
Abstract
The purpose of this quantitative study is to examine the influence of family resilience on the impact of adverse childhood experiences (ACEs) on child health and academic outcomes. The researchers examine nine models corresponding to the outcome's variables. Overall, our study's results show that family resilience is an essential factor in achieving better physical and mental health outcomes for children, and its impact is generally consistent across levels of ACEs. The influence on academic outcomes is less robust; however, family resilience is an essential factor in producing more fully engaged students regardless of their ACEs. Results and professional implications discussed.
Highlights
*This study examines the influence of family resilience on adverse childhood experiences impact on health and academics.
*Family resilience is an essential factor in better physical and mental health outcomes for children.
*Family resilience is an essential factor in producing more engaged students regardless of adverse childhood experiences.
Examining the Influence of Family Resilience on Adverse Childhood Experiences
There is a significant body of literature exploring adverse childhood experiences (ACEs) and the relationship of how these experiences affect the lives of children and their growth and development well into adulthood. Mental health, risk-taking behaviors, substance and alcohol abuse, and decreased life expectancy are some of the outcomes that have been shown to impact those who have experienced ACEs (Soleimanpour et al., 2017). It is important to understand what factors might mitigate the impact of ACEs in children and adolescents. Research has shown that ACEs affect children across demographics, including race, gender, ethnicity, and socioeconomic background (Bright et al., 2015). Increased exposure to ACEs can have a detrimental impact on development, learning, and behavioral outcomes during childhood and adolescence. The purpose of this investigation is to better understand the influence of family resilience on the impact of ACEs on child health and school outcomes.
Importance of Family Relationships
Family relationships are foundational to child development for several key reasons: emotional security, social and moral learning, cognitive and language development, modeling behaviors, and resilience in the face of adversity. The experiences of the individual members, and also the unit as a whole, shape and move the family into specific patterns and dynamics that can have transgenerational consequences. Naturally, both positive and negative outcomes can be expected from family membership. A child's first understanding of the world is through the family. An adolescent's perspective on romantic relationships is based on what was modeled in the family. Expectations of tasks and responsibilities within the home stem from what was required in one's own family of origin. Given the importance of the family unit, it is essential to understand how to create and bolster family relationships.
Healthy family functioning depends on a supportive infrastructure of respectful relationships. This requires emotional safety and a sense of belonging among members, as well as consistent and clear communication (Daines et al., 2021). Families are best understood within the context of their milieu, which can pose numerous hardships, including financial adversity, crime, and limited resources. As families are better equipped to confront challenges and adapt to changing environments, they strengthen their familial relationships (Klever, 2015). The parent–child dynamic is a vital connection within the family. This attachment, in particular, lays the foundation for lifelong relationships outside the family. The degree to which the parent and child attach can create protection or impediments within the child's development. Research shows parental engagement can lessen the cognitive and emotional impact of ACEs on children (Bethell et al., 2016; Okwori, 2022). In addition, Daines et al. (2020) found that positive childhood experiences, such as encouraging mentors and family dependability, were related to healthier families, regardless of reported ACEs. These studies demonstrate how positive family relationships can offset some of the adverse events that can happen to individual members. Just as individuals can be shielded to some degree by their connection to family, the family itself can adapt and overcome.
Family Resilience
Often, resilience is examined based on an individual's experiences and how that person can tolerate what for others may be unbearable. However, understanding family resilience, particularly its relationship to ACEs, is paramount for developing strategies for healthy relationships. Family resilience is the ability of family members to use healthy coping mechanisms under challenging conditions, empowering them to “flourish with warmth, support, and cohesion” (Black & Lobo, 2008, p. 33). It refers to the collective strengths, processes, and resources that families use to adapt, recover, and even grow when faced with difficulties such as illness, loss, trauma, financial hardship, or major life changes. Resilient families can access and use resources within their community and culture, as well as their own biopsychosocial assets (Okwori, 2022). They apply effective communication strategies and work as a unit to achieve goals. Westphaln et al. (2022) found that children with ACEs who had “a supportive neighborhood, parents that experienced emotional support in raising children, and resilient families’’ were able to “flourish” (p. 61). Using the lens of Resilience Theory, families have promotive factors (assets and resources) that encourage growth (Zimmerman, 2013). Resilience Theory highlights what enables people to thrive—not just what makes them vulnerable. It looks at assets (such as skills, competencies, and self-efficacy) and resources (such as supportive relationships, community programs, and opportunities). Family members’ internal assets, such as one's own sense of self-worth, as well as external resources, such as community programs that support parents and children, contribute to family resilience (Zimmerman, 2013). Resilience Theory reframes adversity by focusing on how individuals, families, and communities can draw on strengths and resources to overcome challenges and achieve positive outcomes. It encourages interventions and policies that build protective factors and empower families to adapt and thrive, even in the face of hardship. Family resilience is not about avoiding difficulties—it is about how families come together, adapt, and grow stronger in response to them. It is a dynamic process that can be nurtured and strengthened over time.
Family Resilience and Education
Family resilience and education are closely linked, as a family's ability to cope with adversity directly impacts children's educational experiences and outcomes. The family–school relationship is collaborative, with the school recognizing the need to communicate and partner with the family unit and its resources. This allows educators to move beyond an individual assessment or intervention and see how a family's strengths, resources, and resilience can be tapped to support a student with academic or behavioral issues. Resilient families provide emotional support, encouragement, and stability when children face academic difficulties or setbacks. This support helps students cope with challenges such as poor grades, bullying, or transitions between schools. This type of family resilience perspective views each communication or interaction between school and home as an opportunity not only to improve a student's educational outcomes but also to help the family build additional skills and capacity to overcome challenges that may impede a child's ability to learn and be academically successful. According to Amatea et al. (2006), a key premise of this approach is that, while family resilience mediates how students are prepared to engage at school, family skills/processes can be strengthened by how a school or educator responds to and communicates with the family. Therefore, each family–school interaction guided by a family resilience perspective moves beyond merely responding to a child's needs and can be seen as a preventive measure.
