
Abstract
Professional counselors can play a critical role in treating symptoms of autism spectrum disorder (ASD) among children and working alongside their families. While ethical mandates and best practices for treatment center on holding clinical competencies and working within one's scope, the exploration of counselors in the field who specialize in the treatment of children diagnosed with ASD has not been previously explored in counseling research. Through a focus group format, we utilized interpretative phenomenological inquiry to investigate how six professional counselors who specialize in treating ASD diagnosis made sense in building clinical expertise. Implications for professional counselors were presented to better serve this ever-increasing client population.
Keywords
“Being Able to Think Outside the Box”: Exploring Counselors’ Competency Development Working With Children Diagnosed with Autism Spectrum Disorder and Their Families
The Centers for Disease Control and Prevention (CDC, 2023) has recognized autism spectrum disorder (ASD) as an important public health concern in the United States. ASD is classified as a lifelong, neurodevelopmental condition with a prevalence rate of one in 36 children (CDC, 2023), and is characterized by persistent difficulties in social interactions and communication, restricted interests, and repetitive behaviors (American Psychiatric Association [APA], 2022). Children diagnosed with ASD vary drastically in symptom severity, communication abilities, social interactions, behavior, and cognitive functioning. Furthermore, children with ASD often present with various comorbidities (prevalence rate of 70%–95%), which can complicate the diagnosis and subsequent treatment (APA, 2022). While ASD is prevalent across all races and ethnic identities, researchers have illuminated inequities in the diagnosis and treatment among non-White groups, noting how these glaring disparities carry significant clinical consequences (Rivera-Figueroa et al., 2022). Additionally, co-occurring conditions have been linked to significant clinical implications as they can “mask the expression of autism and delay the diagnosis of autism until later in childhood or early adolescence and the treatment often requires additional psychosocial and pharmacological treatments” (Mosner et al., 2019, p. 3819).
Due to the complexity and prevalence of the diagnosis, there is a need for competent and skilled counselors who can work alongside children with ASD and their families. Outside of rehabilitation counseling literature, an exploration of counselors in the field who specialize in the treatment of ASD has remained largely unexplored. What follows is a summary of best practices when it comes to the diagnosis, treatment, and care coordination of children with ASD, as well as counselor competency development and professional dispositions.
Diagnosis, Treatment, and Care Coordination
Counselors can play a pivotal role in minimizing the gaps in treatment services (Kurz, 2018). Although there is no “cure” for ASD, early detection and targeted interventions can improve a child's communication patterns, social relationships, and harmful behaviors (e.g., self-injurious behaviors; Layne, 2007). Counselors can play a pivotal role during the pre-diagnosis phase by identifying early signs of ASD, referring for a comprehensive evaluation, supporting families as they await the diagnosis, offering relevant resources, and advocating on behalf of the family (Feather et al., 2023).
Since ASD is known as a spectrum disorder, individualized treatment is critical given the wide variation in the type and severity of symptoms (Feather et al., 2023). At the onset of treatment, counselors need to screen for comorbid psychiatric disorders and distinguish symptoms that relate to the core features of ASD versus other mental health diagnoses (Feather et al., 2023; Matson & Golden, 2013). When it comes to children with ASD, counselors must be willing to flex their treatment approach, build rapport, and develop a working alliance with their client (Feather et al., 2023, 2024; Jenkins, 2022). For example, counselors may be flexible, and creative throughout the process (Feather et al., 2023, 2024) and provide a predictable presence and space (Stappelbein et al., 2016). As opposed to applied behavioral analysis, counselors would benefit from focusing on skill development and active collaboration with the client by identifying growth areas, rather than efforts towards “normalization” or suppressing ASD-related behaviors (Leadbitter et al., 2021). Further, there is an increasing trend of strength-based approach in clinical practice, which is correlated with improved client well-being (Feather et al., revise and resubmit; Taylor et al., 2023).
In addition to working one-on-one with the child, it is essential to work alongside caregivers in the treatment process as well (Feather et al., 2023). Raising a child with autism is complex and impacts the family unit as a whole (Boshoff et al., 2018), with caregivers experiencing ongoing challenges (e.g., anxiety, depression) when they need to adjust to additional demands and unexpected roles (e.g., child's advocate; Corcoran et al., 2015). Mental health concerns (e.g., anxiety, depression) can be a strong predictor of caregiver strain, and the social implications of their child's behavior may also lead to caregiver isolation (Boshoff et al., 2018). Further, it can be exhausting, overwhelming, and pose a significant financial burden for caregivers to manage concerns about targeting a treatment that works and the many required appointments to maintain treatment (Valicenti-McDermott et al., 2015).
