
Abstract
Maternal well-being during pregnancy is associated with postnatal maternal well-being. Understanding the risk and protective factors that could have positive and negative effects around the event of childbirth is of utmost relevance. Grounded in self-determination theory (SDT), the present study aimed to investigate the link between (a) prenatal need satisfaction and depression symptoms and (b) postnatal need satisfaction, depression symptoms, and parental self-efficacy in a sample of 94 first-time mothers. Results of the cross-lagged-panel model showed significant paths for the stability of each variable (need satisfaction and depressive symptoms) over time. Additionally, a significant cross-lagged effect was observed (a) from prenatal need satisfaction to postnatal depressive symptoms and (b) on parental self-efficacy. Overall, the results show that in the short-term, the prenatal period may be associated with adjustment to motherhood and the mothering experiences in the postnatal period. SDT-based interventions should be implemented by promoting the fulfillment of basic psychological needs during pregnancy.
Keywords
Public Significance Statements
The transition to motherhood may put mothers at greater risk of distress or depressive symptoms, but the satisfaction of basic psychological needs may have a protective role against dysfunctional adjustment in the perinatal period. These findings suggest the need to increase self-determination theory (SDT) interventions in the field of motherhood.
Introduction
The transition to motherhood is an exciting and positive time of life that begins during pregnancy and continues for some time after the baby's birth (Gillis et al., 2019). However, several studies have shown variability in women's experience during motherhood, with some being more at risk than others for psychological distress (Gugliandolo et al., 2021). Indeed, at least for some women, the transition to parenthood is accompanied by decreased psychosocial well-being (Gavin et al., 2005); specifically, it can be characterized by feelings of uncertainty, distress, and anxiety, and, in some cases, clinical symptoms of stress, depression, and maladjustment (Brunton et al., 2015).
Understanding the transition to motherhood from pregnancy is essential. Maternal prenatal psychological functioning is related to postnatal maternal adjustment, which, in turn, affects the child's psychological development (Brenning et al., 2015). For example, some studies have reported similar rates of maternal depression before childbirth and in the postnatal period, particularly in the last trimester of pregnancy (Baldoni et al., 2020). Perinatal depression is a mental health problem that poses important complications for pregnant and postnatal women and has been associated with preterm birth, low birth weight, dysfunctional practical parenting practices, maternal-infant bonding, and deficits in social and cognitive skills in children (Branquinho et al., 2021). Therefore, it is crucial to identify the potential factors that may influence women's psychological functioning from pregnancy to the postnatal period. Previous studies have estimated the prevalence of depression in mothers during pregnancy to range between 3% and 20% and during the postnatal period between 15% and 30% (Brenning & Soenens, 2017; Gillis et al., 2019; Gugliandolo et al., 2021). Furthermore, while it is common for this period to be particularly stressful, excessive stress levels could lead to clinical symptoms and maladjustment in both the short and the long term (Saxbe et al., 2018). The risk of distress and maladjustment in both the pregnancy and postnatal periods is high, as depression tends to be stable over time and affects parenting or child development. For these reasons, it is important to identify some of the factors that may protect mothers against the risk of psychological distress and malaise.
A recent line of studies has begun to use the SDT (Ryan & Deci, 2017) as a theoretical framework during the perinatal period (Brenning et al., 2015; Gugliandolo et al., 2021; Nachoum et al., 2021; Reut & Kanat-Maymon, 2018). SDT addresses the processes by which individuals seek outcomes, considering the psychological needs implicated in their behavior (Ross-Plourde & Basque, 2019). These needs are universal and essential for healthy psychological and social development. Although each basic need relates to a distinct set of experiences, together they play a critical role in mental health. For this reason, recent research focuses on the link between satisfaction of basic psychological needs and the experience of well-being. The basic psychological needs consist of three components: autonomy, relatedness, and competence. The need for autonomy refers to the degree to which individuals feel volitional and responsible for their own behavior, thus the ability to make informed decisions and perceive oneself as responsible for one's behavior and acting in coherence with one's value; the need for relatedness pertains to the need to feel loved, close and valued by significant others, in short, the individual's perception of secure belongingness and connectedness to others; lastly, the need for competence refers to the need to feel confident in achieving desired goals, and involves the experience of effectiveness when performing activities and reaching one's full potential.
