
Abstract
Technology use in the practice of couple and family therapy has many advantages. The use of online and technology-based modes of communication for therapy, however, presents several valid ethical concerns. In a survey of 226 licensed Marriage and Family Counselors, students, and supervisors, participants were asked to identify ethical concerns and drawbacks of online therapy. Five themes related to this topic emerged: (a) confidentiality, (b) impact to the therapeutic relationship, (c) licensing and liability issues, (d) issues related to crises and risky clinical situations, and (e) training and education. Implications for practice, training, and research are discussed.
Telehealth is an emerging practice among both medical and mental health disciplines. A proportion of the recent growth in telehealth may be due to the increased availability of technology, pressure on health care to become more efficient and affordable, and a mandate to provide equal access to health care (Baker & Bufka, 2011; Perle, Langsam, & Nierenberg, 2011). Online therapy is one common form of telehealth, which is defined as “the use of telecommunications and information technology to provide access to health assessment, intervention, consultation, supervision, education, and information across distance” (Nickelson, 1998, p. 527). It is defined by Dielman et al. (2010) as the “transmission of images, voice and data between two or more health units via telecommunication channels, to provide clinical advice, consultation, education and training services” (p. 12). The National Board for Certified Counselors, Inc. (NBCC, 2008) classifies telephone, Internet, video, e-mail, and chat-based counseling underneath a broad definition of “technology-assisted distance counseling” (n.p.). All modes of this type of mental health treatment share a commonality in that they use either the phone or computer to help therapists and clients communicate. The definition of online therapy, however, may be broadened to include not only synchronous forms of communication (i.e., Skype or Internet chatting) but also to include asynchronous modes such as texting and e-mailing (Hertlein, Blumer, & Smith, 2014).
The use of online practices in psychotherapy, referred to henceforth as online therapy, has several advantages. Barak, Hen, Boniel-Nissim, and Shapira (2008) found online therapy is nearly as or as effective as traditional face-to-face therapy. In particular, online therapy has been found to be effective in treating depression (Mohr, Vella, Hart, Heckman, & Simon, 2008), particularly when access to other providers is limited or to prevent relapse (Garcia-Lizana & Munoz-Mayorga, 2010; Moreno, Chong, Dumbauld, Humke, & Byreddy, 2012), panic disorder (Carlbring et al., 2006), and a host of other presenting problems (see, e.g., Andersson, Estling, Jakobsson, Cuijpers, & Carlbring, 2011; Blankers, Koeter, & Schippers, 2011; Wooton, Titov, Dear, Spence, & Kemp, 2011). Online therapy may also be advantageous in rural areas where access to counseling centers is limited, as well as circumstances where clients are homebound due to physical or psychological illness (Hertlein et al., 2013). Couple and family counselors, as well as other mental health professionals, may find online therapeutic practices more convenient because it often allows for accommodation of hectic or inflexible schedules, as well as a tool for scheduling and appointment reminders.
Despite the effectiveness and convenience, the use of online modes of communication for psychotherapy presents some equally valid ethical concerns. One ethical concern is the assurance of confidentiality (Derrig-Palumbo & Eversole, 2011; Nelson, 2010), characterized by both visual and auditory confidentiality concerns (Nelson, 2010). Auditory concerns are related to cell phone use; as one can carry on conversations with clients at virtually any time, there may be a breach in confidentiality when others nearby can overhear the conversation. Visual concerns emerge when counselors do not protect their computer or tablet screen, provide passwords to others, or use a shared computer. Counselors who conduct services online must weigh potential treatment benefits and ethical risks of saving chat transcripts or e-mail chains, which may contain protected client information. In addition, clients must be made aware of the benefits and risks of electronic communication and therapy via informed consent (Nelson, 2010).
A second issue discussed in the literature is boundary management (Hertlein et al., 2014). With the growing presence of social networking such as Facebook, MySpace, and chat rooms, all participating parties may enter unintentionally into dual relationships or make unintended personal disclosures (Nicholson, 2011). Similarly, if a counselor and client were to become “friends” on a social networking site and subsequently see a photo or post that contradicts information the client reported during a session, counselors have to make decisions about what to do with the information. Further, other friends on a counselor or client’s friend list may become curious as to the relationship between the counselor and client, potentially breaching confidentiality.
