
Abstract
There are currently 2.3 million Americans incarcerated. In 2018, Black males were 5.8 times more likely to be incarcerated than White males. Every aspect of incarcerated individuals’ lives is immensely impacted by the criminal justice system, this includes their romantic relationships. The purpose of this study is to examine if PTSD and depression impact romantic attachment. Using data from the Multi-site Family Study on Incarceration, Parenting, and Partnering study, our independent variables PTSD and depression used the 4-point Primary Care PTSD Scale (PC-PTSD) and The Center for Epidemiologic Studies Depression Scale (CES-D). The dependent variable of romantic attachment consisted of four questions regarding close relationships. Our results showed that race, PTSD, and depression are all significant predictors of romantic attachment within incarcerated males and their non-incarcerated romantic partners. Clinical implications and future directions for incarcerated men and their nonincarcerated female romantic partners are provided.
There are currently 2.3 million Americans incarcerated (Sawyer & Wagner, 2020). Nearly 33% of the incarcerated population are African American individuals (Assari et al., 2018). For example, Black men are given longer sentence lengths than White men (Burch, 2015; Chen, 2013; Nowacki, 2017). Discrimination can exacerbate the effects of incarceration on mental health (Assari et al., 2018). Psychiatric disorders including major depressive disorder (Assari et al., 2015), depressive symptoms (Watkins et al., 2011), hypertension (Hicken et al., 2014), and poor sleep quality (Hicken et al., 2013), thus leading to higher rates of mental illness amongst incarcerated African Americans. Incarceration can cause adverse outcomes for non-incarcerated partners, including relationship stress, dissolution of trust, infidelity, conflict, and violence (Comfort et al., 2018; Harman et al., 2007). Therefore, it is imperative to study the impact of Post-Traumatic Stress Disorder (PTSD) and depression symptomatology for incarcerated individuals and how it impacts their romantic relationships, specifically, their romantic attachment.
Depression and PTSD while Incarcerated
Being involved in the criminal justice system has been shown to increase stress and mental health issues (Sugie & Turney, 2017). Incarcerated males are more likely to suffer from major depression than non-incarcerated males (Edgemon & Clay-Warner, 2019; Turney et al., 2012). There are ten times more mentally ill individuals in prisons and jails than in mental health facilities (Haney, 2017). In 2006, a Bureau of Justice Statistics study reported that over half of the individuals in the U.S. state correctional facilities reported a mental health condition, 33% being major depression (Edgemon & Clay-Warner, 2019). Stressful, hostile, or psychologically abusive settings such as being incarcerated and isolated can be detrimental to individuals’ mental health (Haney, 2017). Several studies have documented how isolated, confined environments can lead to feelings of lethargy, hopelessness, and depression (Haney, 2017; Kupers, 2008). For individuals who are already suffering from depression, isolation only exacerbates their symptoms, leading to a worsened depressive state.
The U.S. Department of Veterans Affairs (2019) estimates that about 8 million adults are diagnosed with PTSD each year. Between 25% and 28% of people with mental illnesses have been arrested (Dewa et al., 2018). Symptoms of PTSD that a person may experience as identified by While in prison, about 48% of incarcerated individuals experience symptoms of PTSD (Piper & Berle, 2019). PTSD’s relevance in criminal justice settings is supported by research that consistently shows individuals involved in the criminal justice system experience significantly higher rates of exposure to trauma than the general population, including elevated rates of recent victimization in adulthood (Sadeh & Mcniel, 2015; Sadeh & McNiel, 2015). Anderson et al. (2015) concluded a high prevalence of Black Americans developing PTSD while incarcerated. In fact, Black Americans who were in prison were twice as likely to have PTSD as opposed to Black Americans who had never been incarcerated. This suggests that incarceration may be a risk factor in developing PTSD (Anderson et al., 2015).
Trauma exposure among incarcerated individuals with mental disorders can cause periods of heightened stress and vulnerability, which may increase the risk for recidivism by triggering the use of maladaptive coping skills (Sadeh & McNiel, 2015). People with serious mental illness who have been released from prison face challenges reentering society because many do not receive the necessary mental health care and adequate transition planning (Baillargeon et al., 2010), thus contributing to the cycle of incarceration.
Incarcerated Romantic Relationships
Incarceration can have an overall negative effect on the quality of relationships (Comfort et al., 2018; Durante et al., 2022; Harman et al., 2007; Tadros, Durante, McKay, et al., 2022), including an emotional strain (Carlson & Cervera, 1991; Martinez & Christian, 2009; Tadros et al., 2020), and feelings of helplessness (Taylor, 2016) for both the incarcerated individuals as well as their non-incarcerated romantic partner. However, for those who maintained some form of contact with an incarcerated individual faced financial tolls, the costs of phone calls and visits were significant and drained resources that family members would have used to pay household bills or buy food (Comfort et al., 2016). When partners’ communication was reduced or eliminated during the males’ incarceration, it created both an emotional impact due to loss of contact and a social impact due to the hiatus in the relationship Comfort et al., 2016).