Adverse Childhood Experiences
Childhood trauma refers to distressing, frightening, or harmful experiences that occur during childhood (typically before age 18) and overwhelm a child's ability to cope. These events can have lasting negative effects on a child's emotional, psychological, social, and physical well-being. Childhood trauma is any overwhelming or harmful experience in childhood that disrupts a child's sense of safety and well-being. Recognizing and addressing childhood trauma is crucial for healthy development and long-term well-being. Perry (2007) defines trauma as any experience that overwhelms the nervous system. Experiences that threaten the physical or emotional safety of children and adolescents, their family and community members, are considered traumatic events (The National Child Traumatic Stress Network, 2022). In the United States, an estimated 64–80% of children experience one traumatic event before the age of 17, with 1 in 6 experiencing four or more (Centers for Disease Control, 2022; Preventing Adverse Childhood Experiences, 2022). Early trauma can affect brain development and stress response systems, influencing how children manage emotions, form relationships, and learn. Without support, trauma can have lifelong consequences, but with care and intervention, children can recover and build resilience.
ACEs were identified by Felitti et al. (1998) as a tool to identify early childhood trauma. The original ACE Study (Adverse Childhood Experiences Study) was a large-scale research project conducted by the Centers for Disease Control (CDC) and Kaiser Permanente in the late 1990s. Over 17,000 adult participants were surveyed about their childhood experiences and current health status. The study sought to understand the relationship between ACEs and later-life health outcomes. ACE scores are measured through the ACE questionnaire, which asks about specific types of abuse, neglect, and household dysfunction experienced before age 18. Each “yes” answer in one of the 10 categories counts as 1 point, yielding an ACE score ranging from 0 to 10. The higher the score, the greater the exposure to childhood adversity. Collectively, the ACE score is a tally of categories of abuse, neglect, and household dysfunction experienced in childhood, and the ACE Study demonstrated a clear link between these experiences and health outcomes later in life. In fact, the CDC (2022) estimates that 1.9 million cases of heart disease and 21 million cases of depression are linked to ACE scores and that families and communities spend approximately 56 billion dollars in healthcare due to ACE-related health issues.
Experiencing traumatic events affects overall well-being and success. ACE scores are linked to developmental delays, poor mental and physical health conditions, and high-risk behaviors (Felitti et al., 1998; Preventing Adverse Childhood Experiences, 2022). ACEs are also associated with increased risks of financial strain, homelessness, and job instability (CDC, 2022). Higher ACE scores are associated with an increased risk of poor outcomes, meaning the more trauma children experience, the poorer outcomes they face. Because of the systemic nature of trauma, children from marginalized communities and females have a higher risk of experiencing four or more ACEs (CDC, 2022). Children and adolescents from low-income communities, violent communities, racially segregated communities, or communities experiencing racism are more susceptible to higher ACE scores. Though the ACE study did not consider systemic oppression as a form of trauma or maltreatment, it is recognized that marginalized communities face greater instances of violence, higher rates of poverty, and less access to resources. These factors, known as social determinants of health, are considered risk factors (CDC, 2022). It should be noted though, that trauma does not affect all children in the same way, while many children experience negative effects, not all are impacted to the same degree, and some show remarkable resilience.
Children and adolescents are a vulnerable population due to their critical neurodevelopmental stages and reliance on caregivers for physical and emotional safety (Perry, 2007; Spinazzola et al., 2018). Much of the amygdala develops between the ages of 0 and 3. This development is susceptible to parental cues, stress, and the environment. Zero to three is critical for the development of healthy attachment, which serves as the foundation of a healthy prefrontal cortex. Therefore, development is dependent on parental attunement, emotional regulation, and a safe environment. Because the brain continues to develop through early adulthood, children and adolescents depend on their caregivers for healthy development. Trauma disrupts development; however, secure attachment, early intervention, and community engagement act as protective factors and support development (CDC, 2022; Perry, 2007; Schore, 2001; Siegel, 2012).
Attachment and Protective Factors
Attachment is a crucial component of development. (Perry, 2006; Schore, 2001; Siegel, 2012). Attachment or attachment styles refer to the internal working models developed in infancy (Bowlby, 1982), which include four styles: secure, anxious, avoidant, and disorganized (Ainsworth et al., 1971; Ainsworth et al., 1978a, 1978b; Main & Solomon, 1990). Attachment is developed through attunement, emotional regulation, and security (Schore, 2001). The more attuned, emotionally regulated, and physically secure the parent/environment is, the more secure the attachment (Perry, 2006; Schore, 2001; Siegel, 2012).
