
Abstract
How best to govern reproduction is the subject of heated controversies and policies on abortion and reproductive technologies present strong variations. Through fuzzy-set qualitative comparative analysis, the article explores the interplay of institutional settings, Christian Democratic politics, women’s movement, and Christian opposition in France and Switzerland since the 1970s. If little evidence is found for any institutional impact on policies regarding abortion and reproductive technologies, the analysis confirms the growing influence of the medical profession over reproductive issues and shows that the success of the women’s movement has been fluctuating while prolife opposition seems to have gradually lost influence.
Keywords
How best to govern the field of reproduction has launched heated controversies for the past decades, and policy makers in Western countries have grappled with highly polarizing issues regarding abortion and assisted reproductive technologies (ARTs). The feminist movement defines procreation in terms of women’s right to choose and calls into question the social obligation of mothering, while the prolife opposition argues in favor the protection of human embryo. Launched by the feminist claims for liberalizing abortion in the 1960s, the controversy has more recently been fueled and redimensioned by the development of the new reproductive technologies. The invention of in vitro fertilization in 1978 has indeed offered more than medical treatment for sterility and has unsettled the traditional family scheme by providing gay couples (Bryld 2001) with access to reproduction.
Most West European countries have been confronted with similar reproductive issues. Nevertheless, policies on abortion and ART present strong variations, both in terms of regulatory scope and content as well as in terms of the policy-making process (Engeli 2009a; Bleiklie, Goggin, and Rothmayr 2004; Stetson 2001). The literature has developed three main explanations for the variations in the regulation of the field of reproduction, which are, respectively, centered on institutional arrangements, on the party system and the presence of strong Christian Democrats, and on the strength of the medical community and women’s movements (Bleiklie, Goggin, and Rothmayr 2004; Stetson 2001). Indeed several studies addressing either the issue of abortion or the ART one have emphasized the high complexity in regulating the field of reproduction and stressed the interplay of explanatory factors that vary across countries and time (e.g., Latham 2002; Mazur 2002; Outshoorn 1996; Stetson 2001; Varone, Rothmayr, and Montpetit 2006). The question remains to account for the full set of variations across the regulation on abortion and ART. To do so, this article aims at further developing the shift from mono-causal to configuring thinking (Ragin 2008) and to take into account the whole spectrum of policy preferences involved in the regulation of the field of reproduction by examining the policies on abortion and ART in France and Switzerland since the 1970s. Faced with multidimensional policy differences, the analysis of policies on abortion and ART pleads for examining the phenomenon of multicausality through fuzzy-set qualitative comparative analysis (Fs/QCA). The configurational comparative method aims at assessing the multicausal nature of social phenomena by revealing how different causal processes may produce similar results.
The article is organized as follows. The first section reviews the main explanations presented in the literature and develops seven hypotheses related to the impact of institutional settings, the configuration of the party system, and the policy preferences of main actors in the field, that is, the medical community, women’s movements, and the prolife movement. The second section discusses the advantages of using Fs/QCA to better apprehend the complexity in regulating abortion and ART and presents the operationalization of the variables and data used in the analysis. The third section discusses the analysis of the policies on abortion and ART in France and Switzerland since the 1970s and shows that even if little evidence is found for a systematic and independent institutional impact on policies regarding abortion and reproductive technologies, the analysis confirms the growing influence of the medical profession over reproductive issues and shows that, on the contrary, the success of the women’s movement has been more fluctuating while the prolife opposition seems to have gradually lost influence on the abortion issue.
Explaining the Complexity in Regulating Abortion and ART: Institutions, Politics, and Policy Networks
Policy making in the reproduction field comprises complex phenomena in which various factors interact. The literature offers three main explanations for the variations in the regulation, which are, respectively, focused on institutional arrangements, on party system and politics, and on the strength of the medical community and women’s movements (Bleiklie, Goggin, and Rothmayr 2004; Stetson 2001). Drawing on the literature, this section develops seven hypotheses to explain divergence among countries and sectors, regarding (1) institutional arrangements and (2) the path-dependency effect, (3–4) politics and the party system, and policy networks composed of (5) the medical community, (6) women’s movements, and (7) the prolife movement.
Institutional Arrangements
Among the explanatory factors of reproductive policies, the effect of institutional factors has been the one most thoroughly assessed. Most comparative research tends to conclude that institutional settings per se do not exert any independent influence on policy content and thus cannot, in isolation at least, account for variations in reproductive policies (Bleiklie, Goggin, and Rothmayr 2004; Engeli 2009a; Stetson 2001; Rothmayr et al. 2004). Rothmayr et al. (2004; also see Stetson 2001) do not identify any systematic patterns in the impact of institutional settings according to the classical typologies of political systems (consensus vs. majoritarian democracies, federalist vs. unitary systems, parliamentary vs. presidential systems). However, institutional factors may exert an indirect impact on the regulation of reproduction. Drawing on Timmermans’s (2001) argument, greater institutional opportunities may enhance the involvement of various actors with competing interests that, in turn, will lead to different policy content than in the case of a lower number policy arena dominated by one major actor (Engeli 2010; Varone, Rothmayr, and Montpetit 2006).
In addition, previous decisions may well exert a well-known effect of path dependency (Pierson 2000), in which posterior decisions follow the trajectory of the initial ones. According to Mooney (2001, 675), policies with a moral dimension “are not less than the legal sanction of what is right and wrong, the validation of a particular set of fundamental values.” Indeed, the discussion of moral values and social norms implied by the regulation of ART and abortion often occurs within a context of high politics that appeals to a broad and polarized audience (Green-Pedersen 2007). It could be thus easier and electorally less costly for governments to stick with prior decisions than to drive major policy change that could lead to clash of absolutes across the electorate (Tribe 1990).
Taken together, these literatures on reproductive policies suggest two hypotheses about the impact of institutional arrangements on the regulation in the field of reproduction. A higher level of institutional access should favor the elaboration of restrictive policies by allowing for a greater number of policy actors promoting restrictive preferences, as argued by Varone, Rothmayr, and Montpetit (2006; Hypothesis 1). On the contrary, the output of the policy-making process should be positively influenced by any prior liberal policy in the field (Hypothesis 2).
Politics and the Configuration of the Party System
Pointing out that reproductive issues have a moral dimension, some scholars argue that the presence of Christian Democrats may well lead to more restrictive policies in the reproduction field, while the presence of strong Social Democrats is often shown as a potential alliance partner for women’s movement and their claims in the reproductive field (Fink 2009; Minkenberg 2002). On the contrary, other scholars argue that political parties prefer to stay out of heated debate on reproductive issues as they may lead to internal division and serious electoral loss (Blofield 2006; Burns 2005; Rothmayr et al. 2004). Accordingly, the strong presence of Christian Democrats should prevent the elaboration of permissive policies (Hypothesis 3), while Social Democrats government should lead to the promotion of a liberal regulatory regime in the field of reproduction (Hypothesis 4).