Incarcerated men living in confinement for more than a year may experience psychological symptoms such as hypervigilance, interpersonal distrust, and cognitive distancing; this can be caused by the isolation and lack of communication with family members or romantic partners (McKay et al., 2018). These psychological symptoms can create further stress for both partners. The incarceration of a family member often exacerbates pre-existing stressors – the costs of visitation, phone calls, and legal expenses needed to support an incarcerated individual can create major burdens on a partner and other family members (Comfort et al., 2016). The time, energy, and money that goes into maintaining a relationship with an incarcerated partner can be overwhelming and expensive, especially if the prison facility requires one to travel (Skipper et al., 2020), this can increase interpersonal stress due to arguments about financial situations (Comfort et al., 2016) thus creating further strain on the relationship.
Adult attachment is conceptualized into two continuous dimensions: attachment anxiety and avoidance (Brennan et al., 1998; Lefebvre et al., 2021). Attachment anxiety is defined as a negative model of the self as unworthy of love. Those who report high levels of attachment anxiety tend to display hypervigilance towards signs of rejection and potential abandonment of their romantic partner. When individuals perceive their relationship is potentially threatened, their attachment system is activated, and they seek constant reassurance and closeness to their partners. Attachment avoidance is characterized by a negative model of others. Individuals with high levels of attachment avoidance often have an excessive need for independence and often are uncomfortable with emotional intimacy. When individuals perceive their independence is potentially threatened, deactivation strategies are used to reduce their sense of vulnerability by repressing their feelings and maintaining a distance from their partner (Bartholomew & Cobb, 2011; Brennan et al., 1998; Lefebvre et al., 2021).
Individuals with attachment anxiety may use aggression towards their partner in an attempt to either get their attention, seek closeness, and increase an emotional connection; individuals with attachment avoidance may attempt to push their partner away, create emotional distance, and increase their independence (Godbout et al., 2017; Lefebvre et al., 2021). For both partners, attachment insecurities have been associated with lower relationship satisfaction—or higher relationship dissatisfaction (Candel &Turliuc, 2019; Lefebvre et al., 2021). Therefore, dyadic contexts where attachment insecurities occur and couples are dissatisfied can create more hostility, criticism, contempt, poor communication, and poor problem-solving skills (Bartholomew & Cobb, 2011; Lefebvre et al., 2021). These dysfunctional attachment behaviors can harm their partner’s relationship satisfaction and can also increase the risk of committing Intimate Partner Violence (IPV) and becoming a victim of IPV (Lefebvre et al., 2021; Mikulincer & Shaver, 2018).
Individuals and their partners’ PTSD symptoms are associated with one partner's lowered perception of their partner's functioning as a romantic partner as well as parenting stress (Fredman et al., 2017). When one partner experiences symptoms of PTSD within parental dyads, the relational satisfaction and functioning may be diminished (Fredman et al., 2017). PTSD symptoms and associated features are said to impair a trauma survivor's ability to effectively relate to others close to them, which results in the partner feeling less satisfied and perceiving more problems in the relationship (Monson et al., 2010). Additionally, emotional numbing may interfere with intimacy and symptoms of anger and agitation caused by PTSD often reduce the partner's sense of safety in the relationship (Dekel &Monson 2010; Lambert et al., 2012). PTSD will increase one's likelihood of experiencing stress, anxiety, or depression (Goff & Smith, 2005; Lambert et al., 2012). Traumatic life experiences are associated with depression and depressive outcomes amongst the incarcerated population (Edgemon & Clay-Warner, 2019). Depression can have a major impact on romantic relationships. Depressive symptoms can cause individuals to struggle with impaired social skills (Sharabi et al., 2016), decreased sexual interest (Kennedy et al., 1999; Sharabi et al., 2016), questioning their relationship (Knobloch & Delaney, 2012; Sharabi et al., 2016), and diminished emotional disclosure (Kahn & Garrison, 2009; Sharabi et al., 2016). Therefore, it is vital to explore how PTSD and depression impact attachment within incarcerated males’ romantic relationships with non-incarcerated female partners, to reduce the adverse effects on relationships. Our research question asks: Does attachment impact PTSD and depression in incarcerated males within romantic relationships with non-incarcerated female partners while controlling for race? We hypothesize that attachment will impact PTSD and depression will impact attachment in incarcerated males within romantic relationships with non-incarcerated female partners while controlling for race.
Method
Data Source
The Multi-site Family Study on Incarceration, Parenting, and Partnering [MFS-IP] evaluated a grant-funded program by the Office of Family Assistance. The purpose of the MFS-IP was to verify how effective the program is at sustaining healthy family relationships in families with incarcerated fathers. The sample consisted of incarcerated men and their female coparenting partners across five states: Indiana, Minnesota, New Jersey, New York, and Ohio. Inclusion criteria consisted of all participants being over 18 years of age and ability to speak English. Interviews were conducted between December 2008 and August 2014 using both audio computer-assisted self-interviews and computer-assisted personal interviews. Incarcerated fathers selected a child closest to 8 years old to be the “focal child”; these men were also asked to identify a female coparenting partner for the study. Coparenting partners may or may not be romantic partners, however, for the purposes of this study, only romantic partners were analyzed. Various recent articles have sought to better understand incarcerated relationships using this dataset (Comfort et al., 2016; Durante et al., 2022, 2023; McKay et al., 2018; Tadros, 2022; Tadros & Ansell, 2022; Tadros & Durante, 2022; Tadros et al., 2021b; Tadros & Vlach, 2022).