Secure attachment acts as a buffer against toxic stress and helps foster resilience (Sciaraffa et al., 2018). Resiliency is understood as the ability to cope with/adapt positively to adverse experiences (Luthar, 2006; Pizzolongo & Hunter, 2011). Securely attached, resilient individuals face fewer developmental delays, increased impulse control, and better emotional regulation (Felitti et al., 1998; Perry, 2006; Schore, 2001 & 2002; Sciaraffa et al., 2018). Secure attachment requires sensitive caregivers (Sciaraffa et al., 2018). Caregivers who are responsive to the child's needs and able to remain regulated through adverse events reduce the neurobiological impacts of stress (Perry, 2008; Schore, 2011; Siegel, 2012). Intergenerational trauma can create barriers to building secure attachment. Parents who experience ACEs are at an increased risk of mental illness, substance misuse, domestic violence, and childbirth difficulties (CDC, 2022). For these parents focusing on awareness, early intervention and treatment are key to providing support and opportunity for better outcomes.
Early intervention can enable the repair of insecure attachment, the initiation of evidence-based treatment, and parental support (Sciaraffa et al., 2018). There are several opportunities for early intervention: yearly wellness and vaccination appointments, childcare facilities, and pre-kindergarten classrooms. Teaching pediatricians, childcare employees, and early childhood educators to recognize the early signs of trauma creates opportunities for early intervention. Some research suggests that training early childhood educators and caregivers on attachment-focused ways to engage with children is also a protective factor (Mortensen & Barnett, 2016; Sciaraffa et al., 2018). However, if access to these professionals is limited, fostering resiliency can become more difficult.
Community is an essential protective factor and social determinant of health (CDC, 2022). The community's protectiveness is determined by many factors: access to healthcare, financial stability, living in low-violence communities, access to high-quality public education, and cost-effective childcare. Communities that provide parent education, economic opportunity, and community engagement promote healthy development. To actively reduce the detrimental impacts of ACEs, communities must be well-resourced, connected, and economically stable.
Methods
The study examines the influence of family resilience on the impact of ACEs on child health and school outcomes. The researchers examine nine models corresponding to the outcome's variables. The data come from the Child and Adolescent Health Measurement Initiative's (CAHMI) National Survey of Children's Health (NSCH) and include surveys from 2016 to 2020 (Child and Adolescent Health Measurement Initiative, 2020). The dataset is available at childhealthdata.org. Given that each of these outcomes is categorical, we run ordered logits for those outcomes with more than two categories (overall health, number of health conditions, impact on daily activities, and days absent from school) and logits for the binary variables (ADD/ADHD diagnosis, mental health treatment or counseling, repeated grade, participation in after school activities, and school engagement). Each model includes the same set of control variables (Appendix 1) along with family resiliency, ACEs, and the interaction between family resiliency and ACEs. The models are weighted according to the procedure outlined in the NSCH Guide to Multi-Year Analysis (2021). The analysis focuses on the interactive effect of family resiliency on ACEs.
Research Questions
To what extent does family resilience influence the impact of ACEs on physical health outcomes?
To what extent does family resilience influence the impact of ACEs on mental health outcomes?
To what extent does family resilience influence the impact of ACEs on school outcomes?
Results
Participants
The sample for this analysis comes from the CAHMI's NSCH and includes surveys from 2016–2020 (Child and Adolescent Health Measurement Initiative, 2020). The dataset is available at childhealthdata.org. The NSCH was a cross-sectional national survey of parents or guardians with at least one child living in the household between the ages of 0 and 17. This study focused on children of school age (6–17 years old; N = 125,005).
Measures
The primary independent variables of interest in this study are family resiliency and ACEs and the interaction between these variables as the research questions examine the moderating influence of family resilience on ACEs on physical health, mental health, and school outcomes. Additionally, the models include a common set of control variables that include the child's gender, race, whether they were born in the United States, the region of the country in which they live, and the year of the survey. Also, in the controls are two family measures: the poverty level of the family and the highest education among adults in the family. Appendix 1 shows the descriptive statistics for these variables.
Family Resiliency
The family resiliency measure was provided in the NSCH data and is a composite measure based on responses to four survey items. These four items are as follows:
When your family faces problems, how often are you likely to do each of the following:
- Talk about what to do - Work together to solve our problems - Know we have strengths to draw on - Stay hopeful even in difficult times.
The response options for each of the questions were none of the time, some of the time, most of the time, or all of the time. In the analysis, we have collapsed the measure into two categories: resilient family (answered most of the time or all of the time to each of the four individual questions) or not resilient family since over 80% of the respondents come from resilient families as well as for ease of interpretation and presentation of the results.
Adverse Childhood Experiences
The NSCH measures nine ACEs. In this analysis, ACEs is a composite measure included in the NSCH of all ACE items categorized as “No adverse childhood experiences”; “One adverse childhood experience”; and “Two or more adverse childhood experiences”. The composite measured is used rather than a count of ACEs due to the distribution of the data with the number of respondents scoring between 3 and 9 ACEs being less than 5% of the sample and with those scoring more than 5 ACEs being less than 1% of the sample.
Dependent Variables: Physical Health, Mental Health, and School Outcomes
This study looks at three outcomes related to the growth and development of children. One in the area of physical health, one in mental health, and one in education. For physical health, the study looks at overall health status. The survey respondent (i.e., parent or guardian) was asked, “In general, how would you describe this child's health?” The NSCH codes this into three categories: Excellent or very good (90.74% of the sample), Good (7.83% of the sample), and Fair/poor (1.43% of the sample). Given the distribution of the data, we collapse the variable into a dichotomous variable of Excellent or very good health or Good/Fair/Poor health.
For mental health, the NSCH asks the following question, “During the past 12 months, has this child received any treatment or counseling from a mental health professional?” For the analysis, we code the variable as “No” (83.19% of the sample) for those responded that the child did not need to see a mental health professional and “Yes” (16.81% of the sample) for those that said either the child had seen a mental health professional or needed to see one.
