
Abstract
Death and bereavement remain a cultural taboo that continues to impact helping professionals. The death of a child is a particularly difficult loss as it challenges expectations about the life cycle. Many clinicians find themselves unprepared and ill-equipped to appropriately intervene. Bereaved couples require knowledgeable and culturally competent support to facilitate positive and healthy outcomes. The aim of this article is to provide clinicians with a theoretical framework and clinical conceptualization to assess and intervene in the lives of bereaved couples.
Losing a child is considered one of the most important stressors in one’s life, with important impact on the well-being of the parents, at the individual level as well as on their couple relationship (Stroebe et al., 2013). Referred as the “unspeakable loss,” it is a loss untimely, against the order of nature, that encompasses not only the physical absence of the son or daughter but also the loss of a future generational line, loss of dreams and aspirations, and loss of birthdays and graduation celebrations, weddings and emotional transitions to college life, and countless other joyous occasions. Instead, parents are faced with the unbearable task of choosing a casket, make funeral plans to bury their child. No wonder it is considered “one of the most severe, enduring and debilitating forms of bereavement” (Oliver, 1999, p. 198). The aim of this article is to provide clinicians with a framework for conceptualization to assess and intervene in the lives of bereaved couples.
Literature Review
Parents’ assumptions about life’s meaning, fairness, and safety may be shattered (Janoff-Bulman, 1992); their sexual lives may be impacted (Dyregrov & Gjestadt, 2011; Hagemeister & Rosenblatt, 1997); and the way they cope with the loss will have an impact on their relationship satisfaction (Barrera et al., 2007; Dyregrov & Dyregrov, 1999; Dyregrov & Gjestadt, 2011; Esakow & Miller, 2013; Gilbert, 1996, 1997; Hagemeister & Rosenblatt, 1997; Hooghe et al., 2018; Lang et al., 1996; Lohan & Murphy, 2006; Reilly-Smorawski et al., 2002; Wing et al., 2001). While the majority of researchers agree that losing a child has an impact on the couple, Lang et al. (1996) argue that the quality and the dynamics of the relationship prior to the loss may have an impact on parents’ grief responses and then on their relationship.
Gilbert (1996, 1997) focuses on differences and similarities in the grieving process and how they can impact the couple relationship both positively and negatively, contributing to either an increased intimacy or to disconnection between partners. Gilbert (1996) argues that when grieving a shared loss, people may make different meanings but still have the expectation that the way they grieve should be similar. For example, one of the partners may deal with grief by focusing more on work projects, while the other finds it hard to focus on work and is more oriented on loss tasks (Stroebe & Schut, 1999). This dynamic can create conflict as some partners find it hard to accept a different style of grieving as being authentic or enough.
Furthermore, Gilbert (1997) highlights areas where parents may differ in the way they understand each other’s grieving and that can create conflict: what is the right way and amount of grieving, “being out of synch,” family goals and roles, and disagreements over what/whom to blame for the death of their child. These aspects contribute to a lack of responsiveness and availability in meeting the other partner’s needs while grieving, which can affect emotional and sexual intimacy and in turn erode the couple’s bond. However, Gilbert noted that synchronous grieving does not guarantee couple satisfaction. When both partners are more focused on loss tasks (Stroebe & Schut, 1999), it is difficult to be present for each other and to give and receive comfort when needed. The author suggests that open communication, intellectual intimacy, sharing the loss through the ability to develop a shared view of it, expressing emotions together, flexibility, and sensitivity and care for each other’s needs may bring partners together and improve intimacy.
More recently, Essakow and Miller (2013) found that mutual understanding of different grieving styles rather than synchronous or incongruent grief (Gilbert, 1996, 1997) contributed to adaptively cope with grief in couples who lost a child. Supporting emotional expression in each partner as well as allowing the need to distance one’s self from time to time was considered very important. The authors find that partners needed to be able to look away from the other and turn more inward in their mourning while having the acceptance and patience of the other. Moreover, they both needed to distance themselves from the pain and focus more on the future of their relationship together as well as look at each other and have a sense of togetherness. “Moving forward was seen as an important need in healing. Moving forward with one another was a major source of comfort and protection” (Essakow & Miller, 2013, p. 306). Similarly, Hooghe et al. (2018) found that both being able to talk and emotionally attune to each other as well as being able to maintain a bearable distance from grief and from each other were identified by couples as being essential for coping with grief after losing a child.
