
Abstract
The authors present the first report of extramedullary hematopoiesis occurring in association with an epithelioid hemangioendothelioma. A 64-year-old man sought medical attention for upper chest pain. CT evaluation identified a 2.8-cm mass involving the right hemithorax in the area of the right upper lobe and superior vena cava. A biopsy revealed the presence of an epithelioid malignant vascular neoplasm, which on subsequent resection was found to be an epithelioid hemangioendothelioma. The neoplasm was closely associated with an area of extramedullary hematopoiesis. VEGF immunohistochemical staining of the neoplasm revealed a ring of intensely positive staining cells around the periphery of the area of extramedullary hematopoiesis. This finding provides evidence for the role of aberrant VEGF expression in neoplasm-induced extramedullary hematopoiesis. This report discusses possible mechanisms by which extramedullary hematopoiesis may occur in vascular neoplasms.
Introduction
Extramedullary hematopoiesis has been observed in close association with vascular neoplasms ranging from low-grade vascular neoplasms such as hemangiomas 1 and hemangioblastomas2,3 to high-grade vascular neoplasms such as angiosarcomas. 4 However, extramedullary hematopoiesis has not previously been described in association with an epithelioid hemangioendothelioma.
Epithelioid hemangioendotheliomas are considered to be vascular neoplasms with metastatic potential. They can occur at any age 5 and are usually found associated with veins. They occur principally in the soft tissue, lungs, liver, and bones. Microscopically, they consist of short cords and nests of epithelioid endothelial cells with eosinophilic cytoplasms embedded within a myxohyaline matrix.
In the following report, we describe for the first time a case of extramedullary hematopoiesis occurring in close association with an epithelioid hemangioendothelioma.
Case Report
A 64-year-old man of Indian descent presented with a 4-day history of upper chest pain that was refractory to analgesic medications. His medical and surgical histories were remarkable for hypertension, for which he was being treated with amlodipine and atenolol, and appendectomy for acute appendicitis. His initial workup included PET and CT evaluations, which revealed a 2.8 cm mass involving the right hemithorax in the area of the right upper lobe and superior vena cava. Pulmonary function testing as well as fiberoptic bronchoscopy revealed no significant abnormalities. The patient then underwent a thoracotomy which identified a 4 cm × 3 cm lobulated superior mediastinal mass emanating from the junction of the superior vena cava and inominate vein. This neoplasm completely encompassed the phrenic nerve and was initially thought to be unresectable. A portion was removed for biopsy, which revealed an epithelioid malignant vascular neoplasm with associated extramedullary hematopoiesis. Then, 4 months subsequent to this, the patient underwent an en bloc resection at the University of Maryland Medical Center where the neoplasm was removed. The surgery involved removal of a portion of the superior vena cava and portions of the mediastinum and lung. Postoperatively the patient’s hospital course was unremarkable, and he was discharged on the sixth day following the procedure.
Materials and Methods
The use of paraffin blocks for this study meets Institutional Review Board and Health Insurance Portability and Accountability Act requirements and has been approved by the Institutional Review Board at the University of Maryland Protocol Number H-29227. The patient’s medical records, including his admission note, progress notes, and laboratory data, were reviewed and analyzed. Resected tissue was fixed in 10% buffered formalin and embedded in paraffin. From this, 5-µm thick tissue sections were cut, and these were stained with hematoxylin and eosin (H&E).
Immunohistochemistry
Immunohistochemical staining was performed using a Ventana ES automated immunostainer (Ventana Biotek, Tucson, AZ), using a streptavidin–biotin–peroxidase detection system. Commercially supplied monoclonal antibodies against CD31, CD34, CD117, and myeloperoxidase were used (Ventana Biotek, Tucson, AZ). VEGF immunohistochemical staining was performed by Laboratory Corporation of America (Labcorp, Burlington, NC) using an anti-VEGF monoclonal antibody (VG-1 clone) from Invitrogen (Camarillo, USA).