Policy Networks
As controversies regarding reproduction cut across the classic right–left political conflict (Burns 2005), the explanation of the variations in governing abortion and ART may instead rely on the configuration of the policy preferences supported by the medical profession, women’s movements, and prolife opposition. The capacity of women’s movements to drive the liberalization of abortion in Western countries remains a contested issue (Stetson 2001; Yishai 1993). In her comparative study of women’s movements influence on abortion politics, Stetson (2001) shows that internal cohesion among women’s movements and the support of powerful women state agencies constitute key factors to obtain substantial policy gains. In addition, several studies also emphasize the powerful interests within the medical community (Latham 2002; Sheldon 1997; Stetson 1996). Monopoly over abortion represents an important professional issue for the medical community. The claim for monopoly over abortion in the nineteenth century was part of physicians’ global strategy to further ensure the professionalization of medicine and to secure their preeminence over midwives (Mohr 1978).
Comparative studies on ART policy mostly concentrate on the regulation of the autonomy granted to the medical community and not much is known about the impact of women’s movements and the prolife movement (Latham 2002). Indeed, Montpetit et al. (2005) show that physicians’ pivotal position in the ART sector relies on their social prestige and professional authority. Nevertheless, as feminist scholars emphasize, governing ART also means deciding whether same-sex couples and singles may access parenthood (Bryld 2001). As a result, governing ART addresses the definition of gender roles as much as the abortion issue did: heterosexual intercourse is not the only path to reproduction anymore, and the traditional heterosexual family does not constitute the sole family scheme available. Women’s movements and prolife groups have felt concerned by the ART issue and mobilized important resources to promote their policy preferences. Accordingly, following Stetson (1996), the whole configuration of actors’ preferences should be analyzed to better explain the variations in the policies on abortion and ART. To do so, three separate hypotheses are formulated for each of these sets of actors: the medical community and the women’s movement should promote permissive policies in the field of reproduction (Hypotheses 5 and 6), while prolife actors should oppose any liberalizing attempt in the field (Hypothesis 7).
While the different explanations regarding the regulation of the field of reproduction have been discussed separately, it is important to stress that recent research goes beyond mono-causal thinking to emphasize the complexity of the regulation. As Varone, Rothmayr, and Montpetit (2006) argues, the multidimensionality of the variations across policies in the field of reproduction makes the explanation complex, and focusing solely on a single type of factors would overall fail to shed light on the puzzling patterns at stake. Several studies indeed demonstrate the high complexity of reproductive regulation and emphasize the interplay of explanatory factors that vary across issues and countries but also across time (e.g., Githens and Stetson 1996; Latham 2002; Mazur 2002; Outshoorn 1996; Stetson 1986, 2001; Varone, Rothmayr, and Montpetit 2006). This analytical complexity, strongly emphasized in the literature, pleads for further developing the shift from mono-causal to configuring thinking and assessing how the different explanatory factors interact in the regulation of the reproduction field. The following section first discusses the case selection and then develops how configurational comparative methods, here Fs/QCA, allow for apprehending the multicausal nature of social phenomena by examining how different causal mechanism may result in similar outcomes.
Method and Data
Case Selection
To assess the causal complexity of regulation in the reproduction field, I select two countries, France and Switzerland, as well as two policy areas, abortion and ART. The selection criteria were driven by the strategy of the compound research design recently proposed by Levi-Faur (2006) to maximize the explanatory capacity of comparative policy analysis. Based on a combination of case selection methods according to the “most different systems” and the “most similar systems,” this strategy allows for increasing the number of cases by varying the levels of analysis (thus, levels of control) in a systematic way. Starting from the observation that there are four main levels of comparison in public policy analysis—national, sectoral, international, and across time—Levi-Faur proposes to select cases that vary on at least two of these levels. The aim is to systematically test hypotheses across levels in an iterative way. The richness of qualitative analysis is preserved, while, at the same time, the capacity for generalization is strengthened.
Accordingly, I selected cases that enable triple contrasts: across countries (Switzerland and France), across sectors (abortion and ART), and across time (from the rise of the second wave of the women’s movement at the end of the 1960s to 2007). At the country level, France is a paradigmatic case of a strong state with a highly centralized decision capacity, while the Swiss political system is more open to social and political demands through its power-sharing structure fostered by federalism and direct democracy. Regarding the sectoral logic, as abortion and ART are both part of the field of reproduction, the regulation could be similar within the field. Nevertheless, government response to reproductive issues does not seem to follow patterns according to sector. The autonomy of the medical community in the ART field is strongly restricted in Switzerland, while it is regulated more permissively in France. Finally, in respect to the evolution of the regulation, the various dimensions of the policy decisions do not systematically follow a similar regulatory pattern. For example, even if the medical community’s autonomy to practice ART is very permissively regulated in France, patients’ access is, on the contrary, restricted to opposite-sex couples only.
Fs/QCA and Multicausality
Governing the reproduction field follows complex patterns of regulation that do not tend to be easily explained by a sole factor, taken separately. As emphasized in the first section, solely focusing on either institutional logic or sectoral logic of regulation would fail to fully explain the multidimensionality in reproductive policies (Engeli 2010; Varone, Rothmayr, and Montpetit 2006). Configurational comparative methods, particularly Fs/QCA, represent adequate tools to better apprehend the complexity of regulating the field of reproduction. Instead of looking for mono-causality or causality in isolation, it allows for identifying, in a systematic way, the configurational impact of various factors and assessing phenomenon of multicausality (Ragin 2000, 2008).
Fs/QCA aims at benefitting simultaneously from the complexity stemming from each qualitative case while helping to identify causal processes that could enhance middle-range generalization. First, Fs/QCA strengthens the explanatory potential of qualitative comparison. It systematizes the empirical test and points to contradictions in the empirical evidence and misspecifications in the explanatory model. Second, it is one of the most formalized tools available to analyze equifinality and causal complexity on the basis of qualitative cases. If a great deal of attention is given to the most important causal paths, those that cover fewer cases are not left out of the explanation. In this sense, Fs/QCA helps to preserve the richness of qualitative comparative studies while helping to draw causal interpretation (Ragin 2008). Finally, Fs/QCA allows for a fine-grained measurement of the dependant variable, the outcome in QCA terminology. In contrast to the classic crisp-set QCA, Fs/QCA introduces multiple value variables, the fuzzy set, which helps to capture more nuanced variation in the observed phenomenon to be explained. Instead of dichotomizing the set into two categories of “in” or “out,” a fuzzy set allows for partial membership of cases in the interval of 0 (nonmembership) and 1 (full membership). With crisp-set analysis, the policies would have been considered as either fully permissive or fully restrictive, which would not adequately reflect the complexity of the evolution of the regulation. Indeed, most regulations analyzed here neither grant full permissiveness nor ban abortion and ART. The following section first presents the operationalization of the dependent variable, the outcome in QCA terms, and then describes the diverging pattern in the trajectory of the regulation of abortion and ART.
