
Abstract
Children with chronic medical needs and their families encounter multifaceted and intersecting challenges, including heightened psychological stress, emotional burden, financial strain, educational barriers, and caregiver burnout. Although existing literature has begun to document these difficulties, it often falls short in capturing the depth, complexity, and meaning embedded within parents’ lived experiences. To address this gap, the present hermeneutic phenomenological study centers the voices of parents raising children with chronic medical needs through in-depth qualitative interviews. By examining how parents interpret and navigate these experiences, this study offers nuanced insights that extend beyond surface-level descriptions of burden. The findings provide meaningful implications for counselors seeking to deliver developmentally responsive, systemic, and family-centered support to this population.
Parenthood represents a significant developmental and relational transition, during which caregivers must navigate evolving roles, sociocultural expectations, and internalized beliefs about what it means to parent effectively (Adams et al., 2021; Orton-Johnson, 2017; Scharp & Thomas, 2017). Within a family systems framework, parenting is understood as a dynamic and often paradoxical experience, characterized by the coexistence of profound joy and considerable stress (Schoppe-Sullivan et al., 2017). These complexities are further intensified for parents of children with chronic medical needs, who must simultaneously manage typical developmental demands while responding to ongoing medical, emotional, and systemic challenges (Myers et al., 2009). For family counselors, this population highlights the importance of attending to the interconnected nature of individual, relational, and contextual stressors, as chronic illness not only impacts the identified child but reverberates across the entire family system.
Understanding the Prevalence of Children With Chronic Medical Needs
Children with chronic medical needs are described using a range of overlapping terms, including complex chronic illness, pediatric medical complexity, special health care needs, life-limiting conditions, and multiple complex needs (Gallegos & Cacchillo, 2023). These classifications encompass a broad spectrum of diagnoses, including respiratory diseases, diabetes, mental health conditions, vision impairments, oral diseases, and genetic or musculoskeletal disorders (Midence, 1994; Myers et al., 2009). Across these conditions, a unifying feature is the requirement for ongoing adaptation, as these diagnoses are typically persistent, not curable, and embedded in the daily lives of children and their families. Such conditions often involve symptom variability, chronic pain, fatigue, and frequent medical interventions, all of which shape family routines and relational dynamics (Kinzel, 1993; Lee & McCormick, 2002; Morse, 1997). For the purposes of this study, the term chronic medical needs is used to broadly capture these ongoing health conditions in children under the age of 18.
The prevalence of children with chronic medical needs has increased substantially over time, rising more than 400% since the 1960s and now affecting approximately 20% of children in the United States, or an estimated 13.6 million individuals (Gallegos & Cacchillo, 2023). Advances in medical care have contributed to increased survival rates for conditions that were once considered terminal, resulting in more children reaching adolescence and adulthood with complex health needs (Kennedy et al., 2007). While these advancements represent significant medical progress, they also introduce ongoing demands for families, who must navigate complex healthcare systems, coordinate care, and adapt to evolving developmental and medical challenges over time.
From a family counseling perspective, the increasing prevalence of chronic medical needs underscores the importance of understanding how these conditions extend beyond the individual child to influence the entire family system. Parents often assume expanded caregiving roles that require sustained engagement with medical providers, frequent appointments, and ongoing advocacy, all of which can be both time-intensive and emotionally taxing (Kennedy et al., 2007). These systemic demands have implications for family functioning, including shifts in roles, routines, and relational patterns. As such, family counselors are uniquely positioned to support families in navigating these complexities by attending to both the practical and emotional dimensions of chronic illness within a systemic and relational framework.
Parental Mental Health and Systemic Implications in Families of Children With Chronic Medical Needs
Parents of children with chronic medical needs experience a complex constellation of psychological, relational, and systemic challenges that extend beyond individual stress and significantly impact overall family functioning. These challenges include elevated parenting stress, financial strain, employment instability, and barriers to securing equitable and inclusive educational opportunities for their child (Arafa et al., 2008; Klassen et al., 2008). Within a family systems framework, these stressors are not isolated to the individual caregiver but reverberate across the entire family unit, influencing marital relationships, sibling dynamics, and broader support networks. The emotional burden associated with caregiving is particularly profound, as many parents describe an ongoing sense of ambiguous loss while attempting to reconcile expectations for their child's future with their present realities (Klassen et al., 2008). In addition to grief, parents frequently report experiencing stress, uncertainty, anger, and marginalization within both social and spiritual contexts, including the impact of ableism and barriers to community support (Arafa et al., 2008; Klassen et al., 2008). These intersecting challenges compound normative parenting demands, positioning caregivers at increased risk for psychological distress and relational strain.