Currently, there is no collectively accepted best course of treatment for ASD, leading caregivers to be unclear on how to advocate for service providers or services (Tonge et al., 2014; Yi et al., 2020). While current best practices include a multimodal approach, it can be difficult and stressful for caregivers to know what this treatment looks like (Tonge et al., 2014). Quality of life among caregivers is linked to their ability to process the emotional impact of their child having a lifelong diagnosis, which may manifest into ambiguous grief (Bravo-Benítez et al., 2019). When working with this specific clinical population, family-centered care is critical as it is a collaborative and empowering practice, where caregivers are respected as the experts and are a resource to the treatment process (Feather et al., 2023, 2024).
Fostering a family-centered approach is critical as families play an essential role in all aspects of treatment (Kurz, 2018; Neely et al., 2012). According to Feather et al. (2023), counselors can provide psychoeducation and teaching strategies and offer feedback to families based on their knowledge and expertise. Layne (2007) suggested counselors share targeted interventions and techniques with caregivers so they are able to manage challenging behaviors and symptoms of the diagnosis. Additionally, counselors can support caregivers by providing psychoeducation on assertive communication and advocacy skills, which will serve them in many situations (e.g., PK-12 school system, doctor's office; Feather et al., 2023), while also promoting realistic treatment expectations (Hohlfeld et al., 2018). In addition, coordination of care is a proactive client- and family-centered practice. Since ASD is a multifactorial condition, a holistic approach that facilitates multidisciplinary links is key to not only treating the diagnosis but also connecting families and children to necessary service delivery components (Antonelli et al., 2009). Care coordination services include clinical referrals, social services (e.g., transportation), insurance, advocacy, and community resources. It is also critical that counselors maintain a multidisciplinary approach, which is crucial when treating a child with ASD (Strunk et al., 2017). Ultimately it is imperative to make sure the client receives the right care in the right place at the right time.
Counselor Competence and Professional Dispositions
Defining counselor competence is a difficult task because it is a complex, multidimensional construct (Sommers-Flanagan, 2015). Typically, competence is defined as having skills, knowledge, professional dispositions, behaviors (Swank & Lambie, 2012), as well as the exercise of judgment (Bernard & Goodyear, 2014) to be considered capable in contributing to positive client outcomes (Sommers-Flanagan, 2015). Clinical supervision is also a critical component of counselor development and includes case conceptualization, skills, and the self as the supervisee (Bernard & Goodyear, 2014). According to Puig et al. (2023), professional counselor dispositions include, but are not limited to, being open, flexible/adaptable, oriented toward social justice and advocacy, holding patience, as well as being creative and intuitive.
As far as the treatment of ASD and fostering expertise, it is imperative that the counselor understands the complexity of the disorder and specialized skills that impact the effectiveness of interventions, mitigation of children's behavior and emotional difficulties, and increases in caregivers’ self-efficacy (Feather et al., 2023; Hohlfeld et al., 2018; Yaholkoski et al., 2021). Positive treatment outcomes have been linked to counselors who embrace a holistic multicultural approach with a specific understanding of the impact of culture and family perceptions of ASD (Ennis-Cole et al., 2013). For clinicians who serve children on the spectrum, competence has also been linked to adequate training and fidelity as well as the ability to implement individualized, evidence-based treatment interventions (e.g., cognitive behavior therapy, behavior therapy; competency (Feather et al., 2023; Iadarola et al., 2017; Wainer & Ingersoll, 2013). Finally, clinicians are shifting their focus from optimal outcome and targeting the classical behaviors associated with the condition (e.g., stimming, eye contact, social interactions) and instead, reevaluating goals and metrics of success that are defined alongside the individual and the person's family. The goal should not be to force and conform to “typical behavior,” but a better quality of life (Dawson & Brandsen, 2022).
Although several constructs and definitions of “clinical competence” exist in the ASD literature, it is difficult to establish objective and generalizable criteria in the field. Similarly, counseling professionals have also noted challenges regarding their development of competence when addressing the symptoms of those diagnosed with ASD (Stoner et al., 2005). The American Counseling Association's (2014) Code of Ethics clearly states, “Counselors practice in specialty areas, counselors take steps to ensure the competence of their work and to protect others from harm” (Standard C.2.b.). While ethical standards note that counselors must demonstrate their competence and ability to provide adequate counseling services, there is a substantial gap in research focusing on the development of clinical expertise specific to ASD. When counselors practice outside of their scope, it can cause harm to both the child diagnosed with ASD and their family (Feather et al., 2023, 2024). The current study aims to explore how counselors who specialize in providing ASD services make sense of their lived experiences developing an expertise to treat the diagnosis. Therefore, the research aims to address the overarching research question: How do counselors describe their experiences developing clinical expertise treating children diagnosed with ASD and their families?