A third issue is the management of crises. Counselors must discern which of their clients are appropriate for online therapy. This includes assessing a prospective client’s ability to recognize and respect boundaries, severity of client problems, diagnostic information, and whether the client is suicidal or homicidal (Chester & Glass, 2006; Perle et al., 2013). Further, counselors must consider how and to whom they will report if a client plans to harm themselves or others, and be able to refer clients to emergency services in their zip code. Mandatory reporting may become a tricky issue when conducting online therapy in a different state than the client, as the question arises as to which state the counselor reports and whether it is ethical to be conducting online therapy outside of the state of licensure (Derrig-Palumbo & Eversole, 2011).
Previous Literature on Managing Ethical Issues
Maheu and Gordon (2000) conducted one of the earliest studies on the counselor’s use of technology with clients. They found 78% of their counselor participants (93% of which were licensed to provide counseling services) reported providing services via online mechanisms to a client in another state. Although 60% indicated they checked the state law where the client was located, nearly three quarters of them (74%) were wrong or uncertain about the state regulations. Further, 48% of the participants indicated they used a consent form prior to the initiation of treatment.
A similar study was recently conducted of psychologists’ usage of online treatments. A sample of 409 licensed psychologists and 308 doctoral-level students responded to items regarding their perceptions of online therapy (Perle et al., 2013). The researchers focused on identifying whether variables such as theoretical orientation, age of the psychologist, and extent to which online practices are involved in treatment (i.e., adjunct to treatment vs. sole treatment modality) affected a psychologist’s utilization of online therapy. Findings indicated psychologists who operated from a cognitive–behavioral stance or systems orientations were more likely to adopt online therapy practices as compared to those who practiced from an existential or dynamic perspective. There were no significant differences between students and licensed professionals with regard to adoption of online therapy practices.
Given the vast nature of providing online services in lieu of information regarding how best to do so (Maheu & Gordon, 2000), and in consideration of Perle et al.’s (2013) contention that many of the ethical issues related to telehealth have been resolved over time and with research, the purpose of this study was to evaluate Marriage and Family Counselors’ (MFTs) perceptions related to the ethics of conducting online therapy, including a valuation of the specific benefits and drawbacks related to ethical concerns.
Method
This study was an exploratory mixed-methods approach (Gambrel & Butler, 2013). Survey data (both open and close-ended questions) were collected from a sample of part- and full-time counselors, and students in MFT programs. Participants were recruited in three main ways: (a) Internet postings (through social media such as Facebook, organizational posting, etc.), (b) advertisements at the American Association for Marriage and Family Therapy (AAMFT) divisional level, and (c) couple and family therapy–themed conferences. We also e-mailed program directors of Commission on Accreditation for Marriage and Family Therapy Education (COAMFTE)-accredited programs and asked them to distribute the survey link to their faculty and students.
We estimated this recruitment procedure may have put us in contact with nearly 2,000 potential participants, resulting in 226 participants for this study. Participants were invited to primarily complete the inventory online (Questionpro.com®). There were two groups, however, who had the option of completing a paper version to be entered into the online tool by an assistant: those who received the request at conferences and those at the divisional level to whom the survey was mailed. This research was approved by a university Institutional Review Board and funded by the Alaska Association for Marriage and Family Therapy.
Instrument
The survey tool was composed of Likert-type, multiple choice, and open-ended items, consistent with an explanatory type of mixed-methods research approach (Gambrel & Butler, 2013). The survey contained 51 items and covered a series of topics including information about the participant’s practice, use of cybertechnology in clinical practice, and the use of technology in supervision, education, and training as well as assessing the perception of ethical concerns. In addition to the information related to ethics, participants were asked about the frequency by which they use various technological services, social networking sites with their clients and colleagues, e-mailing to clients and colleagues, and other ways they might use technology with these groups. For a more detailed description of the survey items, see Hertlein et al. (2014). The findings presented here represent a subset of the complete survey tool and focus on counselor perceptions of the potential ethical issues when participating in online therapy practices, and the extent to which guidelines from other organizations, and opportunities for further training would be desired.
