with the ICU-10. As expected, correlations among the ICU-12 and ICU-10 total and subscale scores were positive, and these effects were moderate to strong in magnitude. The association between the underlying factors for the ICU-10 were found to be somewhat smaller (r = .45) than that of the 12-item version of the measure (r = .63).
It should be noted, however, that this is the first study to investigate the factor structure of the ICU-10, because Ray et al. (2016) did not use CFA in their study. This may explain, in part, the poorer model fit and somewhat attenuated correlations with the subscales specified for the ICU-10 in the current study. In particular, the original approach taken in the development of the 10-item version of the ICU identified items that exhibited the highest IRT discrimination (i.e., slope) parameters based on a unidimensional model. However, the specified CFA for the 10-item version in the current study was based on item loadings as specified in the originally identified bifactor structure for the full ICU (Kimonis et al., 2008). Alternatively, the CFA for the ICU-12 in the current study was based on results of the original development study of the ICU-12 by Hawes, Byrd and colleagues (2014).
Total and subscale scores for the ICU-10 and ICU-12 displayed good internal consistency as they were mostly above .80, considerably higher than the minimum recommended value (Nunnally & Bernstein, 1994). The exception was the Callousness dimension of the ICU-10 that was only marginally above the .70 value. Regarding the mean interitem correlations, good results were also found because the ICU-12 and the ICU-10 were within the recommended value range (Clark & Watson, 1995), revealing adequate heterogeneity between the items. Regarding the corrected item-total correlation range, no problems were found as the ICU-12 and ICU-10 were able to reach the minimum recommended, revealing adequate associations between the items (Kaplan & Saccuzzo, 2013; Nunnally & Bernstein, 1994). These findings provide support for each of these brief versions of the ICU and continue to add to the growing body of literature, showing that the use of fewer, more optimally functioning items can be used to tap into underlying facets of CU traits.
The convergent validity of the ICU-12 and ICU-10 with other measures assessing CU traits and antisocial features revealed generally moderate to large positive associations. The similar positive correlations with the original ICU and the subscales of the YPI and APSD that assess CU traits support the convergent validity of both short forms. Further examination of the correlations with the subscales of the full version of the ICU suggests both convergent and discriminant validity where the respective subscales of the ICU-10 and ICU-12 are positively related to analogous scales of the ICU and show weaker correlations with the other subscales. Even more so, the conditional correlations (i.e., accounting for the other subscale) show unique associations with the analogous subscales of the original ICU and the short forms. There is also evidence for convergent validity when examining the correlations between the ICU-10 and the ICU-12 with the RPQ Reactive and Proactive subscales. That is, across the board, the correlations were positive and moderate to high in magnitude with a considerable degree of consistency across the two versions of the ICU. However, one difference in terms of convergent validity that emerged between the two scales was that the ICU-12 Uncaring subscale was no longer related to the RPQ Proactive scale once the Callousness subscale was accounted for, while the ICU-10 Uncaring subscale was no longer related to the RPQ Reactive scale once Callousness was accounted for. The ICU-12 showed a tendency to display stronger correlations with the original ICU and measures assessing features of psychopathy, and the Callousness dimension showed a stronger correlation with proactive aggression as expected (Kimonis et al., 2008).
In terms of the discriminant validity with the SAS-A, the results revealed the expected negative or nonsignificant correlations (e.g., Hofmann et al., 2009) as these are considered nonoverlapping constructs. The Uncaring dimension showed a stronger negative association with anxiety, as expected based on previous studies (Hawes, Byrd et al., 2014). This association remained even when controlling for the Callousness dimension while the association between social anxiety and Callousness was reduced to nonsignificance once the Uncaring dimension was controlled for. Thus, we must conclude both instruments provided evidence of convergent/discriminant validity in their associations with several theoretically relevant constructs ( American Educational Research Association [AERA], American Psychological Association [APA], & National Council for Measurement in Education [NCME], 2014; Kaplan & Saccuzzo, 2013).
