
Abstract
Therapeutic alliance is associated with treatment outcomes across a diverse range of intervention models and clinical populations. Likewise, the perceived quality of working alliance in adult psychotherapy has been a consistent predictor of engagement, while research with children is limited. This study draws from a sample of 180 children who were involved in a study of the Coping Power preventive intervention for elementary students with aggressive behavior. Approximately 1,080 individual intervention sessions were coded using the Therapeutic Process Observational Coding System (TPOCS-A). Results suggest that bonding, in the early sessions of Coping Power, predicted a reduction in teacher-reported externalizing behaviors. In addition, data analyses revealed that bonding interacted with children’s gender in the latter portions of Coping Power. Higher bonding for girls in later sessions predicted lower teacher-rated externalizing behaviors at 1-year follow-up. Finally, initial levels of aggression moderated the relationship between bond and parent-rated externalizing behaviors during the early and late sessions of Coping Power, with stronger effects for moderately aggressive children. Task orientation, a component of therapeutic alliance, in late sessions had counter-intuitive effect on parent-rated externalizing behaviors, possibly due to therapists’ efforts to impose more structure with children who were not progressing well.
Keywords
Therapeutic alliance is considered a robust predictor of therapeutic outcomes throughout the adult psychotherapy literature (Horvath et al., 2011). Bordin (1979) conceptualized the therapeutic alliance as the agreement between the therapist and client on the tasks and goals of therapy, as well as the quality of the relational bond between the therapist and client. The task refers to the specific activities in which the client engages, goals are the objectives toward which the treatment is aimed, and the bond represents the quality of the relationship between the therapist and client (Safran & Muran, 2000). A positive working relationship has been found to be a critical part of the therapeutic process across interpersonal, psychodynamic, and cognitive therapy models (Accurso et al., 2013) and has been associated with client motivation, session attendance, and engagement in therapeutic tasks (Kazdin et al., 1990) as well as behavioral outcomes in psychotherapy with children and adolescents (Shirk et al., 2011). Conceptually, attention to both the bond and the task can be particularly salient when working with youth and their parents (B. D. McLeod & Weisz, 2005). Despite the theoretical and clinical importance of therapeutic alliance, limited empirical studies have evaluated the influence of therapeutic alliance in child and adolescent psychotherapy (Accurso et al., 2013; Chiu et al., 2009; Shirk & Karver, 2003).
Measurement of Therapeutic Alliance
Many measures exist to assess the therapeutic alliance in youth and adolescent samples (Bickman et al., 2010; Shirk & Karver, 2003). Therapeutic alliance has generally been measured through a single report source, such as child self-report, observer-, therapist-, or parent-report, and occasionally measured using multiple report sources such as parent- and therapist-report (J. McLeod, 2011). Report source is important to consider as youth differ from adults developmentally and may lack the cognitive abilities to evaluate their behavior, emotions, or relationships (Shirk & Saiz, 1992). Beyond this, while each type of report source offers useful insight to the alliance, child-, parent-, and therapist-reported alliance are subjective to the individual’s experience, whereas observer-reported alliance is an objective measure of the construct (B. D. McLeod et al., 2016). It is likely that the lack of uniformity in alliance measures, as well as variance in report source, may contribute to the mixed findings surrounding the influence of the therapeutic alliance in youth psychotherapy (Shirk & Karver, 2003).
Externalizing Behaviors and Therapeutic Alliance
Therapeutic alliance has been studied in relation to a variety of youth mental health difficulties including Attention-Deficit/Hyperactivity Disorder, eating disorders, internalizing symptoms, externalizing behaviors, posttraumatic stress symptoms, and substance use (Lerner et al., 2011; J. McLeod, 2011; Ormhaug et al., 2014; Zorzella et al., 2015). Despite the growing literature related to therapeutic alliance in youth psychotherapy, it remains unclear how the therapeutic alliance predicts changes in youth adjustment over time, specifically within interventions that target externalizing behaviors. Previous investigations found a negative association between therapeutic alliance and externalizing behaviors (Mattos et al., 2017). In a meta-analysis of the therapeutic alliance in youth psychotherapy, Shirk and Karver (2003) found a stronger association between therapeutic alliance and externalizing behaviors than for other patient types, such that it was more challenging yet more critical to establish a positive therapeutic alliance with youth who exhibit aggressive or defiant behaviors compared with youth without these behaviors.
It is worth noting that in this review of 23 studies, only five studies assessed externalizing behaviors specifically and only two studies utilized observer-rated methods to measure therapeutic alliance (Shirk & Karver, 2003). Only one study (Braswell et al., 1985) has examined therapeutic alliance through observer-report within a sample of children with externalizing behaviors. In that investigation, Braswell and colleagues (1985) measured alliance by coding frequencies of on-task and off-task (e.g., interrupting clinician, non-task-related conversation) behaviors from audio recordings of sessions throughout a 7-week intervention for children with attentional and self-control difficulties. They found that child and therapist behaviors which suggest positive, active involvement in therapy tasks is related to improved classroom behavior postintervention and at 10-week follow-up per the teacher report. Of note, this study focused solely on behaviors related to the “task” orientation of the therapeutic alliance in a sample of children with difficulties with attention and self-control.
There is some evidence to suggest there is a nuanced relationship between therapeutic alliance and adjustment over time (Langer et al., 2011). Chu and Kendall (2004) found that engagement in the middle of the intervention was a salient indicator of positive treatment outcomes in a sample of children with anxiety. Few studies have examined this dynamic relationship when working with aggressive youth (Hurley et al., 2015; Lindsey et al., 2019). Ellis and colleagues (2013) highlighted how engagement early in the cognitive-behavioral Coping Power group-based intervention can have a positive influence on engagement throughout the intervention in a sample of children with disruptive behaviors. Recently, Lindsey et al. (2019) found that engagement during the middle phase of the group-based intervention was particularly important for decreased externalizing behaviors in a sample of children with disruptive behaviors at postintervention follow-up. As such, the present study expands upon existing research by examining the unique influence of observer-reported therapeutic alliance throughout the course of an intervention delivered individually on adjustment in a sample of children exhibiting externalizing behaviors.
The Present Study
The present study explored the two dimensions of alliance, bond and task, predicting adjustment over time in a sample of aggressive youth. This study uniquely contributes to the existing literature by investigating the relationship between the quality of therapeutic alliance, measured throughout a 34-session intervention, and long-term functioning in aggressive youth 1-year postintervention. Based on literature which highlights the potential subjectivity and variability between report sources (B. D. McLeod et al., 2016; B. D. McLeod & Weisz, 2005), this study utilized observer-rated methods to objectively examine the alliance in a manualized, school-based, individual cognitive-behavioral intervention. Some argue that the structure of manualized treatments undermines the development of the alliance; however, studies have shown there is no significant difference in the alliance ratings for manualized versus nonmanualized interventions in youth therapy (B. D. McLeod et al., 2016; Shirk & Karver, 2003). In fact, a randomized control trial found that participation in a manualized-guided intervention was associated with stronger therapeutic alliance early in intervention compared with those in the nonmanualized condition, and that alliance between the two conditions converged over time (Langer et al., 2011). The present study expands upon this by coding both the bond and task orientations of the therapeutic alliance from video-recording sessions in an intervention for children who exhibit aggressive and disruptive behaviors. As noted previously, there are many methodologies used to measure therapeutic alliance, and the potential bias associated with any report source is important to consider. Due to the overall aim of understanding the influence of therapeutic alliance on intervention outcomes, generating a standardized, objective assessment of the therapeutic alliance was prioritized; thus, an observer-rated measure of therapeutic alliance was chosen. Furthermore, this study contributes to the existing literature by using an observer-rater methodology with a sample of children exhibiting aggressive and disruptive behaviors.
