
Abstract
A persistent puzzle in American politics is whether shared gendered experiences can bridge enduring racial divides in political attitudes. This study evaluates whether maternal health policy frames can activate gendered solidarity among white women in ways that shape their support for a Black woman candidate. Using a survey experiment fielded to a representative sample of 1,047 white women, I assess how exposure to maternal-health-oriented policy messages influences evaluations of Black women candidates. The results show that white women respond sharply to explicitly race-specific health policy agendas, while gender-only health policy agendas do not meaningfully increase support for a Black woman candidate. Additional analyses using established measures of racial resentment and gender consciousness help illuminate these patterns. Notably, gender consciousness is only reactive to the intersectional policy cues. Exposure to the Black maternal health frame (race and gender) reduces the otherwise positive effect of gender consciousness on support for a Black woman candidate. Taken together, racialized attitudes remain the most powerful and consistent predictor of support, while gender consciousness contributes little to no positive upside for Black women candidates.
Introduction
In May 2022, Vanity Fair spotlighted Louisiana Senator Bill Cassidy for dismissing the significance of Black maternal mortality rates. In an interview with Politico, Cassidy stated, “If you correct our population for race, we’re not as much of an outlier as it’d otherwise appear,” and added, “For whatever reason, people of color have a higher incidence of maternal mortality” (Levin 2022). His remarks draw a sharp line between the experiences of Black women and those of “American” women, effectively disavowing the legitimacy of Black women’s suffering. Cassidy’s comments reflect the persistent racial boundaries that shape definitions of womanhood, reinforcing a historic tendency to exclude Black women from its full recognition. More broadly, his words exemplify the state’s ongoing disregard for Black women’s lives—an erasure with deep historical roots dating back to the early 1800s. 1
However, when women, particularly Black women, gain elected office, their lived experiences often become visible through the legislative priorities they advance. Research shows that women legislators are more likely to champion policies related to women’s health and well-being (Holman 2017). Mayor Muriel Bowser, the first Black woman to serve two terms as Washington, D.C.’s mayor, exemplifies this trend; since her first term, she has introduced legislation and funded studies addressing Black maternal health (McNeely 2022). In a separate branch of government, former Congresswoman Cori Bush has elevated Black maternal health to a national priority, drawing on her own experiences with the health care system to advocate for the support of the Momnibus Act 2 in Congress. Taken together, scholars have documented how Black women political leaders frequently leverage personal narratives to drive meaningful policy change—particularly in advancing the health and wellness of their constituent communities (Brown et al. 2023; Wright 2023).
Recognizing that white women also face maternal health risks, this study evaluates whether maternal health frames can generate greater support for Black women candidates, despite prior evidence that white women are no more supportive of Black women candidates than white men (Philpot and Walton 2007). As Black women politicians outpace their counterparts in pursuing elected office, doing so further examines whether advocacy by Black women leaders can resonate with white women voters. Using a nationally representative sample of over 1,000 white women, this research explores whether shared maternal risk and a common commitment to motherhood can bridge political and racial divides, or whether white women may still reject policies in their own interest when those policies are associated with Black leadership.
The paper begins by outlining key debates around descriptive representation, particularly as they relate to all American women. Because this study centers experiences unique to women and those who give birth, examining descriptive representation provides insight into how identity influences perceptions of political leadership. The paper then argues that maternal health care, given its historical and cultural resonance with womanhood, should be a powerful issue for mobilizing white women voters. The latter half of the paper develops the theoretical framework, highlighting racial resentment and gendered consciousness as central to understanding white women’s political attitudes for the purposes of this study. It then presents the experimental design and hypotheses, grounded in the literature on political behavior and identity-salient framing. Finally, I interpret the results to show how racialized attitudes overpower the impact of gender considerations, and I conclude the paper with a brief discussion on how these findings relate to the empirical evidence from previous U.S. election campaigns.
While this study explores whether a descriptive representative, specifically a Black woman, can effectively build support for their campaign, its central aim is to assess whether racial resentment among white women is strong enough to override a shared vulnerability to maternal health risks and a mutually beneficial, life-affirming policy agenda. My findings suggest that it is. Race-specific health care positions demobilized support for the Black woman candidate, while race-neutral positions, including maternal health, generated modestly positive yet non-significant results.
Descriptive Representation and Support for Women Candidates
Amongst women voters, a long line of inquiries points to women caring and talking more about politics when a woman is running for office (Atkeson 2003; Burns et al. 2001; Hansen 1997). Substantively, female candidates also hold and offer differing perspectives from men. Women representatives are more likely than men to consider vulnerable populations in decision-making (Huddy et al. 2008; Hutchings et al. 2004). For example, women are “eighty percent more likely to mention poverty or homelessness” and more likely to issue government spending on these issue areas (Mendelberg et al. 2014, 2). Women are also more likely to prioritize family and child issues, even after controlling for partisan affiliations (Burns et al. 2001; Carroll 1984; Crowder-Meyer 2010). There is more to be discovered about the conditions in which women’s substantive representation is successful. Mendelberg, Karpowitz, and Goedert find that women’s substantive representation is effective primarily under majority rule (2014). The theory of descriptive representation gets further muddled after considerations of multiple identities and party identification.
Some scholars argue that candidates who embody multiple marginalized identities may be able to elicit support from multiple identity groups simultaneously. For example, in reflecting on the candidacy of former Vice President Kamala Harris, Montoya et al. (2022) examined how intersecting identities can activate feelings of linked fate across groups. Using data from the 2016 Collaborative Multiracial Post-Election Survey (CMPS), they found that respondents of color, both men and women, were more likely to believe that candidates who shared their racial, ethnic, and gender identities would best represent their interests (Montoya et al. 2022, 493). Because shared racial identity often strengthened perceptions of political representation, earlier scholarship suggests that Black mayors, particularly during the 1970s, frequently relied on explicitly racialized rhetoric rooted in shared experiences to mobilize and maintain support among Black constituents (Thompson 2006). Black women candidates have similarly drawn upon their racialized and gendered lived experiences in campaign messaging (Wright 2023). However, other scholarship suggests that adopting post-racial (Wamble and Laird 2020) or universalistic rhetoric (Perry 2011) may be more effective for building broad electoral coalitions. Put differently, scholars argue that explicitly racialized campaign appeals may activate racial resentment or reinforce stereotypes that Black candidates are unable to adequately represent the interests of non-Black voters.
Some scholars have also argued that interest in politics amongst women has less to do with the identity of the women candidate and more with the partisan alignment. Lawless claims that party congruence is the most motivating factor amongst the women electorate and that the candidate’s gender has a marginal effect (2004). In response, Dolan (2014) further argues that gender alone is not a sufficiently mobilizing identity, as people are more likely to align with their racial identity. However, the intersection of gender and race has the capacity to mobilize Black women voters in support of Black women candidates (Stokes-Brown and Dolan 2010). And so, the racial identity strength not only corroborates the findings of Philpot and Walton (2007), the empowerment effect (Bobo and Gilliam 1990; Spence and McClerking 2010), and the concept of “linked fate” for Black voters (Dawson 1994; Gay and Tate 1998), but it also highlights white women’s reluctance to support women-of-color candidates (Matos et al. 2021) and the relative absence of a gendered consciousness with the same mobilizing power as racial consciousness (Gurin 1985).