Outcome: The Three Dimensions of Abortion and ART
Governing reproduction addresses three main questions: How broad will medical autonomy to practice abortion and ART be? Who will have access to abortion or ART treatment? To what extent should the state guarantee access to treatments? Each policy decision represents a particular combination of these three regulatory dimensions, which shift in terms of policy permissiveness: (1) the medical autonomy granted to practice abortion and ART, (2) the restrictions imposed on patients’ access to treatment, and (3) the availability of health care coverage for reproduction-related treatment and state guarantee of abortion provision. 1 As the degree of permissiveness in the regulation of these three policy dimensions may greatly vary, each policy dimension per decision will constitute an observation in the Fs/QCA analysis. For example, the same ART policy could permissively regulate a physician’s autonomy to practice, but at the same time, it could also exclude single women and same-sex couples from access to ART treatments. Along the same lines, broad legal access to abortion would be, de facto, drastically reduced in the case of absence of financial coverage for the treatments. The three policy dimensions are first described substantially, and their fuzzy set calibration, as shown in Table 1, is then explained.
Membership in Fuzzy-Set “Permissive Policies”

Note: IVF = in vitro fertilization; ICSI = intra-cytoplasmic sperm injection; PGD = preimplantation genetic diagnosis.
Calibration: index range (0–0.49) = 0, range (0.5–0.99) = 0.2, range (1–1.499) = 0.4, range (1.5–1.99) = 0.6, range (2–2.49) = 0.8, range (2.5–3) = 1.
Index: Σ (score indic.)/N(indic.).
Medical Autonomy
ART development opens up promising avenues of medical and science research, such as sterility treatment, genetic engineering, and stem cell research. The medical community therefore constitutes a powerful policy target group. Following Bleiklie, Goggin, and Rothmayr (2004), the dimension of medical autonomy is conceptualized as the degree of autonomy granted to the medical community to decide on both the selection of reproductive techniques to be used and the conditions for resorting to these techniques. To best capture policy change in the field, the level of medical autonomy is measured at each policy decision time point through a two-step coding procedure. 2 First, as the “indicator” column in Table 1 indicates, each medical technique is coded as permissively regulated (score = 3 in Table 1, “indicator score” column) if its use is under general permission that can be conditioned by a licensing procedure but is not subject to any substantial restriction or is not regulated at all. The regulation is qualified as restrictive (score = 0) if it is under a general ban, while the regulation is considered as intermediate if the use of the technique is seriously constrained by severe restrictions (score = 1) or delimited by some lighter restrictions (score = 2). The indicator scores are then built into an additive index (“index score” column in Table 1). 3 Second, the index scores are calibrated into a six-value fuzzy set for the Fs/QCA analysis, going from 0 (no membership in the “permissive policies” set) to 1 (full membership in the “permissive policies” set). 4 In other words, as presented in the “fuzzy set” column in Table 1, when the medical community is granted with broad autonomy, this first series of outcomes takes high fuzzy scores. For instance, the score of 1 is assigned to the first French regulation on ART in 1988, which granted full autonomy, while the light constraints imposed in the first Swiss regulation scored 0.8. On the contrary, a low fuzzy score indicates a very limited medical autonomy. The second Swiss regulation on ART is characterized by drastic change in the scope of the medical autonomy. Its score of 0.2 reveals that several ART techniques have been banned while the resort to numerous techniques has been seriously constrained. Scores of 0.4 and 0.6 denote contrasted regulation, the former being still closer to full restrictiveness than the latter (score below 0.5). When looking at the evolution in the regulation of medical autonomy, one observes that if the initial policies granted physicians broad autonomy, the two sectors took diverging paths. If light restriction continues to characterize abortion policies in the two countries, severe constraints were later introduced to ART regulation.
Patients’ Access
The second dimension concentrates on the patients’ access to abortion and ART. Three indicators capture this dimension. In the case of abortion, the first indicator measures whether the access is available on request or can be restricted to grounds regarding serious danger to the woman’s health and life or her socioeconomic conditions. The two other indicators look at whether policies may restrict access according to woman’s age (“under 18” years old indicator in Table 1) and requires going through a dissuasive procedure and a waiting period (“procedure” indicator). In the case of ART, policies may entitle single women, postmenopausal women, and same-sex couples to ART treatments or rather impose strict eligibility criteria relating to civil status and sexual orientation (“civil status”), age (“age”), and medical grounds (“grounds”). As for the dimension of medical autonomy, the coding follows two steps. Each indicator is first evaluated separately and then built into an additive index. The index score is eventually calibrated into a six-value fuzzy set, going from 0 (very restrictive) to 1 (very permissive). As developed above for the regulation of the medical autonomy, fuzzy scores of 1 and 0.8 are assigned to outcomes granting patients with a broad access, while a score of 0.2 denotes highly restricted access to a limited category of patients, opposite-sex couples. As Table 1 shows, the evolution in regulating patients’ access to abortion and ART follows a contrasted pattern across the two policy areas and countries. Women’s access to abortion has been broadened since the first regulation, while patients’ access to ART has been seriously restricted in subsequent regulations in both countries, the policy change being more drastic in the case of Switzerland (falling from 0.6 to 0.2).
Treatment Availability
Feminist research emphasizes that permissive formal access to abortion can be guaranteed only by reimbursement of costs and abortion availability across the country (e.g., Mazur 2002; Yishai 1993). Thus, the last analytical dimension of abortion policies considers three indicators: the level of financial coverage, which can be based on a private insurance system or a national health insurance system, state guarantee of abortion availability across the country, and the existence of some objection clause that allows physicians to refuse practicing abortions (at the individual or unit level). Since state guarantee of availability through provision of sufficient medical coverage and physician objection clause are usually nonexistent for ART treatments, the calibration relies on only the financial coverage indicator. As for the first two dimensions, the additive index is calibrated into a six-value fuzzy set. Looking at the regulatory trajectory of this last set of outcomes displayed in Table 1, the strong variation, once again across policy areas and countries, is striking. On one hand, only at the third policy change did France provision abortion access with full financial coverage in 1982, while the costs of ART treatments have been included in the national health insurance system since the first regulation. On the other hand, only limited financial coverage is provided in Switzerland for ART treatments, while financial provisions for abortion were introduced before liberalizing formal access.
As this brief presentation of the abortion and ART regulations highlights, the trajectory of the three policy dimensions presents shifting patterns and greatly varies across policy areas and countries. To explain the variations in the regulation of the reproduction, seven explanations were developed in the first section, regarding institutions, politics and the party system, and the configuration of policy networks. The next section presents how these explanations have been operationalized as Fs/QCA causal conditions (Table 2) before discussing the main results.