It was hypothesized that a stronger therapeutic alliance would positively influence the long-term functioning of the youth. Specifically, we hypothesized high ratings of both the bond and task orientation of the therapeutic alliance would predict decreased levels of externalizing behaviors over time. Exploratory analyses were conducted to understand the influence of sex, as well as baseline levels of aggression at the time of screening, on the strength of the alliance over time.
Method
Participants
Participants were drawn from a pool of 180 children across 10 elementary schools who received the Coping Power intervention individually as part of a study comparing individual versus group formats of delivery for cognitive-behavioral interventions (Lochman et al., 2015). The sample for analyses for the current study only included children with full therapeutic alliance coding data available (n = 122). The fourth-grade teachers at each school rated the behaviors of all their students using the Teacher Report Form (Achenbach, 1991). The students whose scores that fell at or above the top 25% among their peers for aggressive behavior were invited to participate in the intervention. Each annual cohort consisted of six students per school. The sample was 47% female, and over half of the sample was 10 years old (range = 9.0–11.0 years). Sample participants primarily identified as African American (68.9%). The family income of the participants was reported in the following brackets: none (4.10 %), less than $15,000 (25.41%), $15,000 to $29,999 (30.34%), $30,000 to $49,999 (25.42%), and greater than $50,000 (14.76%). At the time of the intervention implementation, the students and parents received monetary reimbursements (Lochman et al., 2015).
Differences Between Attrited and Nonattrited Participants
Analyses of attrition bias suggest no significant differences in level of aggression nor children’s characteristics (e.g., gender, age, race) between the attrited and nonattrited participants. Because of the screening procedure for children with moderate to high aggression, the sample had elevated externalizing behaviors. As expected, 70.1% of the sample had at-risk teacher ratings for the BASC Externalizing Composite (T score ≥ 60), and 36.2% of the sample had teacher-rated BASC Externalizing Composite scores that exceeded the clinical cutoff (T score ≥ 70). With regard to the parent-rated BASC Externalizing Composite, 48.3% of the sample had at-risk scores and 26.9% of the sample had scores that exceeded the clinical cutoff. Across three cohorts, 30 students from the larger sample moved to a different school during the intervention period. The mean number of Coping Power sessions attended for the individual students who moved was 21.73 (range = 3–33).
Procedure
Preintervention (Time 1) measures were completed by parents of target children at the time of enrollment during the spring semester of the students’ fourth grade year. The Coping Power Program was delivered during the end of fourth grade and continued throughout the fifth grade. Mid-intervention assessments (Time 2) occurred in the summer after fourth grade, postintervention assessments (Time 3) occurred in the summer after fifth grade, and 1-year follow-up assessments (Time 4) were conducted during the summer after students completed the sixth grade. Similarly, baseline data (Time 1) were gathered from teachers of target children during the spring of the fourth grade, postintervention assessments (Time 3) were collected in the late spring of fifth grade, and 1-year follow-up data (Time 4) were collected in the spring of sixth grade. All study procedures were approved by the University of Alabama Institutional Review Board.
The current study gathered Therapy Process Observational Coding System for Child Psychotherapy Alliance Scale (TPOCS-A) ratings of approximately 1,080 prerecorded individual intervention sessions for children in a school-based cognitive-behavioral program. The TPOCS-A measure creates a qualitative rating of the relationship between the clinician and child in each intervention sessions. Each student participated in 34 intervention sessions throughout the Coping Power Program. Sessions 1 to 11 were considered the early sessions of the intervention, Sessions 12 to 23 the middle sessions, and 24 to 34 the late sessions of the intervention. Three sessions from each of the early (Sessions 1, 4, 8), middle (Sessions 12, 16, 20), and late (Sessions 24, 28, 32) intervention stages were systematically selected to be coded as a “case.” Of all participants enrolled in the Coping Power intervention trial, only participants who had video-recording of all nine specific sessions (n = 122) were included in the coding.
Coders (four undergraduate students, one postdoctoral fellow) trained over a 2-month period to establish adequate interrater reliability. The undergraduate students (three females, one male) produced individual scores of coded videos, and the scores were used to calculate percent agreement between the raters’ scores and the lead researcher. The percent agreement between the items of the TPOCS-A measure was calculated to assess the alliance. This was calculated using the exact scores of the 6-point scale, as well as on a one-off (3-point) scale. In addition, intraclass correlation coefficients (ICCs) were utilized to measure the reliability between the individual coders. Once all raters reached 80% agreement or higher on each alliance item, each rater received seven schools across three cohorts to code. Based on the 95% confidence level interval of the ICC estimate, ICC for Coder Level 2-cross session variance was 0.05 and Level 3-Cross Coder Variance was 0.06. The ICC data for interrater reliability was between excellent and fair being 1.00, 0.99, 0.86, and 0.71 for all four raters.
Coping Power Intervention
The Coping Power Program is a manualized cognitive-behavioral preventive intervention for youth at risk for behavior problems (Lochman et al., 2008). The present study only includes the sessions of child intervention, not the parent component (Lochman et al., 2008). The child component addresses social–cognitive deficits in aggressive children identified in prior studies. Main foci of the program include (a) intervention rules, weekly behavioral goals, and contingent reinforcement; (b) organizational and study skills; (c) emotional awareness and anger management skills; (d) perspective taking and attributions of others’ intentions; (e) social problem-solving skills; and (f) coping with peer pressure. The children in this sample were randomly assigned to the individual format condition and received nearly the full dose of Coping Power, with the average attendance rate being 87%.
Participants in the present study sample met with a Coping Power interventionist individually on a weekly basis. Coping Power was implemented by 19 interventionists who primarily identified as White (78%), female (84%), graduate students (84%). The interventionists were randomly assigned to a school based on availability. One interventionist, therefore, worked with a cohort of six children at their assigned school for 1 year. Five interventionists worked with two cohorts across 2 years, and five interventionists worked with three cohorts across 3 years. Interventionists were assigned to the same school if they delivered the intervention during multiple years. The participants received instruction on behavioral and personal goal setting, awareness of feelings and associated physical arousal, use of coping self-statements, distraction techniques and relaxation methods when provoked and made angry, organizational and study skills, perspective taking and attribution retraining, social problem-solving skills, and dealing with peer pressure and neighborhood-based problems by using refusal skills (Lochman et al., 2008). During each intervention session, personal and behavior goals were identified to implement in the week between sessions. Students were encouraged to provide documentation (i.e., teacher or parent signature on goal sheet) of working toward their goal at the next session to earn points and eventually apply their points toward selecting a small prize.
Intervention Fidelity and Quality
To ensure high fidelity of implementation, two doctoral-level psychologists with substantial experience implementing Coping Power met with the interventionists weekly to monitor and provide feedback on program implementation. The interventionists also received monthly supervisory feedback on video-recorded sessions to ensure that program implementation remained consistent. Program leaders rated that they completely or partially completed 91.07% and 86.43% of intervention session objectives, respectively (Lochman et al., 2015), based on the Coping Power Facilitator Guide (Lochman et al., 2008). The Coping Power Fidelity Checklist consists of seven items describing the behavioral goal of each section (i.e., establishing the structure of the program, goal setting, positive feedback, review of main points from previous section, self-instruction and real-life application, prize box, and free time). Each item was scored on a 3-point scale ranging from 0 (not at all) to 2 (completely).
