
Abstract
This study examined whether the links between children’s ADHD symptom severity and academic and social functioning varied based on their aerobic fitness levels. Hierarchical regression models were used to examine the main and interactive effects of inattentive and hyperactive/impulsive (HI) symptom severity and aerobic fitness levels on academic and social functioning in 198 U.S. children (Mage = 6.83; 53% male; 68% White, 14% Mixed Race, 8% Black or African American; 2% Asian; 8% selected the “Other” category when reporting racial identity; across race categories, 15% identified as Hispanic or Latino ethnicity). Children’s aerobic fitness levels were assessed using a multistage fitness test. Parents rated children’s ADHD symptoms, and teachers rated academic and social functioning. Results highlighted negative associations between ADHD symptom severity and adaptive academic and social functioning. Aerobic fitness was positively linked with academic performance. Aerobic fitness moderated the associations between HI symptom severity and academic outcomes, highlighting that aerobic fitness may be protective against academic impairments for children with elevated HI symptoms.
Attention-deficit/hyperactivity disorder (ADHD) affects approximately 7.2% of children worldwide and is characterized by developmentally inappropriate levels of inattentive (IA) and hyperactive/impulsive symptoms (HI; American Psychiatric Association, 2022). Importantly, children with ADHD often experience problems with academic and social functioning (McConaughy et al., 2011). Evidence-based treatments for ADHD include behavioral and pharmacological approaches (for a review, see Evans et al., 2018). However, the ability of these treatments to yield long-lasting effects (Antshel, 2015) and improve children’s academic and social functioning (e.g., Karpenko et al., 2009; O’Connor et al., 2015) is limited. Thus, additional or adjunctive options for child ADHD symptom management are needed.
Physical fitness is operationalized as a set of attributes (e.g., cardiorespiratory and muscular endurance, flexibility, muscular strength, and body composition) that people have or achieve related to their ability to perform physical activity (Caspersen et al., 1985). In typically developing children, physical fitness has been positively associated with academic performance (e.g., Santana et al., 2017) and social functioning (Garcia-Hermoso et al., 2019; LaVigne et al., 2016). Thus, similar to typically developing samples, it is plausible that physical fitness is also linked with better academic and social functioning for children with elevated ADHD symptom severity. Notably, although not specifically examining physical fitness, a related line of research suggests that participation in aerobic physical activity may reduce academic and social functional impairments in children with ADHD (for a review, see Klil-Drori & Hechtman, 2020).
To our knowledge, the links between ADHD symptom severity, physical fitness, and children’s academic and social functioning have not yet been widely studied. Importantly, children diagnosed with ADHD, on average, exhibit poorer academic and social functioning than typically developing children (e.g., Hoza et al., 2005; Loe & Feldman, 2007). Furthermore, physical fitness likely promotes academic and social functioning through its effects on the brain’s structure and function (e.g., Rasberry et al., 2011), and neurocognitive development differs greatly in children diagnosed with ADHD compared to typically developing children (e.g., Chacko et al., 2014). Thus, it is possible the effects of physical fitness on children’s academic and social functioning may vary based on the extent that ADHD symptoms are elevated. Examining the links between ADHD symptoms, physical fitness, and academic and social functioning is critical to determining whether fitness promotion has the potential to augment available ADHD treatments. To fill this gap in the literature, the main goals of the current study were to examine associations between ADHD symptom severity, aerobic fitness, and academic and social functioning and whether the links between children’s ADHD symptom severity and academic and social functioning varied based on their aerobic fitness levels.
Background
Academic and Social Impairments Associated With ADHD
Although not applicable to all children with ADHD (Frazier et al., 2007), many children diagnosed with the disorder experience academic impairments. Specifically, children with ADHD tend to score lower on standardized academic achievement tests and earn lower grades than typically developing peers (for a review, see Loe & Feldman, 2007). Critically, academic impairments linked with childhood ADHD may persist over time. For example, in a large study of adults, those with a childhood ADHD diagnosis were less likely to continue education after high school than controls without a childhood ADHD diagnosis (Kuriyan et al., 2013).
Children diagnosed with ADHD have also been shown to exhibit poorer social skills (Klimkeit et al., 2006), be more rejected by peers, and lack reciprocal friendships compared to peers without ADHD (Hoza et al., 2005). However, not all children diagnosed with ADHD experience social problems (Nijmeijer et al., 2008). Social impairments associated with ADHD may be characteristic of a subset of children with the disorder, such as those who are more aggressive, noncompliant (Erhardt & Hinshaw, 1994), and exhibit conduct problems (Ros & Graziano, 2018). Of utmost concern, children with ADHD and impaired social functioning may be at greater risk for long-term maladjustment. For example, in a large sample of children with ADHD, Mrug and colleagues (2012) found that peer rejection in childhood predicted higher levels of cigarette smoking, delinquency, anxiety, and global impairment (e.g., behavioral and emotional problems, schoolwork problems) in adolescence.
Beyond clinical samples of children diagnosed with ADHD, variability in levels of ADHD symptoms have been linked with academic and social impairments in community-based samples. For example, Rodriguez et al. (2007) noted that elevated levels of IA and HI symptoms were associated with a variety of academic impairments (e.g., reading, writing, mathematics performance) across three large elementary-age European birth-cohort samples. In addition, Stenseng et al. (2016) observed that elevated levels of IA and HI symptoms were associated with greater levels of teacher-rated peer rejection across large cohorts of children ages 4, 6, and 8 years. These examples highlight the importance for research to examine variation in IA and HI symptom severity in young community-based samples, as functional impairments associated with these symptoms are also present outside of clinical samples. Notably, children diagnosed with ADHD experience academic and social functional impairments to different degrees (e.g., Frazier et al., 2007; Nijmeijer et al., 2008). Thus, it is important to examine factors that may influence the relation between ADHD symptom severity and children’s academic and social functioning.
Promoting Academic and Social Functioning via Physical Fitness
Prior research indicates that physical fitness may benefit health and functioning in ways that mitigate academic and social impairments in children with ADHD. Thus, physical fitness may be an important factor to consider when addressing functional impairments associated with ADHD. First, existing literature highlights positive associations between physical fitness and children’s executive functioning abilities (e.g., Van Waelvelde et al., 2020). Furthermore, negative associations between physical fitness and levels of child depressive symptoms have been documented across the extant literature (for a meta-analysis, see Donato et al., 2021), suggesting benefits of physical fitness on child mood. Finally, physical fitness has been positively linked with sleep quality and duration (for a systematic review, see Fonseca et al., 2021). Notably, executive functioning deficits (Diamantopoulou et al., 2007; Tamm et al., 2021), depressive symptoms (Karustis et al., 2000), and sleep problems (Craig et al., 2020; Kirov & Brand, 2014) have all been identified as risk factors for academic and social functional impairments in children diagnosed with ADHD. Given the promise for physical fitness to improve executive functioning, depressive symptoms, and sleep in young children, research exploring links between physical fitness, ADHD symptom severity, and academic and social functioning is needed.