Because the findings in the Perle et al. (2013) study contradicted the findings of the Mora, Nevid, and Chaplin (2008) with regard to differences in student versus professional perceptions and practices, data regarding the importance of using other ethical codes to make decisions were analyzed through a t-test to determine whether there was a difference between students and professionals. The analysis with regard to the open-ended items involved noting common phrases within the answer to each prompt following an open and thematic coding process (Merriam, 2002). Each author reviewed the data and identified themes and then compared the themes with one another in order to determine a final list of themes. Specifically, we employed a bracketing procedure (Patton, 2002) for theme identification and then used the analytic inductive-constant comparative method (Glaser & Strauss, 1967) to analyze themes. This was accomplished through reading and rereading the data to compare the themes with what was being presented in the data upon our read throughs, and making suggestions to modifying the themes if necessary. Any disagreements about the themes were settled through conversation and agreement of what the common theme would be. Final categories were the result of this modification process and a last reading of the data to determine if the data still fit with the solidified themes.
Results
Participants who completed the survey included 226 licensed counselors, Marriage and Family Counselors (LMFTs), and AAMFT clinical, students, and approved supervisor members. The sample was predominantly female (n = 176, 79.64%), Caucasian (n = 185, 84%), and AAMFT clinical members (n = 128, 57.92%) who worked in a private practice setting (n = 92, 38%). Approximately 5% (n = 13) of the sample identified as Hispanic/Latin American, 3% (n = 7) as African American/Black, and the remaining identified as American Indian, Alaskan Native, or of Asian descent (n = 15, 6.6%). Just under half of the participants indicated they work in rural areas (n = 110, 48.5%), 39.2% in suburban areas, and 12.3% in rural areas. A full quarter (n = 67, 27.46%) worked in a graduate program, with 39 of these (58.2%) being students. Another 21.23% (n = 48) worked in nonprofit, state, or community agencies. The remaining participants worked in for-profit agencies, medical facilities, and employee assistance programs, and other (n = 37, 16.37%). Just over half of the participants worked part-time in a private practice setting; 44% worked full-time, and eight reported “other” as their employment status.
Perceived Ethical Issues and Drawbacks in Web-Based Treatment
Five themes emerged with regard to the ethical issues and drawbacks that emerge in online therapy: (a) confidentiality, (b) impact to the therapeutic relationship, (c) licensing and liability issues, (d) issues related to crises and risky clinical situations, and (e) training and education. The most frequently cited ethical issue noted by participants was the issue of confidentiality, mentioned by well over half of the participants. Confidentiality included concerns about privacy, concerns about who could view the video or feedback, and authenticity of the user. Participants believed online therapy introduced questions around authenticity of the user, such as “who has access to the computer” and “the [chance] of loss of control of who has the device at the other end,” particularly when that computer is a home computer. One participant asked, “How can the therapist or client be sure no one else is in the vicinity of the computer—that is, how can you assure confidentiality?” In addition to the issue of other persons physically present in the computer room, there is the risk that someone can gain access to another’s account. According to another participant, “confidentiality is a very big consideration given the number of ways to access personal cyberspace accounts.” Others participants raised the concern that counselors may not be providing treatment to the person with whom they think. Confidentiality was also related to the issue of security for some participants. According to one participant, “security online is not guaranteed.” Several participants noted the potential for hackers and described their belief that the less secure the connection, the potential for a breach of confidentiality.
The second theme was impact to the therapeutic relationship. Several participants noted that messages sent may be misinterpreted or misunderstood, thus compromising client care and the therapeutic process. Another issue was the potential for diffuse boundaries between client and counselor. One participant exemplified this by writing there may be “missed information, lost feelings/understanding, lack of intimacy and disclosure.” Another example is provided by another participant who stated that another issue may be “missing key factors of the human experience—social relationships and nonverbal communication.” According to another participant, online therapy “lacks the opportunity for physical human interaction, such as offering a crying client a tissue or engaging in therapeutic touch, which could possibly act as a barrier to joining effectively with clients.”