Method
Under the social constructivist paradigm, an interpretative phenomenological analysis (IPA; Smith et al., 2009) tradition was employed in the current study. IPA is a methodological approach that is utilized to investigate how individuals conceptualize and interpret the meaning associated with their personal experiences (Pietkiewicz & Smith, 2014), exploring in detail their lived experience and personal account of the topic under investigation (Smith et al., 2009). Additionally, IPA recognizes that the researchers’ own notions are required in order to make sense of the participant's voice through a method of interpretative activity (Miller et al., 2018). For this study, we attempted to make sense and meaning of counselors’ experiences in developing clinical expertise when treating ASD. We toggled between both emic (i.e., counselors’ making sense of their experiences developing their clinical practice) and etic (i.e., the researchers making sense of the data through a psychological and personal lens) perspectives (Smith et al., 2009). To best understand the phenomenon, we explored the lived experience of six counselors working at a single service agency who all had advanced clinical expertise working with children diagnosed with ASD. Specifically, we sought to explore their process of developing clinical expertise with this population. To achieve this goal, we conducted a semi-structured focus group interview and utilized IPA to complete data analyses.
Procedure and Participants
This study was approved by the institutional review board. Once approved, we utilized a purposive sampling method. Participants were exclusively recruited through one child service agency highly specialized in providing ASD services in the northeastern edge of the Midwest region of the United States. This agency was chosen due to being one of the nation's leading providers and innovators of behavioral healthcare and ASD services for youth and their families. To be eligible to participate in this study, the participants were required to (a) hold a license as a professional counselor; (b) self-identify as a specialist treating children diagnosed with ASD and/or their families; and (c) be employed at the service agency. Information regarding the study was provided to the participants and consent was obtained before the focus group.
The semi-structured, in-depth focus group, 1 hr and 22 min in length, was the primary data-gathering source and was used to help construct participants’ perspectives of the phenomenon. The interview guide included six questions related to their lived experience developing their clinical expertise. Example questions included: “How, if at all, did your educational training contribute to your expertise working with autism?” and “What are your post-graduate experiences counseling children with autism and their families?” Semi-structured focus groups are consistent with the epistemological and theoretical underpinnings of IPA, where researchers can build rapport with the participants to have meaningful and authentic conversations (Miller et al., 2018). Gathering data through a focus group format is common in IPA as it elicits feelings among participants and can provide meaningful insights into each participants’ personal experiences (Smith et al., 2009). Focus groups are also an opportunity for participants to co-construct perspectives and can elicit in-depth discussions to facilitate a shared understanding of the phenomenon (Miller et al., 2018). The focus group was audio recorded and transcribed verbatim for data analysis.
The sample size for this study was determined based on recommendations for conducting IPA research to enable an in-depth, mental analysis of a small homogeneous group (Smith et al., 2009). The aim of IPA is not data saturation, but concerned with appreciating the collective sense-making of the phenomena. Thus, the sample comprised six participants which included four women (67%) and two men (33%); all who identified as White and had an average of 8 years of counseling experience treating ASD. All participants were licensed professional clinical counselors and two held a supervisor designation. All but one participant graduated with their master's in community counseling (83%). To ensure confidentiality, participants identified pseudonyms and these names were used during the data analysis process to protect their identities. To review a summary of the participants’ demographic information, see Table 1.
Demographic Table (N = 6).
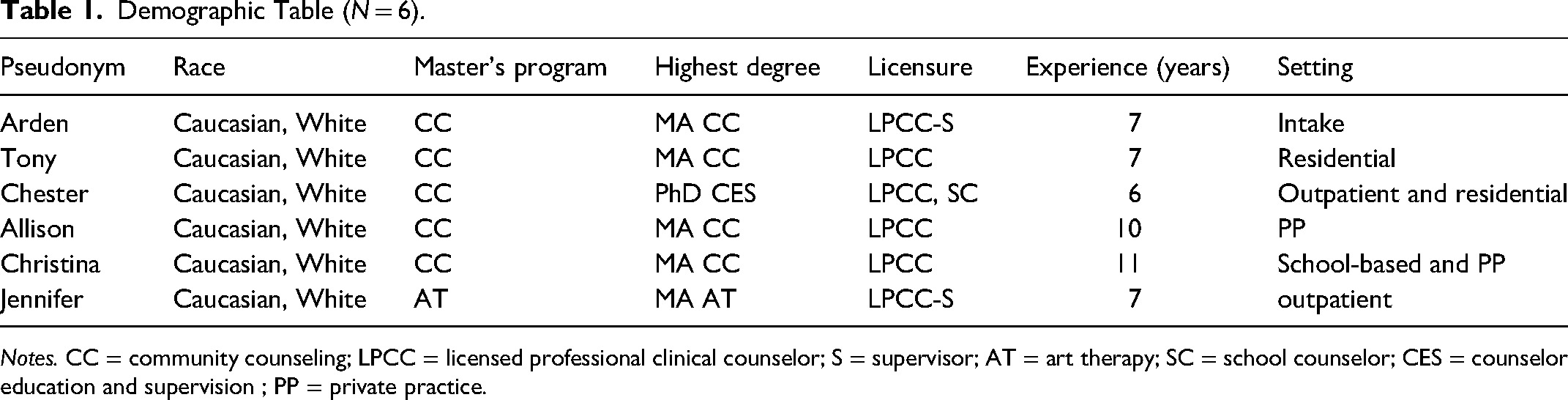
Notes. CC = community counseling; LPCC = licensed professional clinical counselor; S = supervisor; AT = art therapy; SC = school counselor; CES = counselor education and supervision ; PP = private practice.