Measures
Our dependent variable of attachment consisted of four items rated by participants on how much they agree or disagree with the statements in references to close relationships (see Table 1). Our first independent variable was PTSD, measured using the 4-point Primary Care PTSD Scale (PC-PTSD) was used. Each question asked corresponds to one of the four factors that are considered to be specific to PTSD, not confounded by general psychological distress (Foa et al., 1995). The answers are shown in Table 2, the answer selections were all yes or no. Respondents would receive a corresponding score of 0 if they answered no and a score of 4 if they answered yes to each of the questions. This version of the scale was created in a way that the questions are to the point, self-reported measures that are easier to understand as well as in a way that could be implemented in a busier environment where the screener has limited time (Prins et al., 2003).
Attachment.
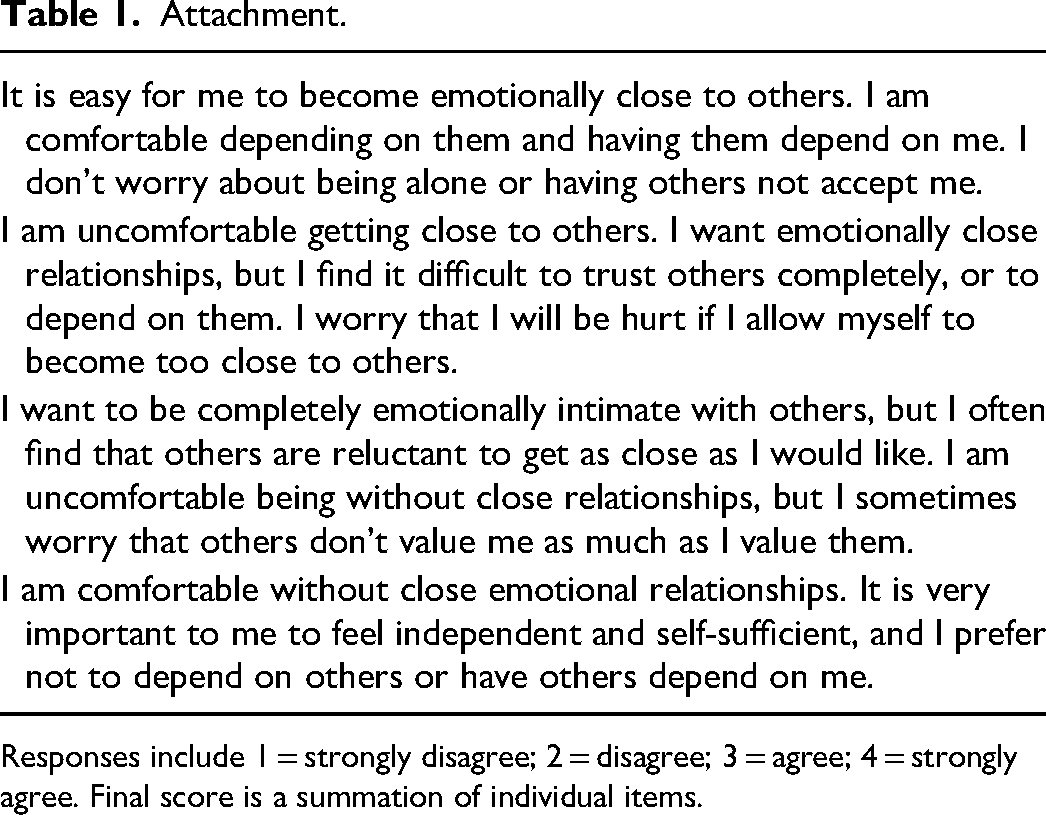
Responses include 1 = strongly disagree; 2 = disagree; 3 = agree; 4 = strongly agree. Final score is a summation of individual items.
Primary Care PTSD (PC-PTSD) questions.