Measures
Three types of measures were employed in this study. The quality of therapeutic engagement was assessed by utilizing an observational coding system; measures of long-term functioning were assessed by examining child externalizing behavior problems and sociodemographic characteristics that might moderate intervention effects.
Therapeutic Alliance (TPOCS-A)
The TPOCS-A (B. D. McLeod & Weisz, 2005) consists of nine items describing the bond and task dimensions of the therapeutic alliance in child therapy. This measure is unique in that it was specifically developed for children, as well as based on observer coding of therapy sessions (B. D. McLeod & Weisz, 2005). The TPOCS-A has demonstrated good internal consistency (α = .95) and convergent validity (.53) with the Therapeutic Alliance Scale for Children (TASC, Fjermestad et al., 2012; B. D. McLeod & Weisz, 2005; Shirk & Saiz, 1992).
The first six questions of the measure assess the “bond” between the child and therapist (e.g., “Experience the therapist as understanding and/or supporting”). The last three questions assess the mutuality of completing the “tasks” of therapy (e.g., “Use therapeutic tasks to make changes outside of the session”). The TPOCS-A Scoring Manual provides procedural guidelines and scoring strategies based on the frequency and intensity of client and therapist behaviors. Strong engagement was characterized by positive affect (e.g., liking, understanding, and caring) and mutual trust. In addition, the coding team identified several supplemental engagement practices and provided operational definitions and examples for each during the coding training process. For example, a child smiling, making eye contact, sharing jokes with an interventionist may suggest they feel connected, or have a strong “bond,” with the therapist. Furthermore, if the child excitedly shows the interventionist that they obtained five signatures on their goal sheet in the last week, this may suggest they feel connected to the goals, or “tasks,” of the treatment.
One investigation examined this measure with a sample (n = 52) of youth with internalizing disorders and suggested the structure of the therapeutic alliance in youth psychotherapy could be described with a one-factor model (Fjermestad et al., 2012). However, theoretical literature suggests that specific attention to both the bond and the task are particularly salient when working with youth and their parents (B. D. McLeod & Weisz, 2005), and empirically, research is needed to further examine this construct within a sample with externalizing behaviors. Therefore, the present study included both the bond- and task-subscales as individual constructs within the analyses. Both subscales are scored on a 6-point scale ranging from 0 (not at all) to 5 (great deal).
Behavior Assessment System for Children (BASC)
The Behavior Assessment System for Children (BASC; Reynolds & Kamphaus, 1992) is a behavior problem checklist completed by children’s teachers and by parents throughout the intervention. The measure has demonstrated strong reliability (α = .80–.89) and construct validity (Doyle et al., 1997; Reynolds & Kamphaus, 1992). The BASC items are rated from 1 (never) to 4 (almost always). The Externalizing Composite (Parent) and Externalizing Composite (Teacher) were derived from the BASC Aggression, Conduct Problems, and Hyperactivity subscales for both parent (possible raw score range: 0–99) and teacher (possible raw score range: 0–111) reports.
Teacher Report Form of Reactive and Proactive Aggression (TRF)
The TRF was completed by each of the fourth-grade teachers as an initial screening measure to identify at-risk aggressive students (Dodge et al., 1997). The six items on this measure evaluate total aggression as well as reactive and proactive aggression. Teachers used a 5-point Likert-type scale from 1 (never) to 5 (almost always), indicating how frequently each item applied to their student. Three items represent reactive aggression (e.g., “overreacts angrily to accidents”), and three items represent proactive aggression (e.g., “threatens or bullies others”). Vitaro et al. (2002) reported high internal consistency for these constructs (α = .83 for reactive aggression, α = 82 for proactive aggression).
Sociodemographic characteristics
Demographic variables were collected via child self-report (e.g., child sex, age, and race/ethnicity).
Analytic Strategy
The variance inflation factor was conducted to assess for multicollinearity of TPOCS-A. The variance inflation factor for early bond and early task was 1.75 and 1.05; therefore, we did not find an issue with multicollinearity (Craney & Surles, 2002).
A three-level growth curve model assessing children’s behavior outcome changes over time includes (a) times of measurement (b) nested within children and (c) nested within the intervention units (six children per cohort per school). Child gender, race, and screening severity as well as interventionist gender and race were covariates and treated as potential moderators. Interventionist gender and race did not emerge as significant predictors and were subsequently removed from the final models. Separate regression analyses were conducted to examine the potential impact of child gender and screening severity on therapeutic alliance. For these analyses, gender was dummy coded as 1 = male and 0 = female. Initial severity of aggression (TRF data, denoted as “Screener” in table and figures) was a measure of total aggression averaged across six items describing reactive and proactive aggression.
HLM 6.02 software was used to perform the data analyses with full maximum likelihood (FML) estimation method (Bryk & Raudenbush, 2002). The unconditional curvilinear growth models were tested by adding a time’s quadratic term to the Level 1 model, and the Deviance Tests indicated that the six outcomes changed over time with a significant curvature pattern, thus requiring a three-level curvilinear growth model. For teacher outcomes, time was coded as 0 as baseline, 1 as postintervention, and 2 as 1-year-follow-up, while for parent outcomes (where data collection took several months for each wave), we used the actual time interval from baseline as the time variable, with baseline set to zero. Curvilinear growth models were tested; however, the change in outcome over time did not show a significant curvilinear pattern and model fit worsened, and so three-level conditional linear growth model was used. Regions of significance were also used to evaluate interactions within the HLM analyses (Preacher et al., 2003).
Results
Preliminary Correlations and Variable Means
Correlations were used to evaluate the relationship between the observable therapeutic alliance in the early, middle, and late stages of the intervention (see Table 1). Bonding early in the intervention was positively, significantly correlated with middle and late bond, as well as early, middle, and late task orientation. Bonding in the middle intervention sessions was also positively, significantly correlated with late bond, middle task orientation, and late task orientation. Finally, bonding in late intervention sessions was positively, significantly correlated with late task orientation. Agreement on tasks early in the intervention was positively, significantly correlated with middle and late task orientation, as well as middle and late bond. In the middle intervention sessions, task orientation was positively, significantly correlated with late bond and late task orientation.
Correlations Between TPOCS-A Orientations.