Data Analysis
We conducted the analysis following the IPA procedure outlined by Smith et al. (2009), which consists of six distinct stages to analyze the data. The first and third authors comprised the research team. We analyzed the focus group interview and engaged in steps 1–5 individually. Step one included reading and re-reading the interview transcript to ensure our understanding and immersion within each participant's narrative and the narrative of the focus group as a whole. We made sure we listened to the recorded interview alongside the transcript to get a sense of the atmosphere, which flowed into step two. Step two consisted of initial line-by-line noting of the phenomenon, where we left content, linguistic, and conceptual comments on the left margin of the transcript. Step three involved identifying common connections across the narratives of the participants; capturing the essence and noting key terms of what the participant was describing. During step four, we developed a comprehensive list of themes and sub-themes. While identifying themes, and by honoring step five, we were cognizant of maintaining the integrity of the theme by systematically referencing the verbatim transcript to ensure the themes matched their experiences (i.e., emic) with our psychological abstraction (i.e., etic). During the final step, step 6, we met as a research team two times, where we reviewed our list of themes of potential significance and during our final meeting, solidified a master list that included direct quotes to support the themes. Throughout the data analysis process, we sought to ensure that the lived experiences of participants were reflected and that analytic procedures were transparent, coherent and rigorous.
Researchers
The first author is a counselor educator and licensed professional counselor for 10 years and supervisor for 7 years. Before licensure, she worked in a residential setting for children with low-functioning ASD and was an associate teacher at a K-12 school for ASD teaching children with high-functioning ASD. She identifies as a White, neurodivergent female, and is a mother. The third author identifies as a South-Asian, neurotypical female and was a doctoral student in a combined Counseling and School Psychology program. She has worked with children and adolescents on the ASD spectrum as a behavioral rehabilitation care provider for an agency affiliated with the Department of Developmental Disabilities, as well as administers a battery of psychological evaluations as a counseling psychologist-in-training in K-12 schools and at an outpatient clinic. Additionally, she was a research coordinator for ASD and other neurodevelopmental disorders in an outpatient hospital clinic setting. Both members of the research team have a professional background working with children with ASD and their families. We chose this study because we have seen the ASD diagnosis on the rise and families unable to access competent, skilled clinical services. We have seen firsthand that when counselors are using best practices and practicing within their scope, they can have a tremendous impact when working alongside those on the spectrum.
Before the data analysis process, the first and third authors met two times as a research team where we explored and reflected on our ontological and epistemological beliefs and thoroughly described our experiences working with children with ASD and their families, as well as how these experiences might influence the data coding and analysis process. During the second meeting, the first author provided training in the IPA framework to the third author. Our positionality to the study is outlined here: As a research team, we held a relativist ontology and believed that the nature of knowledge is transactional and subjective.
Trustworthiness
We utilized several trustworthiness strategies to increase the rigor of this study (Lincoln & Guba, 1989). When discussing our comprehensive list of themes as a research team, we engaged in peer debriefing, where we challenged our psychological abstractions during this process of solidifying themes. Disagreements were discussed until we reached a consensus. We used an audit trail to maintain all materials from the study and to organize our data collection and analysis process. Throughout the investigation, we were mindful to establish a detailed account of the research steps from the start of the research project to the reporting of the findings. We also utilized an external auditor, the second author, who read over the audit trail and engaged in a discussion with the first author regarding the intent of the name of themes based on the data analysis process. This process resulted in refining the names of themes one and two to be more accurate to the phenomenon. Finally, we utilized member checking to make sure that the voices of the participants were represented accurately. The first author emailed all participants the interview transcript and the findings section of the manuscript and asked them to review and provide feedback on accuracy based on their experience. Two participants responded to the request and their comments were encouraging with one participant stating, “I agree with the findings … The comments still relate to my experience as a counselor, even five years later and after the pandemic.”