Participants also characterized the impact to the relationship as one where nonverbal cues and body language would not be as easily read and that subtle cues would be missed. Online therapy was also characterized as one of reduced quality (resulting in “dilute[d] treatment”) due to the lack of face-to-face interactions and “personal connection.” One participant exemplified their concerns in this way: “I am concerned that MFT never becomes an assembly line service through the use of cyber-technologies.” Web-based therapies were also perceived as contributing to greater degrees of difficult in properly assessing clients. In addition to the potential impairment to the relationship in general, the lack of physical presence might impair one’s ability to intervene. As exemplified by one participant: “ … it is more difficult to use body language and positioning to create change and build rapport.” As summed up by one participant, the “quality of service via Skype/e-mail/chat-rooms does not equate to therapy [the] client would receive face-to-face.”
Boundary-related concerns also emerged within the theme of impact to the therapeutic relationship. One participant noted: “client-therapist boundaries may be blurred if client has access to therapist e-mail … ” Participants also cited the potential for dual relationships in that clients might be able to contact their counselors via social media. Also related to boundaries was the decision around “how much to show or share.” Finally, participants reported that the boundary issue might be tied to “over use” of the computer, thus making the counselor more available and risk being perceived as available any time.
A third theme was the potential for having sessions with individuals who are at risk, such as those who are suicidal or experiencing other potential crises. Some of the issues identified within this theme include difficulty in “monitoring self-injurious behavior,” “safety of the client,” and a compromised ability for the counselor to intervene immediately. One participant noted: “if you don’t have the location of the client you are speaking with and they admit to wanting to commit suicide, how do you send help their way?” In addition, participants indicated those participating in online therapy might have difficult properly assessing for risk factors, suicidal or otherwise unsafe clients, and may “[miss] imminent harm.”
The fourth theme was of a professional nature—specifically, liability and licensing concerns. Participants noted concerns related to the 1996 Health Insurance Portability and Accountability Act, record keeping, informed consent, distributing forms and handouts to clients, mandated reporting, and involvement of third-party payers. This may result in issues of, as one participant summed, “credentialing and quality control.” Another issue was the process of conducting interstate treatment as counselors may not be licensed to practice with clients living in another state. One participant exemplified this by stating: “where is the therapy occurring if a complaint is [made? Which] state does it go to?” This theme was also related to the third theme of conducting treatment with individuals at risk. For example, one participant wrote: “if a client has an emergency and you are not accessible, could you be held responsible?”
A fifth theme that emerged was that of the necessity of having proper training and education to deliver and conduct therapies online. Participants cited the mechanics of the computer and that problems may occur with regard to its usage, with some of these tying back to confidentiality. One participant wrote it was important to “[make] sure your cyber connection is secure to maintain confidentiality.” Participants noted the responsibility of the counselor to be knowledgeable about how to conduct sessions over the Internet, including “educating clinicians about using privacy practices, proper use of both personal and professional pages on social media sites.” One example of this is a participant who stated that it was important to assure “all who are required to use the technology are fully trained and can use if effectively.”
Perceived Potential Issues Related to Informed Consent
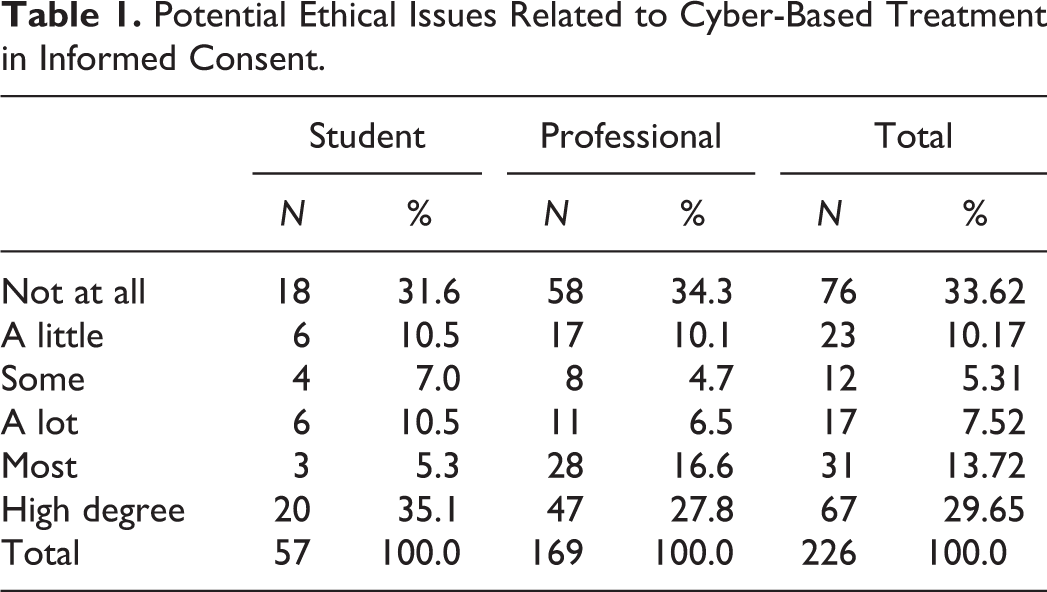
In addition to responses to the open-ended items, participants were asked the extent to which they discuss potential issues related to web-based practices within their informed consent. Approximately one third (33.62%, n = 76) indicated that these issues were not presented at all in their informed consent. Another 10% (n = 23) stated they discussed it to some degree. Nearly another third (29.65%, n = 67) indicated it was included to a high degree in their informed consent (see Table 1).