Satisfying these basic psychological needs or providing conditions that support an individual's experience of autonomy, competence, and relatedness enhances performance, persistence, and creativity. Conversely, the frustration of these needs, when any of the three is unsupported, depleted, or thwarted, can have a detrimental impact on well-being (Brenning & Soenens, 2017; Ryan & Deci, 2017). Thus, the satisfaction of basic psychological needs may play a protective role against dysfunctional adaptation in the perinatal period. Pregnancy poses a challenge as it requires a considerable expenditure of mental energy and practical reorganization of life (Gugliandolo et al., 2021). In addition, the postnatal period itself is a stressful time in life. Caring for the newborn, adapting to the new parental role, and being solely responsible for the baby can have negative consequences for mothers, such as worry, sadness, exhaustion, and stress, which are described as indicators of parental distress (Gillis et al., 2019). Satisfying the need for autonomy in parenting, perceiving oneself as competent in child management, and feeling connected and in a relationship with one's own child can reduce the risk of personal parental discomfort, including depressive symptoms (Brenning & Soenens, 2017; Gugliandolo et al., 2021). In addition, research has provided preliminary support for the role of these three needs in parents’ well-being, for example, in regard to the parental sense of efficacy (Gauthier et al., 2010). Since pregnancy is the anticipatory phase of the parenting role, pregnancy variables can impact mothers’ parental self-efficacy (Gao et al., 2014). For example, social support (Gao et al., 2014) and confidence in one's abilities and possibilities (van der Kaap-Deeder et al., 2015) in the prenatal period have a positive effect on parenting self-efficacy. This is important because these studies highlight how parents’ beliefs about their ability to care for their child can be associated with parent–child actions and dynamics. In fact, parental self-efficacy has emerged as a significant predictor of parenting skills and behaviors, such as the ability to understand and respond to child signals (Boivin et al., 2005; Gao et al., 2014). Indeed, Haslam et al. (2006) found an association between higher maternal self-efficacy and lower levels of depressive symptoms in the postnatal period. When faced with stressful situations, mothers with low self-efficacy are more likely to give up and attribute failure internally, resulting in negative affect. Conversely, mothers with high self-efficacy are more confident, make internal attributions of success, and experience less negative affect. Maternal self-efficacy has been identified as a central factor in maternal adjustment, maternal–infant bonding, and parent and child satisfaction. It is imperative to create conditions during pregnancy that can reduce the risk of low perceived self-efficacy. Past experiences influence self-efficacy (Gao et al., 2014), so creating opportunities that satisfy mothers’ needs and reduce their risk of depressive symptoms may be beneficial for their well-being during this time.
Given that only a few studies to our knowledge have focused on the transition to motherhood within the theoretical framework of the SDT (Brenning & Soenens, 2017; Gauthier et al., 2010), further research is warranted. Prenatal depressive symptoms and being self-determined can be considered two critical components of overall well-being in the context of early parenting.
The Present Study
The general objective of the present study was to examine changes in the associations between the satisfaction of basic psychological needs, depressive symptoms, and perceived parental self-efficacy from prenatal to postnatal. Given that the transition period after childbirth is considered to last up to 3 months (Gillis et al., 2019) and is crucial for family bonding and adjustment, and that many of the physical, psychological, emotional, and social effects of pregnancy continue during this fourth trimester (Matambanadzo, 2014), women were contacted during pregnancy and 3 months after childbirth.
The aim was to investigate the association of effects between constructs using cross-lagged models. These models are well-suited for inferring whether (a) basic psychological needs satisfaction at T1 would have a negative cross-lagged effect on depressive symptoms at T2, (b) depressive symptoms at T1 would have a negative cross-lagged effect on basic psychological needs satisfaction at T2, (c) basic psychological needs satisfaction and depressive symptoms at T1 would have a positive and negative cross-lagged effect, respectively, on parental self-efficacy at T2, and (d) the stability of each variable (basic psychological needs satisfaction and depressive symptoms) across time (T1 and T2).
Method
Participants
A total of 94 first-time mothers participated in this study, with ages ranging from 20 to 43 years old (M = 32.31, SD = 4.45) and were urban participants. At the time of the first measurement, the average duration of the relationships with their partners was 7.75 years (SD = 4.09). Among the 94 women, 60% were married, 3% were in civil partnerships, and 37% were cohabitants. Regarding the level of education, 45% of the participants had earned a first-level degree, 35% had a high school diploma, 18% a post-laurea education, and 2% had a middle school diploma.