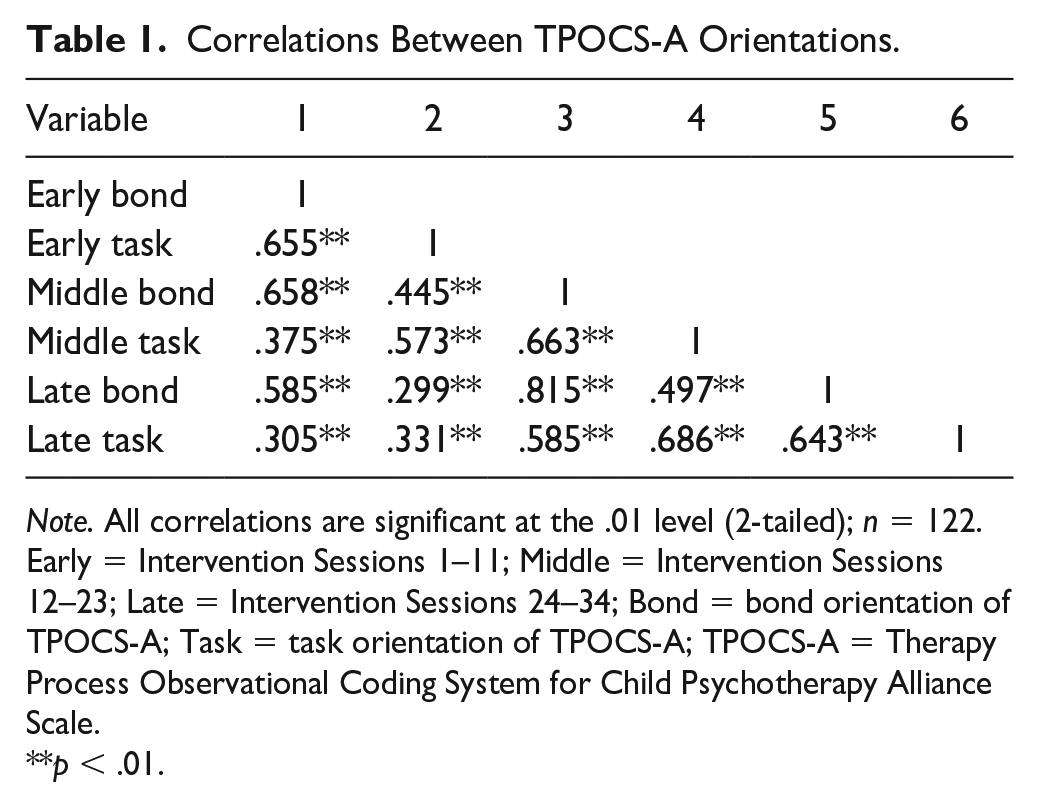
Note. All correlations are significant at the .01 level (2-tailed); n = 122. Early = Intervention Sessions 1–11; Middle = Intervention Sessions 12–23; Late = Intervention Sessions 24–34; Bond = bond orientation of TPOCS-A; Task = task orientation of TPOCS-A; TPOCS-A = Therapy Process Observational Coding System for Child Psychotherapy Alliance Scale.
p < .01.
Table 2 provides the means and standard deviations for the bond and task orientation components of the TPOCS-A measure across three time points. To address missing data, the three-level HLM analyses used FML to estimate model parameters. Mean levels of observed bond increased across early (M = 3.91, SD = .60), middle (M = 4.14, SD = .51), and late (M = 4.17, SD = .47) intervention sessions. Similarly, mean levels of observed task orientation increased across early (M = 3.18, SD = .66), middle (M = 3.55, SD = .70), and late (M = 3.61, SD = .68) intervention sessions. Table 3 provides the means and standard deviations for the externalizing composite of the BASC measure as rated by the teachers and parents at the three intervention time points and 1-year follow-up.
Means and Standard Deviations for TPOCS-A.
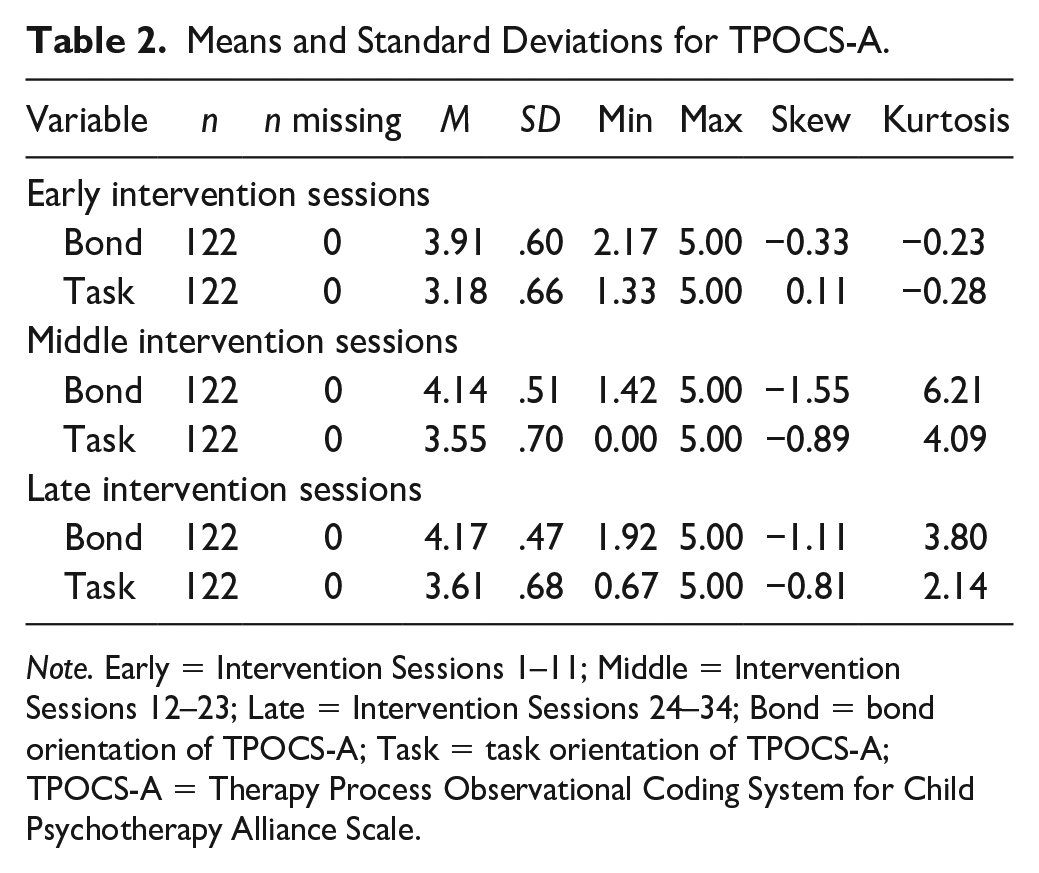
Note. Early = Intervention Sessions 1–11; Middle = Intervention Sessions 12–23; Late = Intervention Sessions 24–34; Bond = bond orientation of TPOCS-A; Task = task orientation of TPOCS-A; TPOCS-A = Therapy Process Observational Coding System for Child Psychotherapy Alliance Scale.
Means and Standard Deviations of BASC Externalizing Composite.
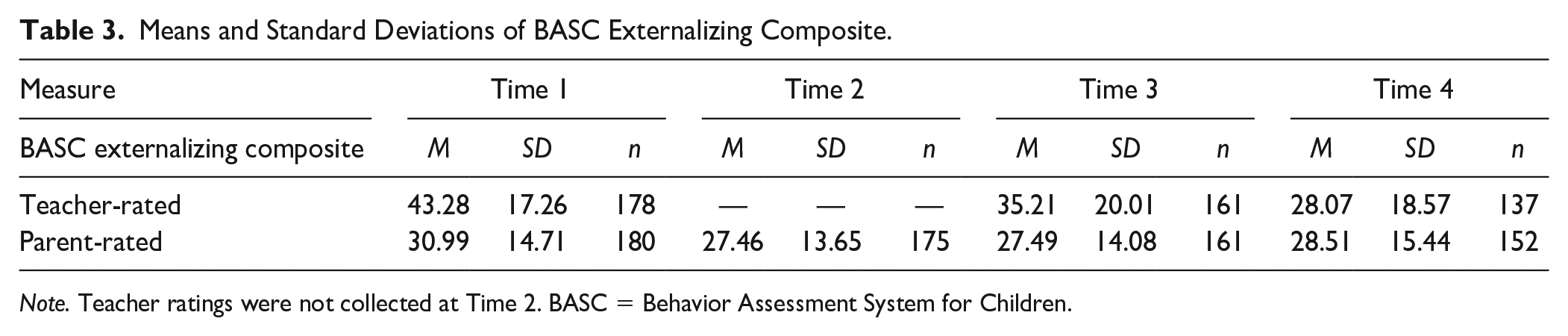
Note. Teacher ratings were not collected at Time 2. BASC = Behavior Assessment System for Children.