Potential Ethical Issues Related to Cyber-Based Treatment in Informed Consent.
The Importance of Other Codes When Making Ethical Decisions
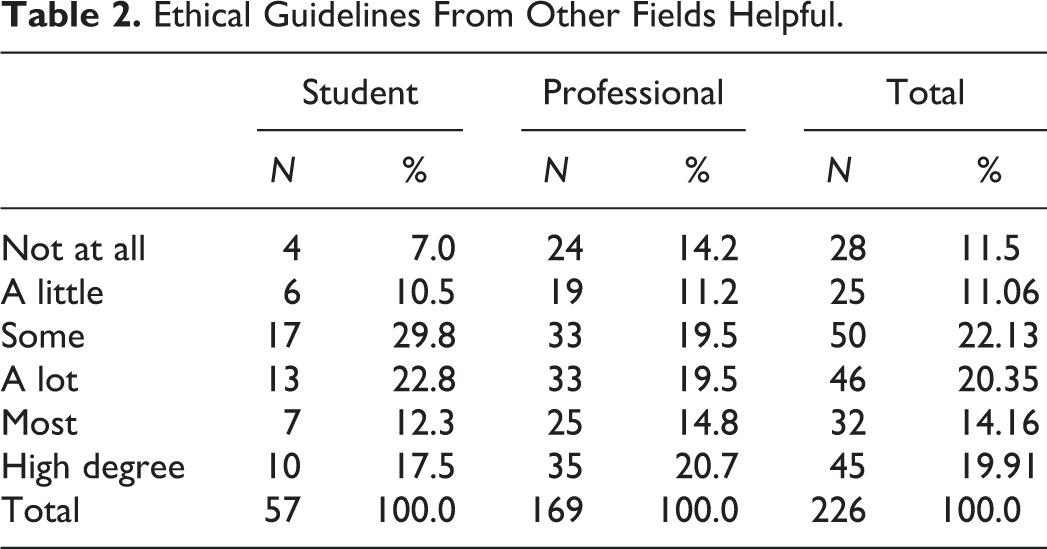
With regard to the total sample (see Table 2), 22% (n = 50) of the sample stated that codes from other disciplines were helpful to understanding how to navigate operating their practice where Internet technologies are concerned. Another 20% (n = 46) found the guidelines helped them a lot, and 34% (n = 77) helped them most of the time and to a high degree.
Ethical Guidelines From Other Fields Helpful.