Importantly, although findings from a small body of literature indicate that participating in physical activity helps improve academic performance (e.g., Pontifex et al., 2013) and social functioning (e.g., Smith et al., 2013) in samples of children with elevated levels of ADHD symptoms, to our knowledge, the associations between physical fitness and academic and social functioning for children with elevated ADHD symptom severity have not yet been studied. However, physical fitness has been positively associated with adaptive academic functioning in typically developing samples (e.g., Castelli et al., 2007; Chomitz et al., 2009). For example, results of a large cross-sectional study of third- and fifth-grade students suggested that higher levels of aerobic fitness were associated with higher reading, math, and writing achievement (Castelli et al., 2007).
Promoting physical fitness may also have positive implications for social functioning. Specifically, higher levels of physical fitness have been linked with lower levels of dyadic loneliness, higher levels of perceived social competence (LaVigne et al., 2016), lower rates of bullying (Garcia-Hermoso et al., 2019), and higher levels of peer acceptance (H. C. Chen 2016) in typically developing samples. In addition, H. C. Chen (2016) identified that cardiorespiratory endurance was a stronger predictor of peer acceptance than other measures of physical fitness. Furthermore, in a recent study with adolescent girls, Delli Paoli et al. (2021) observed that girls with higher levels of aerobic fitness exhibited markers of better self-regulation (i.e., greater increases in working memory and lesser decreases in pleasant affect) following social exclusion than girls with lower aerobic fitness levels. Based on the literature documenting the positive associations between aerobic physical fitness and academic and social functioning in typically developing children, it is plausible that aerobic fitness is similarly beneficial for children with elevated ADHD symptoms, who may be at even greater risk for academic and social impairments.
Current Study
Our study examines whether the associations between ADHD symptom severity and indices of academic (i.e., academic performance and academic competence) and social (i.e., social problems and social acceptance) functioning in school-age children varied as a function of aerobic fitness levels. Notably, our sample included both typically developing children and children at risk for, but not diagnosed with, ADHD. Thus, we analyzed children’s levels of IA and HI symptoms dimensionally to capture variation in, and reflect the full range of, ADHD symptom levels present in our sample. These analyses allowed us to explore whether findings varied based on each of the two ADHD symptom categories.
Given the literature documenting that aerobic fitness in typically developing children has been associated with adaptive academic and social functioning (Castelli et al., 2007; H. C. Chen, 2016), we expected higher aerobic fitness levels to be associated with higher academic and social functioning for all children in the sample. Based on previous work indicating that children with ADHD may experience academic and social functional impairments (e.g., McConaughy et al., 2011), we hypothesized that higher ADHD symptom levels would be associated with less adaptive academic and social functioning. Finally, we hypothesized that aerobic fitness would moderate the associations between ADHD symptom levels and academic and social functioning. Specifically, we expected a buffering effect of aerobic fitness such that the negative association between ADHD symptom severity and adaptive academic and social functioning would be stronger at lower, compared to higher, levels of aerobic fitness.
Method
Sample
Baseline assessment data from a randomized controlled trial were used for this study (Hoza et al., 2015). The goal of the randomized controlled trial was to examine the differential effects of two before-school interventions (i.e., physical activity and sedentary classroom activities) on functional outcomes (e.g., emotion dysregulation, peer functioning, behavior problems, ADHD symptom severity) in both typically developing children and children at risk for ADHD (Hoza et al., 2015). Children in kindergarten through second grade participated in the randomized controlled trial from two small U.S. cities. Four children from the randomized controlled trial sample were missing aerobic fitness data, leaving 198 children for our study’s sample. Due to missing data on academic and social functioning indices, ns varied across analyses from 194 to 196. We included all children with complete data for each given analysis.
Children in our sample ranged in age from 4.44 to 8.90 years (Mage = 6.83, SDage = .96), and 53% of children were male. Parents reported child ethnicity and race on a demographic questionnaire designed specifically to meet the reporting requirements of the study’s grant funding agency. Parents first selected one of two options to indicate their child’s ethnicity: (a) Hispanic or Latino, or (b) not Hispanic or Latino. Parents identified 15% of children in this sample as Hispanic or Latino ethnicity. Parents then selected one of the following seven options to indicate their child’s race: (a) American Indian or Alaska Native, (b) Asian, (c) Black or African American, (d) Native Hawaiian or Other Pacific Islander, (e) White, (f) Mixed—Parents are from two or more different groups, or (g) Other. Per parent reports, the racial composition of the sample was 68% White, 14% Mixed Race, 8% Black or African American, 2% Asian, and 8% selected “Other.”
In this sample, 15% of children were enrolled in special education classes. Most children (80%) lived in two-parent households. Parents of all but one child (n = 197) in the sample reported the highest level of parental education represented in the home where the child lives most of the time. The distribution of parental education level varied such that 8% of parents completed less school than needed to obtain a high school degree, 19% completed a high school degree, 31% received an Associate’s/Vocational degree or completed some college, 27% completed a Bachelor’s degree, and 15% received education beyond a Bachelor’s degree.
Parents provided written consent for their children to participate in the current study. After parents provided consent, children and their parents participated in a two-step screening process to determine eligibility for placement in either an ADHD-risk or typically developing group for the randomized controlled trial (Hoza et al., 2015; see Table 1 for details). Children were screened (N = 428) using parent and teacher ratings on the ADHD Rating Scale IV (DuPaul, 1991) at Step 1. At Step 2, parents of potential participants (N = 338) completed the ADHD module of the National Institute of Mental Health Diagnostic Interview Schedule for Children, Version Four (Shaffer et al., 2000) and the Impairment Rating Scale (Fabiano et al., 2006).
Inclusion and Exclusion Criteria for Participant Eligibility.