Growth Models for Teacher-Rated Externalizing Behavior
Three models were generated to examine the task orientation and bond orientation in the early, middle, and late part of the sessions predicting teacher-rated externalizing behaviors at 1-year follow-up (see Table 4). The first model measured the early therapeutic alliance predicting teacher-reported externalizing behavior. The HLM analyses revealed a main effect of early bonding predicted a declining slope of teacher-reported externalizing behaviors through a 1-year follow-up, t-ratio = −2.45, F(1, 64) = −8.02, p = .17. The results also indicated a main effect of gender, F(1, 64) = 6.98, p = .02, and of initial levels of externalizing symptomology at time of screener, F(1, 64) = 0.94, p = .00. There was not a significant main effect of task orientation, nor significant interactions between the therapeutic alliance orientations and gender or initial level of externalizing behavior (i.e., aggression) at the time of the screener.
TPOCS-A Predicting Externalizing Behaviors Over Time.
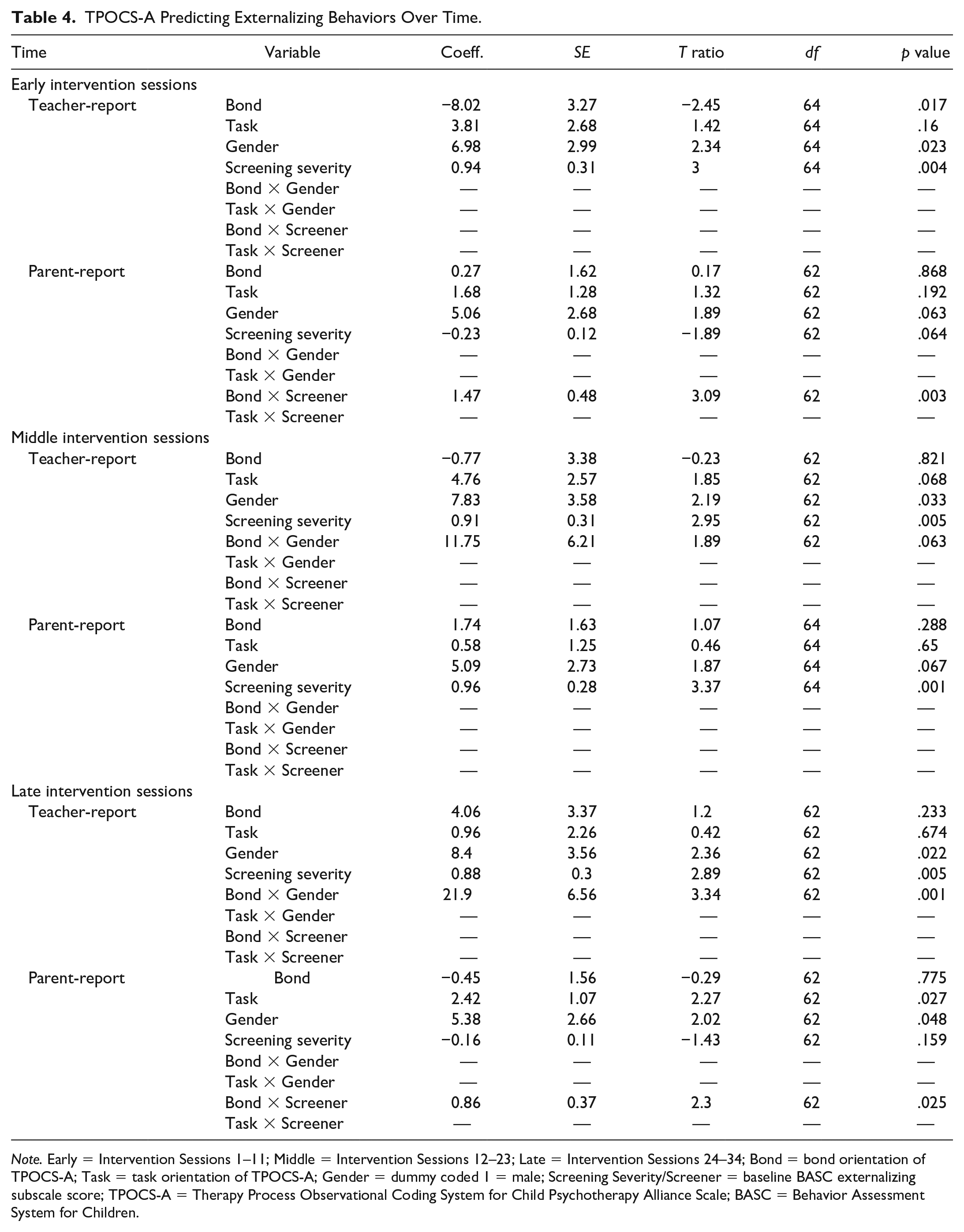
Note. Early = Intervention Sessions 1–11; Middle = Intervention Sessions 12–23; Late = Intervention Sessions 24–34; Bond = bond orientation of TPOCS-A; Task = task orientation of TPOCS-A; Gender = dummy coded 1 = male; Screening Severity/Screener = baseline BASC externalizing subscale score; TPOCS-A = Therapy Process Observational Coding System for Child Psychotherapy Alliance Scale; BASC = Behavior Assessment System for Children.
The second model did not find significant main or interaction effects for therapeutic alliance during the middle sessions of the intervention. The HLM analyses revealed neither bond, F(1, 62) = −0.77, p = .82, nor task orientation, F(1, 62) = 4.76, p = .7, were significant predictors of teacher-rated externalizing behaviors at 1-year follow-up. The results indicated a significant effect of gender, F(1, 62) = 7.83, p = .03. In addition, there was a significant effect of initial levels of aggression, F(1, 62) = 0.91, p = .01.
The third model analyzed therapeutic alliance in the late intervention sessions predicting teacher-rated externalizing behaviors. Again, no significant effects were found for bond, F(1, 2) = 4.06, p = .23, or task orientation, F(1, 62) = 0.96, p = .67. Gender and initial aggression level were significant predictors of teacher-rated externalizing behaviors at 1-year follow-up, F(1, 62) = 8.40, p = .02, and F(1, 62) = .88, p = .01, respectively. The results indicated one significant interaction between bond and gender, F(1, 62) = 21.9, p < .00. Late bond (defined as the last 11 sessions of the Coping Power Program) predicted lower teacher-rated externalizing behaviors in girls but not among boys (see Figure 1A and 1B). Specifically, for girls, late bonding predicted lower teacher-rated externalizing behaviors at 1-year follow-up. In contrast, the greater decline in the teacher-rated externalizing behaviors occurred for low bonding in boys.