Some studies found gender differences in the way parents grieve (Barrera et al., 2007; Dyregrov & Dyregrov, 2017; Lang et al., 1996; Lohan & Murphy, 2006; Schwab, 1990, 1992; Stroebe et al., 2001; Wing et al., 2001). In these research studies, wives in heterosexual couples were found to be more willing to talk about their grief and to express emotional needs than husbands who were more withdrawn emotionally and felt the need to be strong for their wives. The interplay between the male partners’ frustration with the female partners’ grief and the women’s anger over the men’s withdrawal can lead to both being unable to offer each other the comfort and support needed and in turn decrease couple satisfaction with their relationship.
Sexuality is another important aspect of the couple relationship that seems to be impacted by the loss of a child. Several studies focused on this impact (Dyregrov & Gjestad, 2011; Hagemeister & Rosenblatt, 1997; Schwab, 1992). A common result is the founding of a decline in the frequency of sexual intercourse between bereaved couples. There were several reasons that were identified for the decline: intercourse as a painful reminder of their loss, fear of pregnancy, and consequently losing another child. These studies also show that generally male partners were looking more for sexual intercourse as a comforting coping strategy than females. Many women described how physical closeness more than sex had become central in their relationship, but that men easily misunderstood this as a desire for sex. Men, however, looked at sex as a tension reliever and attributed a therapeutic value to it. Both genders could also feel that sex was a sort of life confirmation. (Dyregrov & Gjestad, 2011, p. 311)
Grief Framework
The dual process model (DPM) developed by Stroebe and Schut (1999) is a framework for understanding an adaptational method for coping with grief. The underlying premise is that the better a person is able to cope with loss the more likely they are to adapt to their new life circumstances. Effectively coping with loss reduces some of the secondary effects of bereavement such as mental health stressors and physical ailments over time (Stroebe et al., 2007). According to model developers Stroebe and Schut (1999), the DPM suggests that people cope with loss in two ways. The first is by engaging in loss-oriented coping behaviors that directly address the loss. This refers to actively confronting the reality of the death, evoking memories, engaging in a process of letting go, and establishing continuing ties. Loss-oriented behaviors also include periods of denial and avoiding life changes.
The second aspect is restoration-oriented coping that addresses the secondary losses and additional stressors associated with bereavement and the person’s ability to attend to new life circumstances (Stroebe & Schut, 1999). This refers to the ability to address changes that have occurred as a result of the loss, accomplishing new tasks, beginning to define self in new ways, and exploring new role development. It may also include distractions that take the focus away from grief.
A unique aspect of the DPM is the recognition of the flexibility in the coping process of the bereaved. Stroebe and Schut (1999) state that healthy coping behavior includes oscillating between a restoration orientation and a loss orientation. Healthy coping with bereavement requires attention to both styles. Most bereaved can identify the orientation that is most comfortable and familiar. Often when intervention is necessary, it is due to difficulties oscillating to the other style of coping and finding a helpful balance.
The DPM-R (Stroebe & Schut, 2015) is the revision of the DPM to include the relational aspects of bereavement; it identifies coping responses at the family level. Couples coping with the death of their child may grieve in ways that help or hinder both the individual and relational coping that facilitates healing. The DPM-R suggests the need to address healing at both the individual and relational level. Exploring loss orientation at the couple level includes a shared process of understanding the death and the impact on the couple system. While restoration orientation at the couple level explores meaning making and the “subjective and objective changes within the surrounding world, those that came about as a result of the death” (Stroebe & Schut, 2015, p. 876).
Social Justice
Context is critical for understanding the experiences of the bereaved and facilitating healthy coping. In a diverse country, there is a need to attend to the various needs of clients. It is imperative that we practice in ways that empower and enrich the fullness of clients’ lived experiences. It is the key to know and understand the various cultural identities that are at play.