The correlations between the ICU-12 and ICU-10 with measures of criminal behavior revealed mostly moderate-low negative associations with age of crime onset, and moderate-low positive associations with crime seriousness and the use of physical violence when committing crimes. These findings are consistent with a number of prior studies that have reported similar associations (e.g., Forth et al., 2003; Kimonis et al., 2008; Roose et al., 2010). In addition, the criterion validity of the ICU-12 and ICU-10 with DSM-5’s CD symptoms, diagnosis, and Limited Prosocial Emotions specifier (American Psychiatric Association, 2013) revealed moderate associations that were similar to those found in previous studies using the same short measures or the original ICU (e.g., Essau et al., 2006; Hawes, Byrd et al., 2014). In line with Hawes, Byrd et al. (2014), results from this study also found the Callousness dimension to overlap more substantially with CD symptoms and diagnosis than the Uncaring dimension. In terms of prevalence of CD found in the current sample (94.1%), it was considerably higher than those usually found among forensic samples (Sevecke & Kosson, 2010).
In line with previous investigations (e.g., Colins, Noom, & Vanderplasschen, 2012), ICU-12 and ICU-10 correlations with variables such as alcohol use and cannabis use revealed mostly significant and positive associations that were moderate-low in magnitude. As expected from previous investigations with the ICU, the Callousness dimension showed stronger correlations with these variables than the Uncaring dimension (e.g., Pechorro et al., 2016). Thus, the current study supports the multidimensional nature of the ICU short versions given some of the unique associations with external criteria (e.g., anxiety, age of crime onset, and proactive aggression) identified. However, more research is needed to explore the multidimensional nature of these measures, such as multidimensional item response modeling (MIRT; for a review, see Muthén & Asparouhov, 2016), to provide a better understanding of the ICU.
Findings from this study must be considered in light of several limitations. First, while the current sample is particularly relevant for the assessment of CU traits, its generalizability may be limited due to homogeneity with regard to gender, cultural background, and justice involvement. Furthermore, the cross-sectional nature of the current study did not allow for an examination of the stability of the features assessed by these measures over time. This is notable in light of concerns that have been raised regarding the downward extension of the construct of adult psychopathy to youth (see, for example, Salekin, Rosenbaum, Lee, & Lester, 2009), particularly as findings from several recent studies provide evidence of malleability among these features across development (Fontaine, Rijsdijk, McCrory, & Viding, 2010; Hawes, Byrd, Waller, Lynam, & Pardini, 2017; Hawes, Mulvey, Schubert, & Pardini, 2014).
Establishing cross-cultural validity of construct measures has become an increasingly important area of focus (Beaton, Bombardier, Guillemin, & Ferraz, 2000). Given the increase in the number of cross-national research projects, it is important to ensure that the validity of measures initially designed based on a particular cultural and source language translates to other populations. It is our hope that the development of brief, yet valid self-report measures of CU traits will enable researchers to embed such measures in large-scale longitudinal studies to increase our understanding of these features and improve our ability to accurately assess this construct. This is particularly important considering the implementation of this construct as a specifier in the DSM-5 (American Psychiatric Association, 2013; “With Limited Prosocial Emotions”) and its current consideration for inclusion in the upcoming revision of the International Classification of Diseases by the World Health Organization (Rutter, 2012). It is important to keep in mind, however, that the original ICU along with these recently developed short versions were designed for research purposes as dimensional measures of CU traits. Only recently have researchers begun to determine cutoff scores for use with the full version of the ICU (Docherty, Boxer, Huesmann, O’Brien, & Bushman, 2016). Thus, we recommend that until more research is conducted that establishes widely accepted cutoff scores, that scores from the ICU and its variants be calculated to capture CU traits as a dimensional construct.
The current study provides support for use of the ICU-12 and ICU-10 with detained juvenile delinquents, along with its use across different samples, cultures, and ethnic groups. Overall, findings suggest that of these two brief versions of the ICU, the ICU-12 may provide a better overall assessment of the CU construct. However, this was most evident with regard to the construct validity of the two measures, as they performed equally well in assessing facets of criterion-related validity. Importantly, further psychometric investigations are needed (e.g., cross-validation, test–retest reliability) using both approaches to arrive at a more concrete conclusion. Nonetheless, the present study provides support for prior research suggesting that it may be possible to assess CU traits using fewer items, while improving upon the psychometric properties found on the original version of the ICU measure.
Footnotes
Acknowledgements
The authors thank the following Portuguese juvenile detention centers for their collaboration: Bela Vista, Mondego, Navarro de Paiva, Olivais, Padre António Oliveira, Santo António, Santa Clara, Prisão-Escola de Leiria.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Portuguese Foundation for Science and Technology (FCT; Grant SFRH/BPD/86666/2012) with co-financing of the European Social Fund (POPH/FSE), the Portuguese Ministry of Education and Science (MEC), and FEDER (PT2020 Partnership Agreement; UID/PSI/01662/2013).