Parenting Stress and Mental Health Outcomes
Parenting stress is a pervasive and well-documented experience among caregivers of children with chronic medical needs (Cousino & Hazen, 2013; Klassen et al., 2008). Empirical research consistently demonstrates that parents of children with chronic illness report significantly higher levels of stress compared to caregivers of typically developing children (Cousino & Hazen, 2013). This elevated stress is often associated with the ongoing responsibility of managing complex treatment regimens, coordinating care, and responding to fluctuating health conditions. Moreover, increased parenting stress has been linked to poorer psychological adjustment in both caregivers and children, underscoring the bidirectional nature of distress within family systems (Cousino & Hazen, 2013).
Meta-analytic findings further indicate that chronic caregiving demands contribute to higher rates of depression among parents, with estimates suggesting a 10% increase in clinical depression among caregivers of children with developmental disabilities (Singer, 2006). Parental mental health challenges have cascading effects on family functioning, including increased anxiety and depression in children, diminished academic performance, occupational impairment among caregivers, and strain in marital and parent–child relationships (Dyson et al., 1989; Fisman & Wolf, 1991; Pilowsky et al., 2006). From a family counseling perspective, these findings highlight the importance of assessing caregiver well-being as an integral component of treatment, as parental distress can significantly shape relational dynamics and child outcomes.
Financial Strain and Employment Disruption
In addition to psychological stress, families of children with chronic medical needs often experience substantial financial strain and employment instability. The costs associated with ongoing medical care, transportation to appointments, and specialized treatments can accumulate rapidly, placing significant pressure on family resources (Brown et al., 2008). These financial demands frequently intersect with disruptions in employment, as caregivers may need to reduce work hours, take unpaid leave, or exit the workforce entirely to meet caregiving responsibilities (Foster et al., 2021). Such disruptions can lead to reduced income, diminished savings, and limited long-term career opportunities (Gallagher et al., 2008; Schulz & Sherwood, 2008).
Although policies such as the Family and Medical Leave Act aim to provide protections for caregivers, eligibility limitations exclude many families, particularly women and individuals working part-time or multiple jobs (Heymann et al., 2021; U.S. Department of Labor, n.d.). As a result, families often navigate ongoing financial insecurity, with research indicating that approximately 30% of families experience income loss or job disruption due to their child's medical needs (Heyman et al., 2021). From a systemic counseling lens, these economic stressors are critical to consider, as financial strain is closely linked to increased relational conflict, caregiver burnout, and reduced access to supportive resources.
Educational Barriers and Advocacy Demands
Educational systems represent another significant domain in which families encounter challenges. While education is recognized as a fundamental human right and international frameworks advocate for inclusive and equitable access (United Nations, 2006; Ackerman & Willis, 2019), parents of children with chronic medical needs often report that securing appropriate accommodations is an ongoing and burdensome process. Advocacy efforts can be time-intensive and emotionally taxing, requiring parents to navigate complex institutional systems and, at times, challenge resistance or misunderstanding from school personnel (Ackerman & Willis, 2019; Brown & Leigh, 2020).
The fluctuating nature of many chronic conditions further complicates educational planning, as children's needs may vary over time in ways that are not always well understood by educators (Brown & Leigh, 2020). Parents frequently advocate for accommodations such as extended time, modified participation, virtual learning options, and flexibility for medical appointments. These advocacy demands can contribute to caregiver fatigue and strain family–school relationships. Family counselors can play a pivotal role in supporting parents in these processes by facilitating communication, empowering advocacy efforts, and addressing the emotional toll associated with navigating educational systems.
Emotional Complexity and Grief
The emotional landscape of parenting a child with chronic medical needs is multifaceted and often characterized by the simultaneous presence of conflicting emotions. Parents frequently report feelings of inadequacy, guilt, helplessness, and hypervigilance, alongside moments of hope, pride, and connection. Central to this experience is a form of chronic or ambiguous grief, as parents navigate the ongoing tension between expectations and evolving realities. This grief is not confined to a single event but persists over time, often resurfacing at developmental milestones or during periods of medical uncertainty (Heyman et al., 2021).