Using public opinion data, Matos, Green, and Sanbonmatsu found that “white women expressed the least support for more women of color (WOC) in Congress compared to other racial groups” (2021). Some scholars have theorized this reluctance in racial and ethnic candidate support by white women as the existence of a racial threat (Enos 2010, 2016; Sigleman et al. 1995). Racial threat is a response to greater racial and ethnic diversity, which activates whites’ fear of a changing racial order and supremacy (Key 1949). Studies have since tested the existence of racial threat in support of a candidate (Enos 2010; Giles and Hertz 1994), and ultimately, making sense of the unprecedented win of Donald Trump (Gutierrez et al. 2019; Stewart and Willer 2022). Others hesitate to subscribe to the racial threat phenomenon by positing a perspective that gives credence to early childhood socialization (Henry and Sears 2009; Kinder and Sanders 1996) or education levels that influence racialized attitudes. Taken together, these theories speak to racial resentment in white attitudes and often take shape in their political decision-making (Kinder and Sanders 1996).
Despite the aversion to supporting Black women candidates because of prejudicial aspersions, studies have shown that Black women candidates are more likely to represent the interests of underrepresented groups, including women and other racial/ethnic minorities more than their male and female counterparts (Brown 2014b; Smooth 2006). Moreover, given Black women’s lived experiences and their commitment to advancing the interests of multiple social groups, if there were a scenario in which maternal health policy anchored in life-affirming care is positioned, Black women candidates are the modal candidate in doing so.
The Case for Maternal Health Policy
In 2018, the Kaiser Family Foundation reported that health care is among the top policy priorities for women voters, regardless of party affiliation (Rubin 2018). While American men and women alike view health care as a critical issue, women are up to 14 percentage points more likely than men to prioritize it over issues such as foreign policy, immigration, and gender equity (Deckman 2018). These trends persist even when controlling for partisanship. Similarly, Black women consistently rank health care as a core political concern. 3 I argue that health care is a policy that should create the best conditions for white women to support a Black women candidate, but specifically, a policy adjacent to childbearing, caring, and life-affirming care should produce meaningful results. Maternal health reflects longstanding and evolving political priorities among American women, though the nature of that alignment has varied across time, context, and race.
Maternity and White Women
While health care generally is a suitable domain for exploring women’s political behavior, maternal health specifically holds strategic promise. It sits at the intersection of Black and white women’s political interests, in part because of the deep cultural and ideological significance of “motherhood” in the project of white womanhood.
Historically, white motherhood has operated not merely as a private familial role but as a political institution imbued with racial authority and civic virtue, dating back to the early 19th century (Baker 2018; Cherry 2001; Kerber 1976; Love 2016; McGirr 2015). White slave-owning mothers used their maternal roles to instruct their children on how to treat and punish enslaved people, thereby reinforcing the subjugation of Black people as inherently less than human (Williams 2021). With much of the domestic labor delegated to enslaved and indentured women of color (Collins 1990; Third World Women’s Alliance 1970), one could argue that the primary function of white motherhood became the reproduction of racial hierarchies within the household, training the next generation to uphold white supremacy (Jones-Rogers 2019). In this way, white motherhood was central to what Omi and Winant (2014) describe as “the racial project”: the process by which racial meanings are constructed and institutionalized through both social and political practices. Crucially, Omi and Winant argue that the racial project is not static but deeply responsive to its historical and social context and shifting over time in form and function. Similar to the racial project, the function of motherhood is also evolving, continually adapting to the dominant social and political imperatives of its time (Greenlee 2014).
By the late 19th and early 20th centuries, the role of white mothers evolved alongside state intervention and industrialization. Women advocated for more robust social programs to support American families (Williams 2021). Yet, even as federally funded programs, like welfare, benefited white working mothers, they also deepened racial and economic disparities. White publics resisted extending welfare to single Black mothers, invoking stereotypes of laziness, hypersexuality, and reproducing “incorrigible” Black children (hooks 1981; Omolade 1987; Roberts 2004). Motherhood, in this context, functioned as a mobilizing force for particular policy agendas, reinforcing protections and benefits for white families while simultaneously limiting racial progress. This dynamic illustrates how racial resentment has shaped the logic of white maternal protectivism: motherhood becomes a lens through which white Americans perceive and respond to the perceived threats of Black urbanization and demographic change. These attitudes are less about economic self-interest and more about maintaining racial hierarchies, as evidenced by persistent stereotypes of Black mothers and children (Blalock 1967; Craig et al. 2018; Kinder and Sanders 1996).
Scholars have argued how these anxieties underpin the contemporary resurgence of the “Great Replacement Theory,” the idea that the white racial order is under existential threat due to immigration and racial diversity (Cosentino 2020; Obaidi et al. 2022; Pape et al. 2024; Thompson et al. 2025). Political elites have long responded by encouraging white women to have more children, invoking slogans like “We can’t restore our civilization with somebody else’s babies.” 4 In fact, Nancy Love (2016) argues that many white women are drawn to white supremacist ideologies out of a desire to protect themselves and their children from perceived racial extinction (2016, 92). This framing can help explain why 52% of white women voted for Donald Trump in 2016, despite a campaign steeped in racism, homophobia, and misogyny (Junn 2017) and a contender who marketed her campaign as fighting for women’s rights and opportunity. 5 It also underlies how racial resentment has continued to shape policy preferences and presidential evaluations (Enders and Scott 2019; Strawbridge et al. 2025).
Even when mobilized by racist ends, maternal health as safe birthing practices remain a central concern for many white women, especially among the far right. This alignment creates an odd set of bedfellows with Black women engaged in the fight for maternal health.
Maternity and Black Women
In contrast, Black motherhood has historically been both criminalized and devalued. Black women have faced forced sterilizations, state surveillance, and cultural demonization for having children (Roberts 1997; Zivi 2005). For Black women who chose to bear children, they were often labeled as promiscuous, deviant (Davis 1981; Threadcraft 2016), corrupt (Hancock 2004; Roberts 1997), and responsible for the plight of Black communities (U.S. Department of Labor and Office of Policy Planning and Research 1965). Put simply, motherhood takes on different meaning for Black mothers. Unlike white motherhood, which has been framed as a public good and cornerstone of the nation (Novkov 2008), Black motherhood has often been viewed as a threat. Yet, Black women have continuously redefined motherhood as a form of resistance, meaning-making, and community empowerment (Collins 1990; Cherry 2001; Wright 2022, 2023). As April Cherry notes, “African-American women have used their positions as mothers, othermothers, and community mothers to work towards racial equality”—a sentiment shared by several other Black feminist theorist and Black politics scholars (Cherry 2001; Cohen 2004; Dowe 2023; Kelley 2022; Wright 2023).
One of the most urgent and measurable site of this struggle today is the Black maternal health crisis. Since the CDC began tracking maternal deaths in 1986, rates have more than doubled—from 7 deaths per 100,000 live births in the 1980s to over 17 today (Gingrey 2020). Black women are currently more than three times as likely as white women to die from pregnancy-related complications. Given the disproportionate impact of these disparities on Black women and Black families, some scholars may characterize Black maternal health as a “consensus” issue—one that constitutes a collective political priority for Black communities broadly defined (Cohen 1999).
Importantly, maternal health, unlike abortion, is not broadly seen as a polarizing issue. While 63% of women identify as pro-choice (Gallup 2024), maternal health policy broadly avoids the ideological minefield that can alienate bipartisan coalitions, particularly when it is framed as life-affirming care. Schreiber (2002) also finds that conservative women’s anti-abortion positions are often grounded in a gendered consciousness centered on protecting the sanctity of women’s lives (2002, 338). Taken together, these dynamics suggest that maternal health may constitute a policy domain in which women across race and party lines can find shared resonance, what Derrick Bell (1980) theorizes as interest convergence. It also provides a strategic lens for assessing whether gendered consciousness serves as a mechanism for predicting support for, or opposition to, Black women candidates.