Findings
The research team identified four themes from our phenomenological investigation: (a) assembling the pieces, (b) fundamental counselor traits; (c) client advocacy, and (d) family-centered care. These comprehensive, higher-order themes captured patterns across participants’ experiences focused on their development of building expertise when treating the diagnosis of ASD.
Assembling the Pieces
All participants noted that they built their clinical expertise, piece by piece, through supervision and mentorship, which was critical for their development. Allison added, “I think having a mentor/supervisor who has actually worked with that population is really important. I mean, from a clinical perspective, any sort of clinical expertise is fantastic … having someone [supervisor] who's done it, whether just one-on-one or like in a groupthink [group supervision] is really important for the work.” All participants agreed that collaborating with other professionals and collecting pertinent “pieces” of information about the child with ASD was essential in building clinical understanding and implementing an effective treatment plan. In terms of a multidisciplinary approach, Tony shared his experience working with various professionals, “I think it's important because, you have clinical counselors, you have social workers, and you have BCBAs; those are at least three different lenses that are looking at the client and you get different ways to problem-solve.” Allison also discussed the key role integrated care plays conceptualizing clients: Considering the OTs [occupational therapists], and speech therapists, and everything else, it just helps you to learn the needs of the kids are so complex and so, the speech therapists are really helpful in teaching you how to communicate with them, which plays a huge role into any type of counseling or therapeutic intervention. So, I think the team approach just really helps you to look at the entire picture of the person and figure out what to do, how to build a relationship or how to help them [clients] through particular moments.
Jennifer emphasized, “[Counselors should] get the releases from the family to talk to school, talk to anybody that could give you a better picture of what it looks like for them outside the office because it is not always as telling.”
Participants highlighted building clinical competence through diagnostic considerations; distinguishing ASD from other mental health disorders. Allison shared, “Sometimes people get fixated on the diagnosis and at the end of the day, who cares what the diagnosis or the label is, here's what's in front of you, here's the person with their characteristics, their personality, and their behaviors, and everything else … Work with what's in front of you.” Jennifer mentioned that when diagnosing clients, it is important to consider all the symptoms rather than focusing on ASD only, “If I had everything laid out and it [treatment that targets ASD] is still not working, something else [co-occurring disorder] must be going on.”
Before engaging in treatment planning and targeted interventions, participants identified the importance of leaning into their basic counseling skills: (a) counselor's ability to build rapport with clients and their families, (b) create a safe listening space, (c) provide humanizing respect to clients regardless of their diagnosis, and (d) be consistent, accountable, and predictable when serving clients. Specifically, Jennifer noted that being consistent and predictable assisted with building rapport, trust, and respect: “I mean it's not an intervention but the only thing I can think of is predictability. show up and be consistent. So, if you’re predictable and they [clients] know that – I mean it's not an intervention but it's the only thing that we really can provide them.” All participants noted problem-solving through “trial and error” and strategizing interventions often occurs throughout treatment. In fact, Jennifer empathized, “I think it's a lot of trial and error you know, you go out, you do it [intervention] and you see how clients respond … you could go in on the first Monday and try something and then it fails, and you have to be okay with that and go back, and go back, and go back.” Christina reflected on the importance of an individualized approach, “It's so different for each kid. You’re making their own personal treatment plan.” In addition, participants collectively agreed that “failures” or “errors” have to be acceptable, as it is part of the process when working with the ASD diagnosis since there is no “one size fits all.” Arden noted, “I think it's particularly hard because the spectrum is so big, and you can have the diagnosis but look so different from someone else that – say that for this individual, nonverbal, you know, very limited skills is going to have the same response to an intervention.”
Fundamental Counselor Traits
Participants described specific characteristics and professional dispositions counselors should possess when working with children with ASD and their families. All participants mentioned that counselors should be open-minded, adaptable, willing to learn, patient, maintain a curious position, and hold a strength-based approach. Specifically, Arden recognized, “Just to continue to be open and seeking knowledge and changing viewpoints on things that I [as a counselor] don’t know.” Allison also noted, “I think being able to think outside of the box … It's like you have that flexibility to kind of be creative and figure out what's going to work for that person [client with ASD].” Tony highlighted, “Make the conscious effort to be adaptable to help your client, I think that, you know, any clinician can work with this population. It's just – it's a matter of if you want to put in the work.” Arden held a different position, “It's [Treatment] a very slow process, which is testing all of counselors’ patience, and I don't think, from the start, that everyone is going to be able to treat this population … you just need to be able to grow and learn.” Jennifer mentioned, “You know, like you have to be flexible, and you kind of have to build that relationship and buy into their interests, otherwise none of them are gonna sit across from you in a room for a half hour and just talk.” In addition, a strength-based approach was identified as one of the core characteristics of counseling identity. Allison reflected, “I think being the person who can also point out their [client's] strengths, you know, is huge for them because they oftentimes are not recognized for the things they do well.”