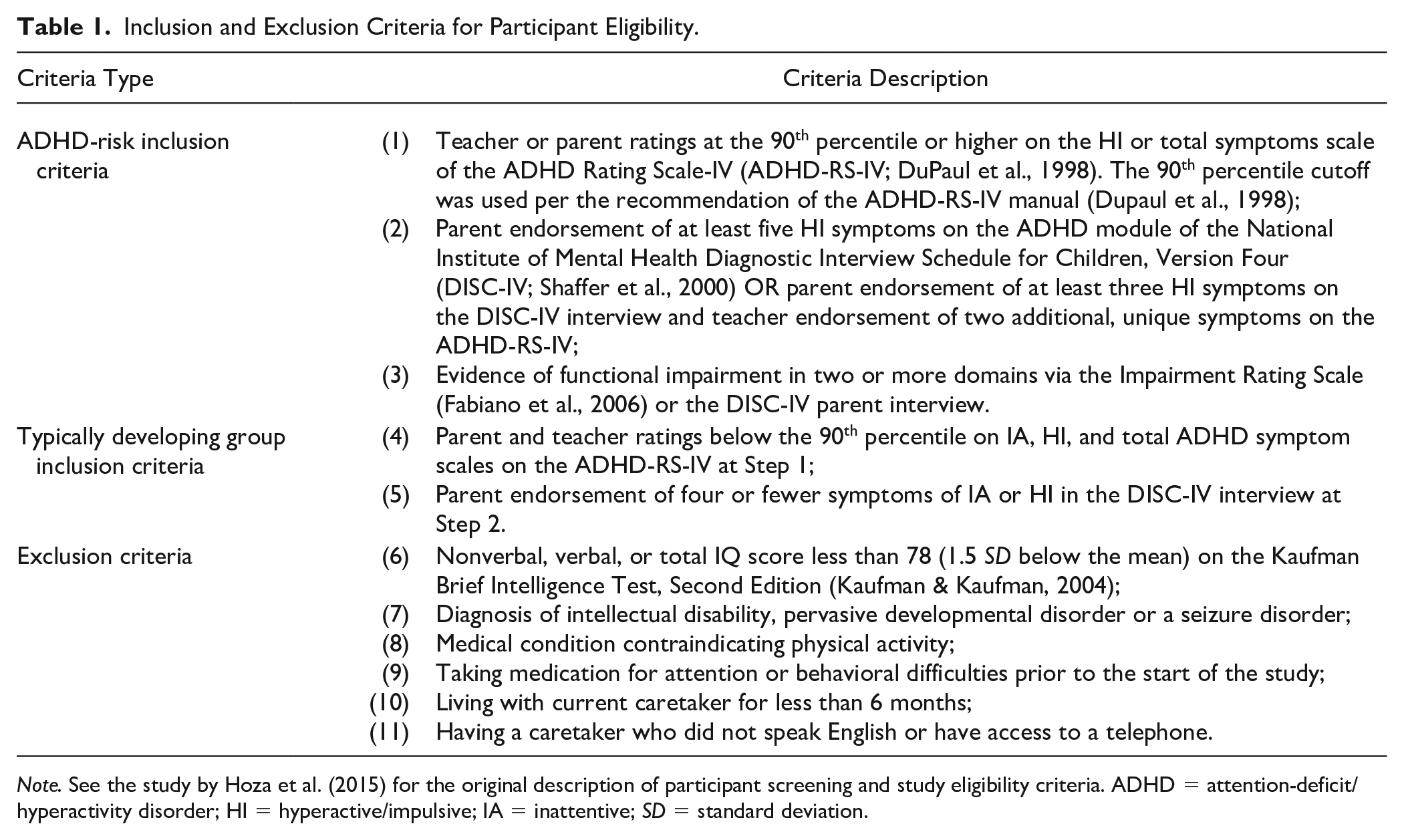
Note. See the study by Hoza et al. (2015) for the original description of participant screening and study eligibility criteria. ADHD = attention-deficit/hyperactivity disorder; HI = hyperactive/impulsive; IA = inattentive; SD = standard deviation.
Of note, the focus on HI symptoms in ADHD-risk classification for this study was in consideration of the young age of children in the sample to account for lower IA symptom presentation at this age (Barkley, 2003). Notably, children taking medication for ADHD at study enrollment were excluded from this sample in an attempt to eliminate any confounding effects of pharmacological intervention on the effects of the physical activity intervention being studied in the randomized controlled trial. However, children were allowed to continue to participate in the study if they began taking ADHD-related medication over the course of the study (n = 4), as it would be unethical to withhold medication (a treatment deemed necessary by medical providers) due to participation in a research study of an alternate intervention. The final randomized controlled trial sample included 94 children in the ADHD-risk group and 108 children in the typically developing group (N = 202). Close to half of the final study sample was in the ADHD-risk group because children at elevated risk for ADHD were purposefully oversampled given the goals of the randomized controlled trial (Hoza et al., 2015).
Measures
IA and HI Symptom Severity
The ADHD Rating Scale-IV (DuPaul, 1991) was utilized to measure IA and HI symptom severity in our study. The ADHD Rating Scale-IV includes two, nine-item subscales capturing children’s levels of IA (e.g., “does not seem to listen when spoken to directly,” “has difficulty organizing tasks and activities”) and HI (e.g., “talks excessively,” “has difficulty awaiting turn”) symptoms, respectively. Parents rated each item on the ADHD Rating Scale-IV on a four-point Likert-type scale from 0 (“Never or Rarely”) to 3 (“Very Often”). Higher scores reflect greater levels of ADHD symptom severity. Children’s mean IA and HI symptom severity scores were utilized in the current study. Scores from the parent version of the ADHD Rating Scale-IV have demonstrated good reliability and validity (DuPaul et al., 1998); in this sample, internal consistency reliability estimates were α = .93 for IA and α = .92 for HI.
The ADHD Rating Scale-IV is an age- and gender-normed measure assessing symptoms of ADHD as specified by the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Importantly, although ADHD symptoms were measured utilizing a DSM-IV rating scale, symptoms remain consistent with current Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association, 2022) diagnostic criteria, as symptoms have not changed across versions (American Psychiatric Association, 2022). Furthermore, as mentioned previously, parent and teacher ratings on the ADHD Rating Scale-IV were collected to determine study eligibility. However, we used only parent ratings in our study to avoid common rater bias with the outcomes of interest, which were measured via teacher report (see the following sections).
Aerobic Fitness
The 15-meter version of the Progressive Aerobic Cardiovascular Endurance Run (PACER; McClain et al., 2006) was used to assess aerobic fitness. Children completed the PACER on a measured course that was marked by cones. The course was set up in the school gymnasium/school cafeteria before the start of the school day. For this task, children ran continuously back and forth across the 15-meter span at a specified speed, which was signaled by an audio tone. At periodic intervals, the time allotted to complete the 15-meter segment shortened, increasing difficulty of the task. Failure to run the full 15 meters in the allotted time on any given segment resulted in a “miss.” Children were allowed two “misses” prior to task termination. The total number of segments completed on the PACER, excluding misses, served as the measure of aerobic fitness utilized in analyses for this study. The PACER has demonstrated good validity and reliability for use with children (Plowman & Meredith, 2013).