Results
Gross Pathological Findings
Macroscopically, the specimen consisted of a 38-g segment of mediastinum and attached lung tissue. The mediastinal portion of the specimen measured 6.5 × 3.5 × 3.5 cm3, and the lung tissue portion measured 4.5 × 1.8 × 1.4 cm3. The specimen was significant for a roughly spherical, tan, firm neoplasm measuring 3.8 × 2.8 × 2.5 cm3. Serial sectioning of the neoplasm revealed that it contained a mixture of fleshy, tan-pink tissue and tan-white fibrotic appearing tissue. The neoplasm approached to within less than 0.1 cm of the nearest mediastinal surgical margin grossly and did not involve the pulmonary tissue.
Light Microscopic Appearance
Microscopically, routine H&E sections from the neoplasm showed the presence of a poorly circumscribed vascular neoplasm consisting of plump, moderately pleomorphic epithelioid cells, with high nuclear to cytoplasm ratios (Figure 1). Some of these neoplastic cells contained cytoplasmic vacuoles, which occasionally formed intracellular vascular channels containing red blood cells (Figure 1). The neoplastic cells lay within a stroma that varied from myxoid to hyalinized in appearance (Figure 2). Embedded within the neoplasm were multiple islands of extramedullary hematopoiesis (Figures 3A and 3B).
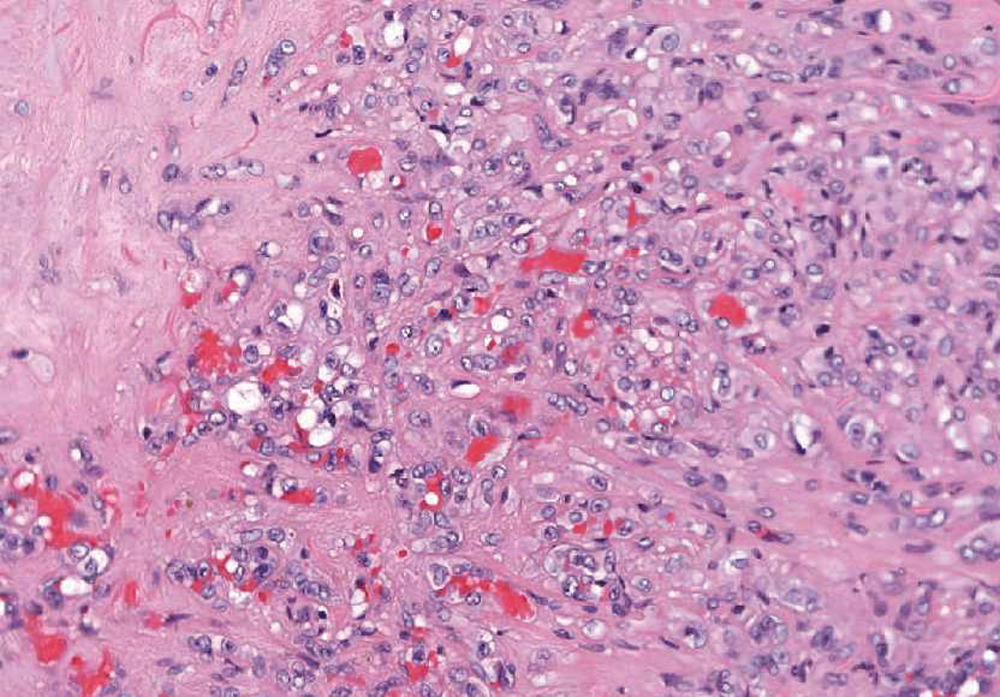
Routine hematoxylin and eosin section from the neoplasm showing the presence of a poorly circumscribed vascular tumor consisting of plump, moderately pleomorphic epithelioid cells
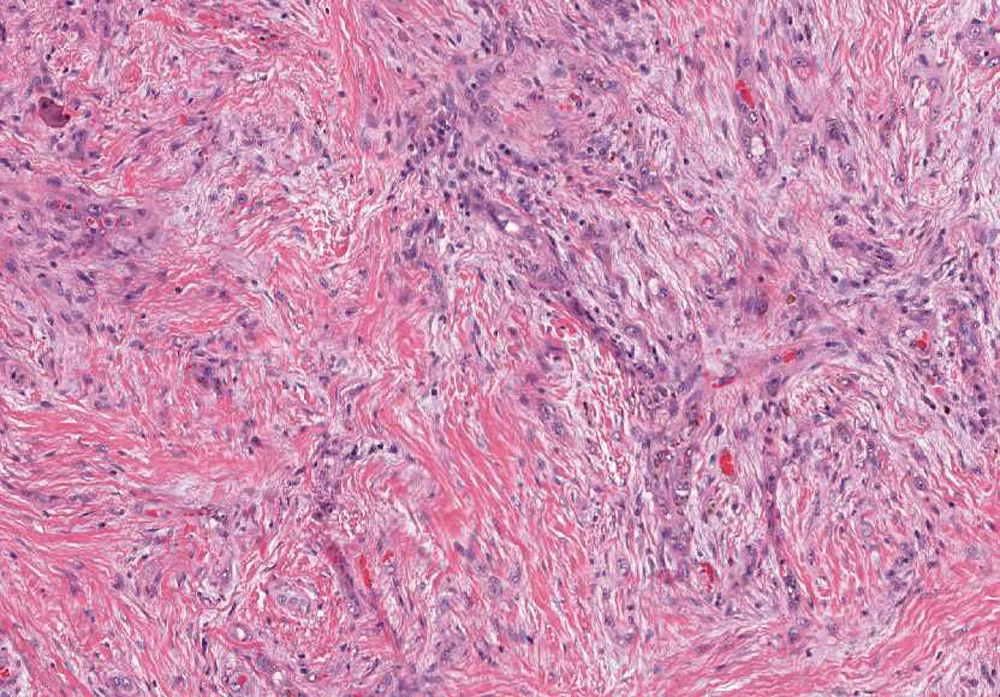
Routine hematoxylin and eosin section from the neoplasm showing the presence of a stroma that varies from myxoid to hyalinized in appearance
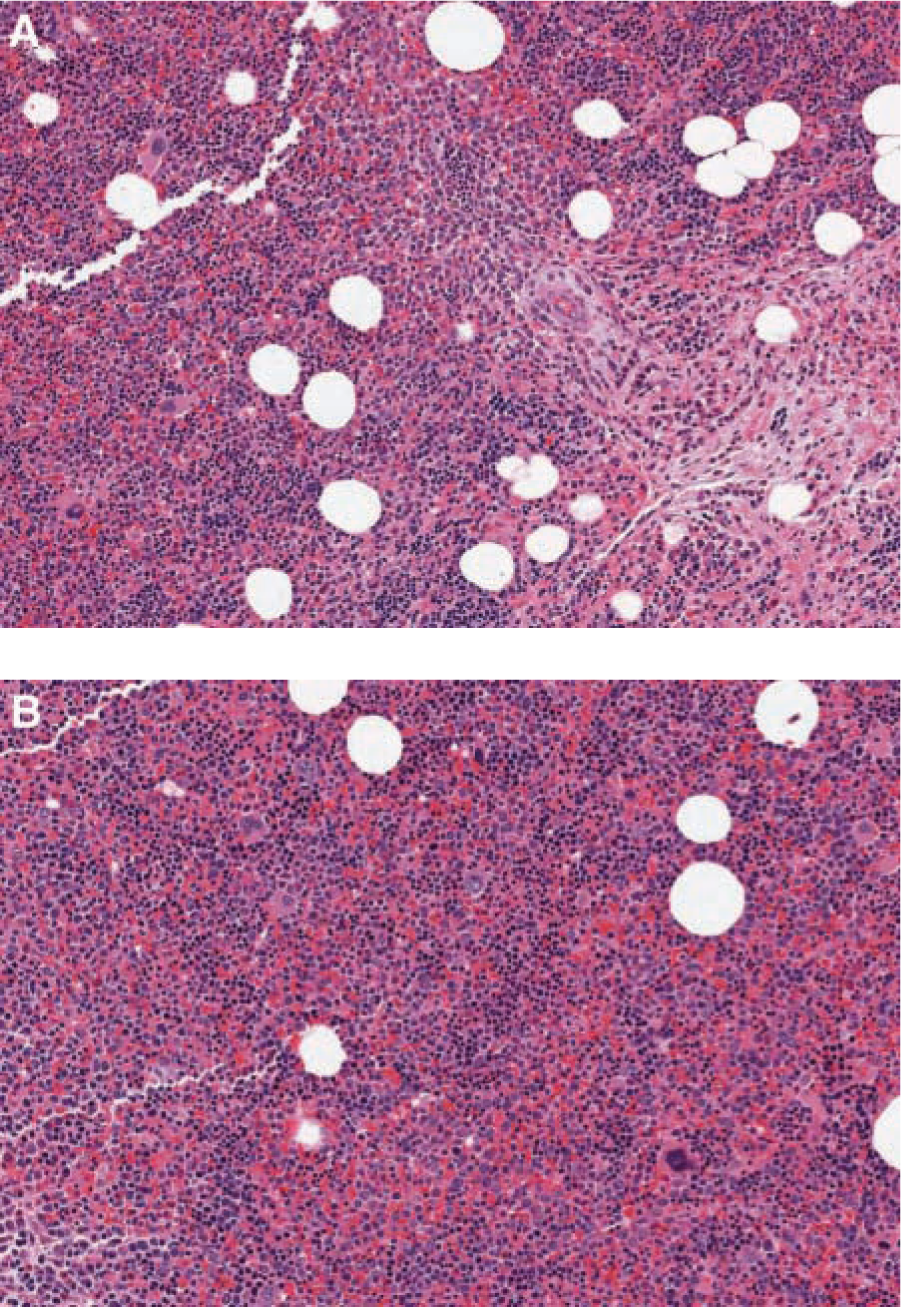
A. Routine hematoxylin and eosin (H&E) section showing the presence of an area of extramedullary hematopoiesis (left) in close association with neoplastic cells (lower right). B. Routine H&E section showing the area of extramedullary hematopoiesis in isolation
Immunohistochemistry
CD31 and CD34 staining were performed revealing strong cytoplasmic staining of neoplastic cells (Figures 4A and 4B, respectively). The neoplasm was diagnosed as an epithelioid hemangioendothelioma. VEGF staining of the neoplasm revealed patchy positive staining that was most intense immediately adjacent to the area of extramedullary hematopoiesis and formed a ring surrounding the hematopoietic area (Figure 5). Immunohistochemical staining was also performed to study the area of extramedullary hematopoiesis. These stains confirmed that this area was composed of a mixed population of hematopoietic cells. Myeloid areas stained with myeloperoxidase (Figure 6A), hematopoietic stem cells (HSCs) and basophils stained with CD117 (Figure 6B), megakaryocytes and endothelial cells stained with CD31 (Figure 6C), and HSCs and endothelial cells stained with CD34 (Figure 6D).