Participants described how managing their own expectations, including treatment uncertainty, frustrations, and accepting mistakes, contributed to developing clinical expertise. As Chester indicated, “Rethink the expectations you have for yourself [as a counselor], and what you are going to be doing and what you are getting out of it, and in general know they [counselors] might have to wait a long time to see results.” Arden shared that a part of counseling children with ASD is to accept the fact that mistakes are naturally bound to occur when implementing treatment interventions, “It can be demoralizing, if you’re not seeing the progress then you might really start to feel negative as a therapist, like ‘I’m just not good at this, I just can’t do this work, I’m in the wrong field.” Tony echoed, “You’re going to mess up… so taking the pressure off yourself and just saying like, ‘At the very basis, my goal for this client is to help them improve something,’ you know, not fix them as a person, because it's insulting to have that mindset of, like, ‘I’m going to fix autism,’ I won’t.”
Client Advocacy
The participants described the importance of client advocacy, which encompassed two domains: (a) counselor advocacy and (b) client self-advocacy. Allison described her experience with supporting her clients and promoting inclusivity in an attempt to normalize ASD in society: I mean this sounds really basic, but I think it's just acceptance … some of our clients, we go out in the community and, you know, people stare because of whatever behavior they’re doing or noise they’re making or something like that and I think just talking to family, friends, whoever, you know, and just kind of making a, like, ‘well, that's just who they are.’ It's just normal, you know? You’re not labeling the experience as unusual.
Participants mentioned a tension can develop between the counselor and family members when the family pushes for a treatment that the child may not be ready for. Jennifer shared: We [Counselors] do become the advocates for the kids, and you kind of take it on because you’re seeing them [clients] here and you’re seeing what they’re struggling with and it's really hard to be neutral and not wanna go challenge the caregivers. So, I think in that way we end up being the advocate for the kid in a lot of ways when it probably comes to things like family therapy or with funding sources that don’t seem to have any understanding of what's going on.
As Jennifer highlighted, counselors are in a position to challenge insurance boards to advocate to provide funding for counseling services. Additionally, all participants made it clear that counselors need to be mindful of what is best for the client's well-being versus tied to a treatment goal. Chester mentioned, “When exactly are you advocating for the client and their wellness? Are we advocating for them to be more in the community but is that from our perspective of wanting more socialization … you’re also keeping in mind, maybe this [treatment goal] isn’t – this is what we [counselors, family] think of as being happy, so then you have those push and pulls … am I advocating against my own client?”
Participants indicated that professionals who work with individuals on the ASD spectrum can advocate for clients’ rights in the community and expose them to the “real world”; however, teaching individuals’ mechanisms to self-advocate is just as valuable. Jennifer disclosed her encounter with a young woman who advocated for herself: We had this girl who had autism and significant mental health issues and, you know, there was a big conversation of, like, ‘she shouldn’t go on this outing,’ and they [staff] fought and she advocated for herself to go, and it ended up being the best thing ever … I’m opening my eyes more to when the staff are coming and advocating for the students and then you know, I think it's really cool when the client can also advocate.
Family-Centered Care
Participants recounted that implementing a family-based practice is critical. Chester emphasized the importance of psychoeducation, “I think the orientation for the parents, sometimes breaking down the concerns into simplified explanations so that the end goal is that the client and the family function better.” It is also important to empathize with the family and acknowledge their experience as indicated by Christina, “I think it's important to really hear the families of everything they’ve went through … treat them [families] like they’re the expert on their child … because maybe we get them [client] when they’re fifteen and we don’t know what happened … we can see on paper what happened, but we haven’t experienced it. So, giving the parents credit that they have dealt with a lot with their child and their home.”
The counselors also discussed assisting the families with accepting the diagnosis and treatment, including setting practical expectations. As Arden mentioned, I think another thing that's really important to think about is helping families develop realistic expectations, because you want to help the family get to a point where they’re not just always going to feel disappointed, like we want them to recognize the little changes, that it might take a year to get to but, you know, to recognize even the little steps in the right direction is progress … helping them come to those, like that acknowledgement, is really – can be a turning point in, like, them understanding their child and accepting their child.
Tony noted the importance of supporting guardians with grief process: I think it's also trying to identify where are they at in the process of grieving the loss of their child and the hopes and dreams that they had before they had, you know, their kid and trying to help them cope with, you know, I see a lot of guilt with my parents, just a lot of guilt around whether it's trying to make sure the relationship stays positive or help the family realize that it's hard and you have to accept who the kid is now.
Christina also emphasized the identification of the gap between the acceptance level of one caregiver versus the other, “I think one parent might be more accepting than another parent and then that puts a divide in their relationship and I think that can be hard too.”