From a family counseling perspective, recognizing and normalizing this emotional complexity is essential. Counselors are uniquely positioned to support parents in processing grief, fostering meaning-making, and developing adaptive coping strategies that account for both the challenges and resilience inherent in their experiences.
Despite a growing body of research on chronic illness and caregiving, much of the existing literature has relied on quantitative methodologies that emphasize measurable outcomes such as stress, depression, and financial burden. While these approaches provide important insights, they often fail to capture the depth and nuance of parents’ lived experiences. As a result, the voices of parents raising children with chronic medical needs remain underrepresented, particularly within family counseling literature.
This gap is significant, as an incomplete understanding of caregiver experiences may limit counselors’ ability to provide responsive, systemic, and family-centered care. Therefore, there is a critical need for qualitative inquiry that centers parental voices and examines how families interpret, navigate, and make meaning of their experiences. The present study seeks to address this gap by offering a phenomenological exploration of parenting children with chronic medical needs, with the goal of informing more effective and compassionate counseling practices for families.
Method
This study employed a hermeneutic phenomenological approach to explore the lived experiences of parents raising children with chronic medical needs. Phenomenological methodologies aim to capture and interpret how individuals make meaning of their experiences (Bhattacharya, 2017; Polit & Beck, 2018). Consistent with hermeneutic phenomenology, this study acknowledged that the researcher's prior knowledge and experiences are not bracketed but instead engaged as part of an ongoing interpretive process. This interpretive stance allowed for a dynamic understanding of participants’ experiences as meaning was co-constructed through analysis.
Researcher Positionality and Reflexivity
The researcher brought both personal and professional experiences related to pediatric illness and family systems into the research process. In alignment with hermeneutic phenomenology, these experiences were not set aside but critically examined throughout the study. Reflexivity was maintained through ongoing journaling conducted before and after each interview, documenting assumptions, emotional responses, and evolving interpretations. This process functioned as part of the hermeneutic circle, allowing the researcher to continually revisit and refine understanding. An external auditor was also engaged to review emerging themes and support analytic rigor, enhancing the transparency and trustworthiness of the findings.
Participants and Recruitment
Participants were recruited using purposive sampling to ensure alignment with the research focus. Inclusion criteria required participants to be over the age of 18 and to have a child under the age of 18 with chronic medical needs. Individuals whose children had solely neurodevelopmental diagnoses (e.g., intellectual disabilities, learning disabilities, attention-deficit/hyperactivity disorder, or autism spectrum disorder) were excluded to maintain focus on chronic medical conditions.
Recruitment flyers were distributed via email to child life specialists at multiple hospital systems, including University Hospitals, Nationwide Children's Hospital, University Hospital, and Akron Children's Hospital. Flyers were also shared across professional and community-based social media platforms and listservs, including Ohio Mental Health Professionals and the Ohio Counseling Association. Five individuals expressed interest and subsequently completed the study. No participants withdrew after providing consent.
Procedures
Interested participants contacted the researcher via email and were scheduled for individual interviews following IRB approval. Prior to participation, individuals received a Microsoft Teams interview link, a Qualtrics survey to collect demographic information, and an informed consent document. Participants reviewed the consent form and provided electronic consent before beginning the interview. All procedures were conducted in accordance with ethical research standards.
Data Collection
Data were collected through semi-structured interviews conducted via Microsoft Teams. Interviews were audio-recorded with participant permission and later transcribed using transcription software (e.g., Otter.ai) and verified for accuracy through comparison with the original recordings. Interviews included open-ended questions designed to elicit participants’ lived experiences.
As part of the interview process, participants were invited to share an image that represented their experience of parenting a child with chronic medical needs. This technique aligns with phenomenological approaches that facilitate deeper reflection and meaning-making by allowing participants to express experiences symbolically, particularly when aspects of those experiences may be difficult to articulate verbally.
Data Analysis
Data analysis followed an iterative process consistent with hermeneutic phenomenology. Transcripts were read multiple times to achieve immersion in the data. Meaning units were identified based on emotional salience, repetition, and relevance to the research question. These meaning units were then clustered into broader themes through ongoing comparison across participants. Analysis occurred concurrently with data collection, allowing themes to be refined as additional interviews were conducted. Data saturation was reached when no new themes emerged, and participant responses reflected redundancy across interviews. Participant-provided images were also incorporated into the analytic process as additional sources of meaning, contributing to the identification and refinement of themes.
