
Abstract
Vaccination day plays a pivotal role in India’s strategy to reduce maternal and child mortality, yet the cognitive and emotional demands placed on Accredited Social Health Activist (ASHA) workers during these sessions remain insufficiently understood. This qualitative study examines the cognitive workload ASHAs encounter in rural immunization settings. Findings reveal that workers operate within an overloaded ecosystem marked by rapid task switching, fragmented documentation, digital unreliability, and decision-making under uncertainty. Drawing on cognitive ergonomics, we propose design interventions aimed at reducing strain and improving workflow reliability. Through a human-centered design (HCD) lens, these insights translate into context-sensitive solutions that support the cognitive and emotional well-being of frontline health workers.
Keywords
Across India’s rural health landscape, vaccination booths serve as critical points of maternal and child health (MCH) care, protecting against preventable diseases. At the center of these efforts are Accredited Social Health Activists (ASHAs), female community health workers (CHWs) appointed under the National Rural Health Mission (NRHM) to serve as the primary link between rural households and the public health system. Their responsibilities span community mobilization, record maintenance, antenatal care (ANC) coordination, accompaniment of pregnant women to facilities, and facilitating immunization services (Patel & Tandon, 2025b). On vaccination days, these responsibilities intensify. ASHAs must simultaneously call beneficiaries, manage queues, update both paper and digital records, support the Auxiliary Nurse Midwives (ANM), and respond to real-time questions from caregivers. These activities unfold rapidly and are frequently complicated by infrastructural limitations, stretching workers’ physical stamina and cognitive capacity. Despite their central role in preventing maternal and child deaths, the cognitive and emotional workloads (C&EW) that ASHAs shoulder during vaccination sessions remain largely unexamined. As immunization programs increasingly depend on their performance, addressing these hidden workloads becomes essential for sustaining high-quality, last-mile healthcare delivery.
THE HUMAN FACTORS BEHIND VACCINATION DAY: CONTEXT OF THE WORK
In India’s rural healthcare system, ASHAs are central to the reach and effectiveness of MCH interventions. Since their introduction under the NRHM in 2005, they have contributed significantly to increasing institutional deliveries, improving family planning uptake, and enhancing maternal and childhood immunization coverage (Ministry of Health and Family Welfare, 2005; Patel & Tandon, 2025a). Vaccination days represent particularly critical points of service, with direct implications for reducing preventable maternal and child deaths (Burger et al., 2022).
Despite improvements in health indicators over the past two decades, maternal and child mortality rates in India remain disproportionately high in rural and underserved regions. According to the Sample Registration System (SRS) statistical report 2020, India’s Maternal Mortality Ratio (MMR) is 97 per 100,000 live births, while the Under-Five Mortality Rate (U5MR) stands at 32 per 1000 live births, with significantly higher rates in rural districts (PIB, 2023). Many of these deaths are preventable with timely immunization, improved ANC, and early treatment for common infections (Finlayson & Downe, 2013). Routine and campaign-based immunization programs, including Mission Indradhanush, protect children from measles, diphtheria, and tetanus, while pregnant women receive critical immunizations that support maternal and neonatal health (Dhawan et al., 2023; PIB, 2024).
The sustainability of these public health gains requires more than adequate vaccine supply and sound program design; it depends fundamentally on the capacity of CHWs to deliver services effectively. Understanding ASHAs’ workload is therefore essential for ensuring consistent and equitable immunization coverage and for safeguarding their well-being. The heightened workforce-to-population demands on vaccination days add significant layers of strain (Kaur et al., 2022; Nair et al., 2021), and excessive workload has been shown to weaken service quality and reduce caregiver trust (Das & Dasgupta, 2015; Manjunath et al., 2022; Meena et al., 2020; Pandey, 2023). Vaccination days create uniquely intense working conditions within a compressed, high-pressure window. Recognizing this concentrated workload is critical, as any strain on ASHAs’ performance directly affects both service quality and the overall success of immunization programs.