Discussion
The current study explored how counselors who specialize in providing ASD services make sense of their lived experiences developing expertise in the ASD population and working alongside their families. The identified themes highlight the essential function of the supervisor as a guide in building counselors’ confidence (Bernard & Goodyear, 2014; Feather et al., 2024) in treating the symptoms of ASD and enhancing clinical practice. Engaging in interprofessional collaboration also built participants’ confidence and case conceptualization skills. When participants collaborated with other ASD service providers, the care coordination efforts provided a comprehensive framework and increased their effectiveness (Antonelli et al., 2009; Feather et al., 2023).
While ASD researchers frequently explore a more systematic treatment selection for individuals with ASD, practitioners are often working with children across a spectrum where experimentation has become a typical practice (Feather et al., 2023). Similarly, participants of the current study described a “trial-and-error” process of finding an effective treatment to manage the co-occurring disorders alongside ASD (Feather et al., 2024). Echoing the research of Mosner et al. (2019), the participants’ reported the complication of co-existing conditions that accompany ASD, often having to sift through the clinical implications of treating multiple complex diagnoses at once. While this can be a difficult process to navigate, the participants of this study highlighted the importance of holding a person-centered approach; not losing sight of the “human in front of you” versus getting lost in the symptoms of the diagnosis, which affirms previous research (Feather et al., revise and resubmit).
Stappelbein et al. (2016) emphasized that consistency and predictability are key when treating autistic clients. Participants in this study provided such an environment, which they attributed to their ability to build meaningful rapport with clients (Feather et al., 2023). Participants also described the importance of monitoring the level of expectations as a counselor. Researchers in the field of counselor identity development note that if a counselor holds themselves and/or a client to unattainable standards, the counseling process will be fragmented (Puig et al., 2023). The findings of this study align with established research in counselor characteristics and dispositions (e.g., willingness to be open-minded and learn throughout the counseling process, curious position, and patience; Feather et al., 2024; Puig et al., 2023). Puig et al. (2023) summarized that through one's professional identity, counselors must be flexible, adaptive, and creative when working alongside clients. The findings illustrate how counselors must hold a strength-based approach where the focus is on clients’ internal strengths and resourcefulness, rather than a deficit-based perspective (Feather et al., revise and resubmit). Previous research by Taylor et al. (2023) found that shifting away from what an individual is lacking to celebrating strengths is a valuable method for boosting well-being among those with ASD.
The identified theme of client advocacy in this study aligns with well-established research on how caregivers who have a child diagnosed with ASD need to advocate within educational, healthcare, and social settings (Feather et al., 2023). While advocacy has also been linked to caregiver empowerment and self-efficacy (Hohlfeld et al., 2018), participants mentioned the tension they experience when the caregiver's goals for the child are outside the client's ability. In these moments, participants reported the need to advocate on behalf of their clients. Additionally, participants articulated the importance of reducing stigma and normalizing autistic behavior outside of the counseling room (i.e., in the community). These findings underscore the importance of teaching clients how to self-advocate; knowing when and how to approach others regarding needs and action steps necessary to meet the needs of clients (Leadbitter et al., 2021).
Participants noted the significance of approaching their work from a family-based practice, and multiple researchers support this approach (Feather et al., 2024; Hohlfeld et al., 2018; Neely et al., 2012). Due to the complexity of ASD, it is important to implement a family-centered care which includes: (a) orienting families to the intricacies of the diagnosis, (b) acknowledging caregivers’ varying perspectives, (c) addressing the concerns related to the child's development, (d) connecting guardians with community resources, and (e) providing caregivers with behavioral and adaptive strategies to administer at home and in community settings (Feather et al., 2024; Hohlfeld et al., 2018). Further, providing caregivers psychoeducation surrounding the ASD diagnosis and connecting them with resources in the community has led to increased caregiver self-efficacy and supported realistic treatment expectations for their child (Layne, 2007). Participants highlighted previous findings that noted the importance of counselors leaning into caregiver input to better understand the client's physical, social, developmental, and family history; caregivers are the experts of their child (Feather et al., 2023).
Finally, participants discussed the role of grief work in their counseling process, echoing previous research (Feather et al., 2023; Neely et al., 2012). Neely et al. (2012) outlined the challenges of adjusting to the diagnosis of ASD when caregivers are expecting to raise a neurotypical child. Attuning to the family's life adjustment to the diagnosis and well-being is critical (Kurz, 2018), and as the participants noted, recognizing there is a difference between the caregiver's (e.g., mother and father) acceptance of the diagnosis. These findings align with Bravo-Benítez et al. (2019) who highlight the importance of targeted interventions that focus on the feelings and manifestations of ambiguous grief that occur among caregivers to improve their well-being and quality of life.