Academic Functioning Indices
Academic Performance
The academic performance subscale from the Teacher’s Report Form (Achenbach & Rescorla, 2001) was utilized as a measure of academic performance in our study. The academic performance subscale includes up to six fill-in-the-blank items, on which teachers write in academic subjects children participate in at school. Teachers rated children’s level of academic performance in each subject on a five-point Likert-type scale from 1 (“Far Below Grade Level”) to 5 (“Far Above Grade Level”). Higher scores reflect greater levels of academic functioning. The academic performance subscale yields raw scores, which are converted into standardized T scores based on child sex and age. T scores were utilized in our study. T scores on the academic performance scale ranged from 35 to 65 in this sample.
Academic Competence
The cognitive competence subscale from the teacher-report version of the Pictorial Scale of Perceived Competence and Social Acceptance for Young Children (Harter & Pike, 1984) was utilized as a measure of academic competence in our study. All items from two versions (preschool and kindergarten; first and second grade) of the Pictorial Scale of Perceived Competence and Social Acceptance for Young Children (Harter & Pike, 1984) were utilized because children in kindergarten through second grades participated in this study. The full combined version of the cognitive competence subscale includes 12 items capturing teacher’s perceptions of children’s abilities across a variety of academic skills (e.g., “Good at numbers”; “Knows alphabet”). Teachers rated each item on the cognitive competence subscale on a four-point Likert-type scale from 1 (“Not Very True”) to 4 (“Really True”). Higher scores on the cognitive competence scale reflect greater levels of academic functioning. Item scores were averaged to produce a cognitive competence subscale score. Ratings on at least half of the subscale items were required to calculate the subscale score. The cognitive competence subscale scores demonstrated good internal consistency reliability in this sample (α = .94).
Social Functioning Indices
Social Problems
The social problems subscale from the Teacher’s Report Form (Achenbach & Rescorla, 2001) was utilized as a measure of social problems for this study. The social problems subscale includes 11 items capturing different social difficulties teachers may observe in their students (e.g., “Clings to adults or too dependent”; “Doesn’t get along with other pupils”; “Not liked by other pupils”). Teachers rated each item on the social problems subscale on a three-point Likert-type scale from 0 (“Not True”) to 2 (“Very True or Often True”). Higher scores reflect lower levels of social functioning. The social problems subscale yields raw scores, which are converted into standardized T scores based on child sex and age. T scores were used for analyses in this study. T scores on the social problems subscale can range from 50 to 100; scores are truncated at a minimum of 50 to reflect that low ratings on subscale items suggest average social functioning (Achenbach & Rescorla, 2001). T scores on this subscale in our sample ranged from 50 to 85. The social problems subscale scores demonstrated adequate internal consistency reliability in this sample (α = .73).
Social Acceptance
The teacher-report version of the peer acceptance subscale from the Pictorial Scale of Perceived Competence and Social Acceptance for Young Children (Harter & Pike, 1984) was utilized as a measure of social acceptance in our study. All items from two teacher-report versions (preschool and kindergarten; first and second grade) of the Pictorial Scale of Perceived Competence and Social Acceptance for Young Children (Harter & Pike, 1984) were utilized because children in kindergarten through second grades participated in the current study. The full combined version of the peer acceptance subscale includes eight items measuring teacher’s perceptions of children’s social acceptance across a variety of common scenarios (e.g., “Has friends to play with”; “Others share with this child”). Teachers rated each item on the peer acceptance subscale on a four-point Likert-type scale from 1 (not very true) to 4 (really true). Higher scores on the peer acceptance subscale reflect greater levels of social functioning. Item scores were averaged to produce a peer acceptance subscale score. Ratings on at least half of the subscale items were required to calculate the subscale score. Of note, missing data analyses revealed that a majority of data (64%) were missing on two of the eight peer acceptance items (i.e., “Stays overnight at friends” and “Eats dinner at friends”). For the remaining six items, missing data rates were 5% or lower. Thus, the two items with the majority of data missing were dropped from the subscale in the present study. The modified peer acceptance subscale scores demonstrated good internal consistency reliability in this sample (α = .95).
Demographic Data
Demographic variables included as covariates in hypothesis tests (i.e., children’s sex and age [in months]) were obtained via parent report.
Data Analysis Strategy
Data were analyzed using IBM SPSS version 26. Hierarchical multiple regression analyses were used to test the study hypotheses. In all regression models, child sex and age were entered as covariates at Step 1. The focal ADHD symptom severity variable (i.e., mean IA or HI symptom severity) and aerobic fitness levels were entered at Step 2. The interaction between the focal ADHD symptom severity variable and aerobic fitness levels was entered at Step 3. Prior to entry into the regression models, continuous predictors were mean-centered, and sex was weighted effect coded. Weighted effect coding is a statistical method utilized to include categorical variables in regression models and moderation analyses such that the estimates for each category represent the deviation from the sample mean (te Grotenhuis et al., 2017). To probe significant interactions, moderation analyses were conducted using the PROCESS macro (Hayes, 2017) to obtain estimates of the effects of IA and HI symptom severity on academic and social functioning indices at low (−1 SD) and high (+1 SD) levels of aerobic fitness.
Results
Descriptive Statistics and Preliminary Associations
Descriptive statistics and correlations for all study variables were examined prior to hypothesis testing and are presented in Table 2. IA and HI symptom severity were associated with less adaptive academic and social functioning across all indices and were negatively associated with aerobic fitness. Aerobic fitness was positively associated with academic performance, academic competence, and social acceptance but was not associated with social problems. Child sex (0 = male, 1 = female) was negatively associated with IA and HI symptom severity and positively associated with academic competence. Thus, on average, boys displayed higher levels of ADHD symptoms than girls, and girls were rated by teachers as higher in academic competence.
Descriptive Statistics and Intercorrelations Among All Study Variables.

Note. IA = inattentive; HI = hyperactive/impulsive.
0 = male, 1 = female.
p < .10. *p < .05. **p < .01. ***p <.001.