At Time 1, the women were predominantly in the last trimester of gestation (months: M = 7.96, SD = 1.04). In terms of the clinical history, the majority of the mothers were under the care of a public gynecologist (76%), had undergone more than five ultrasound scans (66%), and had started taking folic acid when the pregnancy started (67%). With reference to possible problems during pregnancy, 58% reported not experiencing any problems, and 34% only had minor pathologies (e.g., nausea, high blood pressure, loss of appetite, and headaches).
At Time 2, the participants were contacted 12 weeks postnatal when the baby was four months old (M = 3.98, SD = 2.52). It is worth noting that 26% of the mothers had returned to work at this point.
Procedure
The current study presents preliminary findings of an ongoing larger study and data collection, and a preprint has been made publicly available and searchable on Open Science Framework. The expectant mothers in this study were recruited through collaboration with clinics and hospitals in Sicily and Calabria that offer courses in preparation for childbirth or gynecology services and pregnancy support services. Those who expressed their willingness to participate in the research completed a paper questionnaire during pregnancy and were subsequently contacted via email to fill out an online questionnaire approximately 3 months after their expected date of birth. Only women who completed both waves of data collection were included in this study, and multiparous mothers were excluded. Participants were provided information about the study's design, and they gave their voluntary consent to participate. They were assured that their data would be treated confidentially, and they had the freedom to withdraw from the study at any time without providing a reason. Throughout the research process, the confidentiality and privacy of the participants were guaranteed. This study adhered to the ethical standards outlined in the Helsinki Declaration and received approval from the Local Ethics Committee Board. Only expectant mothers who provided signed informed consent forms were eligible to participate.
Measures
Need Satisfaction
The Basic Psychological Need Satisfaction and Frustration Scale (BPNSF; Chen et al., 2015; Costa et al., 2018) was used in this study. Mothers filled out a shortened version of the BPNSF, which consists of 12 items (e.g., “I feel a sense of choice and freedom in the things I do”) divided into six subscales that tap into the satisfaction and the frustration of each of the three basic psychological needs (need for autonomy, need for competence, and need for relatedness). The items are presented after the item stem: “Think in general about this period of pregnancy…” for Time 1 and “Think in general about this period after the birth of your child …” for Time 2. Following procedures (Van der Kaap-Deeder et al., 2020), need frustration items were reversed and averaged with the need satisfaction items into an overall score for need satisfaction that was used in this study. Participants evaluated each item thinking about their life during the pregnancy and postnatal period on a five-point Likert scale ranging from 1 (not true at all) to 5 (completely true). The reliability and validity of BPNSF have been documented extensively (Chen et al., 2015; Liga et al., 2020), and internal consistency in this study was adequate (Table 1).
Descriptive Analyses and Correlations.
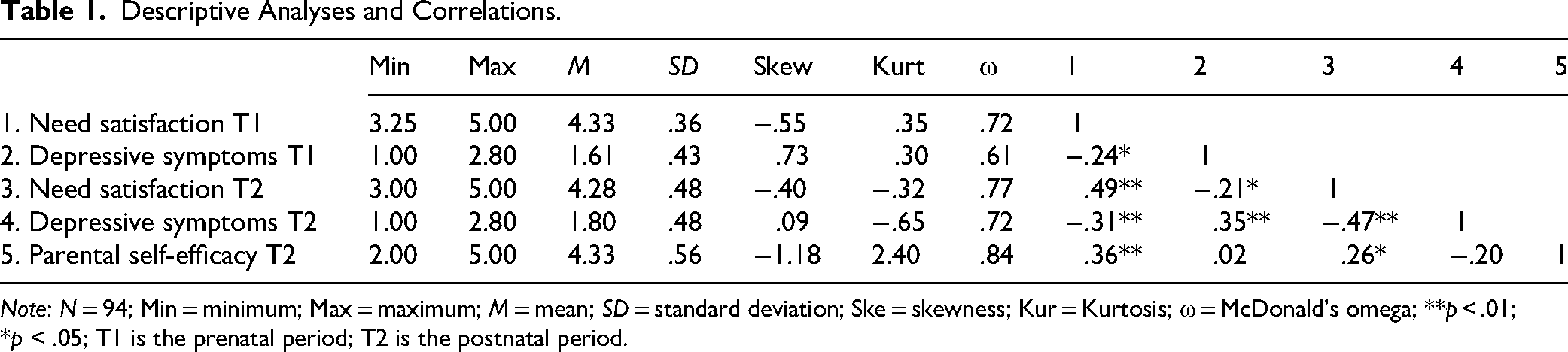
Note: N = 94; Min = minimum; Max = maximum; M = mean; SD = standard deviation; Ske = skewness; Kur = Kurtosis; ω = McDonald's omega; **p < .01; *p < .05; T1 is the prenatal period; T2 is the postnatal period.