The workload of CHWs is shaped by two major dimensions: cognitive and emotional workload (C&EW). Cognitive workload includes attention, memory, multitasking, and real-time decision-making, demands that intensify during eligibility verification, documentation, and caregiver communication (Lieu et al., 2021). Emotional workload involves empathy regulation, responding to caregiver anxiety, addressing mistrust, and managing interpersonal conflict in fast-paced settings. Although these dimensions are recognized globally, few studies examine how they interact during India’s vaccination sessions (Rasid et al., 2025; Szulewski et al., 2021).
Existing research on ASHAs has primarily examined their general responsibilities, the adoption of digital tools, or their role in MCH counseling, with limited attention to the specific C&EW they encounter during immunization work. Although studies have documented task fragmentation, multitasking, and administrative burden among community health workers (Aron et al., 2023; Khandre et al., 2023; Kaur et al., 2022), they rarely investigate how these challenges intensify during tightly scheduled vaccination sessions where tasks must be completed rapidly and in parallel. Prior research focusing on the importance of vaccination, maternal mortality, and related public health outcomes has provided valuable epidemiological insights but has not addressed the micro-level processes that shape CHWs’ experience during vaccination delivery. Studies on immunization programs in India and other LMICs highlight issues such as misinformation, caregiver hesitancy, and interpersonal conflict (Ks et al., 2025; Sauseriene et al., 2024; Di Prinzio et al., 2024), yet they do not connect these emotional stressors to the concurrent cognitive overload that ASHAs must manage. Likewise, cognitive ergonomics research identifies memory load, decision pressure, and task switching as key determinants of mental workload in healthcare settings (Li-Wang et al., 2023; Valdez & Holden, 2016), but these frameworks have rarely been applied to community-based workers who operate in resource-constrained rural environments.
This leaves a clear gap: the underlying cognitive and emotional processes that make vaccination days uniquely demanding for ASHA workers remain largely invisible in existing literature. Most scholarship focuses on outcomes, such as immunization rates or community awareness, rather than on the lived workload that enables those outcomes. Research on CHW burnout, task-shifting, and workload management (Aviraj et al., 2025; Hosseini et al., 2019; Joukes et al., 2018; Shrivastava et al., 2023; Smith et al., 2014) similarly overlooks how vaccination-day pressures arise not from worker inadequacy but from the design of tasks, tools, and environments. Addressing this gap is essential because without understanding the moment-to-moment cognitive effort and emotional regulation required during vaccination sessions, system-level interventions risk being misaligned with frontline realities.
Cognitive ergonomics provides a structured lens for uncovering these hidden demands by examining the mental effort, decision complexity, and attention strain embedded in vaccination-day workflows. Human-Centered Design (HCD) complements this by translating ergonomic insights into grounded, context-appropriate improvements, ranging from streamlined documentation systems and more supportive digital interfaces to micro-environmental modifications that better match ASHAs’ lived working conditions. Together, these perspectives underscore the need for a study that not only identifies the nature of ASHAs’ workload but also informs design strategies capable of reducing strain and strengthening immunization service delivery.
MOTIVATION
Understanding ASHAs’ dual workload is essential because it directly affects both service quality and worker well-being. Examining their challenges in detail allows for the design of tools and workflows that align with the realities of their work, rather than imposing external expectations that may inadvertently increase workload. Such grounded insights support ergonomic interventions that improve the vaccination experience for both workers and beneficiaries.
AIM OF THE STUDY
This study examines the C&EW experienced by ASHA workers during rural vaccination drives in India. It aims to make visible the mental effort, decision-making demands, and emotional regulation required during immunization service delivery. By applying cognitive ergonomics and HCD, the study identifies context-specific, field-grounded solutions that can support ASHAs’ well-being, reduce workload, and enhance the reliability of vaccination workflows.
INSIDE THE VACCINATION DAY: OUR FIELDWORK JOURNEY
Information on ASHA workers’ vaccination day experiences was gathered through direct field observations, informal interviews, and workshop (Shrivastava et al., 2023; Sialubanje et al., 2014). The study was conducted in one administrative block of Jabalpur district, Madhya Pradesh, a predominantly rural area characterized by limited health infrastructure and diverse community health needs. The focus was on understanding the experiences of ASHA workers during both routine and campaign-based immunization drives, as shown in Figure 1. Activities performed by ASHA workers during vaccination days: (a) Explaining the documentation process, (b) updating the documents (paper and digital), (c) ASHA workers discussing doubts with ANM, (d) information documentation and retrieval, (e) inspection by medical officer, (f) rush time, and (g) updating the MCP card.