Dimensions of culture (i.e., race, ethnicity, class, gender, spirituality, age, sexual orientation, nationality, disability) provide context to the experience of the world and how the bereaved process grief. A social justice lens is an epistemology that explains the social power dynamics that create and maintain institutional oppression for marginalized groups and privileges for dominant groups (Molaison et al., 2011). A key component of social justice is understanding the individual, societal, and institutional power structures designed to reinforce inequality in covert and overt ways. This framework challenges structures that create barriers, which prevent marginalized people from contributing their experiences and having them valued. Working from a social justice perspective necessitates dismantling privilege and working to create equal access to resources and opportunity. Aligning a social justice orientation with the DPM is critical for providing the type of support couples need, see Figure 1 for a clear depiction of how the two work well together.
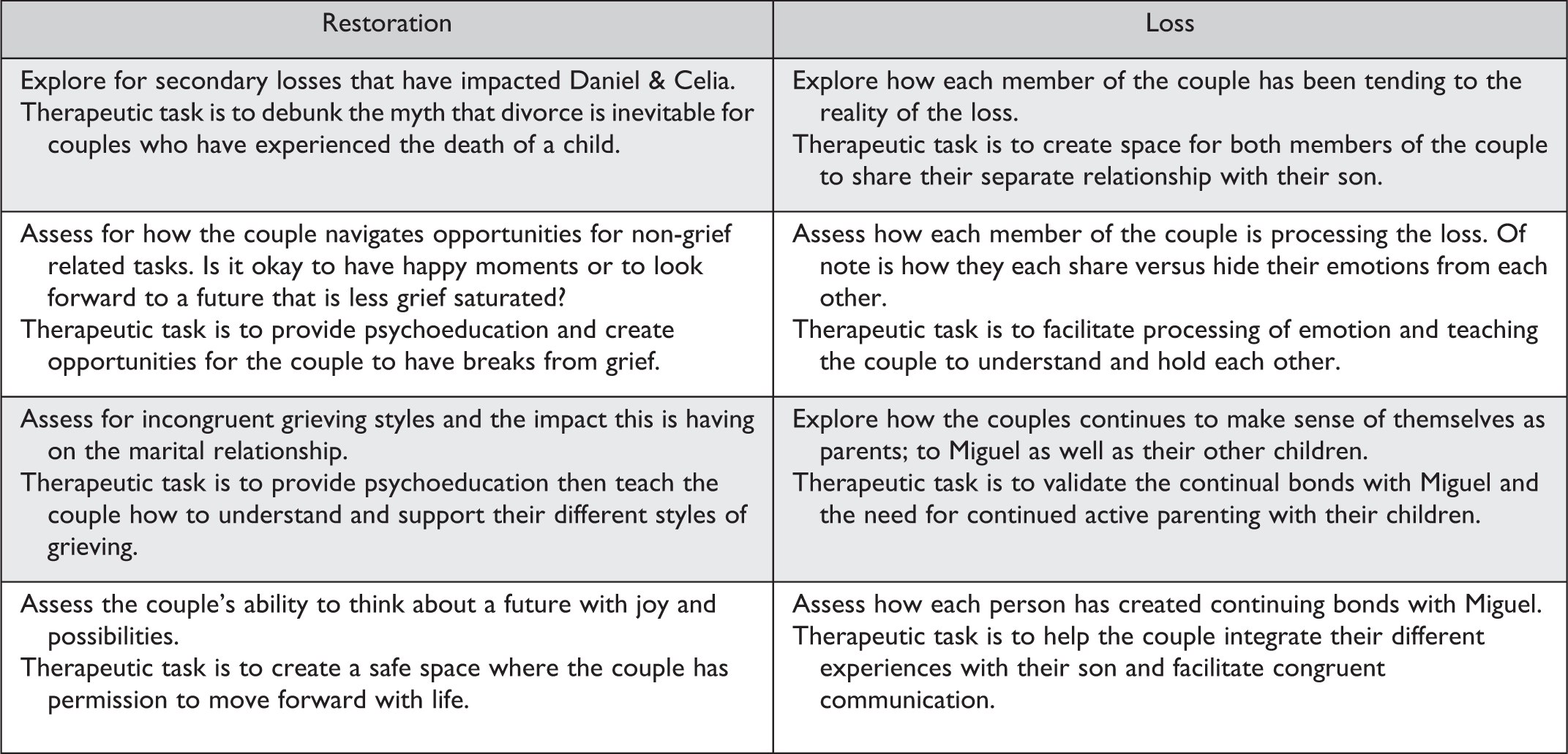
An example of how to assess the case using the Dual Process Model–Revised as a guide for the relational work necessary for healing.