Depressive Symptoms
Women's depressive symptoms were assessed using the short five-item version of the Center for Epidemiologic Studies Depression Scale (CES-D; Bohannon et al., 2003; Radloff, 1991) on a four-point Likert scale ranging from 0 (not at all or less than 1 day last week) to 3 (most/all of the time, 5–7 days last week). Using the CES-D, participants rated how often they had experienced cognitive, somatic, and psychological symptoms of depression during the previous week (e.g., “During the past week, I felt sad”).
The psychometric characteristics of the CES-D have been well shown in previous studies (Olino et al., 2012; Radloff, 1991) and have been documented extensively in the perinatal literature (Baldoni et al., 2020; Brenning et al., 2015; Gugliandolo et al., 2021; Hall et al., 2014; Reut & Kanat-Maymon, 2018). Internal consistency in this study has been reported for Time 1 and Time 2 in Table 1.
Parental Self-Efficacy
To capture the maternal self-efficacy during the postnatal period, the subscale “Parental self-efficacy” of the Parental Cognitions and Conduct Toward the Infant Scale was used (Boivin et al., 2005; Teti & Gelfand, 1991). This subscale refers to the women's perceived ability to carry out tasks associated with the parental role, specifically within the context of caring for an infant. It is composed of six items (e.g., I feel that I am very good at calming my baby down when he/she is upset, fussy, or crying) rated on a seven-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree).
The subscale has been shown to be a valid and reliable measure in past research (Boivin et al., 2005; Gauthier et al., 2010). In the current sample, McDonald's omega was adequate (Table 1).
Data Plan
Preliminary analyses were conducted using the IBM SPSS statistical software. Descriptive statistics such as means, standard deviations, minimum and maximum values, skewness, and kurtosis were calculated for all the study variables. Pearson correlations and independent t-tests were also performed for relevant comparisons. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
To test the cross-lagged path model, the “lavaan” package in the open-source software R was utilized. In such a path, each observed variable at T1 is associated with itself at T2 and the reciprocal cross-lagged paths between variables at T1 (need satisfaction and depressive symptoms) and variables at T2 (need satisfaction, depressive symptoms, and parental self-efficacy). Robust machine learning was used to account for potential violations of the multivariate normal distribution. The cross-lagged structural model (Figure 1) was tested. This model included the observed variables for need satisfaction and depressive symptoms at both measurement times (T1 and T2) and parental self-efficacy (T2).
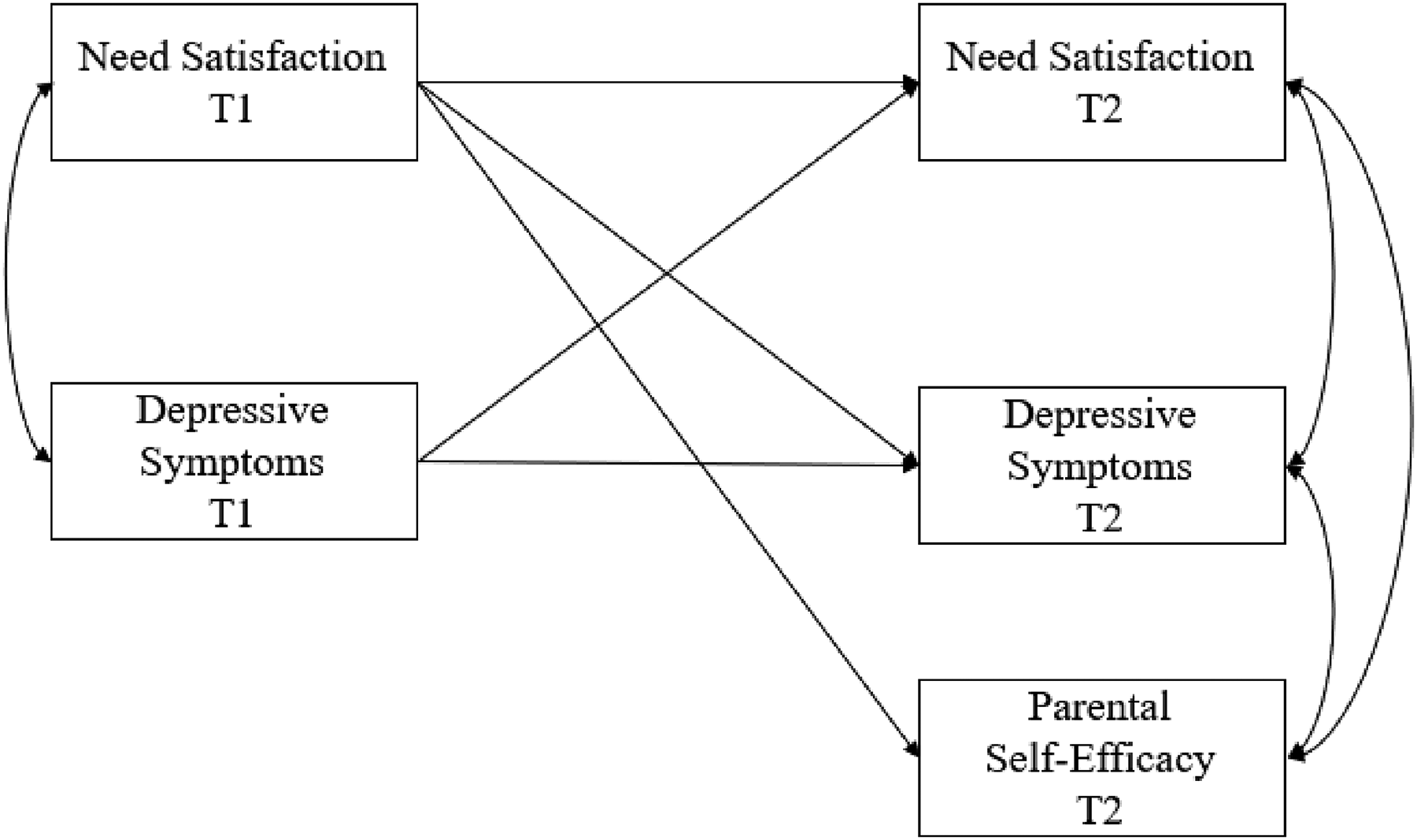
Hypothesized cross-lagged model.