IA Models
Four hierarchical regression models were utilized to examine the effects of IA symptom severity, aerobic fitness, and their interaction on children’s academic and social functioning (see Table 3). At Step 2 in these models, the associations between IA symptom severity and all four academic and social functioning indices were significant after accounting for the effects of the covariates. Specifically, higher levels of IA symptoms were linked with less adaptive academic and social functioning. In addition, at this step, higher levels of aerobic fitness were associated with higher levels of academic performance after accounting for IA symptom levels. However, aerobic fitness was not associated with academic competence, social problems, or social acceptance. At Step 3 in these models, the interaction between IA symptom severity and aerobic fitness was not significant in any models.
Associations Between IA Symptoms and Aerobic Fitness Predicting Academic and Social Functioning.
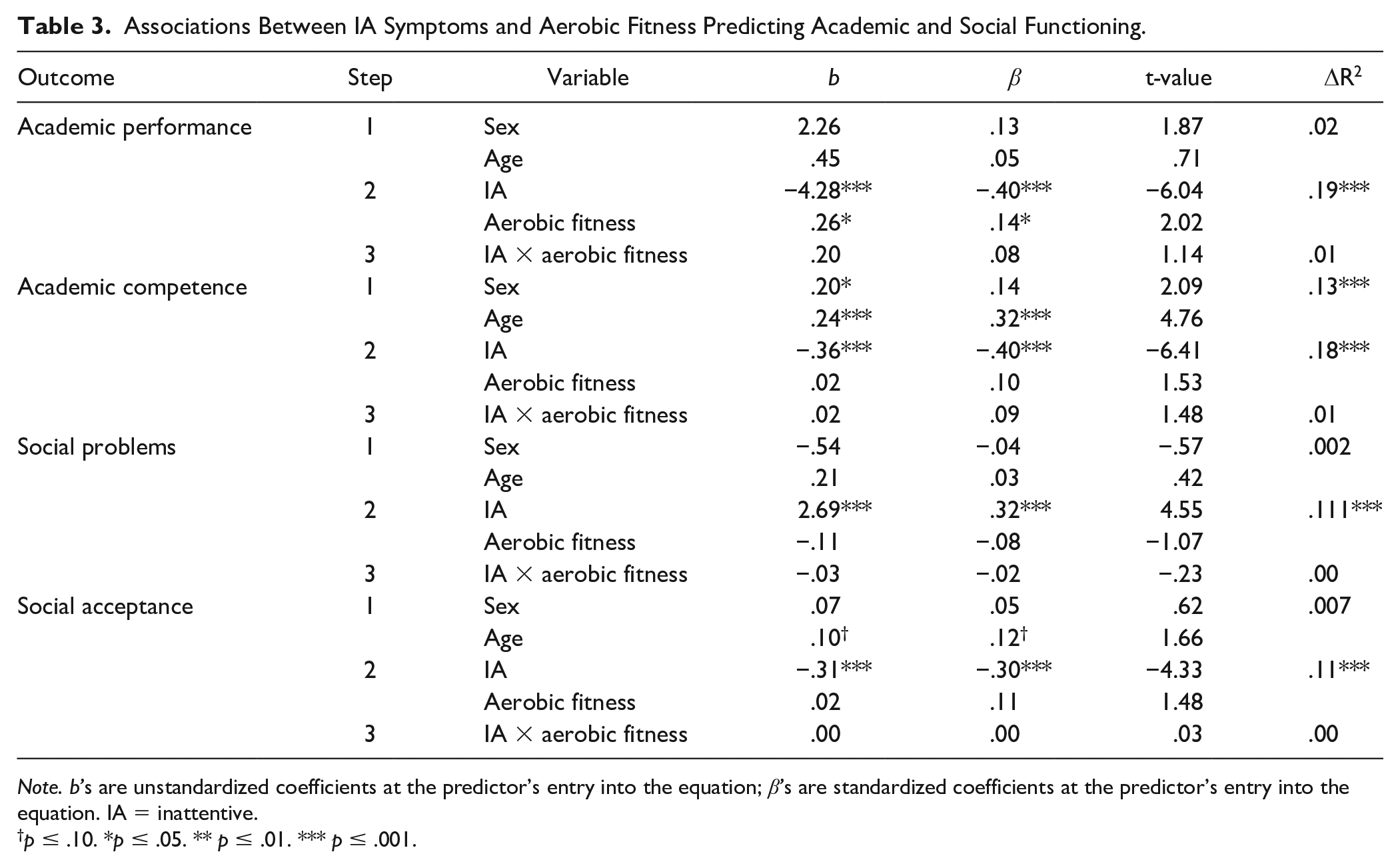
Note. b’s are unstandardized coefficients at the predictor’s entry into the equation; β’s are standardized coefficients at the predictor’s entry into the equation. IA = inattentive.
p ≤ .10. *p ≤ .05. ** p ≤ .01. *** p ≤ .001.
HI Models
Four hierarchical regression models were utilized to examine the effects of HI symptom severity, aerobic fitness, and their interaction on children’s academic and social functioning (see Table 4). At Step 2 in these models, the associations between HI symptom severity and all four academic and social functioning indices were significant after accounting for the effects of the covariates. Specifically, higher levels of HI symptoms were associated with less adaptive academic and social functioning. In addition, at this step, higher levels of aerobic fitness were associated with higher academic performance after accounting for HI symptom levels. However, aerobic fitness was not associated with any of the other academic or social functioning indices. At Step 3 in these models, the interactions between aerobic fitness and HI symptom severity significantly predicted both academic functioning indices and one social functioning index. Specifically, the addition of the interaction term in these models predicted an additional 2% of the variance in academic performance, academic competence, and social problems, over and above the covariates and the main effects of child HI symptom severity and aerobic fitness. The interaction between HI symptom severity and aerobic fitness did not predict social acceptance.
Associations Between HI Symptoms and Aerobic Fitness Predicting Academic and Social Functioning.