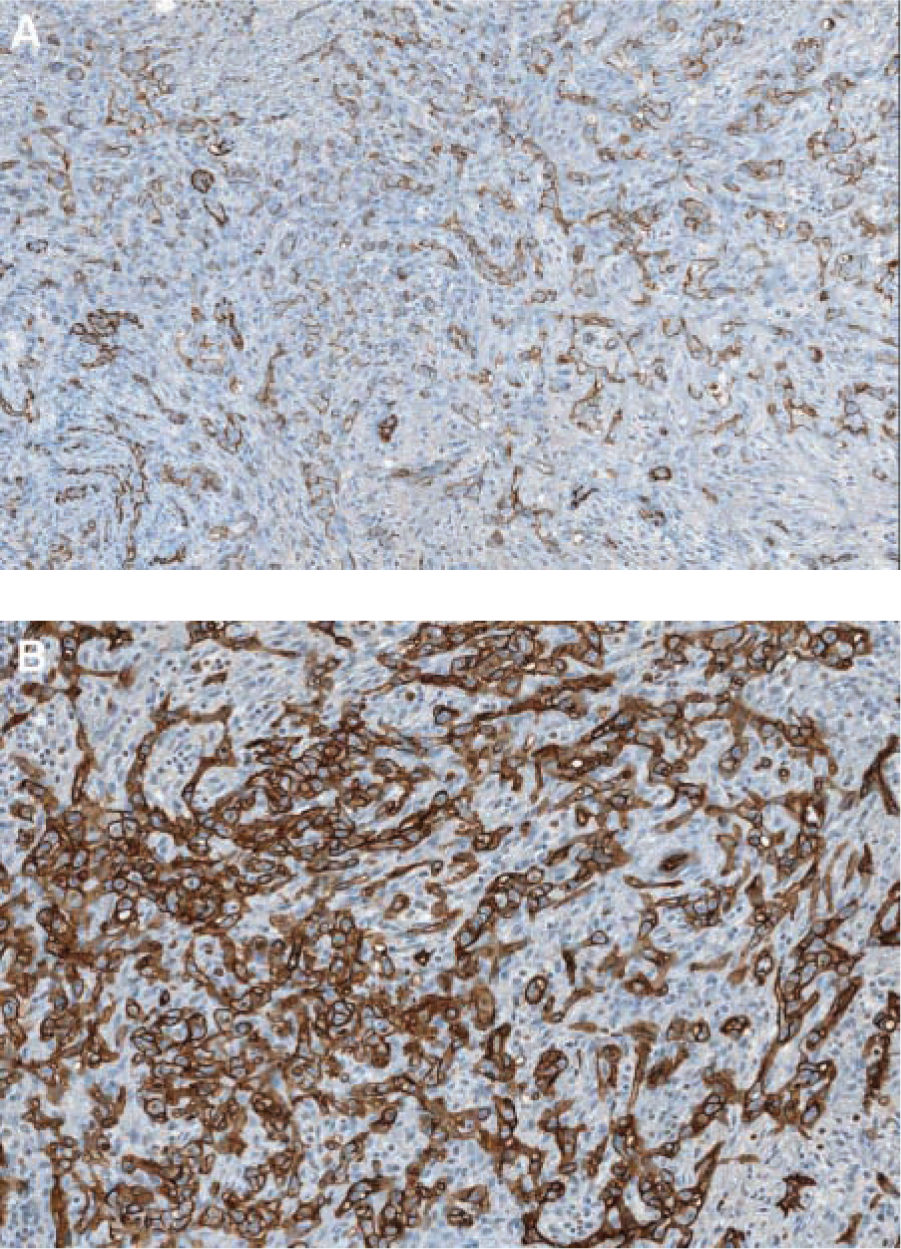
Immunohistochemical stains of the neoplasm: the figure shows positive staining for both CD31 (A) and CD34 (B)
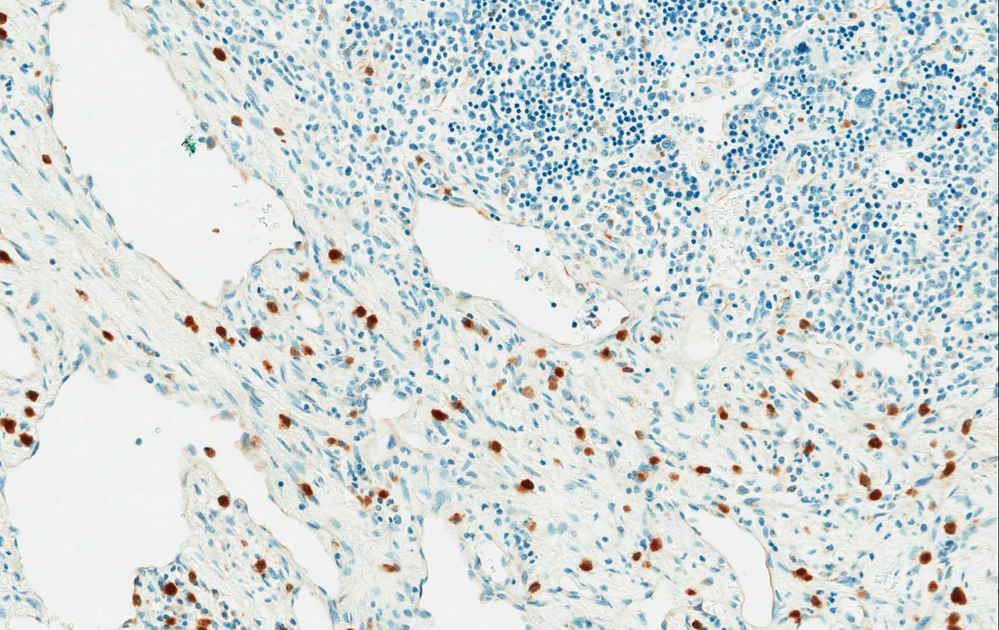
VEGF stain of the neoplasm: this figure shows that the area of hematopoiesis (upper right) is surrounded by a ring of neoplastic cells that stain intensely with VEGF
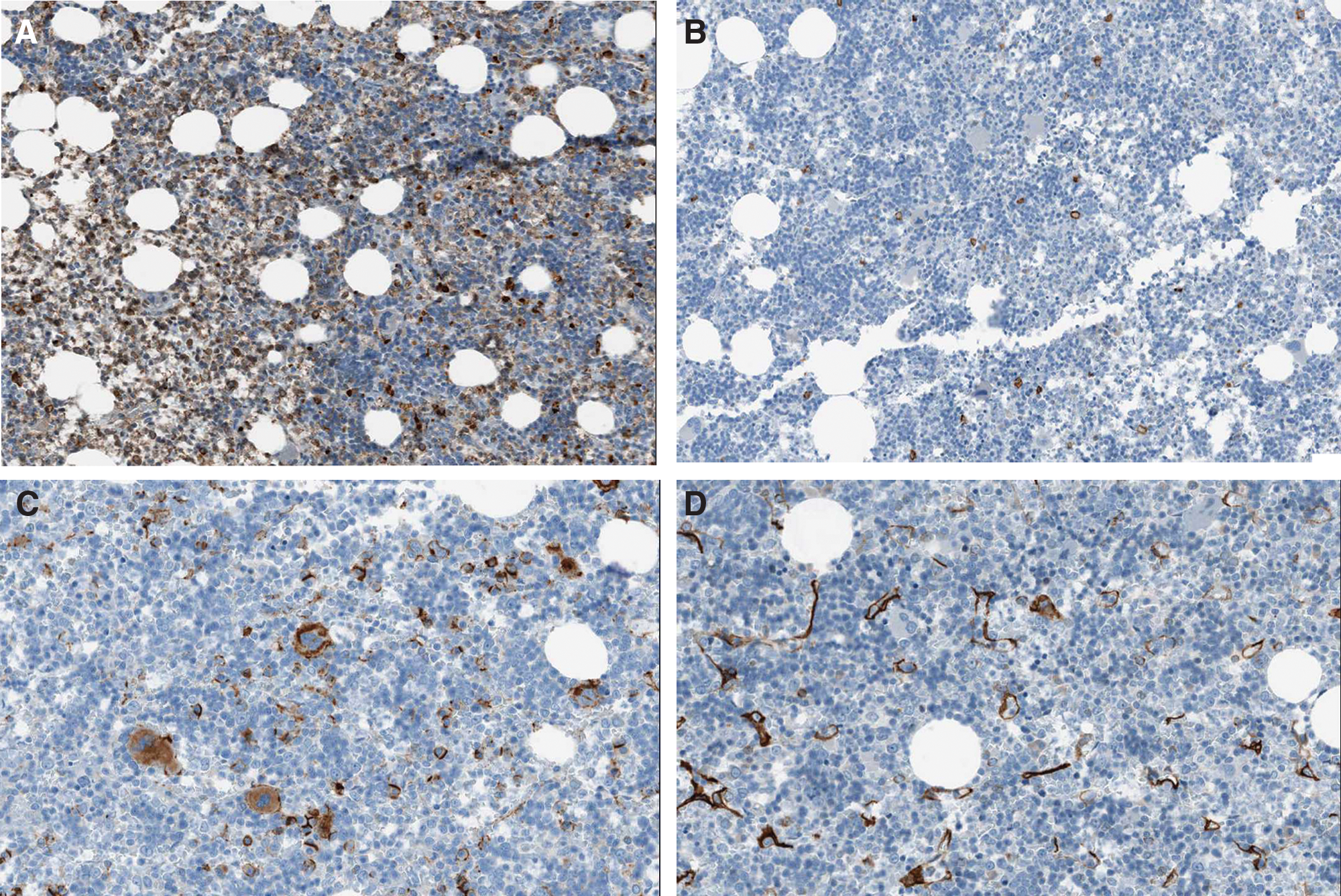
A. Myeloperoxidase stain showing intense staining of a myeloid predominant area (left) with only focal staining of an erythroid predominant area (right). B. CD117 staining of hematopoietic stem cells and basophils. C. CD31 staining of megakaryocytes and endothelial cells. D. CD34 staining of hematopoietic stem cells and endothelial cells
Discussion
The presence of extramedullary hematopoietic tissue in close association with neoplastic cells has been observed for a variety of vascular and nonvascular neoplasms. These include hemangiomas, 1 hemangioblastomas,2,3 and angiosarcomas. 4 Various theories have been proposed to explain the association between neoplasms and extramedullary hematopoiesis. 6 These include direct extension of hematopoietic cells from neighboring marrow cavities, hematopoietic differentiation of multipotent mesenchymal neoplastic cells, or recruitment of HSCs by growth factors produced by the neoplasm and stimulation of these HSCs to proliferate and differentiate. The first of these possibilities seems unlikely in