Trustworthiness
Several strategies were employed to enhance the trustworthiness of the study. First, member checking was conducted by returning transcripts to participants for review; no participants requested substantive revisions beyond minor grammatical corrections. Second, an external auditor reviewed transcripts and emerging themes to support credibility and reduce researcher bias. Third, reflexive journaling was used throughout the research process to document the researcher's assumptions and evolving interpretations. These strategies collectively contributed to the credibility, dependability, and confirmability of the findings.
Demographic Data
All participants completed a demographic questionnaire prior to the interview. Data collected included age, gender, race, child's diagnosis, age at diagnosis, employment status, educational background, and whether participants had additional children with chronic medical needs. Table 1 details participant demographics.
Participant Demographic Characteristics.
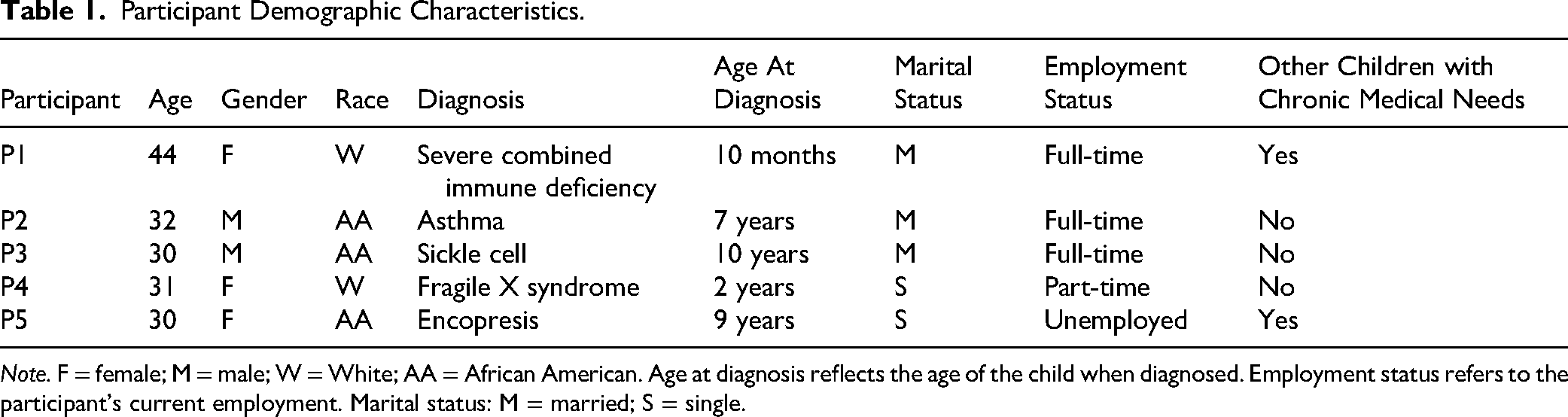
Note. F = female; M = male; W = White; AA = African American. Age at diagnosis reflects the age of the child when diagnosed. Employment status refers to the participant's current employment. Marital status: M = married; S = single.
Findings
The purpose of this study was to explore the lived experiences of parents raising children with chronic medical needs. Through an iterative hermeneutic phenomenological analysis, five overarching themes were identified: (a) navigating multifaceted challenges, (b) sources of support, (c) emotional complexity, (d) meaning-making and advice for other parents, and (e) resilience and post-traumatic growth. These themes reflect both shared patterns across participants and nuanced individual experiences that illuminate the complexity of parenting within the context of chronic medical needs.
Theme 1: Navigating Multifaceted Challenges
Participants consistently described parenting a child with chronic medical needs as a process marked by ongoing, interconnected challenges that extended across medical, relational, and systemic domains. Although each participant's experience was unique, several shared subthemes emerged, including navigating the medical system, impact on the family system, discipline complexities, the desire for understanding from others, and logistical burdens.
Navigating the Medical System
A central challenge described by participants involved difficulties navigating the medical system, particularly in feeling heard, believed, and supported by healthcare providers. Participant 1 described a distressing experience in which her concerns were dismissed and misinterpreted, stating, “I was accused of Munchausen Disorder, that I was causing my kid to be ill. My husband was accused of abusing my child since his diagnosis caused a lot of bruising.” She reflected that these experiences continue to evoke sadness and anger.