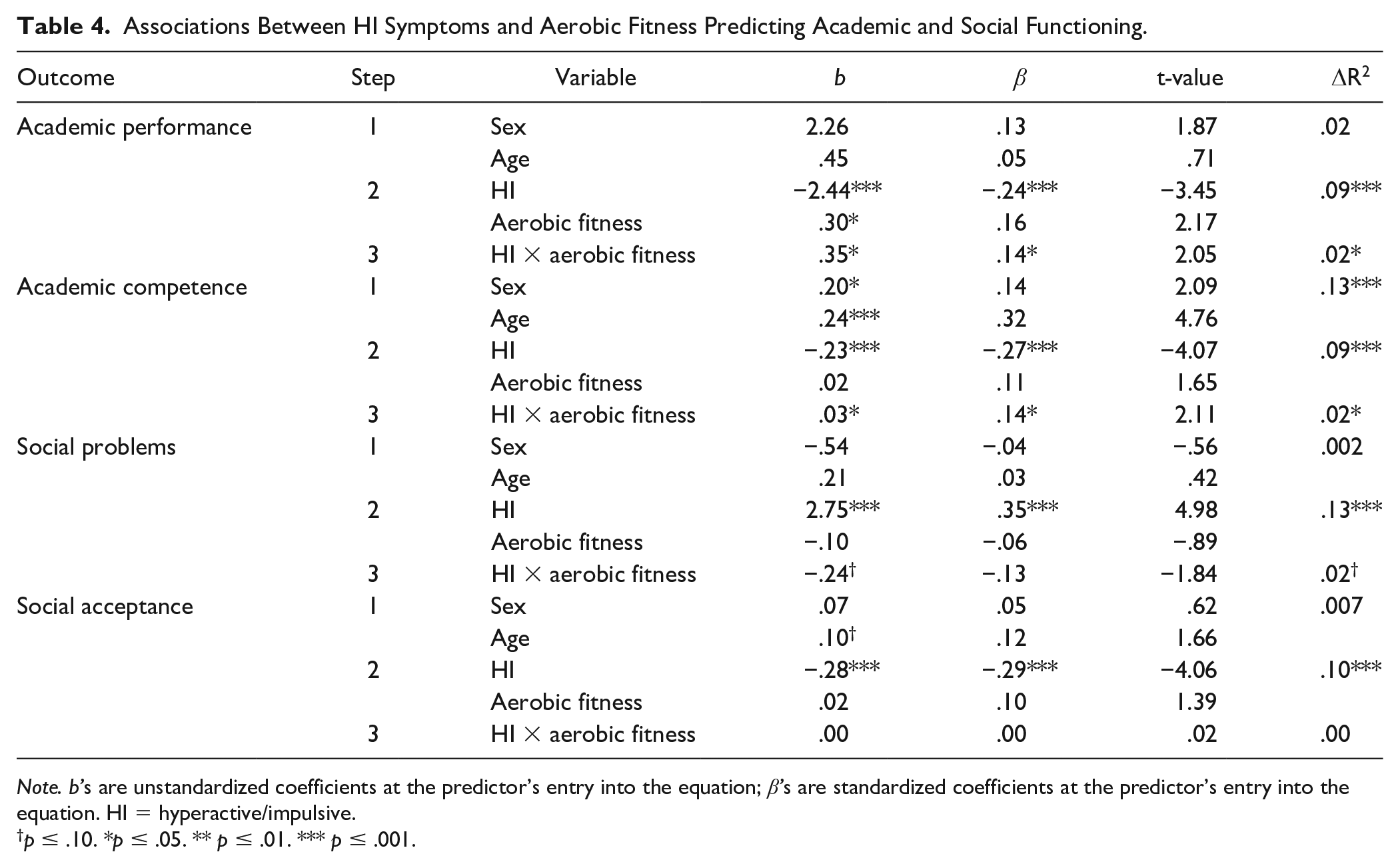
Note. b’s are unstandardized coefficients at the predictor’s entry into the equation; β’s are standardized coefficients at the predictor’s entry into the equation. HI = hyperactive/impulsive.
p ≤ .10. *p ≤ .05. ** p ≤ .01. *** p ≤ .001.
Simple-slope analyses were conducted to probe significant and trend-level interactive effects. When academic performance was the focal academic functioning index, higher levels of HI symptoms were associated with lower academic performance at lower (b = −3.83, β = −.38, p < .001), but not higher (b = −.76, β = −.08, p = .351), levels of aerobic fitness (see Figure 1A). When academic competence was the focal academic functioning index, higher levels of HI symptoms were linked with lower levels of academic competence at lower (b = −.34, β = −.40, p < .001), but not higher (b = −.08, β = −.10, p = .401), levels of aerobic fitness (see Figure 1B). When social problems were the focal social functioning index, higher levels of HI symptoms were significantly linked with higher levels of social problems at lower levels of aerobic fitness (b = 3.72, β = .47, p < .001) and marginally linked at higher levels of aerobic fitness (b = 1.57, β = .20, p = .063; see Figure 1C).
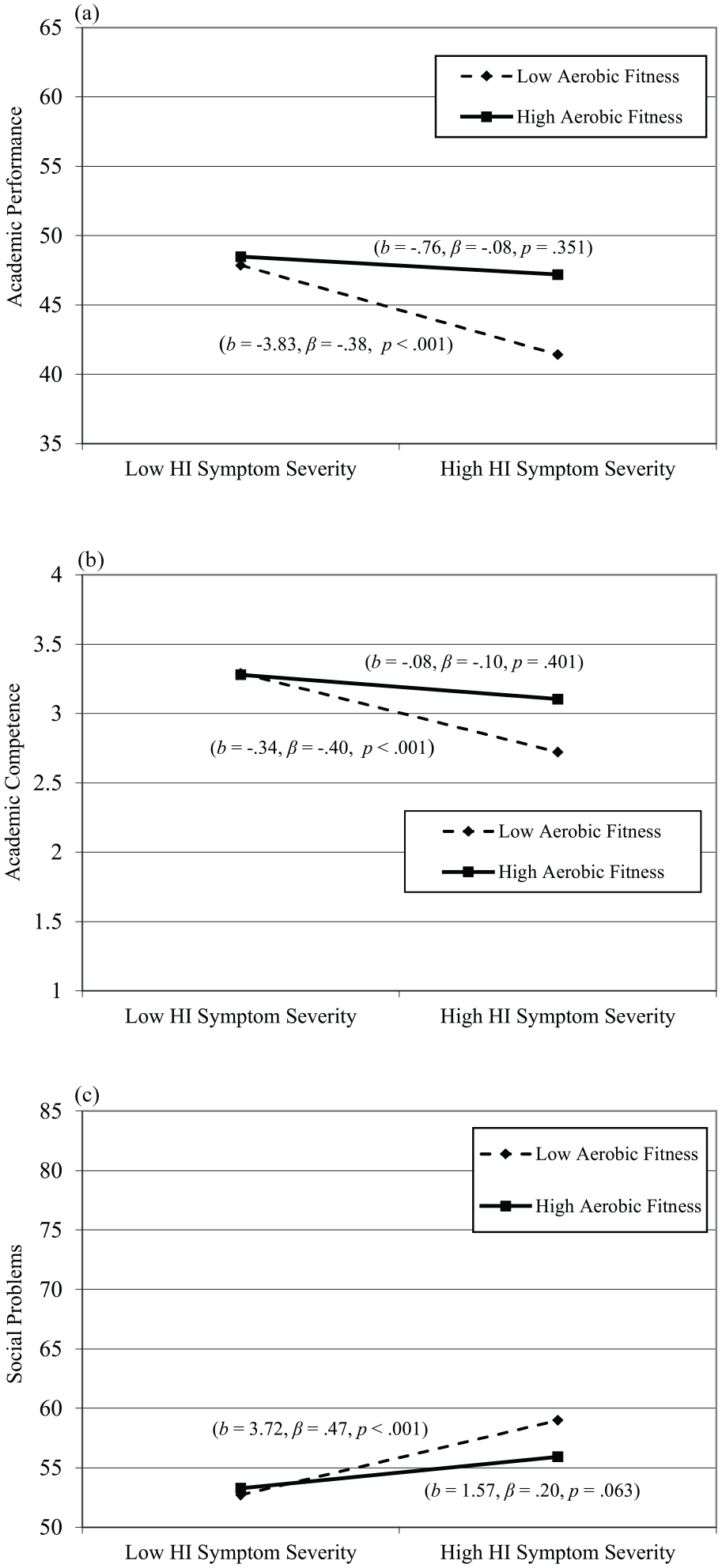
Interactive Effects of HI Symptom Severity and Aerobic Fitness on Academic and Social Functioning Indices. (a) Interactive effects of HI symptom severity and aerobic fitness on academic performance. (b) Interactive effects of HI symptom severity and aerobic fitness on academic competence. (c) Interactive effects of HI symptom severity and aerobic fitness on social problems.