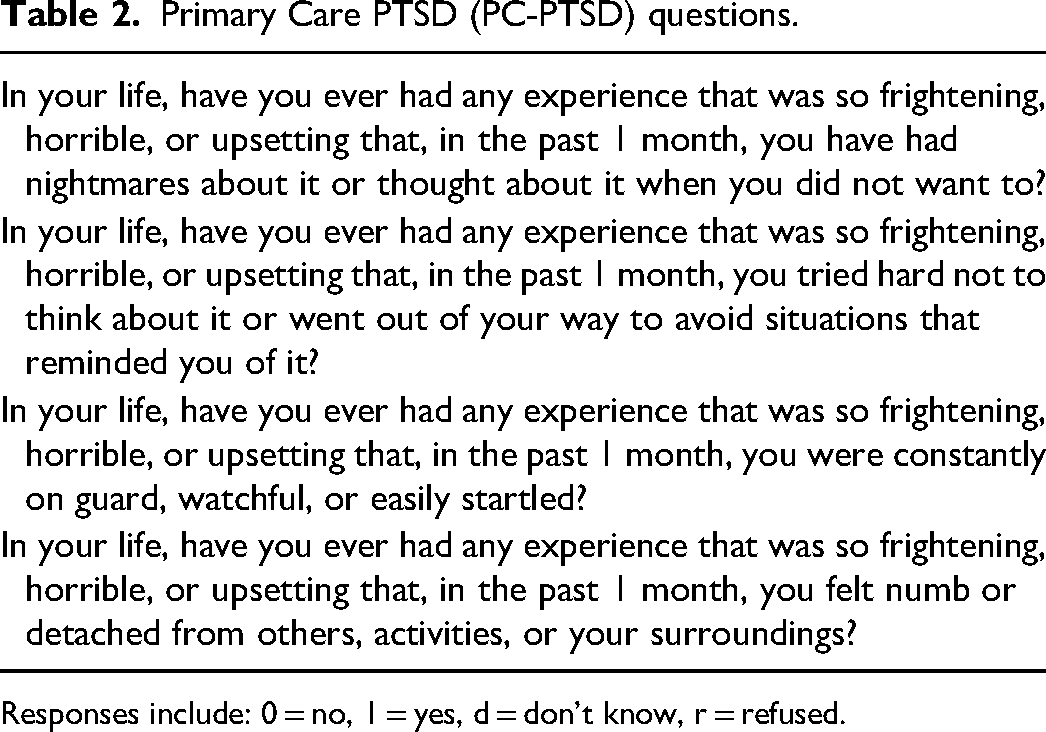
Responses include: 0 = no, 1 = yes, d = don’t know, r = refused.
Our first independent variable is depression which was measured via The Center for Epidemiologic Studies Depression Scale (CES-D) is used to measure the covariate depression. The CES-D is used to identify depressive symptoms in the general population, generally a 20-item measure (Zhang et al., 2012). The MFS-IP consists of a shortened, 9-item CES-D version of the measure. Although the original instrument has 20-items, the shortened version has been validated (Reda, 2011; Zhang et al., 2012). Before its usage in the MFS-IP, several studies have used the CES-D to measure depression within the incarcerated population (Clarke & Waring, 2012; Ramsey et al., 2019). The 9-item CES-D measure consists of the questions shown in Table 3. The mean of the non-missing items is imputed for each missing value. Scores range from 0–27, higher scores suggest the individual is experiencing more depressive symptoms. The cutoff of nine was chosen, nine is 33% of the maximum possible CES-D score. This is consistent with the 10-item CES-D. Scores range from 0 to 30 and have a cutoff of 10%–33% of the maximum possible CES-D score. We also controlled for race, this included six different variables where individuals were able to choose one or multiple responses. If the subject chose multiple they were put into one category rather than creating a variable for each possible combination of races. Participants were asked “Do you consider yourself to be…”. They were also asked to select all that apply to them. The options included, white, black, American Indian, Asian, islander, other race, and multiracial.
9-Item CES-D Scale for Measuring Depression.
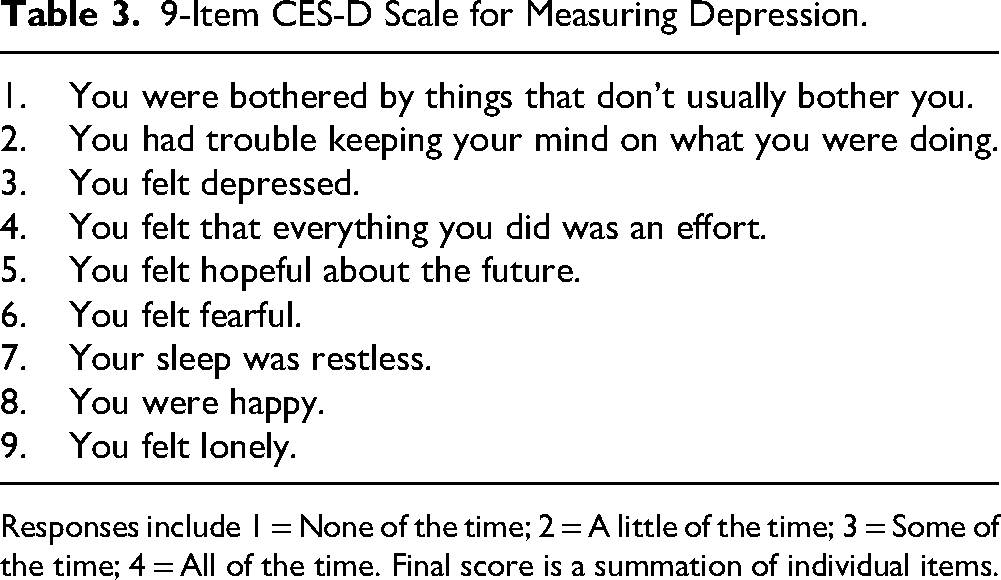
Responses include 1 = None of the time; 2 = A little of the time; 3 = Some of the time; 4 = All of the time. Final score is a summation of individual items.