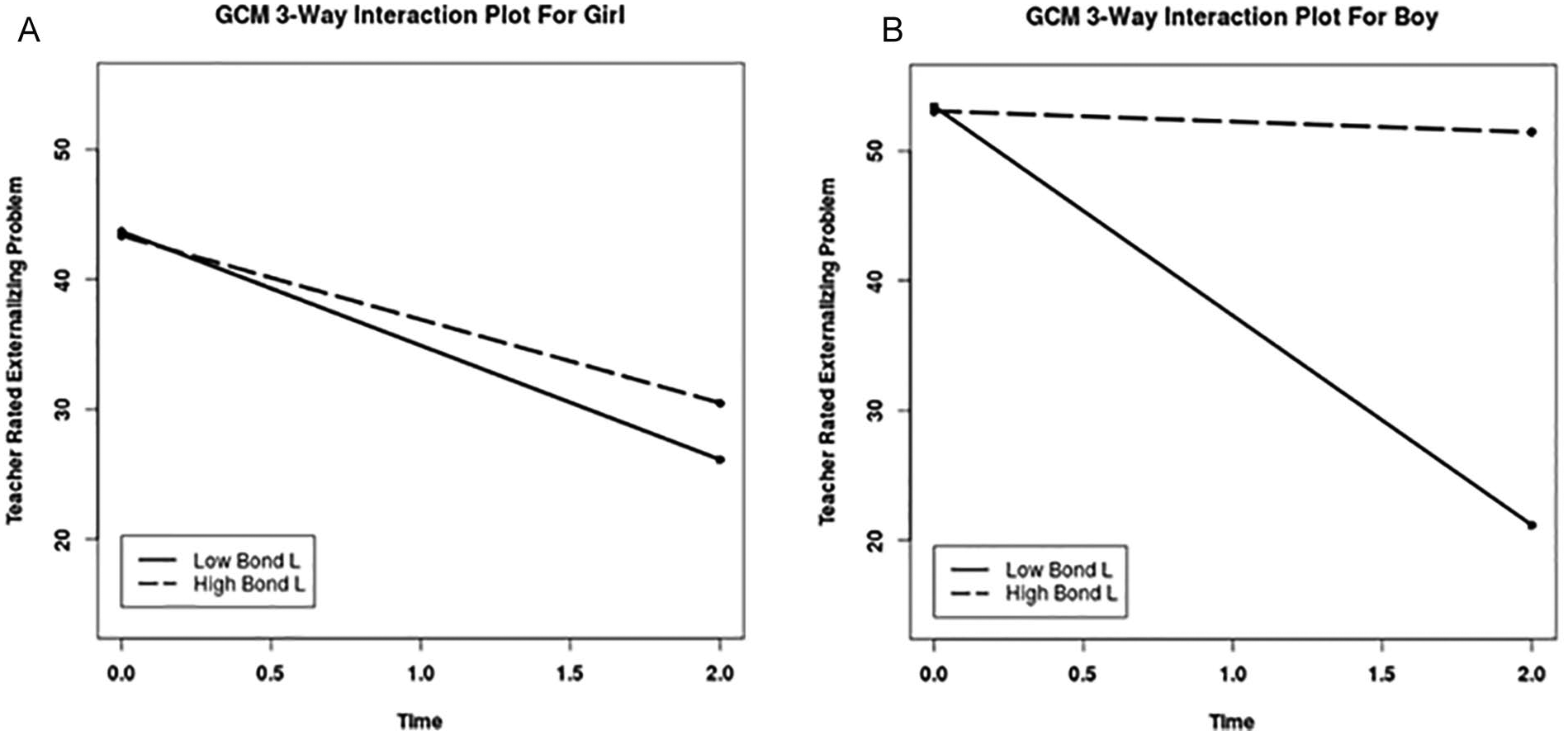
(A) Late Bond × Gender predicting teacher-rated externalizing problems (girls). (B) Late Bond × Gender predicting teacher-rated externalizing problems (boys).
Growth Models for Parent-Rated Externalizing Behavior
Three additional models assessed the task and bond orientations of the therapeutic alliance in the early, middle, and late part of the program predicting parent-rated externalizing behaviors through a 1-year follow-up. For the early intervention sessions, HLM analyses indicated no significant main effect of bond, F(1, 62) = 0.27, p = .87, task orientation, F(1, 62) = 1.68, p = .19, gender, F(1, 62) = 5.06, p = .06, or initial level of aggression, F(1, 62) = −0.23, p = .06. The results indicated a significant interaction between bond and the initial level of aggression at the time of screening, F(1, 62) = 1.47, p = .00 (see Figure 2A and 2B). When children have lower initial levels of aggression relative to other children in this at-risk sample, high bond with the therapist during the early sessions of the intervention is associated with a declining slope of externalizing behavior, whereas a low bond with the therapist during the early intervention session is associated with increased parent-rated externalizing behaviors. However, when children have higher initial levels of aggression, low therapeutic bond scores during the early intervention sessions are associated with a declining slope of externalizing behavior.
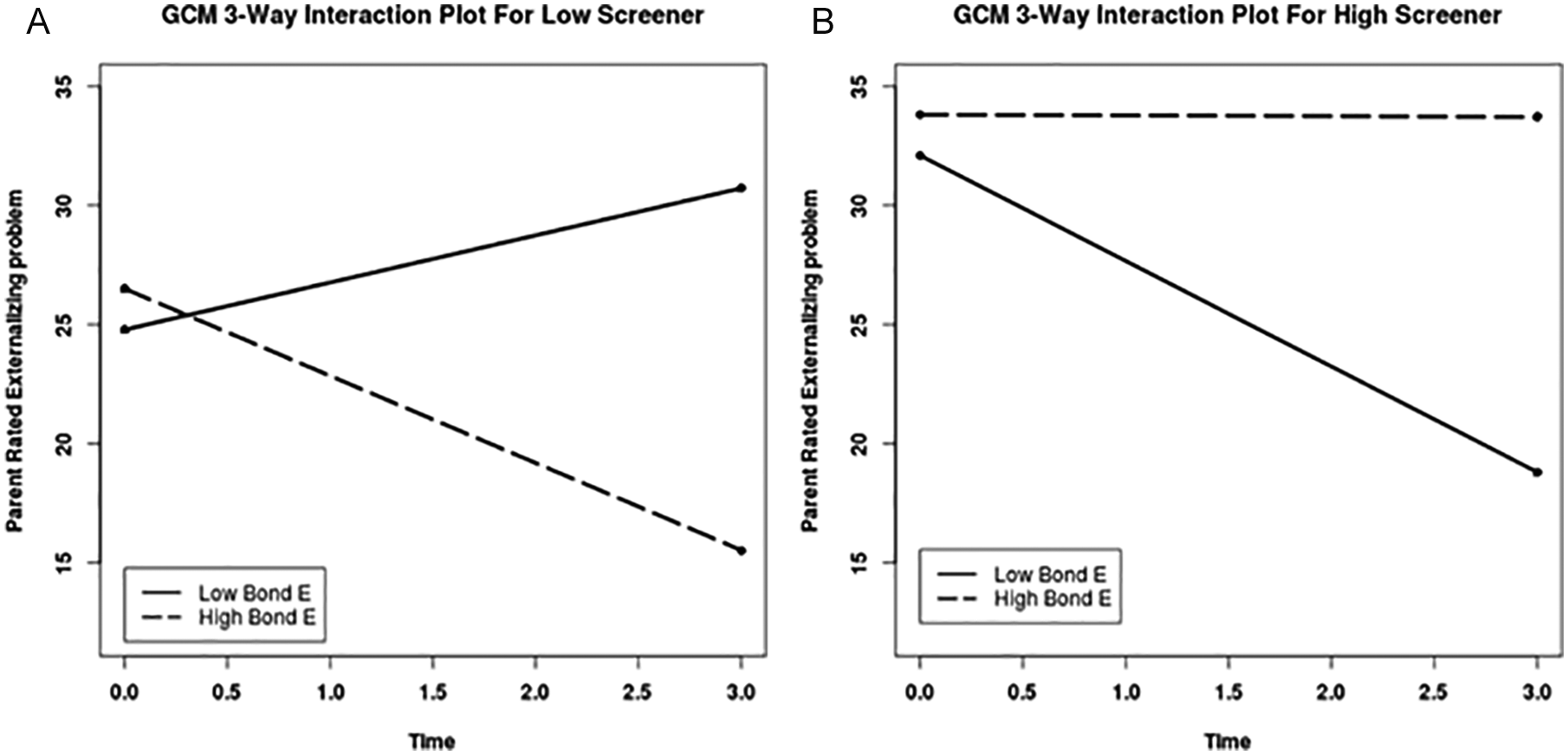
(A) Early Bond × Low Initial Aggression at screener predicting parent-rated externalizing behaviors. (B) Early Bond × High Initial Aggression at screener predicting parent-rated externalizing behaviors.