Taken together, motherhood has never been politically neutral. For centuries, it has been shaped by state policies, cultural norms, and racial hierarchies. Whether white women are encouraged to engage with maternal health policy out of racial preservation or Black women champion it for dignity and survival, the theoretical shared investment in safe birthing conditions should not be ignored. Further, maternal health policy is not only mutually beneficial, but also politically opportune. If there is any issue that could catalyze white women’s support for Black women candidates, this should be it.
Hypothesis
This paper frames maternal health as life-affirming care, presenting it as a non-polarizing women’s issue for two reasons: (1) it can advance multiple political goals, and (2) its historical roots emphasize a conceptual separation from abortion. 6 Positioned in this way, maternal health offers a strategic opportunity to assess whether a unifying policy frame can mobilize white women voters, and whether doing so challenges prior findings that white women are no more or less likely than white men to support Black women candidates (Philpot and Walton 2007). More specifically, this study asks whether emphasizing an assumed shared experience, embedded both in the policy itself and in the candidate’s explicit in-group appeals, can activate a gendered consciousness among white women that has historically failed to translate into meaningful support.
Using a pre-registered survey experiment of over 1,000 white women respondents, I asked questions that gauged attitudes towards a fictional Black women mayor, Carolyn Johnson, after exposing them to one of her policy positions (Maternal Health or Health Care) during a fictional campaign trail. The study was fielded on the CloudResearch survey paneling platform on July 12, 2022. The Northwestern Institutional Review Board approved all study procedures.
To clarify expectations, I distinguish between two related but analytically distinct outcomes among white women respondents: (1) support for the candidate, (2) support for the candidate’s policy positions. For white women respondents, my hypothesis is as follows:
Candidate Support
Maternal health could be categorized as a “gendered” issue, one that affects the well-being of all women and birthing people. Scholarship makes clear that Black women candidates are tasked with combatting stereotypes that suggest they will not advocate for all groups equally but advance the interests of Black people specifically (McDermott 1998); I anticipate that the apparent elevation of a “women’s” issue that does not distinguish across racial lines will signal to white women that their interest will be of importance. Further, studies show that candidates who foreground their motherhood can receive higher evaluations on stereotypically feminine issues (Bauer 2015; Sweet-Cushman and Bauer 2024) and can also elicit a gendered consciousness by articulating injustice in ways that motivate collective action (Klatch 2001; Klein 1984). The candidate vignette that highlights Johnson as a mother, coupled with the gendered “moms’ lives” prime should activate higher evaluations as the literature suggests.
Support for a Black woman candidate will be highest when she advocates for maternal health, relative to all other policy conditions, holding all else constant.
However, since Health Care is considered a universal concern amongst Americans and a political agenda that’s often supported across partisan lines, my H1b is as follows:
Support for a Black women candidate will be second-highest when she advocates for the health care for all (control) condition, holding all else constant.
Further, I do not expect health care for all to influence support for a Black woman candidate in a negative direction. However, studies have suggested that the isolation of race in a political agenda that could be categorized as neutral can produce demobilizing effects for a candidate who advances said issue (Tesler 2012). For that reason, my H1c is as follows:
Support for a Black women candidate will be second-lowest when she advocates for Black health, relative to the control, holding all else constant.
Evidence suggests that Black and marginalized folks are vulnerable to threatening environmental conditions (Bullard 1990), that impacts their material health conditions (Anderson and Fullerton 2012; Kaufman and Hajat 2021; Williams and Collins 2001) with little resolve due to their limited access to proper health care (Anderson 2017; Williams and Collins 2001). For this reason, it is likely for a Black women candidate to advocate for bettering the conditions of Black families. I expect a health care policy that isolates the issues of Black people specifically will demobilize white women because it feeds into the stereotype threat that Black candidates do not advocate for all interests, but Black interests (Conyers and Wallace 1976), and activates racially resentful attitudes (McDermott 1998; Terkildsen 1993; Weaver 2012).
My H1d is quite tricky considering there are not many studies that empirically test the demobilization of white women amid a policy agenda that is “intersectional” in its nature. Since the Black maternal health agenda positions both race and gender, I hypothesize the following:
Support for the Black women candidate will be lowest when she advocates for Black maternal health, relative to all other policy conditions, holding all else constant.
Empirical studies that test an intersectional effect on Black voters are either inconclusive or have a demobilizing effect (Bonilla and Tillery 2020). If a demobilizing effect is present amongst Black voters, I anticipate the same effect, if not greater, among white women voters. Further, considering literature that suggests membership to motherhood is a white experience, I expect the Black maternal health care to be most demobilizing.
Policy Support
While I argue that advocacy for the maternal health policy will garner the greatest support for a Black women candidate (H1a), I also predict:
Support for maternal health care will be strongest among white women respondents, relative to all other policy conditions.
Support for health care for all will be strong, but not as strong as maternal health.
Support for Black health care will be weaker than support for the control condition.
Support for Black maternal health care will be weakest among all policy conditions.
Expected direction of effects by policy condition
Since there are two maternal health agendas under consideration, it is reasonable to expect that, for white women to measure “maternal health” so favorably, “Black maternal health” would fare higher in comparison to all other issue areas. My findings suggest that the racial specification of “Black” maternal health draws a significant gap between the evaluation of the two, with one trending in a positive direction and the other, negative.
Experimental Design and Methodology
Due to the discriminatory institutional and societal structures that have plagued their experience, Black women candidates are often motivated by their radical imagination of a more just world, which then benefits those who look like them “and society as a whole” (Dowe 2023; Kelley 2022). Suppose we understand that the disproportionate death rates of Black Women and children is a crisis worth resolving. In that case, this too falls under a category we can expect Black women to advocate for, which benefits my study in two ways: (1) It is realistic to expect Black women to advocate for maternal health policy positions and (2) Doing so, in turn, benefits the protections of white women’s birthing experience. With the presence of a Black candidate potentially activating racialized attitudes regardless of policy position (Tesler 2012), this study is interested in if exposure to different identity-salient framing of health care would mitigate the extent of racial resentments negative impact, and/or tap into a gendered consciousness that translates into material support for Black women candidates and the policy they advocate for.
Research has shown that social identities such as race and gender shape how individuals perceive themselves and, in turn, influence political behavior (Green et al. 2002; Huddy and Terkildsen 1993; Tajfel and Turner 1986). Scholars have also observed that activating salient social identities can affect policy perceptions and motivate political action (Chong and Druckman 2010; Klar 2013; Winter 2008). Indeed, some argue that social identity often serves as a primary driver of mass political behavior (Achen and Bartels 2016). In survey experiments, framing is a mechanism in which social identities can be made salient, as framing a policy or agenda can help orient how people evaluate it (Chong and Druckman 2010; Entman 1993). Emily Diamond found that presenting a frame on the impact of climate change on future generations was particularly effective in influencing policy support for parents (Diamond 2020). For this survey experiment, I present frames designed to elicit in-group gender 7 salience and highlight shared experiences related to birthing.