In terms of school outcomes, the NSCH includes several potential measures. For this study, we include a measure of school engagement. The NSCH measure stems from the answers to two questions related to caring about school and doing homework. Children who were reported as caring about school and doing their homework were coded as “always engaged in school” by the NSCH and we refer to this as fully engaged. We code school engagement as fully engaged (53.72% of the sample) or not fully engaged (46.28% of the sample).
Data Analyses
Given that each of these outcomes is categorical and binary, we run logit models that include sample weights. The models are weighted according to the procedure outlined in the NSCH Guide to Multi-Year Analysis (2021) which allows for combined multi-year analyses. Each model includes the same set of control variables (Appendix 1) along with family resiliency, ACEs, and the interaction between family resiliency and ACEs. Given that logit coefficients are not straightforward to interpret, we present and interpret predicted probabilities for the likelihood of an outcome occurring across the ACEs categories and by family resiliency and then focus on the interactive effect of family resiliency across the range of ACEs.
Table 1 shows the results from the physical health, mental health, and school models. In each area, having more ACEs leads to less healthy outcomes and less engagement in school while being from a resilient family leads to healthier outcomes and more school engagement. The interaction between ACEs and family resilience is not statistically significant in the physical health and school model, but is statistically significant in the mental health model. While the interaction variable is only statistically significant in one of the three of the models, this does not provide information on the outcome of interest: The influence of family resiliency across the number of ACEs categories (Sciaraffa et al., 2018).
Model Results.
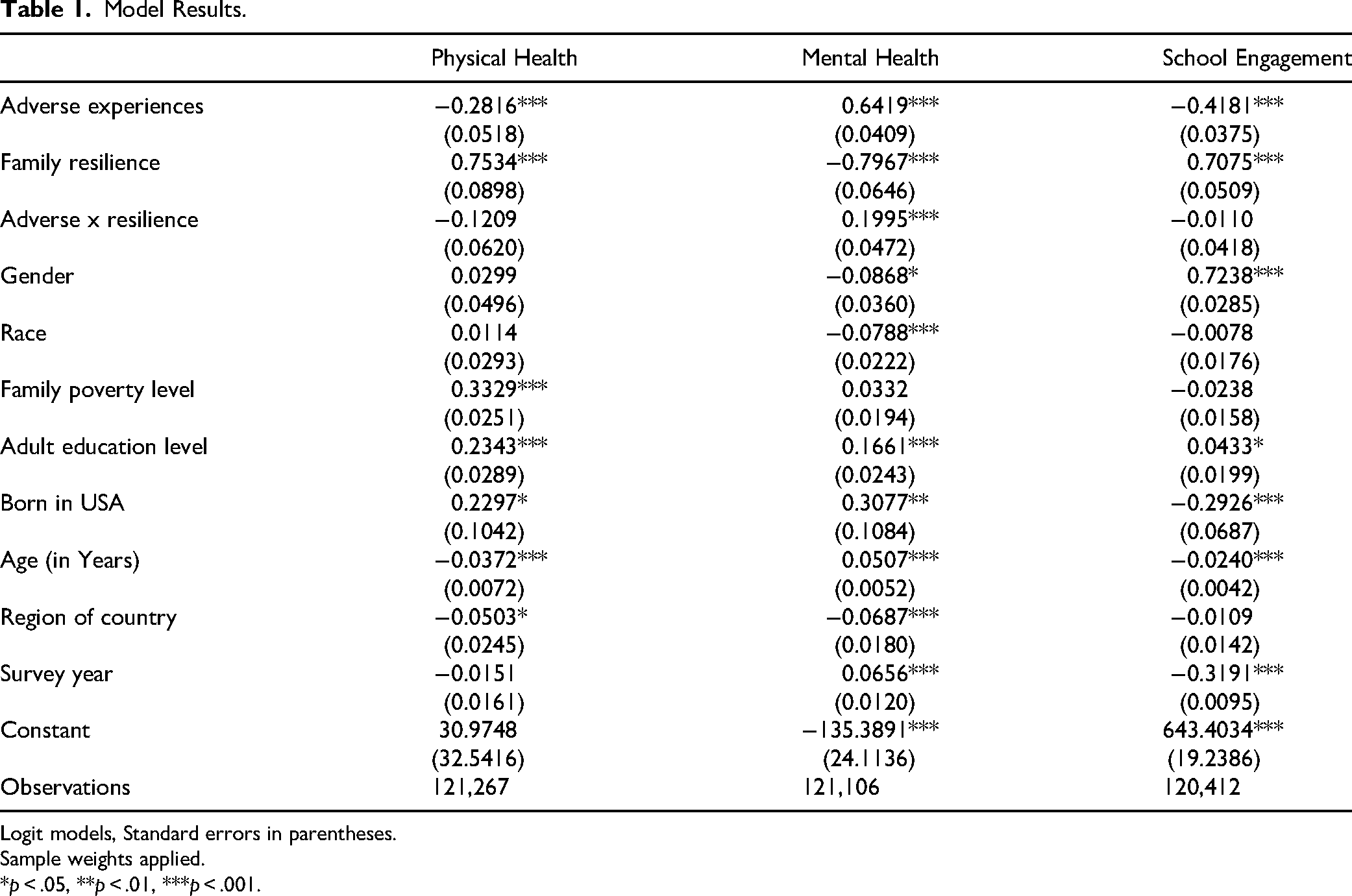
Logit models, Standard errors in parentheses.