Discussion
Our main study goals were to examine the effects of IA and HI symptom severity and aerobic fitness as predictors of children’s academic and social functioning and to investigate whether the relations between children’s ADHD symptom severity and academic and social functioning would vary as a function of their aerobic fitness levels. Notably, our findings highlight the potential for aerobic fitness to serve as a protective factor in the negative association between HI symptom severity and academic functioning.
Main Effects of ADHD Symptoms and Fitness on Academic and Social Functioning
Our results yielded partial support for our first set of hypotheses related to the main effects of ADHD symptom severity and aerobic fitness on children’s academic and social functioning. Consistent with previous literature demonstrating that children with elevated ADHD symptoms often experience academic (e.g., Loe & Feldman, 2007) and social (e.g., Hoza et al., 2005) functional impairments, we observed that both higher IA and HI symptom severity were linked with poorer academic and social functioning in our sample. We also observed that aerobic fitness was positively associated with children’s academic performance but was not associated with academic competence, social problems, or social acceptance, when also accounting for IA or HI symptom levels. These findings differ from positive associations between aerobic fitness and adaptive academic (e.g., Santana et al., 2017) and social (e.g., H. C. Chen, 2016; LaVigne et al., 2016) functioning observed in previous work with typically developing samples.
Our findings likely differ from previous work with typically developing samples due to our inclusion of ADHD symptom severity in our regression models. Although we observed significant bivariate correlations between aerobic fitness and three out of four academic and social functioning indices (with the exception of social problems), these associations did not hold when accounting for ADHD symptom severity in our regression models. Thus, IA and HI symptoms emerged as particularly robust predictors of these functional indices, and there was less unique variance to be accounted for by aerobic fitness with these ADHD symptom severity variables in our models. To our knowledge, our study is the first to examine the effects of aerobic fitness over and above ADHD symptom severity on children’s academic and social functioning. Thus, future replications of our work are needed.
Another possible reason our findings differed from those with typically developing samples could be our use of teacher reports of academic and social functioning. In contrast, some previous studies included child reports of social functioning (e.g., LaVigne et al., 2016) and academic performance measured via standardized tests administered directly to children (e.g., Castelli et al., 2007; Chomitz et al., 2009). Furthermore, our academic competence measure captured teacher’s perceptions of children’s abilities across different academic skills (e.g., good at writing, good at numbers), whereas prior studies with typically developing samples have focused on academic performance only (e.g., test scores; Castelli et al., 2007; Chomitz et al., 2009). Thus, aerobic fitness may be associated with academic skills not captured by our measure, such as test-taking abilities. Finally, we focused specifically on aerobic fitness. In contrast, other studies have included broader physical fitness measures capturing muscular strength (e.g., LaVigne et al., 2016), agility, and flexibility (e.g., Chomitz et al., 2009). Thus, more research is needed before definitive conclusions are possible.
Interactive Effects of ADHD Symptom Severity and Fitness on Functional Outcomes
Our results also provided partial support for our primary hypotheses regarding interactive effects. First, in support of our hypotheses, we observed that aerobic fitness moderated the association between children’s HI symptom severity and both academic functioning indices. Specifically, higher levels of HI symptom severity were associated with lower levels of academic outcomes at lower, but not higher, aerobic fitness levels. Based on our findings, aerobic fitness may play an important role in supporting academic functioning for children with high levels of HI symptoms, potentially serving as a protective factor against academic functional impairments.
In addition, we observed that the association between HI symptom severity and social problems varied as a function of aerobic fitness at trend level, highlighting that aerobic fitness may also potentially serve as a protective factor concerning social problems associated with HI symptoms. However, these findings did not meet the threshold for significance; thus, future research is needed before definitive conclusions can be made. Importantly, our measure of social problems is broad and captures various child social behaviors (e.g., children’s loneliness, tendency to be teased by peers, ability to get along with others). Thus, future research should examine the interactive effects of aerobic fitness and ADHD symptom severity on specific, well-defined social functioning indices (e.g., social skills, peer reputation) to identify which facets of social functioning may be influenced by aerobic fitness levels.
Contrary to our hypotheses, we did not observe significant interactive effects across our models when social acceptance was the focal social functioning index. The differences in our findings related to the two social functioning indices possibly reflect that aerobic fitness may not be powerful enough to be protective beyond the effects of ADHD symptoms on children’s social acceptance. As noted in the literature, the negative reputations of children with ADHD are often enduring and difficult to change among peers (e.g., Hoza, 2007). Importantly, social acceptance depends not only on the behavior of children with elevated levels of ADHD symptoms but also on the characteristics (e.g., receptiveness to being friends, inclusionary behavior) of their peers.