To ensure that respondents received strong signals of the Black women politicians’ gender and racial identity, respondents were exposed to her description that included being the first Black woman mayor of Bowdain, North Carolina, her attendance at a Historically Black College and University (HBCU), and her identity as a mother of three young children. To avoid any bias on perceptions of skin, hair, and overall appearance, a picture wasn’t provided for the descriptor.
While partisanship was also strategically omitted from the candidate descriptor, it is reasonable to expect that some respondents may have inferred that the fictional candidate was a Democrat based on the broader political context. Not only do Black women voters overwhelmingly support the Democratic Party, but in 2020, there were 98 Black women congressional candidates registered as Democrats, compared to 31 Black women Republicans. Thus, Black women Democrats outnumbered their Republican counterparts by approximately 216% (CAWP citation). At the same time, Republican women candidates often rely on rhetorical appeals to family and motherhood (e.g., Sarah Palin) and emphasize their identities as mothers, much like the fictional candidate in our experimental design (Greenlee 2014). Given these dynamics, we concluded that explicitly identifying the fictional candidate as either a Democrat or a Republican would unnecessarily constrain respondents’ evaluations and believe that assessing appraisals of Black women candidates and their nonpartisan policy agenda is best accomplished without specifying their partisan affiliation.
After reading the candidate description, respondents were prompted to read one of four policy platforms Johnson articulated at a recent mayoral forum. The candidate description was held constant across conditions, while the policy platform varied according to the randomly assigned treatment.
My independent variable is the identity of Carolyn Johnson as a Black woman mayor and the policy positions she advocates for. My dependent variables are (1) support for the candidate and (2) support for the policy. 8 Suppose Carolyn Johnson receives greater support in the maternal health domain than the general health care one. In that case, there’s something meaningful to be said about women’s issues having the capacity to galvanize white women voters, even if posited by a racialized candidate. The extent to which they would support Carolyn Johnson over a white women candidate positioning the same agenda is not discussed in this experiment, but an avenue worth exploring should this be what I find. Should this not be what I find, theories surrounding the lack of support for Black women candidates are arguably sustained, because even policy agendas that are non-racialized in framing and speak specifically about interests that concern all women, couldn’t overcome white women’s historical aversion to supporting Black women candidates.
Experimental conditions by racial and gender prime
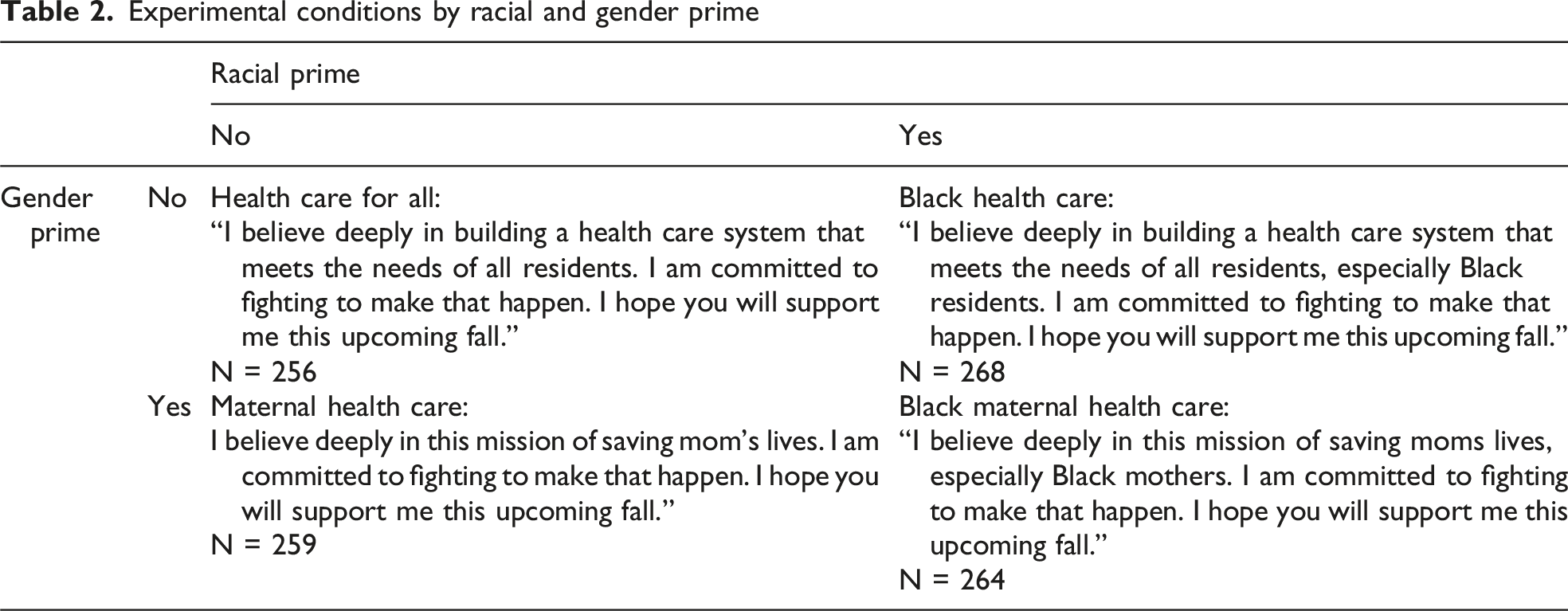
The statement presented in Table 2 represents the closing appeal associated with each policy vignette. The language used in these statements was adapted from mayoral debate transcripts analyzed in prior research and was designed to reflect the style and substance of local campaign rhetoric. The full text of each policy vignette is provided in the supplemental materials.
Once exposed to one of the four conditions with the corresponding policy vignette, respondents were prompted to answer questions about their favorability for the candidate, overall approval of their platform and their perceived knowledgeability and/or competence. These conventional battery questions were measured using appraisal items commonly employed in political behavior research and the American National Election Studies (Funk 1996, 1997; McGraw 2011). 9 Additionally, respondents’ support for the policy agenda themselves were measured by their responses to “How much do you agree with Carolyn Johnson’s position on the issue?” Responses were measured on a scale of 1–4 (1 = Strongly Agree | 4 = Strongly disagree), averaged, and compared across experimental conditions.
Results
With a total sample of 1,047 responses 10 I summarized and analyzed the data using R Studio. The population was a nationally representative sample of white women with an average age of 44 and moderate political identity, leaning Republican. The white women in my sample were married and with an average income between $40,000 and $49,000. 11 Like previous scholarship, I found racialized attitudes to be the most significant explanatory variable, but my findings suggests that something interesting is also happening with gender.
While all policy positions produced less favorable results for the Black women candidate than health care for all (control), findings presented below in Figure 1 suggest that the two racially-oriented positions correspond to the lowest levels of political favorability for Carolyn Johnson, with both racial treatment variables being statistically significant.