Sample weights applied.
*p < .05, **p < .01, ***p < .001.
To understand the substantive effects of these results, Table 2 shows the predicted probability for the main effects of ACEs and family resilience, all else being equal, for each outcome. For physical health, having 0 ACEs predicts a 92% likelihood of being in excellent or very good health, having 1 ACE decreases this to an 88% predicted likelihood, and having 2 or more ACEs lowers this 84%. Individuals from a resilient family have a 90% predicted likelihood of being in excellent or very good health while being from a non-resilient family decreases this chance by 7% to 83%.
Predicted Outcomes, Main Effects.
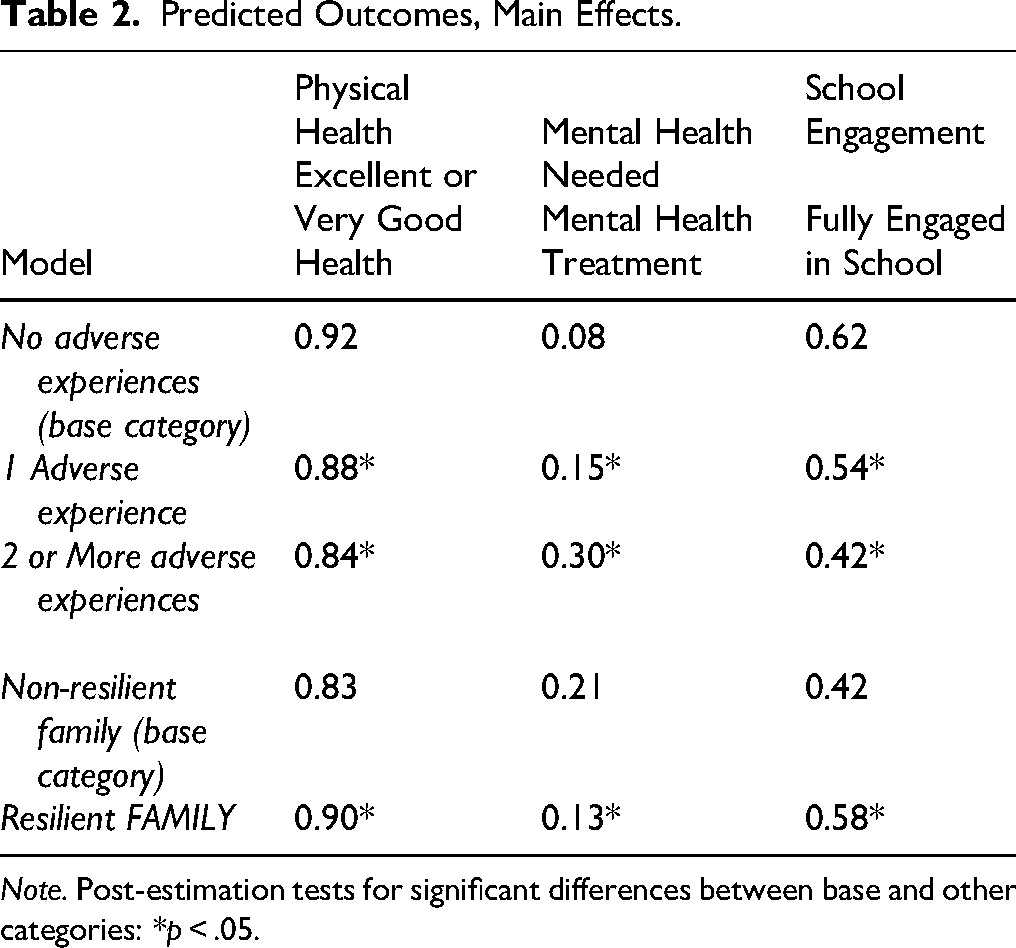
Note. Post-estimation tests for significant differences between base and other categories: *p < .05.
For the likelihood of having received any treatment or counseling from a mental health professional in the previous year, those with 0 ACEs have a predicted likelihood of 8%, 1 ACE increases this to 15%, and having 2 or more ACEs leads to a substantial increase to 30%. Those children from a resilient family have a 13% predicted likelihood of having sought mental health treatment in the previous year compared to 21% for those not from a resilient family.