The cross-lagged model hypothesized is defined by the paths from the two observed variables at T1 (need satisfaction and depressive symptoms) to all the same three and new observed variables at T2 (need satisfaction, depressive symptoms, and parental self-efficacy). Need satisfaction at T1, and depressive symptoms at T1 were allowed to correlate with each other, and in the same way, need satisfaction at T2, depressive symptoms at T2, and parental self-efficacy at T2 were allowed to correlate (Burkholder & Harlow, 2003; Orth et al., 2024).
Three models were tested and compared: the full, the baseline model, and the trimmed models. The full model tested included stability paths, correlations within time points, and cross-lagged paths. The baseline model was a model that took account of stability paths and correlations within time points. Finally, the trimmed model was trimmed to obtain the most parsimonious model. The trimmed model included all significant stability paths and cross-lagged paths emerged from the initial model, omitting all nonsignificant paths. This process helps identify the model that best fits the data and provides the most concise representation of the relationships among variables.
Results
Descriptive and Preliminary Analyses
From a sample of 630 expectant mothers, the 94 women who participated in both T1 and T2 were included in the study. In order to verify the effect of this attrition, a t-test for independent groups with basic psychological needs satisfaction and depressive symptoms as test variables was used. No attrition occurred between T1 (i.e., pregnancy) and T2 (i.e., 3 months postnatal). Statistical comparisons between women who dropped out and women who completed the two times revealed no statistically significant differences in the level of variable basic psychological needs satisfaction, t(625) = −1,045, p = .30, and depressive symptoms, t(625)= −744, p = .46.
The descriptive statistics and correlations for the study variables are presented in Table 1. Correlational analysis showed that prenatal basic psychological needs satisfaction moderately and negatively correlated with postnatal depressive symptoms (r = −.31, p < .01), strongly and positively with postnatal basic psychological needs satisfaction (r = .49, p < .01). In addition, prenatal depressive symptoms weakly and negatively correlated with postnatal basic psychological needs satisfaction (r = −.21, p = .05), moderately and positively with postnatal depressive symptoms (r = .35, p < .01). Regarding the association with parental self-efficacy, only basic psychological needs satisfaction correlated significantly. Specifically, prenatal basic psychological needs satisfaction was weak and positively correlated with parental self-efficacy (r = .36, p < .01). No significant correlations were found between prenatal depressive symptoms and parental self-efficacy (r = .02, p > .05).