12
Relative to the control condition, support for the Black woman candidate declined significantly when she endorsed a Black health policy (95% CI [−0.527, −0.017]). Support also declined when she endorsed a Black maternal health policy (90% CI [−0.478, 0.034]). This suggests support for H1c and marginal support for H1d. Candidate support. Note. Figure represented with 95% confidence intervals, n = 1,047.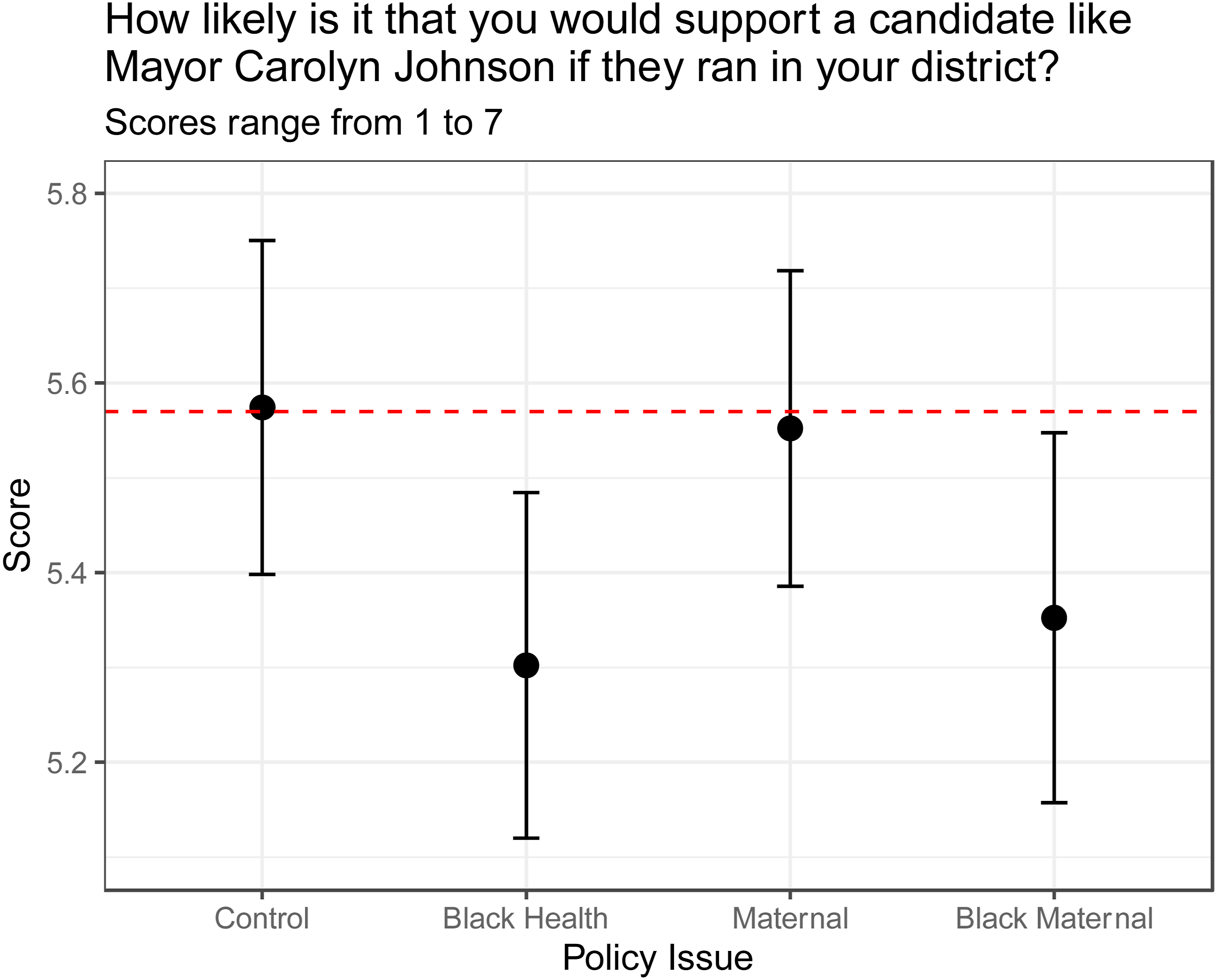
Since the scores are above 5, a facile viewing of these responses may suggest tension with foundational theory, 13 but I would underscore that, without an alternative candidate for the respondents to rate, we cannot make any claims regarding relative favorability of other hypothetical candidates (put differently, the respondents may very well be predisposed to rating candidates on the higher-end of the 1–7 scale). 14 What we can assess is how support varies across issue frames, using health care for all, an agenda historically favored among women voters and one that is neither racialized nor gendered, as a reference category.
Among the experimental conditions, we can also see from Figure 1 that support for a Black women candidate is strongest amongst respondents exposed to the maternal health treatment. However, the estimated effect of the maternal health treatment was substantively small and statistically insignificant (95% CI [−0.279, 0.235]), indicating that support did not differ from the control condition. Therefore, H1a is not supported.
When asked about their views toward the policy position, as illustrated by Figure 2, respondents still appeared most favorable toward the maternal health policy. However, the maternal health policy was once again not statistically distinguishable from the universal health care control condition (95% CI [−0.105, 0.160]). Likewise, neither the Black Health (95% CI [−0.177, 0.085]) nor the Black Maternal (95% CI [−0.189, 0.074]) policies produced statistically significant differences for policy support. Policy support. Note. Figure represented with 95% confidence intervals. n = 1,047.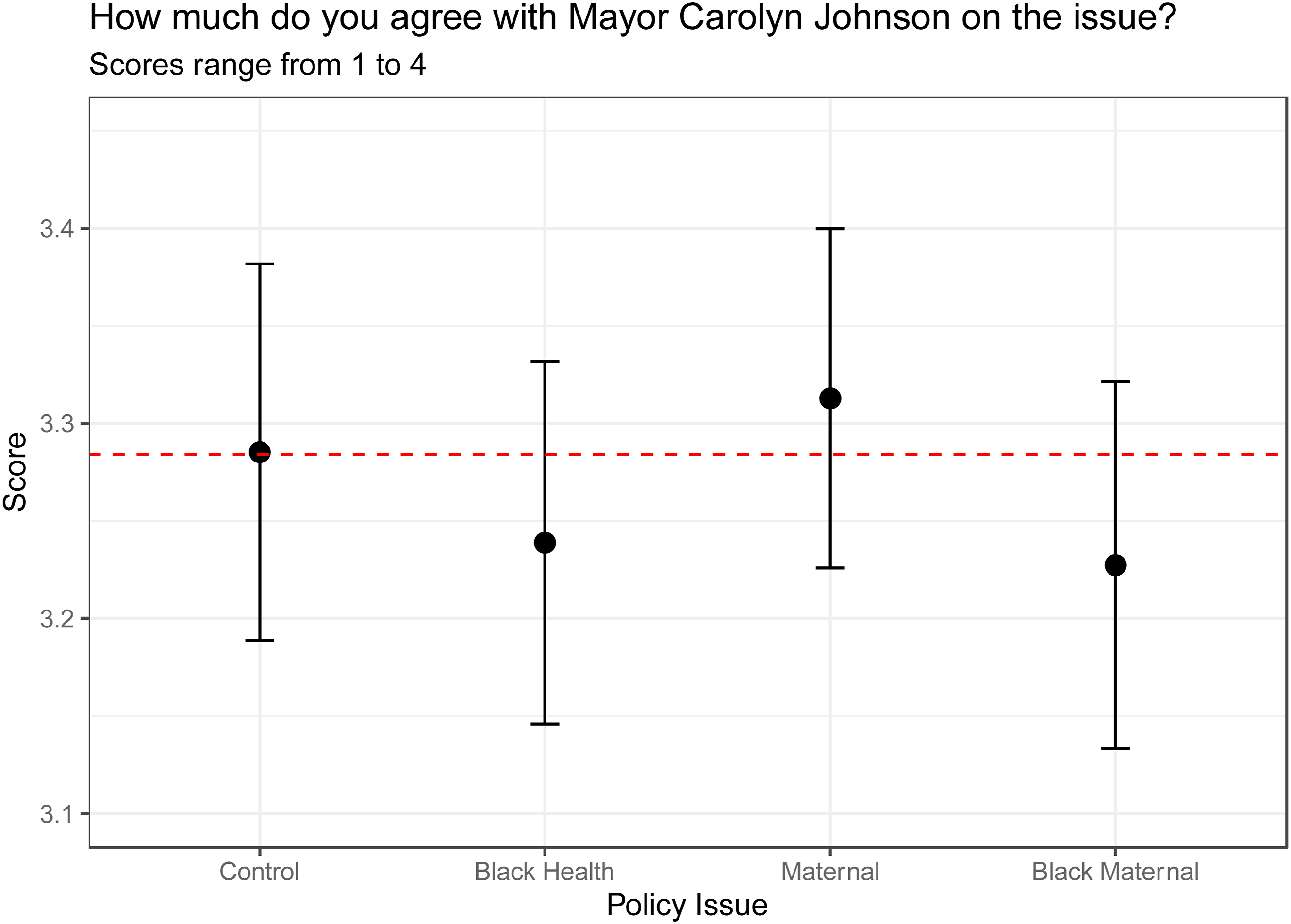
These findings suggest that white women respondents evaluated the policy proposals advanced by a Black woman candidate similarly, regardless of whether those proposals were framed as universal, gender-specific, or race-conscious initiatives.