Analytic Strategy
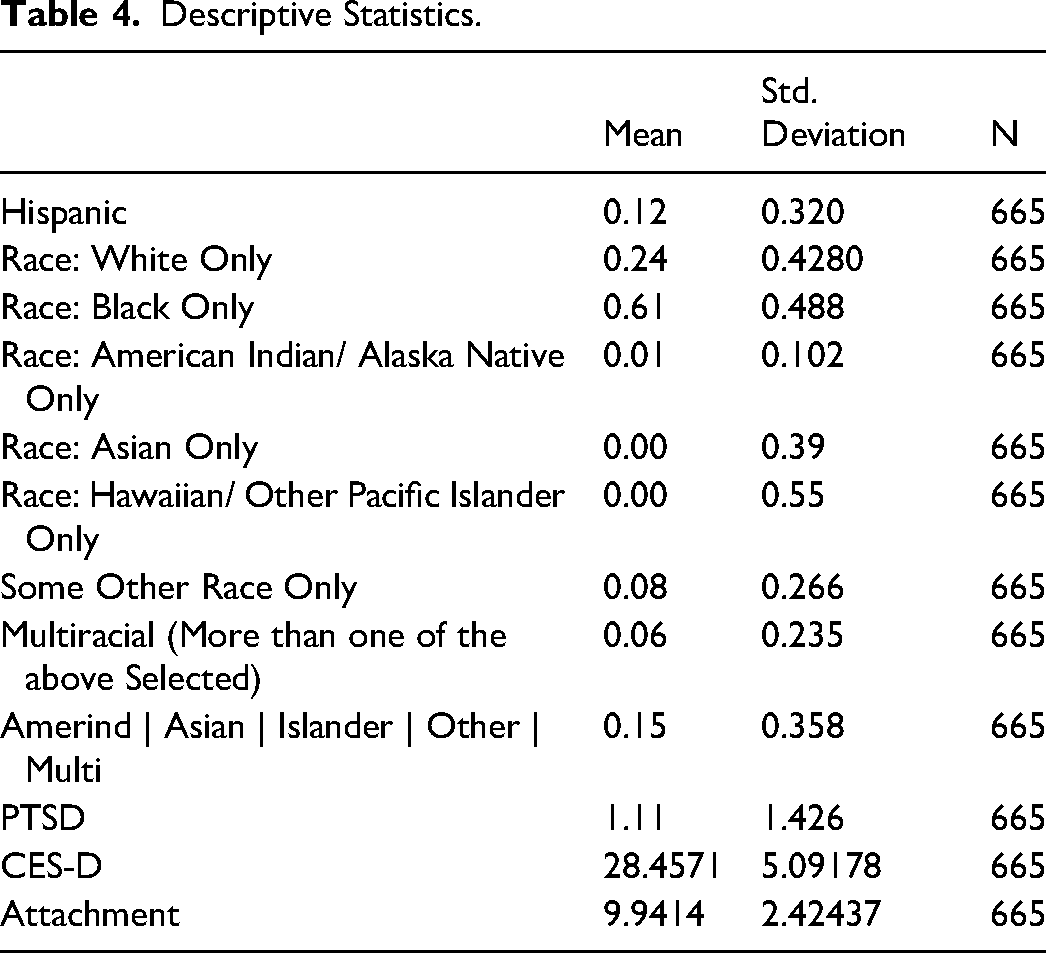
To start, we examined variables for attachment, PTSD, depression, and race. The overall participants were combed through in order to only pull data collection from those of couples. In order to run descriptive statistics and a linear regression, the collective variables for depression and attachment were compiled separately and were recoded. This was to have the variable reflect that the responses were as follows, (Attachment) 1 = Strongly Disagree, 2 = Disagree, 3 = Agree, 4 = Strongly Agree; (CES-D) 1 = A little of the time, 2 = Some of the time, 3 = Most of the time, 4 = All of the time. Once recoded, both variables were computed for their sums, after this step we were then able to run descriptive statistics (Table 4). We then ran a multiple linear regression (Table 5), this consisted of the independent variable and dependent variables in their dichotomous forms. This analysis assesses if the independent variables are a predictor of the dependent variables with one control variable.
Descriptive Statistics.
Regression.