Another model measured the therapeutic alliance during the middle intervention sessions predicting parent-rated externalizing behaviors. The model results indicated that bond, F(1, 64) = 1.74, p = .29, task, F(1, 62) = 0.58, p = .65, and gender, F(1, 64) = 5.09, p = .07, were not significant predictors of parent-rated externalizing behaviors. The results indicated initial levels of aggression at the time of screening positively predicted parent-rated externalizing behaviors at 1-year follow-up. There were no significant interactions in the model for therapeutic alliance during the middle intervention sessions.
Finally, the last model measured the therapeutic alliance for the late intervention sessions predicting parent-rated externalizing behaviors. There was not a significant main effect of bond, F(1, 62) = −0.44, p = .78, or initial aggression, F(1, 62) = −0.16, p = .16. The results indicated, however, task orientation during late intervention was a significant predictor of parent-rated externalizing behaviors, F(1, 62) = 2.45, p = .03. The model indicated a significant effect of gender, F(1, 62) = 5.38, p = .05. In addition, there was a significant interaction between bond and initial aggression levels at the screening, F(1, 62) = 0.86, p = .03 (see Figure 3A and 3B). This interaction with initial aggression was similar to the interaction found for bonding during the early intervention sessions. When children have lower initial levels of aggression relative to other children in this at-risk sample, a low bond with the therapist is associated with increases in parent-rated externalizing behaviors and a high bond with the therapist is associated with a declining slope of externalizing behavior. However, when children have higher initial levels of aggression, both low and high therapeutic bond scores during the late intervention sessions are associated with a declining slope of externalizing behavior.
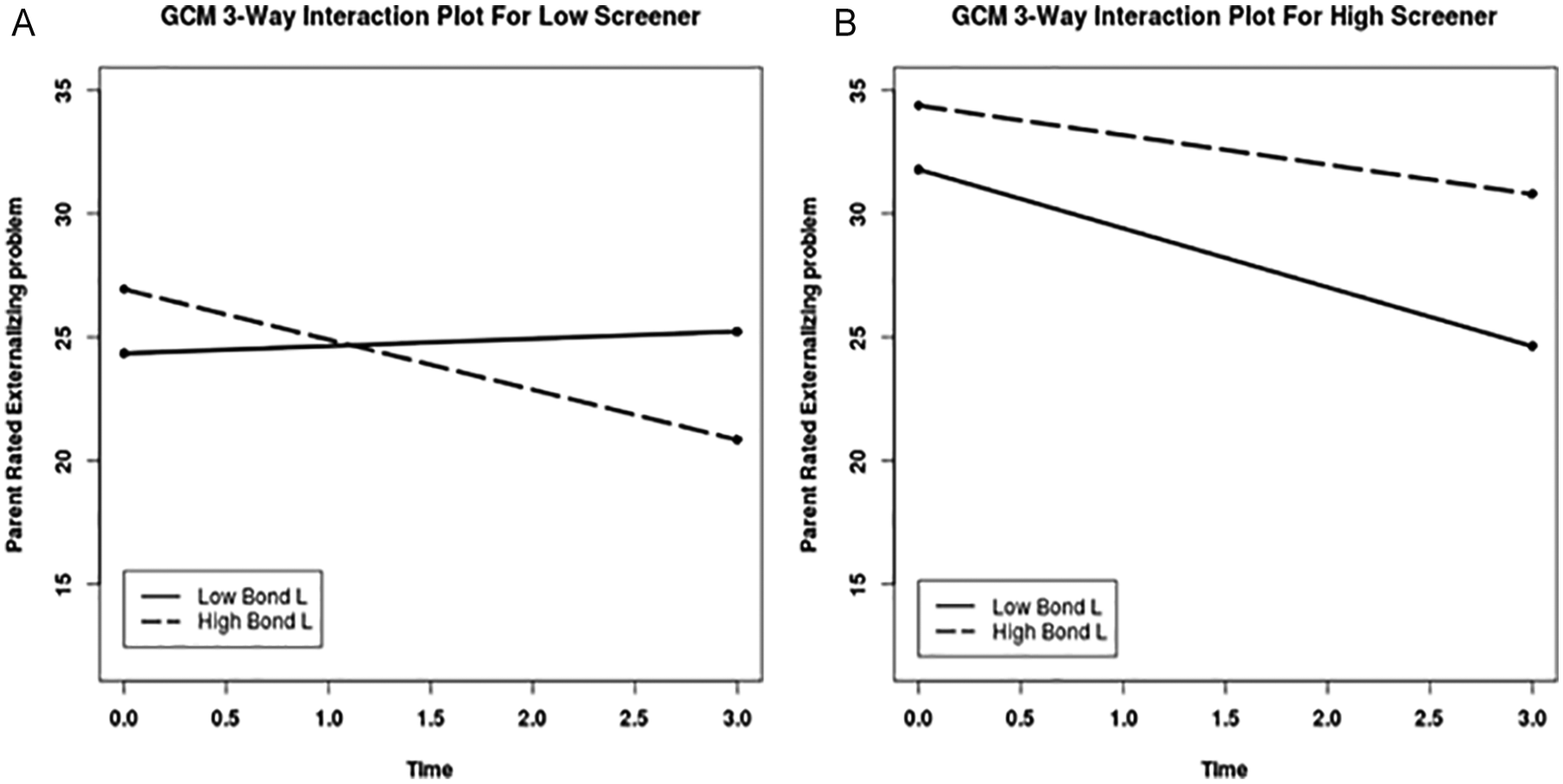
(A) Late Bond × Low Initial Aggression at screener predicting parent-rated externalizing behaviors. (B) Late Bond × High Initial Aggression at screener predicting parent-rated externalizing behaviors.