Results for the remaining dependent variables illustrated in Figure 3 below remain mixed, with the gender-specific maternal health condition continuing to emerge as the most favorably evaluated condition but continually failing to reach statistical significance and therefore does not support H2a. Candidate and policy support by experimental conditions. Note. Results displayed in Figure 2 reflect the OLS regression coefficients of each group across the dependent variables. The bars show the 95% confidence intervals.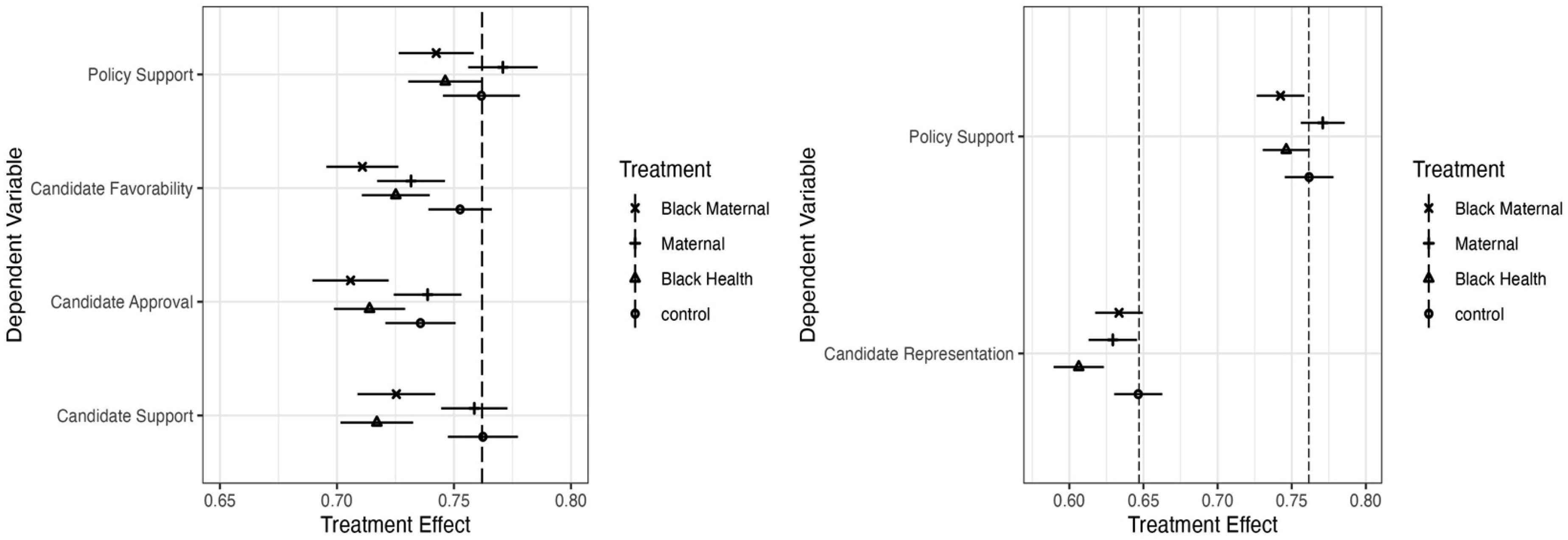
By contrast, Black health and Black maternal health consistently fall to the bottom, never surpassing the control condition. In fact, the only statistical relationship observed in some of the dependent variables emerge in the racialized policy conditions, most clearly reflected in the dependent variable measuring support for the Black woman candidate (Figure 1).
Taken together, these findings suggest that white women’s evaluations of Black woman candidates were shaped more by backlash to race-specific policy appeals than by support for gender-specific policy appeals. Levels of support for the gender-specific condition were not statistically distinguishable from the control condition. In contrast, the largest declines in candidate support occurred when the candidate advocated for policies explicitly targeting Black health and Black maternal health disparities, suggesting a stronger negative reaction to race-conscious policy framing.
As mentioned, although support for the maternal health condition was not statistically significant, respondents nevertheless rated it as the most favorable policy position overall. Yet, for some outcomes, such as when respondents were asked whether “Mayor Carolyn Johnson has the ability to represent your interests,” the only statistically significant effect was the negative impact of the Black health condition. 15 Notably, the intersectional Black maternal health frame was no longer significant in this model. This pattern raises the possibility that respondents may be reacting differently to purely race-specific cues than to gendered or intersectional ones, prompting further examination of the underlying attitudinal mechanisms driving these evaluations. To better understand what may be shaping these response patterns, I incorporate additional analyses using established measures of racial resentment and gender consciousness.