Cross-Lagged Path Analysis
The baseline model, which took account of stability paths and correlations within time points, shows insufficient fit indices, χ2(4) = 19.19, p = .00, Y–Bχ2(4) = 22.19, p = .00, comparative fit index (CFI) = .77, root mean square error of approximation (RMSEA) = .20, 90% CI [0.12, 0.30], standardized root mean square residual (SRMR) = .11. Inserting a process including all stability paths, correlations within time points, and cross-lagged paths, the model is saturated so fit indices cannot be estimated. Finally, with the trimmed model deleting all nonsignificant paths and including all significant stability paths and cross-lagged paths emerged from the full model, considering that the full model is saturated (zero degrees of freedom), the chi-square difference test is equivalent to the significance of the chi-square value of trimmed models, χ2(4) = 4.66, p = .32, Y–Bχ2(4) = 4.51, p = .34, CFI = .99, RMSEA = .04, 90% CI [0.00, 0.17], SRMR = .04. Results showed good fit indices and a not significant chi-square value, suggesting that the full model may be the more parsimonious.
The cross-lagged full model was used to test the proposed model (Figure 1), and the model obtained is shown in Figure 2. Results of the cross-lagged-panel model showed significant paths for the stability of each variable across time: need satisfaction from T1 and T2 (β = .47, p < .01), depressive symptoms from T1 and T2 (β = .29, p < .01). A significance cross-lagged effect was also shown from need satisfaction at T1 to depressive symptoms at T2 (β = −.23, p = .01) and parental self-efficacy at T2 (β = .39, p = .01).
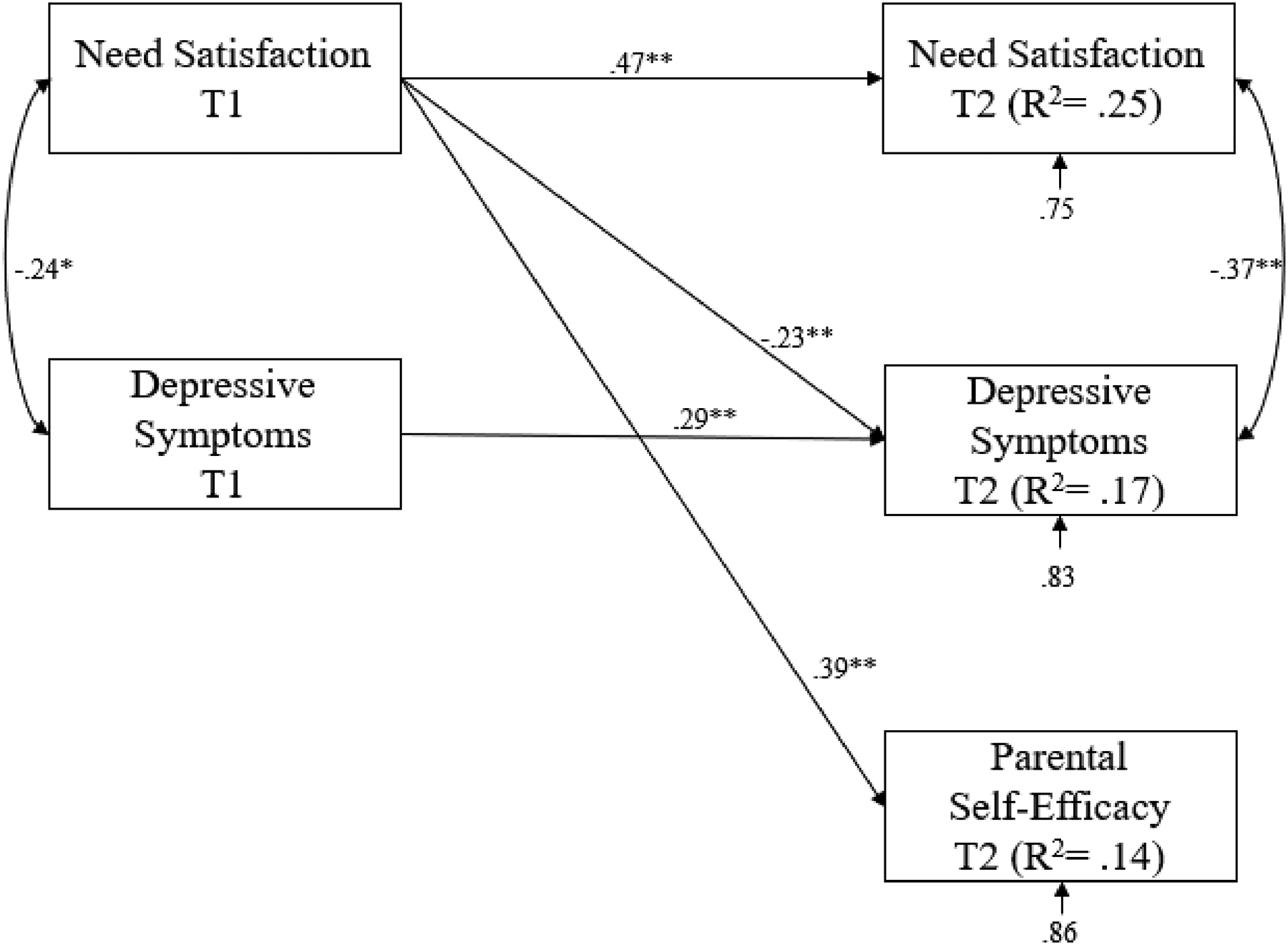
Graphical representation of the cross-lagged path analysis (N = 94); standardized path coefficients. **p < .01; *p < .05.
Discussion
This study aimed to examine the relations between basic psychological needs, depressive symptoms, and perceived parental self-efficacy in women contacted during pregnancy and 3 months after childbirth. To test the hypotheses, a two-wave cross-lagged model was implemented, and results showed significant paths for the stability of each variable (need satisfaction and depressive symptoms) across time. Furthermore, prenatal needs satisfaction is related to postnatal depressive symptoms and parental self-efficacy.
The first hypothesis of this study explored the cross-lagged effect of prenatal psychological need satisfaction on postnatal depressive symptoms. Results showed that prenatal psychological need satisfaction related negatively to postnatal depressive symptoms. These results align with the main principles of SDT, which emphasize the importance of basic psychological needs for well-being and psychological adjustment (Ryan & Deci, 2017). Women's feelings of confidence in one's own ability (competence needs satisfaction), experiences of connection and intimacy (relatedness needs satisfaction), and feelings of being independent and guided by internal and approved choice (autonomy needs satisfaction) are assumed to be particularly relevant when investigating postnatal depressive symptoms (Brenning & Soenens, 2017; Gauthier et al., 2010).