Incorporating a social justice lens with the DPM requires family therapists to examine the couple’s loss orientation process through a lens that understands dynamics of power and oppression. Accepting the reality of the loss and finding ways to share emotions should be facilitated within a context of understanding how the couple’s dimensions of culture (i.e., race, gender, class, spirituality, ethnicity, age, disability, language, sexual orientation, etc.) organize this experience. A social justice lens posits that power dynamics within these identities privilege some groups over others. While this is true at a societal level, it is also present within the family. A socially just family therapist uses a knowledgeable and nuanced approach when facilitating conversation to raise these dynamics in a sensitive yet meaningful way.
Clinical Example
The Rodriguez’ entered therapy approximately 15 months after the death of their youngest son, Miguel (10). The couple, Daniel (50), a mechanic and manager at an auto body shop, and Celia (47), an administrative assistant at a large company, have been married for 23 years. They have two surviving children, Juan (16) and Angel (12). The Rodríguez’ identify as Latinx from Puerto Rico. The couple entered therapy because although it had been over a year, they felt they were growing apart and feared that the death of their son would lead to a divorce.
Assessment and intervention that is culturally sensitive requires therapists identify specific culturally relevant rituals for healing; explore beliefs about the dying, death, and afterlife; and examine how the client’s dimensions of culture organize to create rules about healthy and unhealthy responses to loss (Rubin et al., 2012).
Questions about spirituality are common when grief occurs. Socially just therapists are comfortable navigating exploration about spirituality and how their beliefs may be impacting how they make sense of the loss as well as rules and rituals for healing. Again, it is important for therapists to encourage the couple to share their beliefs and hold space for the ways they may be convergent or divergent.
Therapists should assess for gendered expectations regarding the expression of grief. Couples may not be aware of the impact of these stereotypes and how often they work to limit authentic healing. Therapists can assist clients in deconstructing the limiting beliefs and facilitating opportunities for each member of the couple to support their partner.
Engaging this couple from a socially just perspective includes exploring how ethnicity has shaped their lives. What does it mean to Celia and Daniel to be Puerto Rican? How do they participate in their culture? How have they navigated through experiences of oppression? What are the cultural ways in which they process grief? Who participates in their community of support?
Class status also dictates the way couples are able to process loss and tend to restoration. The death of a child may present a significant financial crisis in addition to the emotional affects. Class determines what access to resources the couple may have and how they go about obtaining what they need for their family. While it is often an American taboo to discuss class, it is necessary to create space for the couple to have these deliberate conversations. How has the couple been impacted financially? How might this affect their ability to plan for the future?
According to the revised DPM model for families (Stroebe & Schut, 2015), families and couples alike go through an oscillation process between loss- and restoration-oriented experiences in their everyday life. In their work, Stroebe and Schut stress out the importance of integrating family processes as well in understanding grief and in clinical work. We concur with their opinion in working specifically at the couple’s level when there is a direct impact as it happened for Daniel and Celia (see Figure 1 for assessment).
One of the foundational aspects of addressing loss in couples who lost a child is creating a safe therapeutic place where intense emotions can be expressed and new, shared meaning can be created while healing the wounds of the couple’s soul. Validation as well as normalizing grief and oscillation processes are very useful in creating safety in the therapy room. For Celia and Daniel, it may be relieving to hear that their difficulties are not an uncommon place to be in their couple relationship after losing their son.
The myth that couples typically divorce due to grief has been perpetuated throughout the media. Therapists can normalize the fear yet share clinical evidence that this is not actually true for most grieving couples. Grief often exacerbates underlying tensions within the relationship, and therapists have an opportunity to help the couple navigate these issues. Therapists should encourage couples to grieve together, sharing their grief in addition to their individual processes. Other goals for therapist should be to assist couples to develop ways to honor and remember their son or daughter as well as to support the couple in reinvesting in life and the future.
One of the most important and in the same time the most difficult tasks for the parents is relocating their departed child (Stroebe & Schut, 2015; Worden, 2018). Addressing with Daniel and Celia how they continue to have a relationship with Miguel, in what ways the relationship is the same and in what ways it is different, what do they miss about him being physically present but in the same time how is he still part of the family can help them make meaning of their loss differently. The idea that death may end a life but does not end the relationship can be comforting and can restructure the story the couple is telling themselves about their loss. Religious and spiritual beliefs can play an important role in meaning making. For Daniel and Celia, their catholic views of Miguel being now with his Heavenly Father, in a place of love and peace, without struggles and pain, can give some comfort and can help them to move on with their life.