Similarly, Participant 5 described frustration with the delayed recognition of her child's needs, recalling, “He's just a boy, he's normal. But he wasn’t eating properly, and he was struggling… I knew something more was going on!” She further shared a particularly challenging interaction: My son's doctor one time suggested my son wear diapers at school due to his accidents without taking into account how this might increase the bullying my son was already going through. Ultimately, it just felt often like we were pulling teeth to get him the care he needed!
Collectively, these narratives highlight the emotional and relational strain embedded in navigating medical systems, where parents often occupy dual roles as both caregiver and advocate.
Impact on the Family System
Participants also described how chronic medical needs reverberate across the entire family system, shaping relationships among siblings, partners, and extended family members. Participant 1 reflected on the unintended emotional impact on her other child, stating, “my son who was ill, his brother started having flashbacks his brother was going to die.” She elaborated:
“He hid things well… we thought he was too young to really understand what was going on… but he picked up on it.”
Other participants described the strain of balancing competing needs within the family. Participant 5 shared, “I have two kids and must parent them very differently… I feel like I am being pulled!” Similarly, Participant 3 noted relational tension within his marriage, explaining, “Relationships can be a challenge… but one good thing is we always find a way to come to a common ground… our child comes first.” These accounts illustrate how chronic illness reshapes family roles, expectations, and emotional dynamics, often requiring ongoing negotiation and adaptation.
Complexities of Discipline
Participants described discipline as a particularly nuanced and challenging aspect of parenting within this context. Participant 4 shared: “My kids has meltdowns. He fights. He hits himself… it's a lot different than just putting them in time-out.” She further noted the difficulty of navigating external judgments, stating, “My husband's family thinks I need to be stricter… they don’t understand how difficult it is.”
Participant 1 similarly reflected on the tension between empathy and structure: “Discipline is hard. If you snap at me because you aren’t feeling well, I have a hard time punishing that.” At the same time, she emphasized the importance of maintaining boundaries, noting that “one doctor did share… the importance of continuing to discipline our child… and it was helpful advice.” These experiences highlight the complexity of parenting decisions within the context of chronic illness, where typical disciplinary approaches may require adaptation.
Desire for Understanding and Social Validation
A pervasive theme across participants was a desire for greater understanding from others, including peers, educators, and other parents. Participant 4 described her child's difficulty forming peer relationships: “he is trying to interact… they kind of just pushed him away.” Participant 5 similarly connected this lack of understanding to bullying experiences, stating, “we are changing schools… other kids just don’t understand what my son is going through.”
Participants also described feeling misunderstood by other adults. Participant 4 reflected:
“It affects the relationship between me and other grown-ups… they may think I’m strong, and I’m strong, but not that strong.” These narratives underscore the relational isolation that can accompany parenting a child with chronic medical needs.
Logistical and Role Overload Challenges
Participants described significant logistical challenges, including managing employment, finances, healthcare coordination, and educational systems. Participant 5 shared, “it is hard to stay employed, I’ve lost a lot of jobs because I have to take care of my son,” while Participant 3 noted, “Work has been a big challenge… I have had to take time off.”
Educational systems also presented ongoing barriers. Participant 5 explained: “It's hard… schools say that they have the support, but they really don’t have the support for that child… it just seems like it's always something.” Participants frequently described a sense of role overload. Participant 1 captured this experience by stating, “I felt like I couldn’t be nurse, mom, teacher—all the things.”
Theme 2: Sources of Support and Connection
Participants described support as essential to navigating the ongoing demands of parenting a child with chronic medical needs. Although the types of support varied, a consistent thread across narratives was the importance of connection, whether through counseling, family and community relationships, spirituality, or access to tangible resources. At the same time, participants highlighted barriers to accessing support, underscoring the complexity of sustaining these systems.
Counseling as a Space for Processing and Relief
Several participants identified counseling as a meaningful outlet for emotional processing and coping. Participant 2 described the value of having a space to speak openly, stating, “I have a personal counselor I talk to whenever I feel overwhelmed… I speak my mind freely… and my counselor can offer solutions.” Similarly, Participant 1 emphasized the importance of therapeutic fit and modality, noting, “having different types of counseling to find what worked best for us was like the very top most helpful thing.” She reflected on her experiences with multiple approaches, sharing, “I did like cognitive behavioral therapy… but I did also EMDR, which I found super helpful… for medical PTSD.”
At the same time, access to counseling was not without barriers. Participant 4 described the logistical challenges of engaging in therapy, stating, “finding a counselor for myself has been challenging. Like, when do I do it, I can’t leave my son easily.” This tension reflects the broader paradox of needing support while simultaneously facing barriers to accessing it.