Fuzzy Membership in Causal Conditions
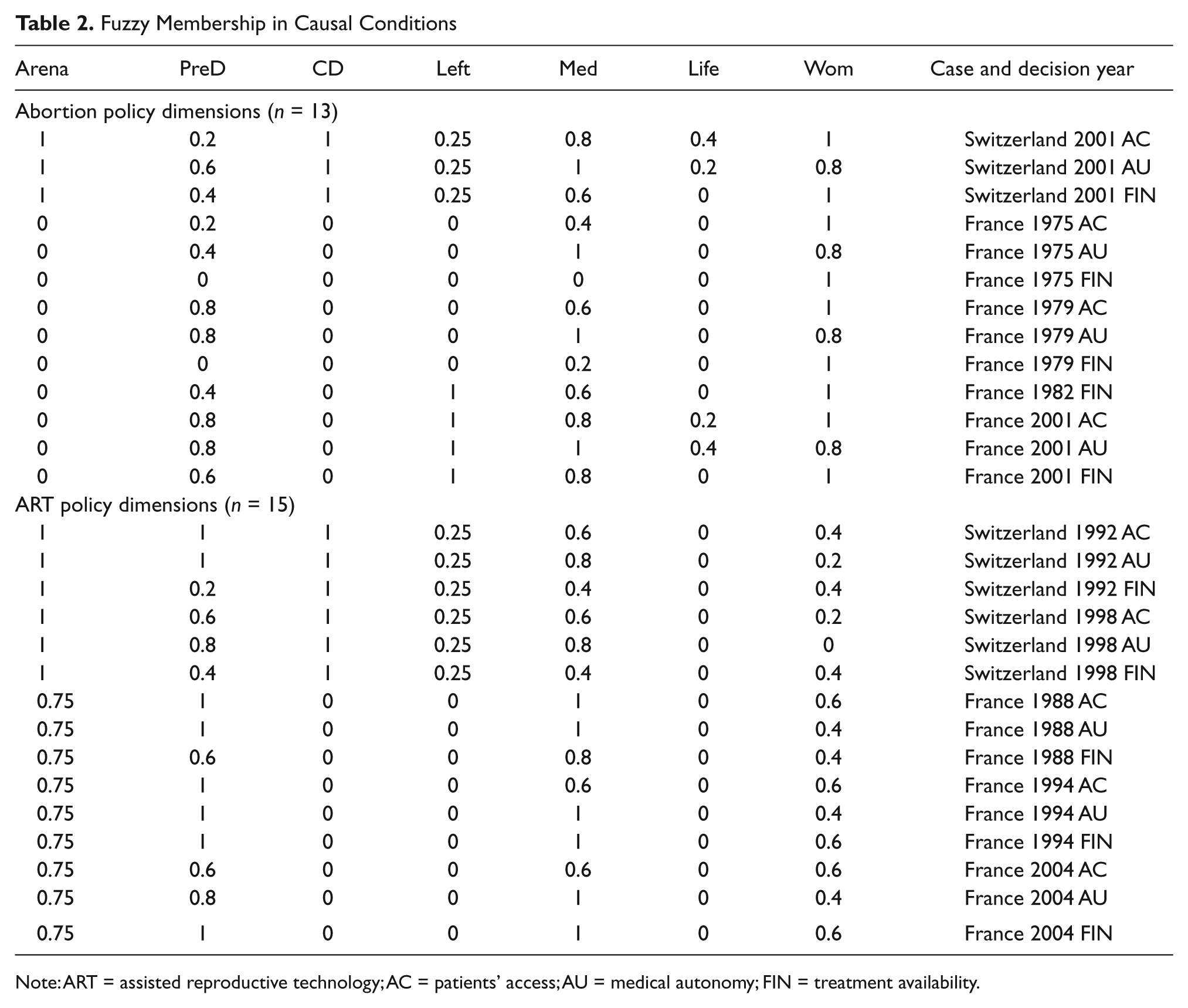
Note: ART = assisted reproductive technology; AC = patients’ access; AU = medical autonomy; FIN = treatment availability.
Causal Conditions
The first two hypotheses engaged with neoinstitutionalist arguments regarding the impact of institutional access and path dependency on the regulation of reproductive policies. The first causal condition captures the number institutional arenas in a three-value fuzzy set (“arena” condition in Table 2). In Switzerland, direct democracy and the preparliamentary legislative consultation procedure provide important points of access to the decision-making process, and the causal condition related to the number of policy arenas is coded 1 for all of the Swiss policies.
The French system remains mostly centralized. However, in the case of ART, a broad public consultation has been led during the entire process. This exceptional consultation has made the decision-making process more open than usual. Accordingly, a score of 0 is assigned to all French policies on abortion and a score of 0.75 is assigned to ART policies. Regarding the effect of path dependency, the “PreD” condition in Table 2 takes the fuzzy set value of the prior decision in the field. 5 Turning to the conditions related to politics and the party system, the two causal conditions regarding Social Democratic government (“Left” condition in Table 2) and the presence of a Christian Democratic party in the system (“CD” condition) are coded 1 in case of presence and 0 in case of absence. Finally, the policy preferences regarding the three policy dimensions of the main actors in the field, that is, the medical community, women’s movements, and prolife groups, have been thoroughly assessed through the same coding scheme used for evaluating the policy dimensions. 6 This coding scheme allows for a fine-grained evaluation of the policy preferences and enhances the comparability across cases. To trace the evolution in the policy position of these three sets of actors, the degree of permissiveness of their policy preferences was assessed in regard to the three policy dimensions (patients’ access, medical autonomy, treatment availability) at each policy decision time point as shown in Table 2 (the causal conditions “Med” for the medical community, “Wom” for women’s groups, and “Life” for prolife groups). 7
Analytical Procedure
The Fs/QCA analysis proceeds in two steps. 8 The first step consists of constructing the so-called truth table. The truth table maps out the logically possible combinations of causal conditions, that is, the multidimensional vector space encompassing all the combinations among the different fuzzy sets. In this analysis, seven causal conditions are included, so the vector space has 128 corners (27), meaning that there are 128 logically possible combinations of conditions. 9 However, not all of these combinations are supported by empirical evidence. Table 3 lists the membership score distribution of the twenty-eight empirical cases across the logical configurations of conditions. The cases studied represent only 11 of 128 logically possible combinations (rows 1 to 11). The 117 other combinations are logical remainders. These combinations could be logically possible but do not match any of the twenty-eight cases empirically apprehended in this analysis. Before reducing the logical complexity, the empirical relevance of the causal configurations is assessed according to the number of cases with fuzzy-set memberships greater than 0.5 (“n” column) and the level of consistency (“consistency” column), that is, the degree to which a causal combination of conditions is a subset of the outcome. 10 The second step consists of analyzing the truth table and reducing the logical complexity by the use of the Quine–McClusky algorithm (Ragin 2008) to identify sufficient causal path(s) leading to the outcome (here, permissive policies) and to the negation of the outcome (here, restrictive policies). 11 In the following section, the configurations of conditions leading to permissive policies and to restrictive policies are discussed in turn.