In this study, routine workdays were also analyzed using the same qualitative methods to establish a qualitative baseline for comparing C&EW between routine and vaccination contexts. This baseline enabled assessment of whether and how workload-related task demands increased during vaccination days. Routine workdays refer specifically to ASHA workers’ regular community-based activities, including home visits, follow-ups, and village-level outreach. Routine workdays do not include hospital reporting days, emergency response situations, or special campaign activities.
Participants
The investigation employed the multistage sampling design recommended by the National Health Systems Resource Center (NHSRC), New Delhi, to evaluate the ASHA program in India. Twenty Anganwadi centers (AWCs) and sub-health centers (SHCs) were randomly selected across the block, which were selected through purposive sampling, according to the MMR, transport issues, and reliability on ASHA workers in the area (Patel & Tandon, 2025a), from where sixteen ASHA workers were included through random sampling. There were no specific exclusion criteria; all ASHA workers who were present and willing to participate on the vaccination days were included. All had prior involvement in both routine immunization services and national campaigns such as Mission Indradhanush. Participants ranged in age from 28 to 46 years and had 5–10 years of experience, with a mean age of 40 years. Most of them (12) were educated up to 8th and 10th grades, living in a semi-pucca house in joint family, and the population covered in the range of 800–1500.
Data Collection Procedures
For both routine workdays and vaccination days, the researcher conducted field observations using an observation sheet (refer to Appendix A) at selected Anganwadi villages or vaccination booths. These structured observations also focused on understanding the sequence of tasks performed by ASHAs, the physical setup of the vaccination site, interactions with other health staff and community members, and any visible challenges such as crowding, digital disruptions, or counseling (see Figure 2). Task flow of ASHA workers on vaccination days.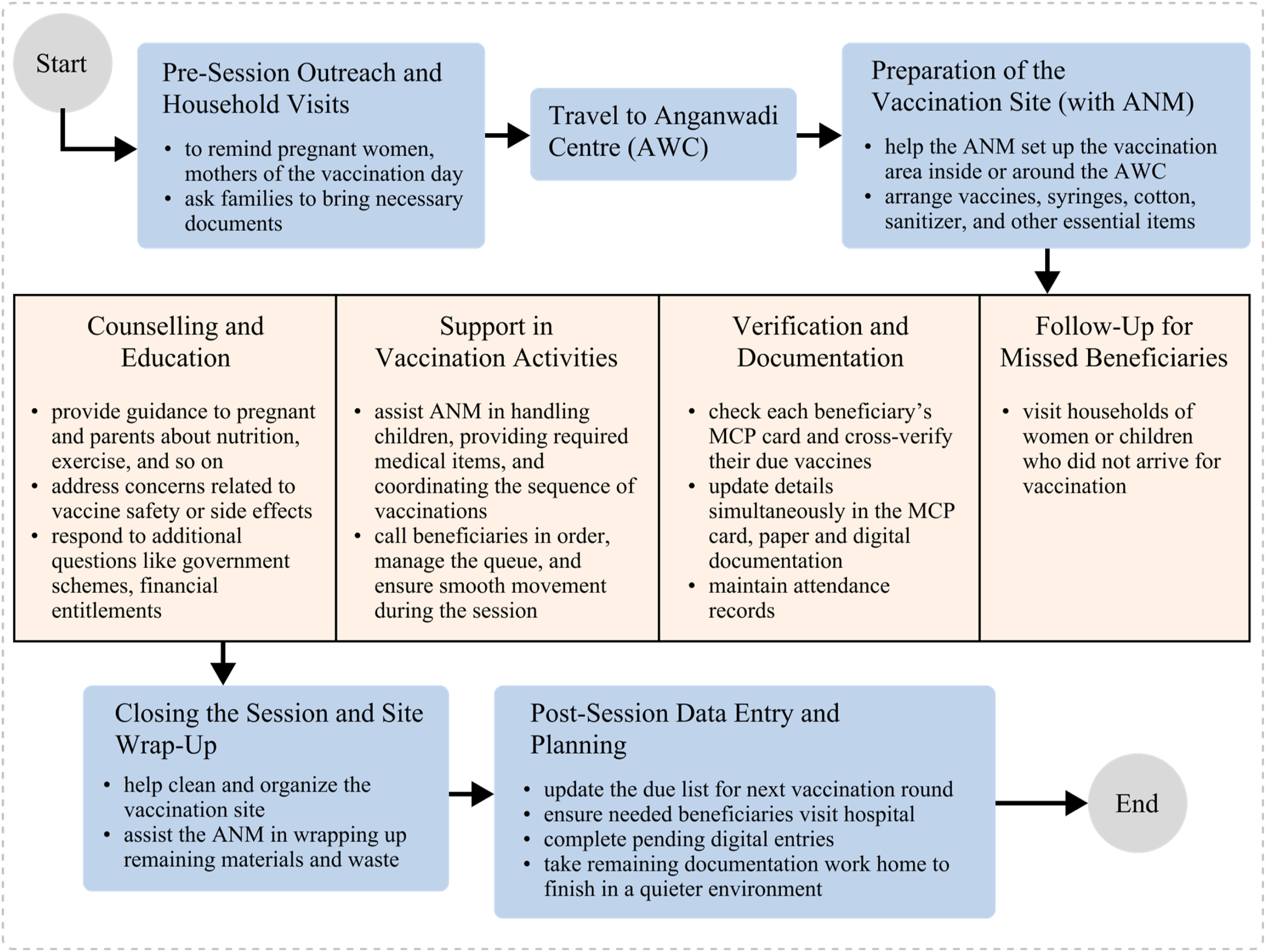
Observational field notes were documented through written diary entries, photographs, or audio notes, depending on participant comfort and situational appropriateness, consistent with established human factors approaches to field observation and task analysis (Meena et al., 2020; Stanton et al., 2013).