the present case because no bone tissue was found associated with the areas of extramedullary hematopoiesis. The second possibility, that of the presence of hemangioblasts or some other type of stem cells within the neoplasm, may be relevant to the frequently observed extramedullary hematopoiesis that occurs in association with hemangioblastomas.7,8 However, a neoplasm composed of hemangioblasts or some other type of stem cells would be expected to be composed of poorly differentiated mesenchymal cells, 8 as opposed to the moderately differentiated epithelioid cells observed in this case. Therefore, this possibility also appears to be unlikely.
The final possibility, that HSCs were recruited to the site of the mediastinal neoplasm and proliferated as a result of growth factors secreted by the neoplasm appears to be the most likely explanation in this case. The specific growth factor that is most commonly associated with neoplasm-induced extramedullary hematopoiesis is VEGF. VEGF mRNA is substantially upregulated in most solid neoplasms 9 and especially in vascular neoplasms such as epithelioid hemangioendotheliomas.10,11 In fact, VEGF levels are the most specific growth factors for endothelial cell neoplasms and have been suggested as a surrogate marker for monitoring the efficacy of therapy in hemangioendotheliomas. 11 Elevated VEGF levels are associated with HSC mobilization from the bone marrow to the source of production.12,13 In addition, elevated VEGF levels cause HSC proliferation. 14 Finally, elevated VEGF levels, either on their own or in conjunction with other cytokines such as Ang-1, cause extramedullary hematopoiesis.12,13,15
In the present study, we have identified an area of extramedullary hematopoiesis in close association with an epithelioid hemangioendothelioma and have shown that the hematopoietic area is ringed by cells expressing high levels of VEGF. These findings are therefore in accordance with those cited earlier12,13,15 and provide further evidence for the role of aberrant VEGF expression in neoplasm-induced extramedullary hematopoiesis.
HSC differentiation is often disturbed in cancer patients. This is obviously most pronounced in patients with hematopoietic malignancies such as leukemias. However, it also occurs in a wide range of nonhematopoietic malignancies (reviewed in Podar and Anderson 16 ). It is believed that VEGF plays a crucial role in the dysregulation of hematopoiesis that occurs in cancer patients.15,16 Future studies of the role of VEGF in hematopoiesis will no doubt provide a better understanding of the mechanism by which dysregulation of hematopoiesis occurs and will likely lead to improved therapeutic strategies for cancer patients.
Footnotes
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
These studies were funded in part by the University of Maryland School of Medicine, Department of Pathology.