Contrary to expectations, for the second hypothesis, prenatal depression was not found to be related to basic postnatal psychological needs, although prenatal depressive symptomatology has often been reported as the best predictor of postnatal adjustment problems. It is possible that the lack of official recognition and less distinct or clear symptoms of depression during pregnancy contributed to this finding. It is also important to note how common it is for expectant mothers to feel a sense of unease that is not necessarily pathological. However, with adequate social support and personal resources, the natural changes and psychological adaptations required during pregnancy may not necessarily pose a risk for postnatal adjustment difficulties (Tissera et al., 2021).
In addition, we proposed to test the link between depressive symptoms and psychological need satisfaction during pregnancy with perceived parental self-efficacy three months after childbirth. The results showed that only prenatal needs satisfaction was related to parental self-efficacy. The satisfaction of women's need for competence, relatedness, and autonomy seemed to present an important resource in the perception of being a good parent and in influencing mothers’ beliefs about their ability to take care of their child. Indeed, some early determinants of parenting perceptions and behaviors, according to which the quality of parenting is influenced, are the parent characteristics (Boivin et al., 2005). Mothers are led by their needs, which play a prominent role in the development and adjustment to the new parental role and in their early interactions with the young child, such that may influence their beliefs and expectations about parenting. The present study makes it possible to observe that the satisfaction of women's psychological needs during pregnancy is a critical resource for new mothers. That is, basic psychological needs would help to explain why some mothers are more satisfied in motherhood than others. According to van der Kaap-Deeder et al. (2015), when mothers experience in general a sense of psychological freedom and volition (i.e., autonomy satisfaction), feel able to effectively engage in daily activities (i.e., competence satisfaction), and feel related to other persons (i.e., relatedness satisfaction), they are likely to have more parental self-efficacy and with feelings of satisfaction with one's parenting. In contrast, as in the study by Gauthier et al. (2010), the results of the present research show that the link between prenatal depressive symptoms and perception of parenting quality was nonsignificant. However, these results suggest that depression symptoms may not be a primary determinant of the self-efficacy experienced by new mothers in the first months after childbirth. This is due to the fact that maternal self-efficacy has a protective role against depressive symptoms during motherhood (Haslam et al., 2006). Moreover, since the perception of self-efficacy grows over time and with experience, it is likely to be assumed that any prenatal depressive symptoms may not have a total impact on parental self-efficacy. Despite this, the role of this construct later on cannot be excluded; for example, with more life experience, mothers may become more conscious of their personal strengths and weaknesses, so that their parental self-efficacy becomes more highly correlated with depressive symptoms (Gauthier et al., 2010).