Consistency Test of Causal Conditions for Permissive and Restrictive Outcomes
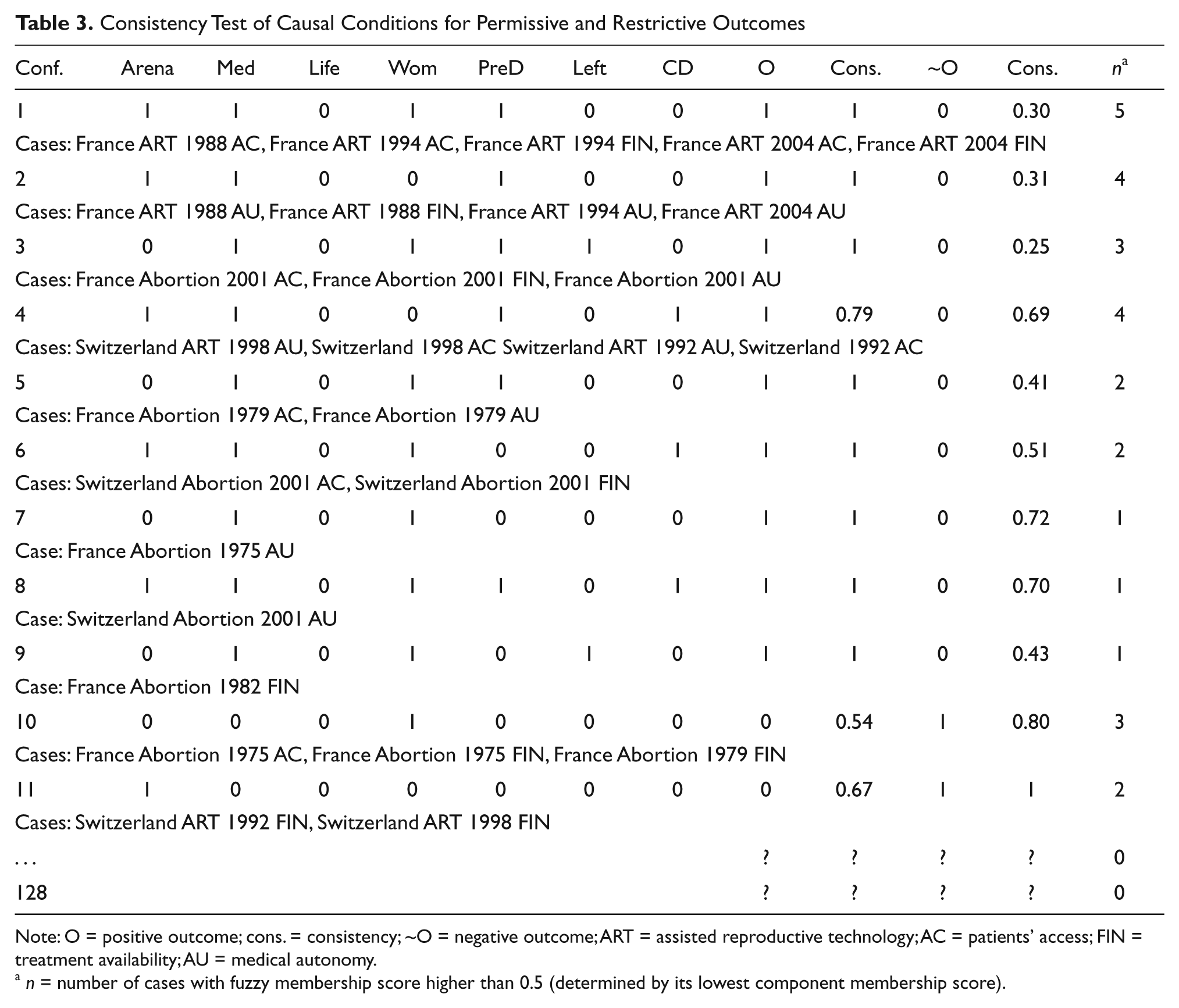
Note: O = positive outcome; cons. = consistency; ~O = negative outcome; ART = assisted reproductive technology; AC = patients’ access; FIN = treatment availability; AU = medical autonomy.
n = number of cases with fuzzy membership score higher than 0.5 (determined by its lowest component membership score).
The Different Paths to Permissive and Restrictive Policies in the Reproduction Field
Permissive Paths
The combinations of causal conditions that lead to permissive policies are the first to be minimized, the permissive outcomes being coded as 1 in Table 3 (“O” column). Because the total number of cases is rather small, a frequency cutoff of 1 was chosen which means that every configuration is taken into account in the analysis, and a consistency value of 0.78 was fixed as the benchmark criterion. Accordingly, the outcome’s scores produced by configurations displaying a consistency value less than 0.78 are set to 0 (rows 10 and 11 in Table 3), while the others are set to 1 (rows 1 to 9). 12 Through the minimization procedure, Fs/QCA calculates at least two solutions. The former results from the minimization based on the inclusion of both empirical cases and logical remainders and thus offers the most parsimonious solution. The latter is obtained from the empirical cases only and yields a much more complex solution. Table 4 displays the different sufficient paths toward liberal policies.