Using a composite score for racial resentment on the X-axis and a composite score of support for the Black woman candidate on the Y-axis, Figure 4 plots the interaction between racial resentment and candidate support across the four versions of the health care frame. As expected, racial resentment is a strong and consistently negative predictor of support for the Black woman candidate. However, the slope of this relationship varies modestly by treatment. Interaction of racial resentment.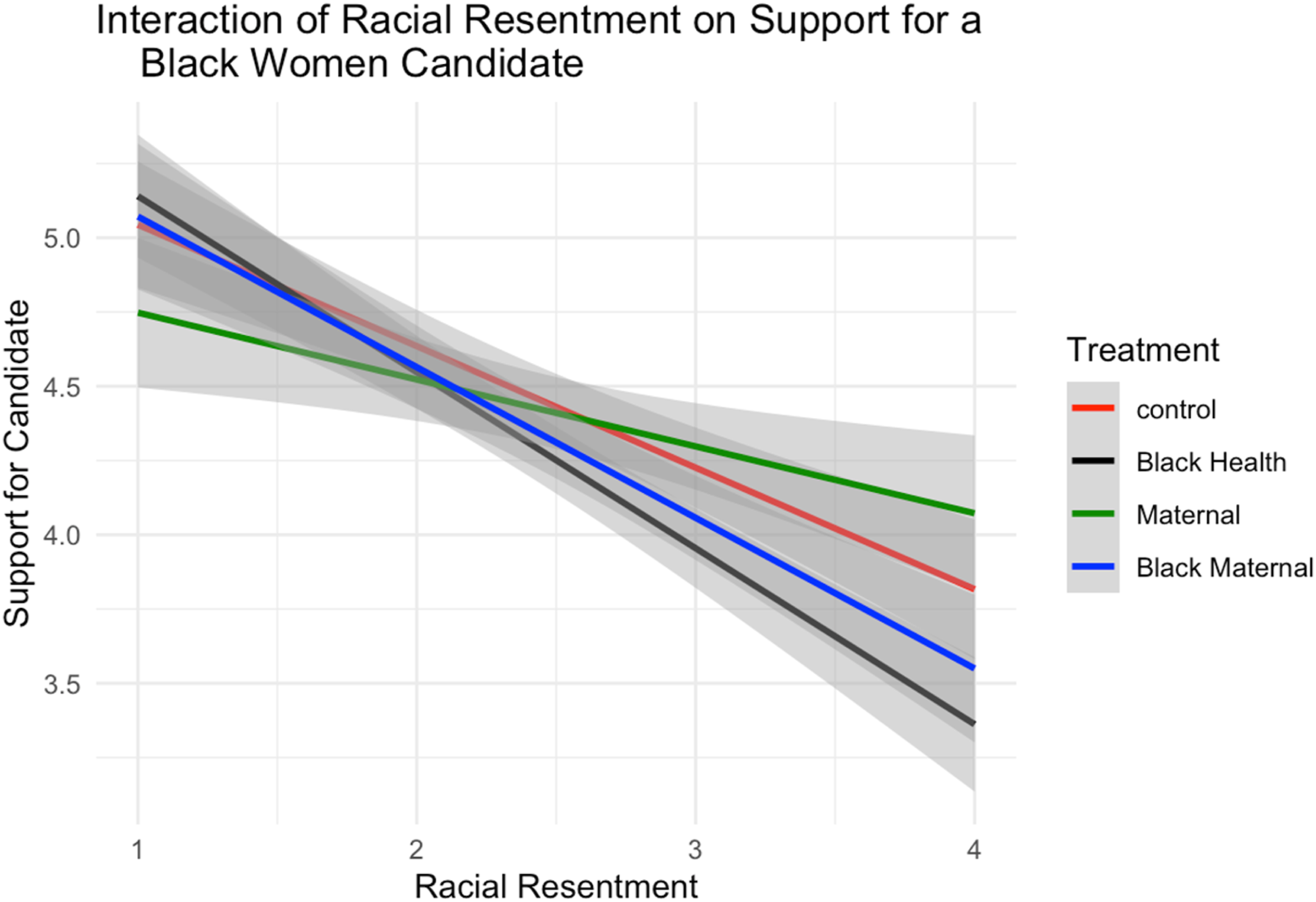
The maternal health frame produces the least negative association between racial resentment and support, but the interaction term is small and statistically insignificant, indicating that this frame does not meaningfully alter the impact of racial resentment in either direction. By contrast, the explicitly racial frame (Black health) significantly strengthens the negative effect of racial resentment on support. The intersectional frame (Black maternal health) falls between these two: its interaction term is negative but not statistically distinguishable from zero, suggesting only a marginal, or at best ambiguous, intensification of resentment’s effect. Taken together, these patterns imply that while explicitly racialized policy cues amplify the influence of racial resentment, adding a gendered component softens that amplification slightly. For white women respondents, maternal language may introduce just enough gendered resonance to reduce (though not eliminate) the heightened penalty associated with racialized frames.
To probe this gendered dynamic further, I next examine an interaction between treatment condition and gender consciousness. While standard measures of gender consciousness were included in the survey, prior research suggests that these scales often capture liberal feminist ideology rather than a broader sense of gendered identity (Klatch 2001; Schreiber 2002). To avoid producing a measure that would disproportionately reflect liberal attitudes and risk alienating conservative women, I constructed a composite score using two items that tap a wider range of gendered meaning-making. To assess whether gender matters in respondents’ political lives, participants were asked: “When you make political decisions, how important is your gender identity?” To gauge the extent to which respondents perceive a shared fate or collective identity among women, they were asked: “How much would you say that women in this country have a lot in common with one another?” 16 The average of these items forms the composite measure of gendered consciousness used on the X-axis, with the composite support measure on the Y-axis.
Figure 5 shows that respondents with stronger gender consciousness tend to evaluate the Black woman candidate more positively. Gender consciousness then serves as a strong and positive predictor of support. However, unlike racial resentment, this relationship is relatively stable across treatment conditions. None of the treatment interactions reach conventional levels of statistical significance relative to the control frame. The only condition approaching significance is the race-and-gender treatment (Black maternal health). Rather than activating a cross-racial gendered solidarity, my findings suggest that this intersectional cue marginally dampens the otherwise positive association between gender consciousness and candidate support. Interaction of gender consciousness.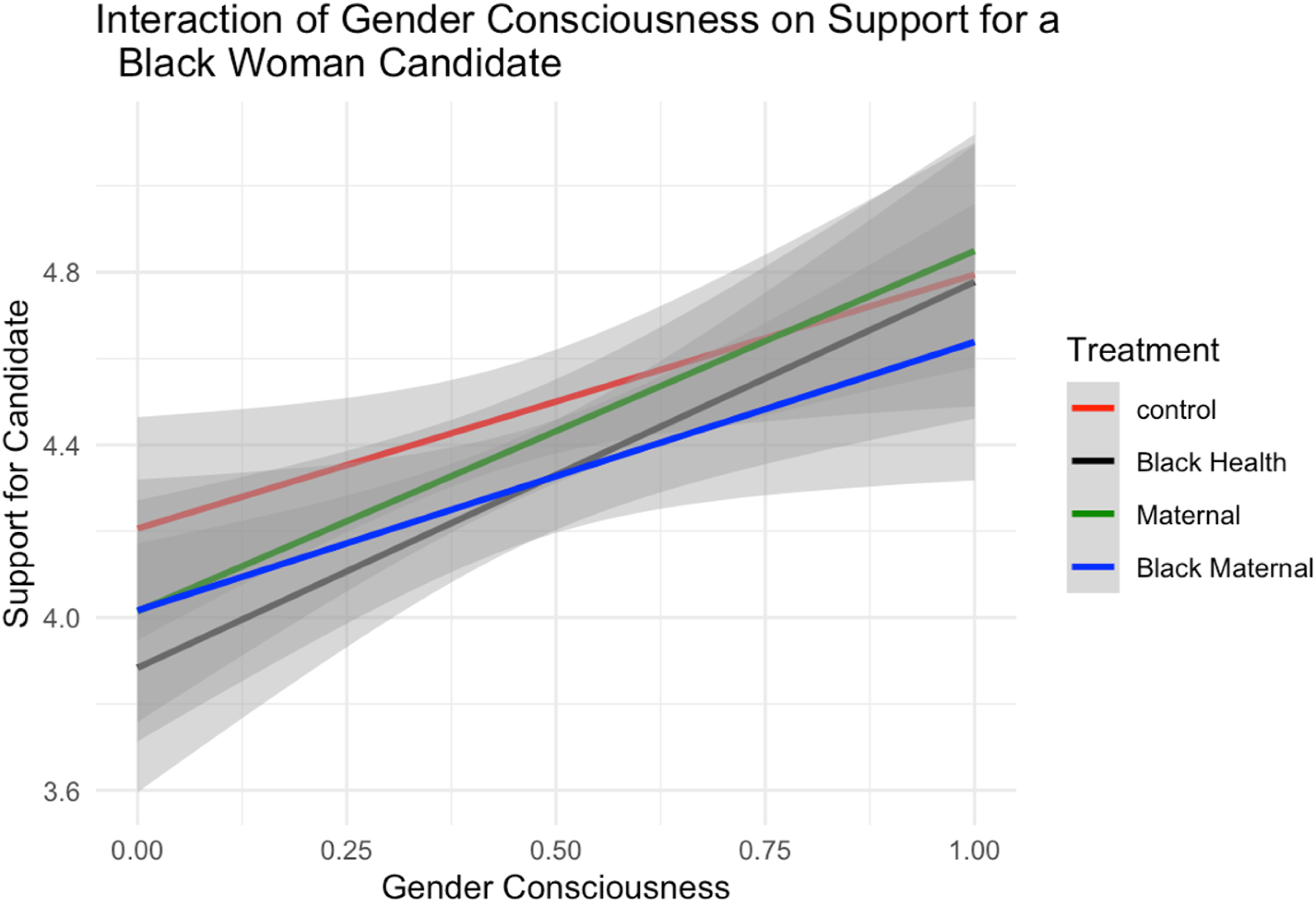
Discussion
While the existing literature has explored how racialized and non-racialized policy arenas are vulnerable to backlash and white racial animus (Gilens 2009; Hurwitz and Peffley 1997, 2010; Kam and Burge 2019; Kinder and Sanders 1996; Piston 2010; Tesler 2012), there has been limited knowledge on the role of gender dynamics within these policy arenas. Studies have made clear that gender alone does not have the mobilizing effects that race and/or race consciousness has (Dawson 1994; Gurin 1985; Philpot and Walton 2007) or a Black feminist consciousness (Simien and Clawson 2004). However, when a Black woman candidate, whose existence is both racialized and gendered is advancing a policy agenda, it would be naïve to think the only identity at play in the electorate’s evaluation is racial. Intersectionality theory makes clear that Black women’s racial and gendered identity is inextricable (Brown 2014a; Gay and Tate 1998; Simien and Clawson 2004). Integral to this paper is understanding if, and how, the gendered identity of a Black leader can influence policy support, or if we can expect a spillover effect similar to what Tesler observed with Obamacare (Tesler 2012). 17 Another, perhaps more important, aim is to explore if a policy that is gendered and beneficial to the in-group (all women and birthing people) can supersede these racialized effects and garner support from white women.
Throughout the research process, I was challenged to think deeply about how abortion, and the thorny feelings it conjures, could potentially impact white women’s attitudes toward maternal health policies. Consequently, I was hyper-cognizant of the language I used when designing this survey experiment. There’s enough literature to suggest that maternal health is often decoupled from abortion and, in fact, frequently anchors conservative arguments against abortion. Anti-abortion feminists during the late 1960s and 70s began making arguments against the feminist movement, claiming abortion produced greater harm for women and that violence 18 “is a violation of basic feminist principles” (Oaks 2009). Moreover, anti-abortion feminist organizations like the Susan B Anthony List, Feminists for Fetal Life (FFL) and the Concerned Women for America (CWA) posit that all women have the right to life, including the fetus (Markowitz 1990; Schreiber 2002). Further, they are gender conscious in their aversion for abortion (Schreiber 2002). I argue that this “maternal” language circumvents these criticisms because it orients the mind around mothers and/or childbirth, and, notably, centers life-affirming care, rather than narratives of sterilization and freedom of choice that are typically associated with abortion.