Regarding the latter hypothesis, prenatal depressive symptoms are related positively to maternal depressive symptoms three months after childbirth. Effectively, studies focused on the perinatal period found that depression during pregnancy is one of the strongest risk factors for maternal depressive symptoms during the early postnatal period (Cena et al., 2021). Since depressive symptoms are not always transitory, but can also relate to postnatal depressive symptoms, it is important to focus on these specific domains precociously. The last hypothesis also showed a positive association between basic psychological needs satisfaction during pregnancy and specific psychological needs satisfaction after childbirth. These results are in line with previous research that focused on the interrelation between psychological need satisfaction at the general and specific experience (Milyavskaya et al., 2013). Psychological need satisfaction at two distinct levels of experience contributes to well-being, both measured concurrently and prospectively. In other words, during pregnancy, women who generally feel competent are more likely to experience feelings of competence while interacting with their child, and women who feel autonomous are more likely to experience choice and psychological freedom in childcare. Lastly, women who generally express a need for relatedness are more likely to feel close and intimate with their babies.
It is important to acknowledge the limitations of this study. The use of self-report questionnaires and measures adapted to the perinatal period limits the accuracy of the results. Future studies could use specific and periodic measurements during the prenatal and postnatal periods. A second limitation is that several other variables could be relevant to understanding these relations. Future studies could integrate with other outcome variables, such as perception of perceived support, which could affect the adaptation and well-being of mothers during the transition to motherhood. Also, depressive symptoms were operationalized in this study in terms of frequency of depressive feelings, not in terms of severity. Future research could use more differentiated instruments to assess well-being and malaise. Future studies should confirm these findings by implementing longitudinal designs with these variables. Finally, this study was based on a convenience sample limited to heterosexual expectant mothers who mainly participate in childbirth preparation courses. The findings may not be generalizable to women with different relationships or conditions.
Overall, these results highlight the importance of need satisfaction when investigating individual well-being in new mothers during the transition to motherhood, a time of uncertainty and changes. Although basic needs can be affected by daily fluctuations, results provide evidence that psychological need satisfaction creates a long-term positive experience during the transition to motherhood. Indeed, Mabbe et al. (2018) suggest that parents could be advised to organize their daily lives as much as possible around experiences that satisfy their needs, and to be mindful of experiences that frustrate them.
This result has a strong practical implication, suggesting that it is important during pregnancy that the future mothers feel satisfied in their needs for autonomy, competence, and relatedness. In light of this, it is essential to prevent expectant mothers from having negative experiences, such as depressive symptoms, and to promote greater perceptions of self-efficacy. There is strong evidence for the effectiveness of SDT-based interventions across a wide range of health domains (Gillison et al., 2019). These studies have examined how the satisfaction of these three psychological needs predicts autonomous motivation, adaptive behavior, and psychological and physical health (Ntoumanis et al., 2021). From an application point of view, it is important to implement evidence-based programs aimed at satisfying mothers’ basic psychological needs.
Footnotes
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
MG: Conceptualization, methodology, formal analysis, data curation, and writing—original draft. MCG: Conceptualization, data curation, and writing—review & editing preparation. FL: Conceptualization, visualization, and supervision. SG: Conceptualization, visualization, and supervision. All authors take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to and have approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Research Involving Human Participants and/or Animals
This research involves human participants. The authors complied with the American Psychological Association's ethical standards in the treatment of participants for this work. This research has been approved by the local institutional research ethics committee (IBM/Committee of CeRip of the University of Messina, Protocol no. 0092084 of 3 October 2019). No animals were involved in this study.
Data and Code Availability
The data and the code that support the findings of this study are available from the corresponding author upon request.