Implications
This study has useful implications for professional counselors when building clinical competencies and engaging in best practices working with clients with ASD and their families. The findings reiterate well-established research on the importance of supervisors and clinical mentors who can build supervisees’ ASD expertise. Supervisors must foster a holistic multicultural practice, where culture and family perceptions are at the center of treatment, not at the margins (Ennis-Cole et al., 2013). Inequities in the diagnosis and treatment among non-White groups continue to plague the helping field and these glaring disparities carry serious clinical consequences (Rivera-Figueroa et al., 2022). Consistent with the research findings of Feather et al. (2023), participants indicated not only the importance of interdisciplinary collaboration to provide a different frame to conceptualize the client's presenting concerns but also building their own competence to treat the diagnosis of ASD. Obtaining the release of information from caregivers and partnering with other service providers can offer alternative viewpoints and perspectives on case management, treatment, and validity of the interventions. Dual-diagnosis concerns were highlighted in the findings, and counselors need to screen for comorbid psychiatric disorders and distinguish symptoms that relate to the core characteristics of ASD versus other mental health diagnoses (Feather et al., 2023; Yaholkoski et al., 2021). Further, the participants highlighted that counselors need to engage in a trial-and-error process when identifying an individualized treatment that meets each client's needs (Feather et al., 2024).
Basic counseling skills were also noted in the findings as a component of professional counselor identity and building expertise to treat the diagnosis (Feather et al., 2024). Counselors need to humanize their clients and not lose sight of the individual in front of them (Feather et al., revise and resubmit). Participants also articulated the fundamental professional traits that may be required when treating the diagnosis such as being: (a) creative or “think outside the box,” (b) flexible, (c) adaptive, (d) open-minded, and (e) willing to learn throughout the counseling process. Holding patience is key when working with children and families as well (Feather et al., 2024). Treatment can be slow and having realistic expectations for the client and yourself as a counselor is critical. Routine, consistency, and predictability were also highlighted by the participants. Predictability can be demonstrated in three ways: (1) by the counselor, (2) through the physical space (i.e., the counseling room), and (3) the visual support for clients to thrive in treatment. Predictability, consistency, and routine reduce clients with ASD stress levels and power struggles, improve cooperation and motivations, create an environment of security and comfort, build a strong working alliance, and boost learning (Stappelbein et al., 2016).
The counselors that participated in the study voiced how counselors are positioned to foster a strength-based approach; recognizing clients’ strengths as opposed to their deficits (Feather et al., revise and resubmit). The neurodiversity movement is pushing for practitioners to focus on skill development and active collaboration with the client to identify growth areas, rather than energy towards neurotypicality or masking (Leadbitter et al., 2021). Counselors need to speak up if a treatment goal is affecting the client's well-being and when the client is making progress, even if it is slow and/or minute. Counselors in the study recognized the importance of client advocacy to reduce stigma and normalize autistic behavior in and outside the counseling room. In addition, building self-advocacy skills with their clients and advocating on behalf of the client with family was seen as a vital component of the process.
When it comes to a family-centered care, participants identified the importance of: (a) providing psychoeducation on the child's presenting symptoms, (b) targeting any adjustment and/or grief concerns, (c) collaborating and setting realistic treatment expectations, and (d) engaging in care coordination efforts (Feather et al., 2024). Caregivers’ quality of life has been linked to their ability to process the emotional impact of their child having a lifelong condition, which may manifest into ambiguous grief and leaving space to mourn the challenges they may face is essential to meet their parental responsibilities (Bravo-Benítez et al., 2019). Counselors should provide psychoeducation to caregivers and connect them with resources in the community, which has been correlated with overall well-being and quality of life for both the child and family (Hohlfeld et al., 2018).
Limitations and Directions for Future Research
There are several limitations to this study that must be acknowledged, including the utilization of a focus group, multicultural considerations, and transferability. While focus groups are dynamic and can lead to interactive group discussions, they may also influence responses and participants may be reluctant to share different opinions (Dilshad & Ijaz Latif, 2013). Therefore, future researchers must be mindful to build rapport with all participants and encourage candidness; making sure they know all of their perspectives are important to hear. While IPA by definition requires a small, homogeneous sample (Smith et al., 2009), our sample represents the perspective of white counselors and therefore may limit transferability. Future researchers should recruit a more diverse pool of counselors who also specialize in the treatment of ASD and expand outside of a single agency. Although we recruited from a single service agency that is known for clinician expertise in ASD, future researchers should have a process to verify participant expertise. This could include engaging external individuals to nominate counseling experts in the field of ASD and engaging these individuals in a Delphi study to identify specific aspirational competencies counselors should hold to treat the diagnosis.
Footnotes
Author Note
The first author received financial support through the Southern Association of Counselor Education and Supervision's research grant. This study was approved by the University of South Carolina's Institutional Review Board. The authors certify that this study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.