Informal interviews were conducted between the duty and after the vaccination event, according to the ASHAs’ availability and preference. These were conducted in Hindi or the local language by a female researcher fluent in the local dialect, which helped establish rapport and openness. Each interview lasted between 15 and 25 min, either continuously or in discrete segments. Followed a semi-structured guide that explored topics from their daily task flow (see Figure 2), such as documentation practices, counseling, and so on, for emotional and workload challenges. Informed verbal consent was obtained from all participants, and interviews were noted or audio-recorded with their permission. All the transcribed verbatim received in Hindi was translated into English to ease the analysis process. The complete interview guide is presented in Appendix B (Patel & Tandon, 2025a). In addition, an informal, small-group workshop involving four ASHA workers was conducted at the AWC, a familiar setting chosen to support participant comfort and open discussion. It is consistent with participatory and human-centered qualitative research approaches (Sanders & Stappers, 2008).
Field observations, informal interview, and workshop data were triangulated throughout analysis. Observational notes on task flow, interruptions, time pressure, documentation behavior, community interactions, and environmental constraints were used to refine interview and workshop prompts, verify reported experiences, and strengthen the reliability of emerging themes. This approach is consistent with healthcare research that applies qualitative methods, especially structured observation and interviews, to analyze cognitive demands and workflow characteristics in naturalistic clinical environments (Graham et al., 2022; Shan et al., 2023).
Cognitive and Emotional Constructs
To systematically identify C&EW in the ASHA workflow on vaccination days, the cognitive workload constructs include task switching, multimodal documentation, information recall under time pressure, error, memory load, attention demand, and real-time decision making (Salvendy, 2012; Wickens, 2002). The emotional workload constructs include empathy management, frustration, stress, fatigue, conflict negotiation, and physical and emotional exhaustion, as detailed in Appendix C (Glomb & Tews, 2004; Jeung et al., 2018).