Sufficient Paths toward Permissive Policies
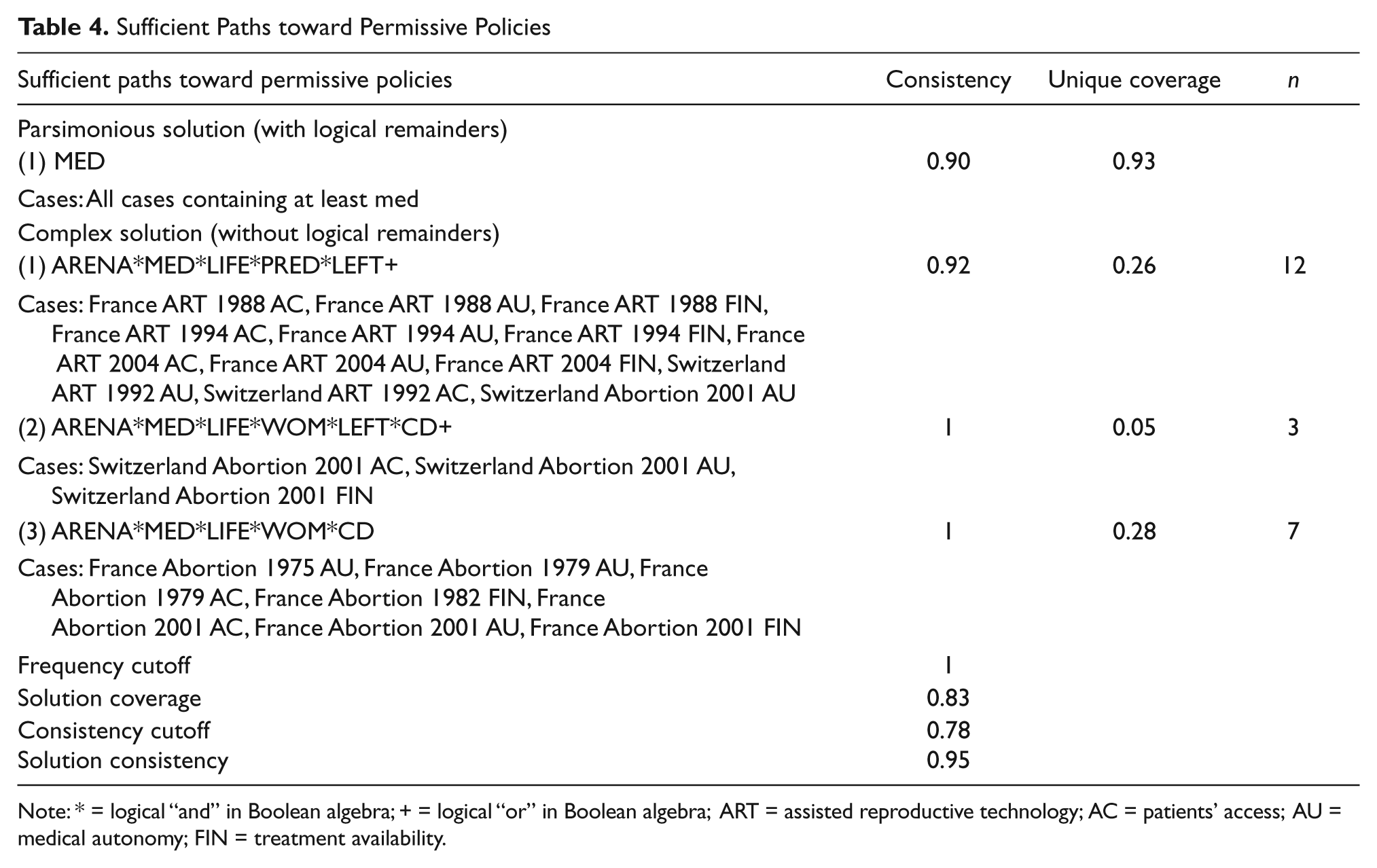
Note: * = logical “and” in Boolean algebra; + = logical “or” in Boolean algebra; ART = assisted reproductive technology; AC = patients’ access; AU = medical autonomy; FIN = treatment availability.
Let us first examine the most parsimonious solution identified on the basis of all the logical remainders. This solution would lead one (wrongfully) to an impressively parsimonious conclusion: the medical community is systematically successful in supporting permissive policy preferences, as the MED condition would be in itself sufficient and necessary to produce a positive outcome. However, this solution is based on numerous unsustainable simplifying assumptions that imply “difficult counterfactuals” (Ragin and Sonnett 2005). To reach this solution, assumptions specifying, for example, causal configurations where prolife movements would be in favor of a full liberalization abortion were used. If this situation is logically possible, it is, at best, empirically highly implausible. Accordingly, this so-called parsimonious solution should not be considered as the best “empirically driven” solution for the cases studied here. 13
Let us turn to the complex solution, which indicates three alternate paths toward permissive reproductive policies that are identified solely on the basis of empirical cases. As the analysis covers a relatively small number of cases, the complex solution results in a much more robust solution than the parsimonious one. At first glance, if the medical community seems to be an important causal condition, the complex solution confirms that there is more than one way to reach permissive policies on abortion and ART and that all paths are composed of a combination of conditions, which means that no single causal condition decisively favors the elaboration of a permissive policy. Indeed, the three paths better specify the impact of the medical community. The complex solution is highly coherent as its consistency value is almost perfect with a value of 0.97 (of a maximum of 1) 14 and has an acceptable coverage of 0.83 (of a maximum of 1). Detailing the values for unique coverage, Table 4 shows that the second path has a very low value, meaning that it does not cover, by itself, many empirical cases. The first and the third paths are more comprehensive and cover a large set of cases. 15 To facilitate the interpretation and the discussion of the results, the three paths can be grouped according to the presence or absence of many policy arenas.
The first two paths correspond to situations of decision making in numerous policy arenas. The first path includes a high number of policy arenas (ARENA) combined with (*) permissive preferences of the medical community (MED), restrictive preferences of the prolife movement (LIFE), permissive prior decision (PRED), and the absence of strong left-wing party in the government (LEFT). In others terms, when the decision-making process takes place in many policy arenas, when leftist parties are not strong, and when physicians express permissive preferences, the resulting policies tend to continue to be permissive, decision after decision, even with the opposition of the prolife movement. 16 The second path shows that the permissive claims of the women’s movement (WOM) even with the presence of the Christian Democratic party (CD) in the political system can be substituted to the causal condition related to the existence of a permissive prior decision. In both paths, the policy preferences of the medical community are very important, as this condition is included in the two terms.
However, physicians are not strong enough to impose, solely, their permissive policy view in a context of numerous policy arenas. On the contrary, they either benefit from the support of the women’s movement (as the second path points out) or, more often, express their strategy in a favorable policy context with a permissive precedent decision, as it has occurred most often in the case for ART policies (according to the first path). In the ART sector in both countries, the technological development precedes by far any public regulation, and the medical community enjoyed a high degree of autonomy for many years. In fact, this situation did make them powerful players, as they imposed most of their policy preferences during the elaboration of the first decisions on ART in 1988 in France and in 1992 in Switzerland. The intervention of the medical community was legitimized by their scientific expertise and their social prestige. Being at the same time the main implementer of the regulation and the tenants of the technological development, the medical community benefited from both consequential institutional and prestige resources. However, if the medical community remained very strong during the revision of French policy, it was not the case in Switzerland, as will be shown below. The third path corresponds to most of the liberalization process of abortion in France, where the arenas were few and closed. With the exception of the number of arenas, this last path is somewhat similar to the second one. When they share common interests, the medical community and the women’s movement foster a strong alliance to impose a permissive regulation of abortion in France. However, the analysis of the sufficient paths leading toward restrictive policies shows that fostering such an alliance is not easy, especially where financing the coverage of abortion is concerned.
Finally, if the Fs/QCA analysis of the permissive outcome does offer a number of meaningful results, the three paths contain, nevertheless, some conditions that are more difficult to interpret as solely the empirically observed cases were included in the minimization. Obviously, the preference of the prolife movements and the presence of strong Christian Democrats did not play key roles in promoting permissive policies. If the Christian Democrats and prolife actors were not successful in preventing the elaboration of rather permissive policies, they, nevertheless, played an important role in the political process. Christian Democrats and prolife groups managed to veto several abortion reform attempts in Switzerland, Christian Democrats benefitting from their veto position in parliament while the prolife actors launched several initiatives and referenda in the direct democratic venue to postpone abortion liberalization.