Based on previous literature citing how younger counselors are less likely to provide telemental health services (Simms, Gibson, & O'Donnell, 2011) and information from the Perle et al. (2013) study comparing student and professional perceptions of online therapy, we hypothesized the student perceptions may differ from those of practicing counselors and performed t-tests to determine whether there were significant differences on this. Further, since there was a rather large difference between students and professionals (n = 57 and n = 169, respectively), we made comparisons using a random sample of the professional sample to reduce the risk of making a Type I error. The final analysis to determine differences in the sample included 57 students and 57 professionals. The results indicated that students differed from professionals on certain variables. Specifically, students were more likely than professionals to agree that ethical guidelines from other fields (i.e., American Counseling Association [ACA], American Psychological Association [APA]) are helpful when making ethical decisions regarding the use of web technologies in practice (M student = 3.63; M professional = 2.96; t = 2.128, p = .036, df = 112). Students also differed from professionals in their interest in becoming certified to specialized in cyber-based practices if that option were to exist (M student = 4.04; M professional = 3.26; t = 2.128, p = .032, df = 112). Students were also more likely to agree with the statement that graduate programs should be teaching more about the use of technology in supervision (M student = 4.32; M professional = 3.51; t = 2.485, p = .015, df = 112) and would be more interested in learning about technology in supervision (M student = 4.32; M professional = 3.40; t = 2.658, p = .009, df = 112). There were no statistically significant differences with regard to how the students and professionals viewed whether cyber-based therapies should be used in rural areas (t = −1.090, p = .278, df = 112), whether cyber-based therapies should be used in urban areas (t = 1.776, p = .078, df = 112), whether cyber-based therapies should be used in suburban areas (t = 1.754, p = .082, df = 112), and whether there are potential ethical issues related to cyber-treatment that are addressed in one’s informed consent (t = .304, p = .761, df = 112).
Discussion
Perceived Disadvantages
One of the clear disadvantages expressed by the participants was the issue of confidentiality and the need to maintain a therapeutic relationship. This is consistent with Maheu, Pulier, McMenamin, and Posen’s (2012) work, which emphasized one of the challenges in using telehealth as the impact on the relationship between physician and patient, as well as issues with regard to confidentiality. Key strategies for managing client privacy, include limiting information on handheld devices, encryption (Mallen, Vogel, & Rochlen, 2005), password protection, and firewalls or a secure Internet connection (Maheu, Pulier, McMenamin, & Posen, 2012).
Another disadvantage and ethical concern mentioned by participants was the issue of who was on the other end of the computer or electronic device. Literature in psychology emphasizes the need to establish a process by which the treating professional identifies that the client is who they purport to be and are able to legally give consent for treatment (Fisher & Fried, 2003). MFTs, like any other mental health professional, need to establish a procedure by which they are able to confirm someone’s age, legal status, and identification prior to engagement in an online therapeutic relationship. This might include passwords for the client, meeting someone face-to-face for the initial session, and using video conferencing as opposed to e-mail (Fisher & Fried, 2003).
Another issue mentioned by participants in the study was liability. This theme emerged related to working with risky clients and potential complaints with concern placed on the counselor’s portion of liability in such situations. One question central to this issue may be establishing whether a therapeutic relationship exists (Barnett & Scheetz, 2003). Barnett and Scheetz (2003) noted two factors that determine whether a therapeutic relationship exists, which are (1) exchange of money and (2) number/frequency of communications. Kluge (2011), however, noted that there might be more to consider in terms of liability; for instance, there can be a question of ownership in the problem liability. Missed cues because of a reliance on online communication may open op both client and counselor to liability. Potential remedies can include the development of an informed consent that includes information of concern with regard to liabilities, and the engagement in online practices that include predominantly structured interventions and/or have been tested and found to be evidence based (Kluge, 2011).
Implications for Training
As mentioned earlier, most of the participants indicated they rarely or never use video calling software or websites with their clients. This finding contradicts the earlier research by Maheu and Gordon (2000), which cited a majority of counselors practice online with out-of-state clients. When combined with the open-ended items in the current study, it seems clear that MFTs believe that training needs to accompany the use of such technologies in practice. One of the issues that emerged from the open-ended items is recognition that MFTs providing this treatment be trained to do so. A similar stance is outlined by the APA in their ethical standards: Standard 2.01c requires psychologists who wish to expand the scope of their practice to techniques or technologies that are new to them to undertake relevant education, study, consultation, or experiences to obtain the qualifications necessary as established by the field. (Fisher & Fried, 2003, p. 104) Finally, the American Counseling Association ethical codes (ACA, 2014) also identify this by stating: Counselors who engage in the use of distance counseling, technology, and social media develop knowledge and skills regarding related technical, ethical, and legal considerations (e.g., special certifications, additional coursework; p. 17).