Another important part of working with couples who lost a child is helping them understand differences in grieving. Gilbert (1996, 1997) ascertains that both couples who grieve synchronously and couples who grieve “out of sync” can fail to provide emotional support to each other and can struggle in their relationship. Processing emotions during couple sessions and helping partners to witness each other’s sadness, anger, or other emotions can be very powerful in re-creating a sense of togetherness for couples and a new shared meaning about loss (Walsh & McGoldrick, 2004).
Witnessing each other’s sadness, crying together, being mad at the senseless death, and even mad at God who allowed this to happen will contribute to a sense of togetherness and sharing the burden for Celia and David, which has the potential to maintain and increase relational satisfaction. Helping Celia understand that the fact that Daniel does not cry as much as Celia, that he stays at work longer hours after Miguel’s death, is part of his way of grieving may contribute to a more positive outlook on the relationship.
Another aspect to be addressed with Daniel and Celia should be their sexual relationship, in what ways it changed and in what ways it stayed the same after the death of their son. According to Gilbert (1996, 1997), sexual mismatch is another aspect that contributes to out of sync grieving between partners. Divergent and/or different needs for sexual activity are considered to contribute to a low sense of intimacy between partners. For Daniel, being sexually intimate may fulfill an attachment need for connection, while for Celia, participating in sexual activities may be a painful reminder of how Miguel was conceived and of his absence.
Couples’ therapists can help Daniel and Celia create a shared meaning by helping them create shared rituals for grieving, participating together in events that celebrate Miguel’s life, and working together on restructuring roles within the family structure (Walsh & McGoldrick, 2004). Because Miguel was killed while riding his beloved bike, Celia and Daniel may decide to participate actively in advocating for more bike routes in their neighborhood, which are clearly marked. They honor Miguel’s life hoping to help other kids enjoy more safely one of his favorite activities. Expressing together the love they share for their son may help rekindling the love they have for each other.
As their most important tool in clinical work, therapists working with grief and loss should engage in a continuing process of self-reflection. Baldwin (2013) suggests four key principles of self-examination: the principle of transparency, allowing clients to view the therapist’s humanity; the principle of authenticity defined as being fully present in relationship to self; the principle of self-awareness; and the principle of congruence, meaning there is a close relationship between beliefs, feelings, communication, and behavior (Satir, 1988).
It is very important for the therapist working with a couple like Celia and Daniel to examine their own believes, attitudes about death in general, their own mortality, and death of children. We suggest that for this work it would be helpful to answer questions such as how do I think about my own death? What do I believe happens after death? Where do these beliefs come from? What does it mean to express grief? What is the way I express grief? Where do I have the freedom to express grief and loss and when, where, and in what ways do I feel constrained? What do I think about death of children? Celia and Daniel’s therapist should be curious about the relationship they have with their attitudes and beliefs and how they impact their work with the couple.
Conclusion
While there is some recognition in the field about the need for more research on integrating couple and family aspects of grieving (Gilbert, 1997; Stroebe & Schut, 2015), there is still a paucity of studies and literature on the topic. This work is meant to provide guidelines on addressing specifically grieving in couples who lost a child. Being one of the most significant stressors that one can encounter during a lifetime, the death of a child has a powerful impact on both individual and relational processes in a couple or a family. We encourage couple therapists working with this specific population to look at emotional aspects of grief as well as creating a shared new meaning of the loss experienced as well as a shared, reintegrated meaning of their relationship with the lost loved one and their new life as a couple. We suggest that creating rituals of remembrance, participating in advocacy events honoring the life lost, and finding time for directly expressing feelings with each other are all steps that are helpful in the healing process.
Furthermore, future research should focus more on dyadic processes of grieving in couples in order to gain a better understanding how relational aspects can contribute to better individual outcomes as well as relational satisfaction. More studies on differences in grieving based on cultural aspects are needed. We understand that there is a diversity of rituals for grieving in various cultures, based on race, ethnicity, or religion, but as of now, we do not know what the differential impact on bereaved couples and families is.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.