Restrictive Paths
If the configuration of conditions leading to permissive policies presents interesting results, the analysis would be incomplete if the path or paths toward restrictive policies are left unexplained. Let us start again from the truth table presented in Table 3 and study the negation of the permissive outcome (~O), that is, the restrictive outcome. For the minimization of the configuration of conditions leading to restrictive policies, the frequency cutoff is set to 1 as before, and the consistency cutoff to 0.8, as Table 3 indicates an important drop, from 0.8 to 0.7.
The parsimonious solution for explaining restrictive policies, which includes all the logical remainders, is, in itself, no more satisfying than was the parsimonious one for permissive policies (Table 5). Once again, the parsimonious solution stresses the importance of the medical community’s preferences as a sufficient cause by itself. For the same reasons of implausibility as before, this solution is not considered to be empirically and theoretically sustainable; accordingly, the discussion relies on the complex solution. This solution leads to two different paths, which, once again, specified the impact of the medical community and are differentiated according to the number of policy arenas. If the solution consistency is rather acceptable, the solution coverage is, however, quite low. A couple of empirical cases are indeed not explained in these two paths; they are discussed later on.
Sufficient Paths toward Restrictive Policies
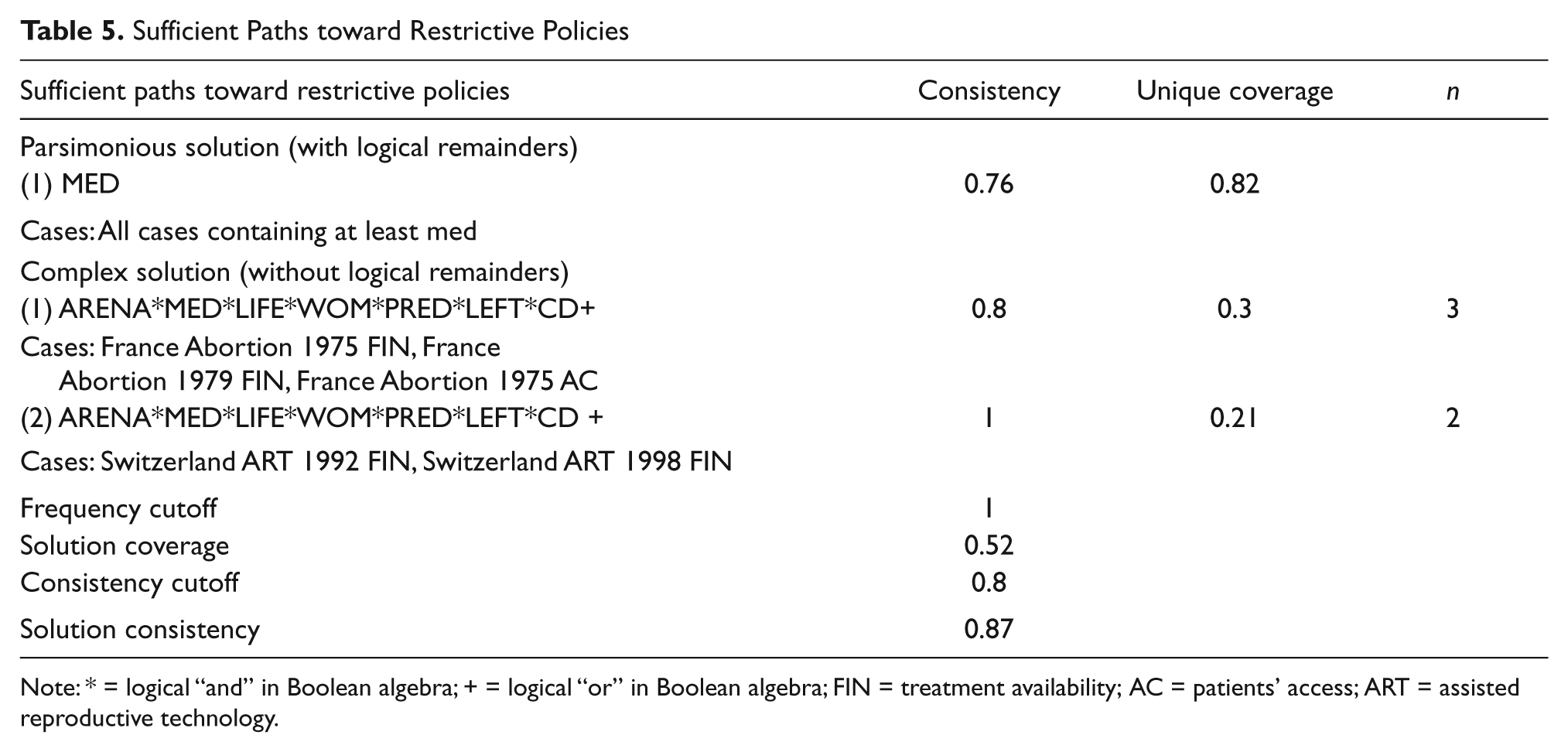
Note: * = logical “and” in Boolean algebra; + = logical “or” in Boolean algebra; FIN = treatment availability; AC = patients’ access; ART = assisted reproductive technology.
The first path corresponds to the restrictive regulation of abortion financial coverage in France during the 1970s. It confirms the analysis of the liberal path: physicians are powerful actors who can block, at least in the case of few policy arenas, the permissive claims of the women’s movement for abortion free of charge. The second path represents an easily understood situation. Even in the case of a high number of policy arenas, if no one wants a permissive regulation, consequently the policy will become restrictively regulated, as was the case for the extremely low financial coverage of ART treatments in Switzerland. Neither physicians nor the women’s movements defended permissive preferences, while the prolife groups were strongly mobilized against ART and attempted to block the process through referendum and popular initiative several times. Sole moderate right-wing parties promoted permissive regulation. Isolated, they did not manage to counter this broad set of restrictive policy preferences.