To that end, maternal health framing acknowledges the feedback that Black feminists and reproductive justice scholars have provided—which takes on a wide range of issues rather than one that is unidimensional and often polarized. bell hooks claims “While the issue of abortion was and remains relevant to all women, there were other reproductive issues that were just as vital which needed attention and might have served to galvanize the masses”. While social science and health scholars are still fighting to decouple the term “reproductive rights” and justice from “conjuring up preconceived thoughts and beliefs that have become even more polarized” (Onwuachi-Saunders et al. 2019), the “maternal” association with health does not harbor similar sentiments.
This study is limited in its scope for a few reasons. First, it relies on the responses of white women who have access to CloudResearch. While the platform considers its scope to be nationally representative, there is a skew towards white women on lower end of the socioeconomic spectrum. Future research would couple these experimental findings with other methods of investigation like polling data and interviews to make more robust claims on the role gendered policies play in evaluating Black women candidates. For researchers who are similarly interested in exploring gendered consciousness amongst white women, my research suggests a gendered policy position may slightly attenuate the extent of racial resentment’s negative impact on support for non-white candidates. However, whether this mitigating effect can underpin meaningful outcomes for Black women candidates remains up for debate.
I would be remiss if I didn’t connect these findings to the political strategies of Black women candidates and the broader implications for coalition building. Both Hillary Clinton in 2016 and Kamala Harris in 2024 made concerted efforts to galvanize white women voters. However, Kamala Harris and the Democratic Party adopted a new strategy in 2024: to target the perceived “silent majority” of white women who hold political views that diverge from those of their husbands.
To reach this group, the Democratic Party made explicit appeals warning that a second Trump presidency would worsen conditions for Americans, particularly regarding gender equality, reproductive rights, and access to health care. These appeals sought to evoke concern and political consciousness among white women, encouraging them to align with a party invested in protecting women’s liberties, even if doing so meant breaking with their conservative partners. 19
In highlighting Kamala Harris as the candidate to support, former First Lady Michelle Obama said to attendees in Kalamazoo, Michigan, a predominantly white district in a key battleground state: There’s more at stake than just protecting a women’s choice to give birth…A women’s body is complicated business y’all. Yes, it brings life and that’s a beautiful thing, but even when we are not bearing children there is so much that can go wrong in any moment. Every woman here knows what I’m talking about.
Here, Mrs. Obama appeals to a shared understanding of the female body, hoping to galvanize white male voters to recognize what’s at stake for the women in their lives. Implicit in this approach is the assumption that white women are already persuaded.
This strategy directly aligns with the theoretical framework of my experimental design. My findings suggest that such language could reduce the negative impact of racial resentment on support for Black women candidates. Yet, empirically, the 2024 election demonstrated that this strategy had a negligible impact in expanding Kamala Harris’s vote share. With the rejection of H1a, my findings in this manuscript mirror this reality.
As more Black women politicians seek and win elected office, and as candidates consider adopting campaign strategies similar to Harris’s, I hope this study contributes to a broader body of work that offers insight into how race-conscious, gender-specific, and intersectional approaches may perform across different political contexts.
Supplemental Material
Supplemental Material - Women Representing Women: Maternal Health Advocacy and the Limits of Gendered Solidarity
Supplemental Material for Women Representing Women: Maternal Health Advocacy and the Limits of Gendered Solidarity by Andrene Z. Wright-Johnson in Journal of Applied Gerontology
Footnotes
Acknowledgments
The author gratefully acknowledges the Center for the Study of Diversity and Democracy (CSDD) and the participants in the Racial and Ethnic Politics Lab at Northwestern University for their valuable feedback and support throughout the development of this project. The author is especially grateful to Alvin Tillery, Tabitha Bonilla, Matthew Nelsen, and Amanda D'Urso for their continued guidance and thoughtful comments. The author also thanks Ray Block Jr., LeAnn Banaszak, the participants in the American Politics Workshop at Penn State University, the Institute for Research on Race and Public Policy (IRRPP), and the anonymous reviewers at PRQ for their care and constructive feedback.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.