Relational and Community Support
Participants consistently emphasized the role of relationships in sustaining them through difficult moments. For some, support came from friendships and community members. Participant 3 described a moment of crisis in which community intervention was lifesaving:
“It was a community person that noticed… and rushed to get an inhaler… that was how my son was saved… I’m here today because of the support I’ve gotten.”
Others described the importance of family support. Participant 5 shared, “My mom is my son's aide which makes a big difference,” while Participant 3 noted, “I wouldn’t know what I would have done if my family didn’t offer the kind of support they have.”
These accounts reflect the deeply relational nature of caregiving, where support systems serve not only practical functions but also emotional and existential ones.
Accessing Formal Resources
Participants also identified formal supports and resources as critical components of their experience. For example, Participant 1 described the impact of the Dragonfly Foundation, noting its role in addressing “isolation, post-traumatic stress, the anxiety of recurrence, and the emotional, physical and financial toll on the family.” Participant 5 similarly emphasized the importance of resource access, stating, “resources are out there, and I wish more parents knew about them,” referencing organizations such as the Ohio Board of Developmental Disabilities and Ohio Rise. These narratives highlight both the availability of resources and the ongoing need for increased awareness and accessibility.
Spirituality as Meaning-Making and Coping
Spirituality emerged as a significant source of meaning, hope, and resilience for several participants. Participant 3 described engaging with his religious community as a source of strength, stating, “I do know this thing will come to pass due to my faith.” Participant 2 echoed this sentiment, sharing, “I take it to God… I pray, I sing… that's the only thing that really encourages me.”
Participant 5 articulated a nuanced understanding of spirituality, explaining, “I don’t feel like if I pray all my problems are just going to go away… but spirituality has helped me realize that we all go through life with difficulties.” Collectively, these experiences suggest that spirituality serves not only as a coping mechanism but also as a framework through which participants make sense of their circumstances.
Theme 3: Emotional Complexity and Ambiguity
Participants described their emotional experiences as multifaceted, fluid, and often contradictory. Rather than a singular emotional response, parenting a child with chronic medical needs was characterized by the coexistence of sadness, anger, uncertainty, and, at times, joy. This emotional complexity reflects the ongoing and evolving nature of caregiving within this context.
Sadness and Grief
Sadness emerged as a common emotional experience, often tied to uncertainty, loss, and witnessing a child's suffering. Participant 2 reflected, “I felt a little bit sad… I wondered why my child,” while Participant 3 shared, “I am sad I can’t take it away from him.” Participant 4 described the moment of diagnosis as “probably the most challenging and sad day of my life.”
For some participants, sadness evolved over time. Participant 1 noted, “it's better now… but I still can get kind of sucked into the negative feelings,” suggesting that grief may persist in cyclical or reactivated ways. Participant 5 offered a nuanced perspective, describing how sadness shifted in meaning over time: “I feel like I can talk about it now and it helps with the sadness… I’m proactive… but the sadness I get now is when he's getting bullied… I hurt for him.”
These narratives reflect forms of ongoing and ambiguous grief that are not tied to a single event but instead embedded within daily experiences.
Holding Multiple Emotions Simultaneously
Participants frequently described experiencing multiple emotions at once, highlighting the paradoxical nature of their roles. Participant 4 captured this complexity, stating, “It's been the happiest and the saddest thing I’ve done in my life.” This coexistence of joy and pain reflects the relational depth of caregiving, where moments of connection and growth exist alongside ongoing challenges.
Anger and Frustration
Anger also emerged as a salient emotional response, often directed toward systems, social interactions, or experiences of misunderstanding. Participant 4 shared, “I get angry when other parents… don’t understand,” while Participant 1 expressed lingering frustration with medical professionals, stating, “I still get upset thinking about what doctors put us through.”
These expressions of anger reflect not only emotional responses but also broader experiences of marginalization and invalidation.
Theme 4: Resilience and Post-Traumatic Growth
Despite the challenges described, participants also identified ways in which their experiences fostered personal growth, strengthened relationships, and reshaped their perspectives. These narratives reflect elements of resilience and post-traumatic growth, illustrating that parenting within this context is not solely defined by hardship. Participant 1 described a shift in perspective, stating: “I think also just appreciating things more… like the sunshine, the kids smiling… just letting it soak in.” Similarly, Participant 2 reflected on personal growth, noting: “It is making me a better person… I’ve gotten to have a very, very deep relationship with my child… it's made me even closer to my child.” These experiences suggest that caregiving can deepen relational bonds and foster increased intentionality in parenting.