Yet in the case of MFTs, we acknowledge that we are seeing more of these cases (Goldberg, Peterson, Rosen, & Sara, 2008), yet the training opportunities are lagging behind. In the case of psychologists, over 70% of them were interested in learning more about web technologies in their practice (Perle et al., 2013). This finding was fairly consistent with our MFT sample, where 85.3% (n = 153) indicated they were somewhat interested in learning about web practices. With regard to the AAMFT Code of Ethics (2012), section 1.14 electronic therapy provides general guidelines as to how one may proceed with online therapy. Specific details, however, are lacking to inform the MFT on the ethical considerations involved with this mode of treatment. With the use of video calling, websites, and other forms of electronic communication for therapeutic purposes becoming more prevalent, it leaves one to wonder why the AAMFT 2012 Code of Ethics still lacks precision in how counselors should incorporate technology into practice.
With regard to the therapeutic relationship, participants in our study, as well as in the Nelson (2010) study, described (a) the importance of face-to-face contact with clients and (b) their perception that online therapy detracts from the quality of the therapeutic process. This perception, however, has not borne out in the data (Wade, Wolfe, & Pestia, 2004). In only one study, face-to-face treatment has been preferred over online therapy (Rogers, Griffin, Wykle, & Fitzpatrick, 2009). This topic is specifically addressed within the ACA (2014) ethical codes, where counselors are advised to consider how differences between face-to-face and online counseling might affect the therapeutic process. Counselors should gain more education, and training aimed at bolstering their therapeutic skills and methods by which to provide effective online therapy in combination with reducing fears around online practices as a way to minimize any negative impact to the therapeutic relationship (ACA, 2014).
Implications for Clinical Practice
The most recent iteration of the ACA’s Code of Ethics (2014) highlights specific practice with regard to Internet-based counseling. These include practical guidelines such as how to communication with clients about confidentiality and its limitations in a virtual practice, the importance of verification of the identity of the individual receiving services, and how to ensure that the services provided are effective. In addition, the ACA ethical code identifies the importance of communicating with a client about the presence of social media and the limits and boundaries accompanying use of such technologies.
Currently, there are some ethical guidelines in the most recent AAMFT Code of Ethics (2012) which attend to the role of Internet in practice. One is subprinciple 1.13, dedicated to electronic therapy. It states: Prior to commencing therapy services through electronic means (including but not limited to phone and Internet), Marriage and Family Counselors ensure that they are compliant with all relevant laws for the delivery of such services. Additionally, Marriage and Family Counselors must: (a) determine that electronic therapy is appropriate for clients, taking into account the clients’ intellectual, emotional, and physical needs; (b) inform clients of the potential risks and benefits associated with electronic therapy; (c) ensure the security of their communication medium; and (d) only commence electronic therapy after appropriate education, training, or supervised experience using the relevant technology. (AAMFT, 2012)
Implications for Research
The sample in this study represented a group of MFTs who, by in large, refrained from using technology or web-based devices in their practices. This finding contradicts the findings of Maheu and Gordon (2000) which found that three quarters of practitioners were engaging in some form of web-based practice, primarily without regard to accurate information about state laws regarding online therapy practice. From this lens, their perceptions about the ethical challenges related to the practice of online therapy and web-based communication with clients is limited to those who do not necessarily practice this work. Future research might seek to incorporate the voices of those who are currently augmenting or operating their practice solely through online methods. In addition, because so many of the concerns were related to issues of confidentiality, further research may want to seek efficient and accurate ways to assess a given online system as a way to assist counselors in identifying the most secure channel through which to interact with their clients.
Limitations
This study presents the responses of those who have little practical knowledge about the subject, and therefore provides little new information for the field of MFT. Unfortunately, however, there were not enough MFTs in the study who exclusively used web-based practice as their primary treatment modality. Therefore, we listed our findings as “perceptions” of advantages and disadvantages as a way to demonstrate a higher degree of transferability. In addition, if few of the participants used online therapy, the concerns raised might reflect fantasized drawbacks instead of actual drawbacks, thus inhibiting them from using online therapies as a successful adjunct to treatment. On the other hand, there were several practitioners who indicated that they do not participate in online therapy, yet were clearly using technology in some way with their clients (i.e., texting, e-mail, etc.).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the Alaska Association for Marriage and Family Therapy and parts of it were previously presented at the 2011 Alaska Association for Marriage and Family Therapy Annual Conference in Anchorage, Alaska.