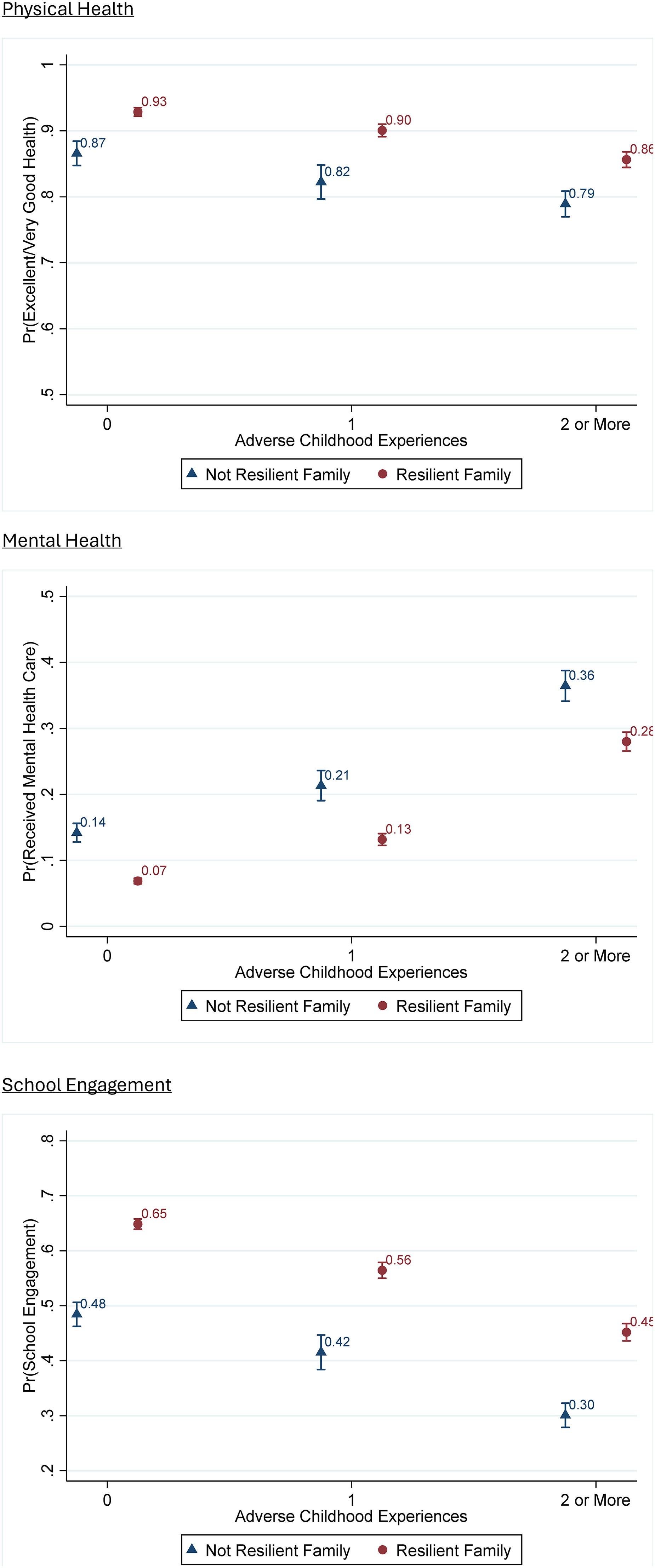
Finally, in terms of school engagement, having 0 ACEs predicts a 62% of being an engaged student compared to 54% for those with 1 ACE and only 42% for those with 2 or more ACEs. Family resilience has a 16% increase in the likelihood of being an engaged student (58% for resilient families and 42% for non-resilient families). The real outcome of interest is the moderating influence of family resilience on ACEs across these outcomes. Figure 1 and Table 3 show the results. Coming from a resilient family leads to significantly better outcomes across each category of ACEs. In terms of physical health, it leads to between a 6 and 8% increase in the likelihood of being in excellent or very good health and decreases the likelihood seeking mental health treatment by 7–8%. Finally, it increases the likelihood of school engagement by 14–17%. Across each of these outcomes, the difference in family resilience is statistically significant within each level of adverse experiences.
Predicted outcomes: interaction.
Predicted Outcomes, Interaction.
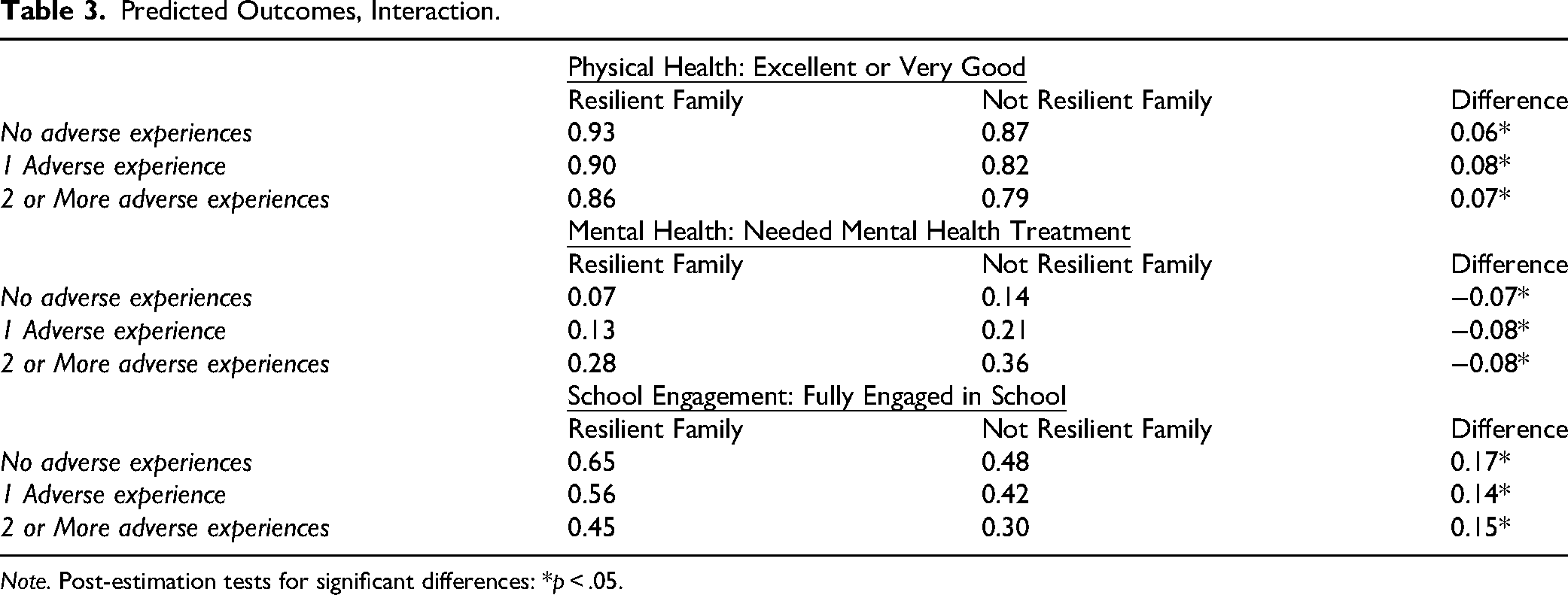
Note. Post-estimation tests for significant differences: *p < .05.