Participant 3 also highlighted growth in his child, stating, “it is amazing to see my son… has knowledge beyond what his age bracket normally would have,” suggesting that adversity may contribute to developmental and relational strengths. Importantly, participants did not frame resilience as the absence of struggle, but rather as something that coexists with ongoing challenges. Their narratives reflect an evolving process of meaning-making, adaptation, and connection that continues over time.
Discussion
The findings of this study both align with and extend existing literature on the experiences of parents raising children with chronic medical needs. Consistent with prior research, participants described elevated stress, emotional burden, and the ongoing demands of caregiving (Cousino & Hazen, 2013; Singer, 2006). However, the present study offers a more nuanced understanding of these experiences by illuminating the simultaneous presence of multiple, and at times conflicting, emotional states, including grief, joy, frustration, and resilience.
This emotional complexity underscores the importance of moving beyond deficit-oriented frameworks that focus solely on burden and pathology, toward more holistic and relational understandings of caregiving. Participants’ narratives reflected not only distress but also meaning-making, connection, and growth, highlighting the dynamic and evolving nature of parenting within the context of chronic medical needs. From a family systems perspective, these findings reinforce that the impact of chronic illness is not confined to the individual child but is embedded within broader relational, social, and systemic contexts.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, consistent with qualitative research, the findings are contextually bound and reflect the specific experiences of participants who elected to share their stories. As such, the findings are not intended to be generalized but rather to offer in-depth insight into the phenomenon under investigation.
Second, participants were recruited through professional networks and community-based platforms, which may have shaped the types of experiences represented in the data. Individuals who chose to participate may have been more willing or prepared to reflect on and articulate their experiences, potentially influencing the nature of the narratives shared.
Third, the sample primarily reflected parents who were not in the immediate aftermath of diagnosis, which may limit the extent to which these findings capture the experiences of families in earlier stages of adjustment. Future research may benefit from exploring how experiences evolve across different phases of caregiving.
Finally, consistent with hermeneutic phenomenology, the researcher's positionality and prior experiences informed the interpretive process. Although reflexive journaling and the use of an external auditor were employed to enhance transparency and trustworthiness, interpretation remains co-constructed and shaped by the researcher's lens. This reflexive engagement is viewed as a strength of the methodology while also representing an inherent limitation.
Implications for Family Counseling
The findings of this study have important implications for family counseling practice. Counselors are uniquely positioned to support parents navigating the complex emotional landscape associated with raising a child with chronic medical needs, including experiences of ambiguous loss, chronic stress, and caregiver burnout. Interventions that emphasize meaning-making, emotional validation, and flexibility in coping may be particularly beneficial.
Importantly, the findings highlight the need for counselors to adopt a systemic perspective. Chronic medical conditions impact not only the identified child but also sibling relationships, marital dynamics, and broader family functioning. As such, family-based interventions that attend to relational patterns, role shifts, and communication processes may enhance overall family resilience.
Additionally, counselors can play a critical advocacy role by supporting families as they navigate medical and educational systems. This may include assisting parents in articulating their needs, addressing systemic barriers, and fostering collaboration across systems of care. Training programs should prepare counselors to engage with these complex, intersecting systems while maintaining a culturally responsive and family-centered approach.
Future Directions
Future research should continue to expand qualitative inquiry in this area by exploring diverse family structures, cultural contexts, and caregiving experiences. Longitudinal research may provide valuable insight into how parental meaning-making and coping evolve over time, particularly across developmental transitions and stages of illness. Additionally, there is a need for intervention-based research that examines counseling approaches specifically tailored to families of children with chronic medical needs, with attention to both individual and systemic outcomes.
Conclusion
This phenomenological study contributes to the counseling literature by centering the lived experiences of parents raising children with chronic medical needs and illuminating the complexity inherent in these experiences. Participants’ narratives revealed a dynamic interplay of challenge, connection, and growth, offering a more holistic understanding of caregiving beyond deficit-based perspectives. As one participant reflected, “It's been the happiest and the saddest thing I’ve done in my life… it has brought happiness to me.” By foregrounding the voices of parents, this study provides meaningful insight into the relational and emotional dimensions of caregiving and offers guidance for more responsive, systemic, and compassionate family counseling practice.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.