Discussion
Determining the effectiveness of child therapy is critical to addressing the emotional and behavioral needs of vulnerable children. Both researchers and practitioners agree that understanding the client-therapist alliance and its potential protective effects warrants empirical attention. The purpose of this study was to determine if observer-rated therapeutic alliance could be protective against negative outcomes for children participating in the Coping Power Program. The study contributes to the growing literature endorsing the utility of the TPOCS-A measure to objectively assess the bond and task orientations of the therapeutic alliance. Findings from this study also build on existing research examining the relationship between therapeutic alliance and psychotherapy outcomes in aggressive youth. In the present study, bond significantly predicted teacher-rated externalizing behavior in the early and late intervention sessions as either a main effect or an interaction with gender or initial levels of aggression (i.e., screener). There was a main effect of bond during early intervention sessions predicting teacher-rated externalizing behaviors. However, the main effect of bond was moderated by initial levels of aggression at early and late intervention stages predicting parent-rated outcomes, and also moderated by gender during the late intervention sessions predicting teacher-rated outcomes, which together provide a more comprehensive understanding of the utility of bond when working with aggressive children. Finally, there was a significant main effect of task orientation predicting parent-rated outcomes in late intervention sessions. Bond and task orientation during the middle intervention sessions were not related to outcomes.
Early Bond and Externalizing Behavior in the School Setting
The current study found that bond, not task orientation, is a significant predictor of better behavioral outcomes. Specifically, bonding early in the intervention predicts decreases in externalizing behaviors in elementary school children per teacher report. Furthermore, as bond held value across time while task orientation did not, this result indicates that developing an emotional foundation with a child is important even in a manualized intervention program. This finding speaks to the importance of engaging children in a manner that develops an emotional connection in the first few sessions. It is possible that developing a strong alliance early in the treatment process better enables the child to receive and benefit from a manualized cognitive-behavioral intervention.
Interaction of Bond and Level of Initial Aggression in the Home Setting
The therapeutic bond also emerged as an important predictor of changes in children’s externalizing behavior in the home setting according to parent reports. The importance of effects of the therapeutic bond across settings increases the importance of this key clinical indicator, and the variation in specific findings reflects some variations in how children’s behavior is displayed in home versus school settings because of differences in the social and academic demands of the settings. It is worth considering the influence of reporter, in that a parent is a constant observer of a child’s behavior over many years and may have existing ideas about their child’s behavior, whereas a teacher has the opportunity to observe the child during one academic year. However, it seems likely that the structure imposed by the environment and response to the child of each environment may be a more salient influence on children’s behavior.
Initial preintervention levels of aggression moderated the relationship between therapeutic bond and parent-rated externalizing behaviors during both the early and late intervention sessions. Specifically, at both time points for children with low levels of initial aggression, a high bond with the therapist predicted a decrease in parent-rated externalizing outcomes; however, for children with high levels of initial aggression, a low bond predicted a decrease in externalizing behaviors. This suggests developing a foundational bond between the therapist and child is influential in reaching cognitive-behavioral treatment outcomes, but it is equally important to adapt one’s approach based on the child’s initial aggression level.
The present study suggests it is advantageous for the therapist to prioritize developing a strong relationship with children who exhibit moderate levels of aggression compared with their peers who behave more aggressively. However, for highly aggressive children, although the bond did predict lower amounts of parent-rated externalizing behaviors postintervention, the results suggest the strength of the relationship is less salient. For children who exhibit less initial aggression, therapists may find developing a strong, engaging relationship occurs with minimal effort and quickly provides a context for the child’s behavioral and emotional development. For children who are highly aggressive at the beginning of the treatment, it may be more efficacious to deliver the intervention in a manner which facilitates a general comfort with the clinician but maintains a structured environment that prioritizes the content of the intervention over the interpersonal relationship. It would be advantageous for clinicians to attend to the behavior of the child and adapt their approach to developing the bond accordingly.
Gender as a Moderator
Bond was a significant predictor of decreased externalizing behaviors for girls during early and late sessions of Coping Power. However, for boys, bond was significant early in the intervention and was not found to significantly predict decreased externalizing behaviors in the middle and late sessions of the intervention. It is worth noting that teachers reported higher initial levels of externalizing behaviors in boys than girls (see Figure 1A and 1B). It is possible that at higher levels of externalizing behaviors, it is more important to engage with and form a bond with the child in the first few sessions to reach desired therapeutic outcomes. For boys specifically, when they become connected early with the interventionist, they may be better equipped to proceed and benefit from the cognitive-based therapy presented in the sessions. While continued bonding remained important for girls, these findings indicate the need to anticipate this issue of early bonding and response to the varied needs across gender. These findings provide further evidence of the salience of the bond between the client and therapist. It is important for clinical trainings to emphasize the transformative potential of bonding in the initial sessions when working with youth exhibiting aggressive behaviors, even in the context of a manualized intervention.
Task Orientation
Contrary to expectations, during the late intervention sessions, task orientation emerged as a positive predictor of parent-rated externalizing behaviors. Specifically, the results suggest that during the last sessions of the intervention, when the agreement and mutuality of tasks was high, parents rated their child as exhibiting more externalizing behaviors. It is interesting to note this effect was not found for teacher-rated outcomes during the late sessions, nor at any other time point across parent- or teacher-rated outcomes. One interpretation of this finding may be when a clinician perceives a child as not progressing as well as expected, the clinician may adapt their adherence to the intervention protocol in an effort to create a more structured session and present the material in a more organized manner. While it may be a natural response to emphasize the goals and tasks of the intervention when a child appears disengaged or it is near the conclusion of the intervention, it is necessary for the clinician to refocus on bonding with the child.
Next Steps and Implications
The current study demonstrates the importance of the therapeutic alliance, specifically a strong bond, in decreasing externalizing behaviors in children participating in a manualized intervention. The bond between the child and clinician was particularly salient during the early and late intervention sessions predicting teacher- and parent-rated outcomes. Specifically, for children exhibiting moderate levels of aggression at baseline, a high bond predicted decreased parent-rated externalizing behaviors, and for children exhibiting high levels of initial aggression, a low bond predicted a decrease in externalizing outcomes. The study also indicates that developing a strong bond in early sessions with the child predicts reduced teacher-rated externalizing behavior outcomes across gender. Bond was a significant predictor of decreased externalizing behaviors for boys only for bond assessed in the early sessions. However, for girls, ratings of therapeutic bond were important predictors of reductions of teacher-rated externalizing behaviors when bond was assessed in both early and late parts of the intervention. The study demonstrates the positive impact of developing a strong emotional foundation within the context of a manualized intervention for in a school age sample.
There are mixed findings in the literature about the association between alliance and therapeutic outcomes; however, this study contributes to the growing empirical evidence demonstrating that therapeutic alliance is associated with positive behavioral outcomes. Specifically, the present study indicates that a strong therapeutic alliance is related to decreases in teacher- and parent-reported externalizing behaviors in a sample of elementary school children, and is an important aspect of manualized, cognitive-behavioral treatment. It is important for therapists to receive supervision and training on developing rapport and engaging children from the beginning of treatment to increase the efficacy of the intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported by grants from the National Institute of Drug Abuse (R01DA023156) and the National Institute of Child Health & Human Development (R01HD079273) and a Diversity Supplement for the NICHD parent grant for the first author (R01HD079273).