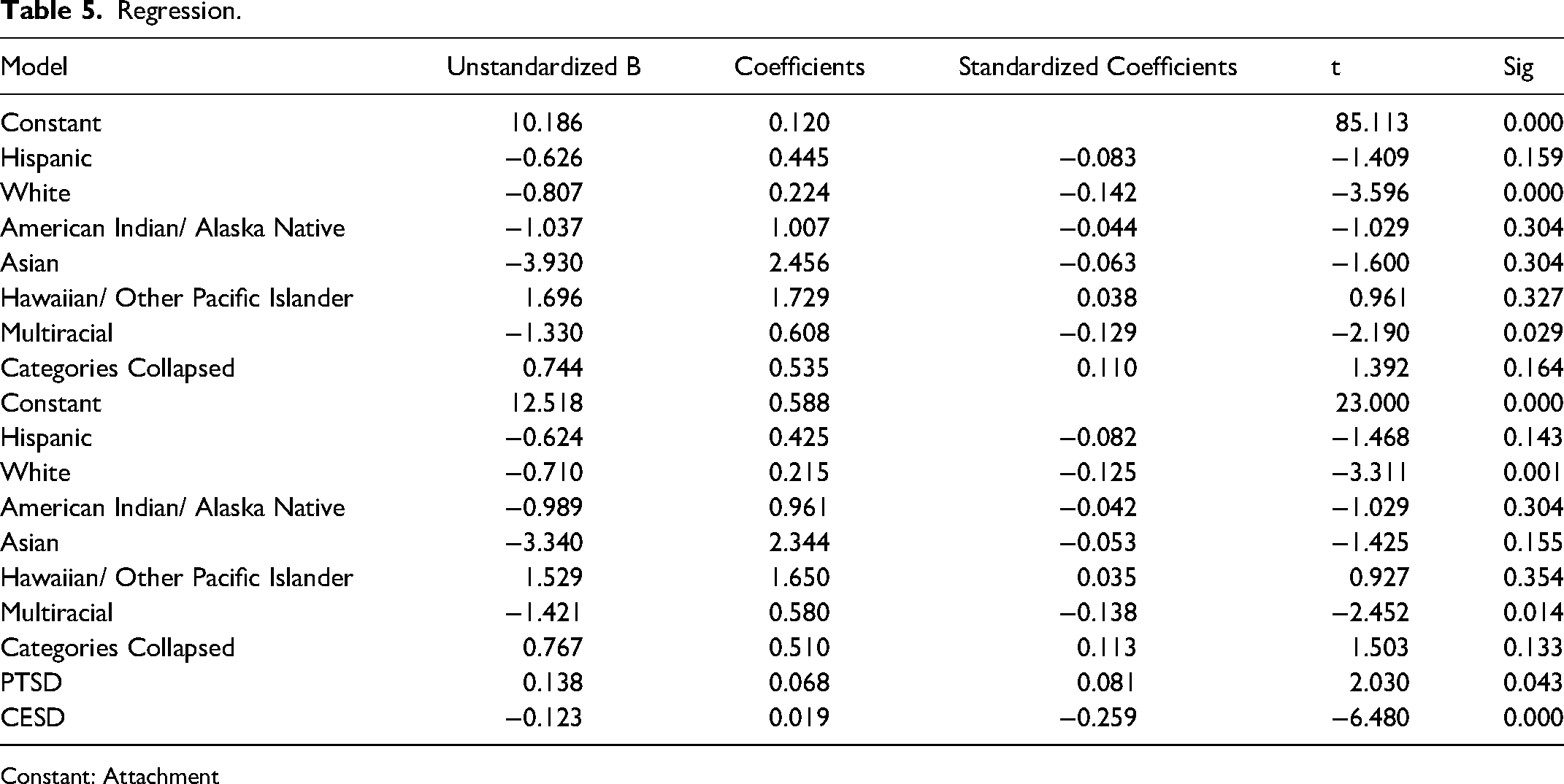
Constant: Attachment
Results
The sample consists of a medium to large sample size (n = 665). Within the sample, the highest mean was the race of Black 0.61 (SD = 0.48), then followed by White, 0.24 (SD = 0.4280), then Hispanic, 0.12 (SD = 0.320). The races that were present in the study that had minimal averages were other race, 0.06 (SD = 0.235), followed by multiracial, 0.06 (SD = 0.235). Lastly with a tie in means between Hawaiian/other pacific islander, 0.00 (SD = 0.55) and Asian 0.00 (SD = 0.39). The descriptive statistics can be found on Table 4. The regression, as shown on Table 5, shows the correlations and the significance of our dependent variable and our independent variables. Multiracial, −0.047 (p < 0.05), had a positive correlation with the dependent variable, attachment. The regression equations in model one and model two differ slightly when running one including PTSD and depression (model 2) and one without (model 1). Model 1 regression is run with the following equation F(7, 657) = 3.079, p < .05, while model 2 was run using F(9, 655) = 10.081, p < .05.
The variables include the race of White (p < 0.000) and depression (p < 0.000). These variables show that if a respondent were both White with reported symptoms of depression, the more likely they are to have a direct tie with our dependent variable, attachment. Within our independent variables, five of them have a statistical significance with our dependent variable, romantic attachment. These are as follows, white: t(657) = 3.596, p < .05, multiracial: t(657) = −2.190, p < .05, PTSD: t(655) = −6.480, p < .05, and depression t(655) = −6.480, p < .05. Therefore, each of the independent variables predict consensus of attachment as hypothesized.