Most importantly, this influence is consistent across the levels of ACEs. This suggests family resilience does not negate the negative effects of having more ACEs, nor does having more ACEs limit the positive effects of family resilience. This consistency is important but it reminds us that resilience is a buffer but not a cure. Family resilience is characterized by supportive relationships, adaptability, and healthy communication and can buffer or mitigate some of these adverse effects, but it cannot erase them entirely. The biological and psychological impacts of trauma can persist even in resilient families.
From a statistical standpoint, there are very minor differences in the influence of family resilience when comparing across the level of ACEs. Substantively, however, this consistent effect is important as family resilience leads to better health and school outcomes even for those dealing with more ACEs and this positive influence is consistent across a number of ACEs. The role of family resilience does not fall apart if someone has experienced more adverse experiences.
Discussion
The first research question examines the extent to which family resilience influences the impact of ACEs on physical health outcomes. Our findings suggest that having more ACEs is associated with worse physical health outcomes, whereas growing up in a resilient family is associated with better physical health outcomes across all three models. As previously mentioned, ACE scores correlate with developmental delays, poor mental and physical health conditions, and high-risk behaviors (Felitti et al., 1998; Preventing Adverse Childhood Experiences, 2022). Higher ACE scores are associated with an increased risk of poor outcomes, meaning the more trauma children experience, the poorer outcomes they face. The implications of ACEs for physical health are clear, so a better understanding of mitigating factors, such as having a resilient family, could be highly impactful as we work with children/adolescents and their families. Data from this study reveal that those from resilient families are less likely for their health conditions to affect their daily activities compared to those from non-resilient families. For physical health, having 0 ACEs predicts a 92% likelihood of being in excellent or very good health, having 1 ACE decreases this to an 88% predicted likelihood, and having 2 or more ACEs lowers this 84%. Individuals from a resilient family have a 90% predicted likelihood of being in excellent or very good health while being from a non-resilient family decreases this chance by 7% to 83%. These findings suggest that children and adolescents from resilient families recognize the positive daily impact of resilience and how it helps lessen the impact of their medical conditions.
The second research question explored the extent to which family resilience influences the impact of ACEs on mental health outcomes. Based upon our findings, children from resilient families are less likely to have mental health concerns compared to those from non-resilient families, and this influence of family resilience is consistent across ACEs. The CDC (2022) estimates that 21 million cases of depression are linked to ACE scores and that families and communities spend approximately $56 billion in healthcare due to ACE-related health issues. Data also shows the influence of family resiliency on seeking mental health treatment or counseling. Those children from a resilient family have a 13% predicted likelihood of having sought mental health treatment in the previous year compared to 21% for those not from a resilient family. Knowing that family resilience could once again (similarly to physical outcomes) lessen the daily impact of mental illness suggests that family resilience gives children/adolescents the ability to use healthy coping mechanisms within challenging conditions. These family coping strategies are internal assets that can not only promote personal growth but also help them flourish within their neighborhoods and communities.
The final research question sought to better understand how family resilience influences the impact of ACEs on school outcomes. The data shows having 0 ACEs predicts a 62% of being an engaged student compared to 54% for those with 1 ACE and only 42% for those with 2 or more ACEs. Family resilience increases the likelihood of being an engaged student. Over the 3 areas of focus, the most significant influence of family resilience relates to school engagement. Students from resilient families are more likely to be fully engaged in school than those from non-resilient families across the ACEs categories. According to Bryan et al. (2020), school–family partnerships can foster educational resilience, and our findings show that family resilience can foster educational engagement in schools. These protective factors, while varying from student to student and family to family, can significantly impact academic and behavioral outcomes. It seems that cultivating positive environmental factors, such as resilience within families and schools, could counteract both academic and behavioral risks in children's and adolescents’ lives.
Limitations
The present study contains limitations that must be considered when interpreting the results. The data analyzed were limited to one dataset (the CAHMI's NSCH) over 4 years. Another noted limitation of this study is that the data are collected via self-report rather than through clinical interviews. There is also the potential for reporting bias inherent in parent-reported survey data and the cross-sectional nature of the dataset, which precludes causal inference. When evaluating implications, unmeasured confounders, such as community-level factors or school climate, that may influence both family resilience and child outcomes should be considered. This study provides empirical evidence on family resilience and ACEs. It also highlights the need for additional research that examines predictors of resilience and ACEs.