Finally, the analysis of the restrictive paths reveals two contradictions, which confirms the low value of the solution coverage. In one instance, the identified paths do not capture one empirical case: the Swiss restrictive regulation of the patients’ access to ART in 1998. This case shares the same combination of conditions as the second path, with one exception: the absence of prior permissive decision. Indeed, the explanation of the lower degree of patients’ access to ART in Switzerland is quite complicated. The first regulation, in 1992, was a constitutional article, and the access was rather permissively regulated, as the article did not say much about it. The regulation of 1998, still in effect at the present, is a federal law that covers the patients’ access much more comprehensively than did the constitutional article, thereby adding consequential and very detailed restrictions. In a second instance, one case is obviously “misclassified,” the regulation of women’s access to abortion from the French law of 1975. This case shares the same configuration of conditions with the French regulation of abortion financial coverage during the 1970s. However, the three cases do not share the same empirical outcome. While access to abortion was liberalized in 1975, the financial coverage was provided much later, only in 1982. On the side of the financial coverage, the reluctance of the medical community was strongly reinforced by the unconditional opposition of prolife actors. Prolife actors as well as the Catholic Church were consulted during public hearings led by the parliamentary commissions in charge of the reform of the abortion law in the first half of the 1970s. According to them, provisioning public financial coverage for abortion would not have been less that legitimizing or even promoting abortion. It seems that their complaint was heard. The absence of financial coverage and the introduction of a physician’s conscientious objection clause specifically related to abortion were conceded to the religious actors in the 1975 law. Prolife actors and the Church successfully protected this policy asset until the Social Democrats came to government in 1982. In this sense, the first French abortion reform can be best described as a policy compromise: abortion was allowed on women’s request, as the feminist groups requested, but its access was not facilitated by the state. No financial coverage was provided, and public hospitals were not required to provide any abortion provisions.
Conclusion
Governing reproduction has exerted a high level of political polarization since the end of the 1960s. Abortion has caused a heated controversy that was then redimensioned by the development of ART techniques in the 1980s. While addressing similar fundamental questions on reproductive rights, professional autonomy, and the status of the embryo, governing reproduction has revealed strong variations across policies and countries. The Fs/QCA analysis of the French and Swiss policies on abortion and ART since the 1970s shows that different institutional configurations tend to produce rather similar permissive policies. Neither the number of policy arena available nor the presence or absence of strong Christian Democratic and left-wing parties tend to produce a systematic impact on the content of the policies as the Fs/QCA identified rather comparable alternate paths. These findings are very much in line with comparative research on abortion and ART that conclude that institutions tend to exert less influence in the regulation of the reproduction field (Bleiklie, Goggin, and Rothmayr 2004; Outshoorn 1996; Stetson 2001). As Outshoorn argues (1996, 161), in most Western European countries the regulation of reproduction is not part of “the normal business of politics.” Controversies over reproductive issues reveal important divisions across the political space but also within political parties. As a result, Social Democrats did not always act as an uncontested champion of abortion liberalization, nor were they the main promoters of a liberal stance on the ART technological development. As previous research pointed out, the impact of the Social Democrats has been at best moderate (Bleiklie, Goggin, and Rothmayr 2004; Stetson 2001). In France, abortion access was liberalized under a right-wing government, but the Social Democrats greatly extended the financial coverage of abortion once in power in the 1980s. The previous center-right government introduced measures targeting only women with low economic resources. In Switzerland, the Social Democrats were, at first, much embarrassed by the first popular initiative on abortion launched in the beginning of the 1970s. The initiative, supported by the second-wave feminist groups, requested the full liberalization of abortion. Only two Social Democratic MPs voted in favor of the initiative. Because of the small number of cases, the conclusion tends to be less straightforward for restrictive policies. It seems that when policy arenas are rather few and closed, it is more difficult for one actor alone to impose its policy preferences, as pointed to by the French policies on abortion during the 1970s. Mostly excluded from the decision-making arena, the women’s movement did not receive any support and failed in obtaining financial coverage of abortion. Only when the left came to power in 1981 was the movement’s claim satisfied. The question remains to determine whether this failure during the 1970s is mainly the result of the movement’s characteristics, notably its growing internal division, or the limited institutional access provided by the French style of strong state. Indeed, variations among the policies analyzed here seem to be significantly better explained by a sectoral logic of regulation.
In France and Switzerland, reproductive controversies systematically involved the same triangle of actors, the medical community, feminist movements, and the prolife movement. The edges of the triangle, certainly, vary according to the resources at disposal. Policy actors benefit from various sets of resources such as financial and organizational as well as institutional. In both countries, medical associations, women’s movements, and prolife groups were provided with institutional access during public hearings and consultation. The intervention of the medical community was legitimized by its scientific expertise and social prestige. Feminist movements suffered from divisions over which strategy to adopt and over which alliances to foster, while the prolife movement has gradually lost some traditional allies among the right wing. Nevertheless, in each controversy, in one way or another, doctors, feminists, and the prolife movement represented strong actors in the struggle. Comparing abortion reforms in Western Europe, Outshoorn (1996) pointed out that with the growing ART sector, physicians might become a key adversary to women’s movements and replace the Christian Democrats’ opposition. In her study on France and the United Kingdom, Latham (2002) also emphasized the growing influence of the medical profession over reproductive issues. The analysis of the evolution of the policies on ART and abortion in France and Switzerland presented here confirms that the medical community has proven to be a very powerful actor not only in the ART sector but also in abortion regulation (Engeli 2009a, 2010). If physicians were granted a privileged position in the policy-making process in the ART sector, they also successfully imposed numerous preferences in regulating abortion since the beginning of the 1970s. Nevertheless, physicians did not manage to keep the ART issue within their auto-regulation sphere. Once the ART issue reached the political agenda, physicians either were constrained to accept compromise or forged alliances with the women’s movement (Engeli 2009a). The influence of women’s groups has been rather variable. Success in the struggle over abortion came earlier in France than in Switzerland, where abortion was fully liberalized only in 2002. On the contrary, feminist groups successfully contributed to the elaboration of a very permissive law on ART in Switzerland, while a serious lack of support isolated them in France. If the struggle on abortion, to a certain extent, reunified the women’s movements, the ART issue profoundly divided them. Weakened by internal division, some Swiss women’s groups still benefited from the support of the Social Democrats and the Greens. Their gendered anti-ART discourse resonated far beyond their direct capacity of influence. In France, women’s groups were also very divided but did not forge any alliance. As a result, they were soon isolated in the ART policy network and had to struggle against both the medical community and prolife actors (Engeli 2009b). Prolife groups certainly did not succeed in banning abortion and ART in France and Switzerland. Most of the time, policy decisions in the field of reproduction did not match their preferences. They nevertheless may have prevented a worsening of the defeat, at least temporarily. In France, they reinforced the opposition of the medical community to provide financial coverage for abortion during the 1970s. They lost this asset only when the Social Democrats came to power in 1981. In Switzerland, the prolife groups recently launched, in January 2010, a popular initiative aimed at excluding abortion from the compulsory health insurance scheme. In 2002, they lost the battle on liberalizing abortion access and were faced with a severe defeat at the polls. A large majority of the Swiss citizens approved the liberalization of abortion policy and rejected the abortion ban initiative. The future will tell whether they will be able to win again on the financial aspect of the regulation the reproduction. 17
Footnotes
Acknowledgements
The author is grateful to Dorothy McBride, Mona Lena Krook, Frédéric Varone, Alison Woodward, and the anonymous reviewers for their helpful comments on previous drafts of this article.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.