Highlighting this idea, a study comparing contingency-management training for school-age children with ADHD to contingency-management training plus additional social-inclusion training for peers found that only the latter treatment condition improved social acceptance of children with ADHD (Mikami et al., 2013). Thus, although there is preliminary evidence suggesting that participation in regular cardiovascular exercise, which would likely increase aerobic fitness, improves social skills in children with ADHD (for a review, see Den Heijer et al., 2017), improved social skills at the individual level may not be enough to bolster social acceptance, which also relies on peer characteristics. It is also possible that although some social problems may be easy for teachers to observe (e.g., not getting along with peers), teachers may not be the best reporters of children’s social acceptance. In fact, we had to drop items that teachers did not regularly answer from our social acceptance measure. These items pertained to children’s social interactions outside of school (e.g., eating dinner at friends’ houses), which may have been challenging for teachers to accurately rate. Future research should include additional measures of social acceptance (e.g., peer nominations) to address this potential issue.
In contrast to our hypotheses, the effects of IA symptom severity on all four indices of children’s academic and social functioning did not vary as a function of aerobic fitness levels. Importantly, some prior research suggests IA symptoms may be more strongly associated with executive functioning deficits than HI symptoms in children with ADHD (Willcutt et al., 2005). Thus, these null findings were particularly surprising if, as speculated previously, the effect of aerobic fitness on academic and social functioning in children with elevated ADHD symptom levels is due to associations with their executive functioning abilities. However, when accounting for IA symptom levels in our regression models, aerobic fitness was only associated with one academic functioning index (academic performance).
It is possible that interactive effects between IA symptom severity and aerobic fitness did not emerge in the current study due to aspects of sample recruitment. We employed a community sample originally recruited for a randomized controlled trial, and children were included in the ADHD-risk group if they displayed at least five HI symptoms across parent and teacher reports. Thus, children who presented with only elevated IA symptoms (e.g., without additionally displaying elevated HI symptoms) were not included in our sample. As such, our recruitment strategy might have made it difficult to detect our effects of interest. Future research should continue to explore the associations examined in our study in a sample that also includes children with elevated levels of IA symptoms only, as is it difficult to know whether our findings would be replicated in a sample including children with that specific symptom presentation.
Importantly, the results of our study should only be interpreted within the context of additional key limitations of our data that we have not previously discussed. First, our data are cross-sectional; thus, we cannot conclude whether higher aerobic fitness levels are causally associated with academic and social functioning in children with elevated HI symptom severity. Longitudinal research examining the effects of aerobic fitness on academic and social functioning over time in children at risk for ADHD is needed. Furthermore, we were limited by our use of an archival dataset, which included a measure of child race/ethnicity that, in current times, could be considered restricted. Future studies should prioritize the use of more-refined and inclusive measures of child race/ethnicity.
Despite these limitations, our findings highlight an important avenue for future research, as promoting children’s aerobic fitness may potentially augment treatment strategies aimed at addressing academic impairments often experienced by children with ADHD (e.g., Loe & Feldman, 2007). We hope our findings will serve as preliminary support for continued longitudinal research into the links between ADHD symptom severity, aerobic fitness, and academic and social functioning. Furthermore, as hypothesized previously, aerobic fitness may be beneficial for academic and social functioning in children with ADHD because it may improve aspects of health that children with ADHD often struggle with, including executive functioning abilities, mood, and sleep quality and duration. To our knowledge, tests of these specific mechanisms of effect have not yet been conducted and should be the focus of future research.
Clinical Implications
This study extends the existing literature documenting the positive effects of physical fitness on typically developing children’s academic outcomes by highlighting that aerobic fitness may be a protective factor for academic performance and competence for children with elevated HI symptom severity. These findings are important given that children with elevated HI symptom severity may be more likely than typically developing peers to experience academic impairments (Loe & Feldman, 2007). Thus, even small effect sizes (as observed in our study) related to physical fitness above and beyond HI symptom severity are meaningful given the need to identify avenues to reduce academic impairments typically experienced by children at elevated risk for ADHD. Furthermore, our results highlight the potential for aerobic fitness to be protective against social problems among children with elevated HI symptom severity although these findings only occurred at trend level.
Overall, our findings suggest the potential utility of promoting children’s aerobic fitness as a strategy for addressing academic, and possibly some social, impairments associated with HI symptoms. Only incorporating interventions to improve physical fitness would likely not be enough to fully address the shortcomings of current ADHD treatments in improving children’s academic and social impairments. However, incorporating strategies to help children improve their aerobic fitness could potentially augment these treatments. Notably, in many communities, there may be opportunities to promote physical fitness without great financial cost. For example, physical activity can be incorporated into programs at schools, and providers can encourage ideas for engagement in physical activity that are of little cost to families (e.g., playing in the park, going for family walks/hikes). Future research into the effects of physical activity interventions on academic and social functioning in children with elevated ADHD symptom severity is warranted.
Beyond supporting academic and social functioning, encouraging physical fitness in young children with ADHD symptoms may have additional important health benefits. Specifically, there is a growing literature documenting a positive link between ADHD diagnoses and obesity (for a review, see Cortese & Vincenzi, 2012). For example, a study comparing obesity prevalence rates in large cohorts of children with and without select health conditions (e.g., asthma, hearing/vision impairments, learning disorders, autism spectrum disorder, and ADHD) found that 18.9% of children with ADHD were obese compared to 12.2% of children without any of these health conditions (A. Y. Chen et al., 2010). Thus, while our findings indicate aerobic fitness may buffer otherwise negative academic outcomes for children with elevated HI symptoms, the broader literature also suggests that promoting positive health outcomes, like physical fitness, in children with and at risk for ADHD may also be critical for physical health.
Conclusions
The current study highlights the possibility that aerobic fitness may be protective against functional impairments among young children with heightened levels of HI symptoms, who may be particularly vulnerable to academic impairments. We hope these findings will set the stage for future research, given our study’s correlational and preliminary nature. Specifically, understanding why aerobic fitness influences the associations between HI symptom severity and academic functioning is an important next step toward informing ADHD interventions. Furthermore, longitudinal studies exploring the potential benefits of aerobic fitness on academic functioning in clinical samples of children with ADHD are needed. Ultimately, such studies will strengthen our knowledge of the potential utility of promoting aerobic fitness as an academic improvement strategy and an adjunct to treatment for children diagnosed with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported primarily by grant number R01MH082893 from the National Institute of Mental Health to Betsy Hoza and John T. Green. This research was supported in part by the United States Health and Human Services (USHHS), Administration on Developmental Disabilities (ADD), grant award 90DD0645, to the Center on Disability and Community Inclusion, University of Vermont. The views expressed in this article are solely those of the authors and do not necessarily reflect the views of the National Institute of Mental Health, the USHHS, or the ADD, and no official endorsement should be inferred.