Conclusion
Overall, our study's results show that family resilience is an essential factor in achieving better outcomes for children, and its impact is generally consistent across levels of ACEs. The influence on school outcomes demonstrates family resilience is a central factor in producing more fully engaged students regardless of their ACEs. This consistency of our data across our areas of focus is important and reminds us that resilience is a buffer but not a cure. Family resilience is characterized by supportive relationships, adaptability, and healthy communication and can buffer or mitigate some of these adverse effects, but it cannot erase them entirely. The biological and psychological impacts of trauma can persist even in resilient families. Children with more ACEs fare worse across physical health, mental health, and school outcomes, while our findings demonstrate family resilience can mitigate these effects similarly across levels of ACEs.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix 1: Control Variables
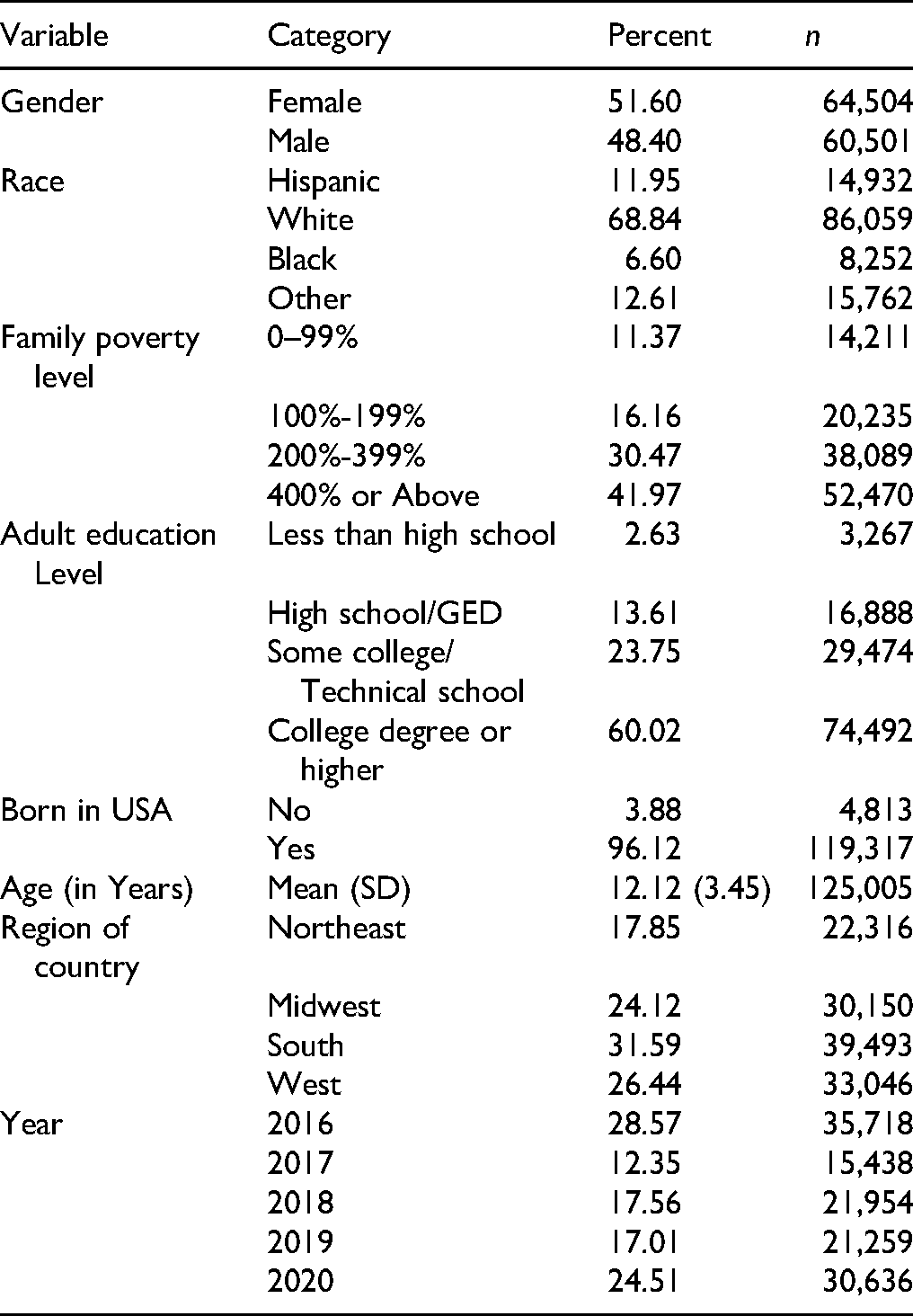
| Variable | Category | Percent | n |
|---|---|---|---|
| Gender | Female | 51.60 | 64,504 |
| Male | 48.40 | 60,501 | |
| Race | Hispanic | 11.95 | 14,932 |
| White | 68.84 | 86,059 | |
| Black | 6.60 | 8,252 | |
| Other | 12.61 | 15,762 | |
| Family poverty level | 0–99% | 11.37 | 14,211 |
| 100%-199% | 16.16 | 20,235 | |
| 200%-399% | 30.47 | 38,089 | |
| 400% or Above | 41.97 | 52,470 | |
| Adult education Level | Less than high school | 2.63 | 3,267 |
| High school/GED | 13.61 | 16,888 | |
| Some college/Technical school | 23.75 | 29,474 | |
| College degree or higher | 60.02 | 74,492 | |
| Born in USA | No | 3.88 | 4,813 |
| Yes | 96.12 | 119,317 | |
| Age (in Years) | Mean (SD) | 12.12 (3.45) | 125,005 |
| Region of country | Northeast | 17.85 | 22,316 |
| Midwest | 24.12 | 30,150 | |
| South | 31.59 | 39,493 | |
| West | 26.44 | 33,046 | |
| Year | 2016 | 28.57 | 35,718 |
| 2017 | 12.35 | 15,438 | |
| 2018 | 17.56 | 21,954 | |
| 2019 | 17.01 | 21,259 | |
| 2020 | 24.51 | 30,636 |