Discussion
Using the 4-point Primary Care PTSD Scale (PC-PTSD) and The Center for Epidemiologic Studies Depression Scale (CES-D), our study sought to understand if PTSD symptoms and depression impacts attachment in incarcerated males within romantic relationships with non-incarcerated female partners while controlling for race, using six different racial variables. We hypothesized that PTSD symptoms and depression will impact attachment in incarcerated males within romantic relationships with non-incarcerated female partners while controlling for race.
When controlling for race the six variables participants could identify as were White, Black, American Indian, Asian, Islander, other race, or multiracial. However, 61% of respondents identified as Black this is due to the disproportionate representation of black males in the criminal justice system. Incarceration rates for Black males were at least 6 times those of white males for all age ranges (Williams et al., 2019), and in 2016, (41.3%) of incarcerated individuals in state and federal prisons were black males (Carson, 2018; Williams et al., 2019). Which explains why most of the participants in our study were Black males thenWhite (24%) and Hispanic (12%) were the highest average race that participants identified as.
We found a positive correlation between multiracial individuals and attachment. This may be due to the attachment theory reflecting Western styles of thinking and relatedness (Brown et al., 2008). Western goals for attachment are based on individuals forming a safe base and personal exploration with the ultimate goal of autonomy, where collectivist culture for example may have a goal of mutual effort rather than self-reliance (Brown et al., 2008). When reviewing cross-cultural research, there emerges a theme that the dynamics described in attachment theory reflect Western ways of thinking and styles of relatedness. Attachment goals from a Western perspective move the individual from reliance on a safe base to personal exploration encompassing a wider and wider periphery, with the goal of autonomy. However, in collectivist cultures, for example, the goal of the caretaker would be more apt to encourage mutual effort rather than reliance on self.
We found that White individuals who reported symptoms of depression were strong predictors for romantic attachment. An extensive amount of research has been conducted that supports a direct positive relationship for adult insecure attachment styles and depression (Dagan et al., 2018; Murray et al., 2021; Spruit et al., 2020). Additionally, 62% of white incarcerated males in state prisons and 71% in jails were found to have a mental illness (Bureau of Justice Statistics, 2006). Due to white incarcerated males’ high prevalence for mental illness, it may explain the impact on romantic attachment. Further, we found that if participants identified as White, Black, or Multiracial and had PTSD or depression were more likely to impact romantic attachment for incarcerated males than their non-incarcerated female partners. This may be due to several things. PTSD symptoms may impair the trauma survivor's ability to adequately relate closely to others, which can leave their partner feeling less satisfied and create more problems in the relationship (Lambert et al., 2012), lack of connection can create impaired attachment within the relationship. Further, a recent study found that having PTSD symptoms may be a predictor of a higher risk of coparents not making decisions together and not supporting their partners’ decisions in reference to their shared child (Tadros, Durante, Sugrue et al., 2022). Thus, looking at these factors may provide more insight into barriers to attachment.
Clinical Implications
Our study showed that race, depression, and PTSD are all significant predictors in attachment between incarcerated males and their non-incarcerated romantic partners. These results display the need for clinical intervention to strengthen attachment amongst incarcerated males, and their nonincarcerated romantic partners may help decrease depression and PTSD. PTSD can be debilitating due to its impacts on multiple aspects of an individual's life and daily functioning. PTSD is linked to higher recidivism rates, which shows the significance of enforcing policies that support a more stable re-entry into the community (Piper & Berle, 2019). Due to race being a significant predictor in attachment, PTSD, and depression amongst incarcerated individuals, it is vital to be aware of racial inequalities within adverse experiences. Race, ethnicity, and socioeconomic status can present barriers to recognizing mental health issues and the need for treatment. Intervention methods should address unique issues individuals may experience– such as immigration, poverty, and diverse cultural norms– to reduce the unequal disparity of who accesses mental health services (Villatoro et al., 2018). Racially minoritized individuals with lower socioeconomic status are at an increased risk for incarceration (Turney & Goodsell, 2018); this risk increases the risk for generational trauma within a family that incarceration can cause. This generational trauma needs to be considered in treatment programs. With the increase of incarceration rates in the U.S., having a parent in incarceration is no longer an uncommon childhood event. The Centers for Disease Control and Prevention (2020) states that Childhood Experiences (ACEs) have an immense impact on future violence victimization, perpetration, and lifelong health and opportunity. It is essential that treatment addresses any childhood trauma that may have occurred, such as parental incarceration. In addition to ACES, incarcerated individuals may have additional pre-existing trauma and the trauma that can come from being incarcerated. Trauma reporting is super sensitive, especially for individuals with severe mistrust; thus, they may not have reported it. Individuals impacted by trauma are more likely to engage in and benefit from Trauma-Informed Care (TIC) services when they feel safe, empowering, and welcoming (Yatchmenoff et al., 2017). Essential components of TIC are awareness of the prevalence of trauma, understanding about the impact on service utilization and engagement, and commitment to incorporating those understandings in policy, procedure, and practice (Yatchmenoff et al., 2017).