Data Analysis Process
A thematic analysis approach was used, with codes developed inductively from the data collected. The coding process was iterative: initial open codes were progressively refined into broader categories aligned with the C&EW constructs. We examined both cognitive and emotional components separately to maintain conceptual clarity for tasks done by ASHA workers on routine workdays and vaccination days. Workload levels were rated using a three-point Likert scale (low, medium, and high) to clearly differentiate task demands. Themes were validated through repeated comparison across data sources, and representative quotations were selected to illustrate key insights. This process strengthened the rigor of the analysis and enhanced the overall validity of the findings. A detailed thematic table is provided in Appendix C.
Ethical Consideration
Ethical approval for the study was granted by the Ethical Committee of PDPM Indian Institute of Information Technology, Design and Manufacturing, Jabalpur, Madhya Pradesh. All ASHA workers were informed about the nature and importance of the study and took consent before performing research.
FINDINGS: COGNITIVE AND EMOTIONAL DEMANDS ON VACCINATION DAY
Vaccination days created an environment marked by cognitive congestion, rapid task switching, and emotional unpredictability. Appendix D clearly stated that vaccination days demand more C&EW to ASHA workers. Eight themes emerged that illustrate how ASHAs navigate a dense set of responsibilities under constrained conditions tabulated in Appendix C.
The first theme concerns the management of concurrent and overlapping responsibilities. ASHAs were required to coordinate crowd movement, verify eligibility, update multiple documents, respond to community queries, and support the ANM, often within the same moment. Participants described the session as one in which “everything happens together,” leaving little cognitive space for prioritization, planning, or reorientation. This simultaneity produced sustained attention demands and greatly increased the risk of omissions or misentries.
Multimodal documentation formed the second theme. Workers updated information across the MCP card, the ASHA diary or self-maintained registers, and digital systems such as the UWIN application. They frequently switched between these formats while managing beneficiary flow. Many expressed fear of making mistakes because supervisory audits could highlight discrepancies. Digital interruptions added further complexity, as app crashes or poor connectivity disrupted workers’ mental tracking of which beneficiaries had been recorded. These factors produced high memory load, increased error potential, and persistent anxiety about correctness.
A third theme emerged around continuity of care. Vaccination day responsibilities extended beyond the booth, as ASHAs were expected to visit homes of absentees, sometimes repeatedly, to ensure complete coverage. Supervisory checks reinforced this expectation. These follow-up tasks added additional cognitive demands, such as remembering households, tracking absentees, and planning routes and created emotional pressure due to the fear of being questioned if beneficiaries remained unvaccinated.
Community interaction constituted another major theme. ASHAs frequently provided health education and explained vaccine benefits, side effects, and post-care instructions. These conversations required real-time recall of medical information and adaptation of messages to caregivers with varying literacy levels. Because they occurred amid noise, crowding, and administrative duties, the cognitive effort involved was substantial. Workers simultaneously managed emotional labor, as they were expected to remain composed, reassuring, and respectful regardless of the caregiver’s attitude.
Emotional labor intensified further during episodes of mistrust or conflict. Some workers reported being accused of acting out of financial motives or being questioned aggressively about delays or side effects. Although these encounters were emotionally charged, ASHAs were expected to de-escalate tensions, maintain composure, and continue persuading families to vaccinate their children. Such situations required significant emotional regulation and personal resilience.
The sixth theme highlighted ASHAs’ informal role as system navigators. Caregivers frequently approached them with questions about government schemes such as Ayushman Bharat, Samagra ID, or Aadhaar-linked financial processes. Responding to these queries required instant recall of procedures, eligibility criteria, and bureaucratic steps. Although not part of their formal vaccination duties, these inquiries increased cognitive load and occasionally displaced attention from core tasks.
Environmental and contextual stressors formed the seventh theme. Workers faced poor lighting, a lack of seating, weather challenges, noise, congestion, and occasional supply delays. These conditions interfered with documentation accuracy, attention stability, and the ability to focus during interactions with caregivers. Physical discomfort often compounds cognitive fatigue.
Finally, ASHAs reported substantial physical and emotional exhaustion by the end of the day. Prolonged standing, repeated calling of names, crowd management, continuous documentation, and extended emotional engagement produced both bodily discomfort and mental fatigue. Many described a “heavy head” or body ache and skipping the household chores following each vaccination session, reflecting the cumulative effect of sustained multitasking and emotional labor.
DISCUSSION
The findings demonstrate that vaccination days constitute a cognitively and emotionally intense microenvironment that differs significantly from ASHAs’ routine workdays (see Appendix D). Routine tasks such as household visits and counseling sessions are spread throughout the day, providing opportunities to pace attention and emotional engagement. In contrast, vaccination days compress numerous responsibilities, mobilization, verification, documentation, digital entry, counseling, and conflict management, into a short and inflexible timeframe (Aviraj et al., 2025; Ks et al., 2025). This creates a high-density workload that taxes attention, memory, and decision-making continuously. Emotional pressure also increases when workers deal with hesitant caregivers or interpersonal conflicts in crowded and time-sensitive settings.
Cognitive ergonomics helps clarify why vaccination sessions are particularly demanding. The rapid succession of tasks generates frequent attention shifts, each associated with cognitive costs. Memory load increases as ASHAs track beneficiaries across paper and digital platforms while simultaneously responding to queries. System unreliability disrupts cognitive continuity, causing workers to lose track of tasks, checklists, or digital entries. Environmental noise and physical discomfort further reduce cognitive capacity.
HCD offers a pathway for addressing these demands by translating ergonomic insights into practical improvements. Rather than imposing new tools or expectations, design interventions must align with the realities of ASHA workflows, physical environments, and emotional contexts. Together, cognitive ergonomics and HCD illuminate how system redesign, whether digital, organizational, or environmental, can support ASHAs’ performance and well-being.
IMPLICATIONS FOR DESIGN AND SYSTEM IMPROVEMENT
The findings point to several opportunities for improving vaccination-day workflow. Reducing redundancy in documentation could significantly ease mental load; consolidating MCP, diary, and digital entries into a unified system would minimize the need for repeated information retrieval and cross-checking. Similarly, digital tools that operate reliably in low-connectivity environments would help prevent cognitive disruption caused by app crashes or delays. Incorporating offline-first design, autosave features, and simplified interfaces could reduce workers’ need to reorient themselves after interruptions.
Environmental enhancements may also reduce C&EW. Stable seating, adequate lighting, designated documentation spaces, and clearer queue arrangements would help ASHAs maintain focus. Additionally, tools that support health communication, such as visual cue cards or structured scripts, could relieve memory load during counseling. Training in emotional regulation or conflict management may also help workers navigate stressful interpersonal encounters more effectively.
Finally, system-level processes should recognize follow-up visits and system-navigation tasks as legitimate components of ASHAs’ workload. Designing schedules, incentives, and tools that account for these hidden responsibilities could create a more supportive work environment overall.
CONCLUSIONS
ASHA workers shoulder the intertwined demands of manual labor, administrative responsibility, emotional regulation, and system navigation during vaccination sessions. These demands intensify due to environmental constraints, redundancy in documentation, digital unreliability, and socially sensitive interactions. Understanding vaccination-day experiences through the combined perspectives of cognitive ergonomics and HCD makes visible the hidden forms of mental and emotional labor that are critical to public health delivery. Improving tools, workflows, and environments in alignment with ASHAs’ lived context can reduce C&EW, strengthen service reliability, and enhance worker well-being. Supporting ASHAs through thoughtful design is essential to achieving sustainable and equitable MCH outcomes.
LIMITATIONS
The study was conducted in a single rural block within one district, and the findings reflect the sociocultural and infrastructural characteristics of that specific context. This study solely relies on the qualitative method rather than quantitative estimates of workload. The quantitative and cross-regional research would help validate and extend the applicability of the recommendations presented here.
Supplemental Material
Supplemental Material - Designing for Cognitive Relief: Qualitative Study of ASHA Workers During Rural Vaccination Drives in India
Supplemental Material for Designing for Cognitive Relief: Qualitative Study of ASHA Workers During Rural Vaccination Drives in India by Sakshi Patel and Puneet Tandon in Ergonomics in Design.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
![]()
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.