Incarceration can create disruption and cause hostility in romantic relationships (Turney et al., 2012). Many incarcerated individuals have reported that they wish to maintain a relationship with their romantic partner (Comfort et al., 2016; Hairston, 1991). The importance of maintaining strong relationships with romantic partners and families during incarceration has been shown to help individuals post-release by having higher success rates and lower recidivism rates which can prevent the incarcerated individual from continuous crime involvement (Apel, 2016; Harman et al., 2007; Van Schellen et al., 2012). Marriage and Family Therapy (MFT) can assist in strengthening relationships, reducing dysfunction in families (Tadros & Finney, 2018, 2019; Tadros et al., 2020), assist with the transition back into society (Tadros et al., 2021c), help with by increasing the involvement and support within the family system to create resilience when facing adversity (Taylor, 2016), build healthy communication within the family, encouraging mutual respect, and strengthen interpersonal relationships (Tadros et al., 2021c. MFTs can improve incarcerated coparenting by encouraging family resilience frameworks that apply systemic theory application and assist incarcerated individuals with their mental health care treatments (Tadros, 2022; Tadros & Finney, 2018, 2019). MFTs are able to provide a deeper level of caring, understanding, and emotional resonance (Aponte & Ingram, 2018), thus creating a safe and understanding environment for incarcerated individuals to receive adequate treatment catered to their specific struggles.
Due to the 2020 Coronavirus pandemic and the recent increase of Telehealth services, we must explore the use of teletherapy in incarcerated settings. Telemental Health (TMH) services use technology, specifically video conferences, to provide mental health care such as evaluation, medication services, and psychotherapy (Morgan et al., 2021; Whaibeh et al., 2020). Using THM services is easier to access for individuals who live far away from the facility their loved one is incarcerated (Tadros et al., 2021a). It can also lessen the financial burdens that come with visitation or in-person therapy. During longer incarceration sentences, it is vital to maintain connections, not only for the individual’s mental health but also because support is a significant factor in success after release (Dallaire et al., 2021). TMH can make therapy services for incarcerated individuals more accessible, which can help with mental health problems, including depression and PTSD, and relational problems such as attachment.
Limitations
Although the current study has a variety of strengths, this study also coincides with several limitations. We used secondary data assembled for the MFS-IP and used only a single (baseline) interview wave Following the programs’ qualification criteria on which the original study focused, the sample consists completely of incarcerated men in state prisons at baseline, who are involved in a committed intimate or coparenting relationship with a different-sex partner. Consequently, the current research does not reflect the experiences of individuals in same-sex relationships, nor does it consider those incarcerated in immigration detention facilities or jails. Secondary data limits researchers’ flexibility to ask questions the way they want, when, where, or how they would prefer to. For example, this version of the PC-PTSD scale was designed so that the questions are short, self-reported measures. The questions do not allow us to determine if the PTSD symptoms were present before incarceration or during. PTSD symptoms may be unknown to the participants which may not be reflected or reported. Further, reporting of trauma is super sensitive especially for individuals with severe mistrust thus they may not have reported it even if it is conscious to them.
Future Research
Our study examined attachment in romantic couples, PTSD, and depression. The study focused on incarcerated men and their nonincarcerated partners. Our study used the PC-PTSD scale which did not allow us to determine if the PTSD symptoms were present before incarceration or during. This study would benefit from adjusting the use of a scale that allowed us to differentiate between if symptoms were during or before incarceration in males. However, more research also needs to be conducted that can be used to provide support and treatment for those impacted, not only as individuals, but also their family members including how PTSD and incarceration may impact family relations. Within these family relations, it would be beneficial to note and examine the partner of the incarcerated in more close detail. In another study, one could examine the incarcerated males’ PTSD and depression and how it impacts their partners mental health and/or their relational satisfaction. Furthermore, instead of studying incarcerated males and their nonincarcerated partners, we would flip the role to study incarcerated women. If we studied women, there would be major differences, for example, women have a higher rate of mental health disorders like PTSD and depression. Women in prison report higher lifetime and current prevalence rates of PTSD than nonincarcerated women (Harner et al., 2015).
Further, we recommend collecting new data to reflect the impact that the global pandemic may have had on different aspects of incarcerated men and their non-incarcerated romantic partners’ life. This data was collected 2008–2014, thus, the COVID-19 pandemic may have changed results. If our study was conducted in the current day using current data from 2020-2022, the outcomes may have been different due to coinciding challenges experienced by incarcerated individuals and their families in the current political climate, as well as the recent COVID-19 pandemic (Tadros et al., 2021a, 2021b). Future studies should examine therapy sessions using TMH for incarcerated individuals to decrease partner conflict and examine how the pandemic impacted incarcerated men and their non-incarcerated romantic partner's relationships. Further research and advocacy for instilling the importance of mental health and family relations in the correctional system is highly critical in helping individuals reduce recidivism rates and develop healthier and less stressful lives.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article