
Abstract
We present a case of clear cell meningioma with unusual clinical and pathologic features. The patient was a 54-year-old man who underwent laminectomy and durotomy for an intradural tumor in the lumbar spinal canal. Sections showed a predominance of dense collagenous tissue with irregularly shaped and irregularly sized magenta-colored extracellular deposits. On electron microscopy, these deposits were osmiophilic and “petaloid.” The final diagnosis of clear cell meningioma rested on relatively inconspicuous intervening nests of glycogen-containing clear cells that were positive for epithelial membrane antigen. The unusual extracellular deposits seen in this case have previously been characterized as tyrosine-rich crystals of the type most commonly seen in salivary gland tumors. Recognition of this tumor as a clear cell meningioma, despite misleading clinical features and initially challenging histologic findings, is not only a matter of diagnostic accuracy but also imparts important prognostic information.
Case Report
The patient was a 54-year-old man with a 2-year history of back and right leg pain. Magnetic resonance imaging of the lumbar spine showed a tumor in the spinal canal at the level of L3–L4 (Figure 1A). This was described as intradural, well-defined, and homogeneously enhancing; it extended along the right L4 nerve root with some bony remodeling of the L4–L5 neural foramen. Over 7 months, the tumor grew 5 mm to a maximum dimension of 4 cm. The favored radiologic diagnosis was schwannoma. The patient underwent L3–L4 laminectomy and durotomy for resection of the tumor.
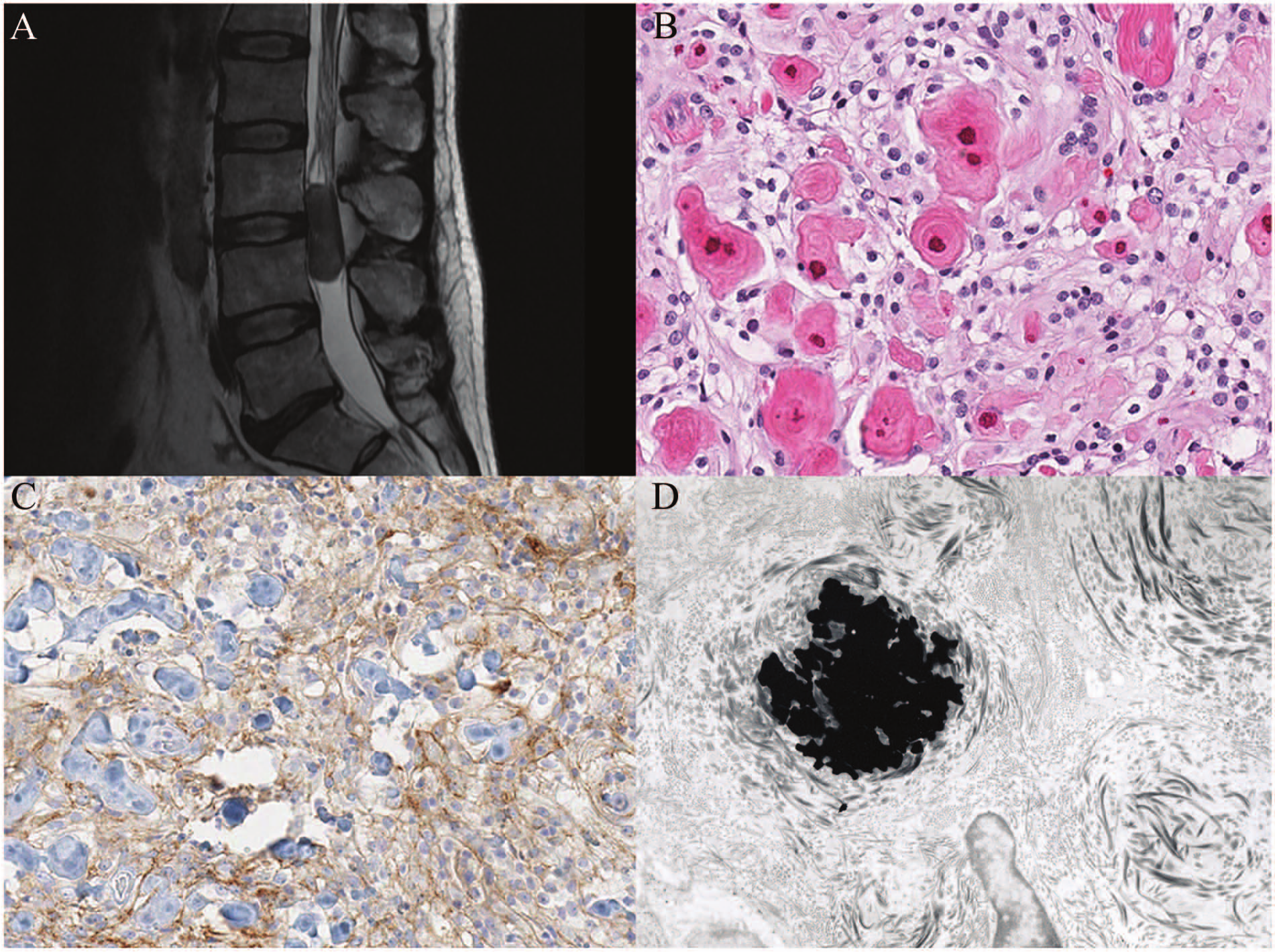
A, Sagittal T2-weighted magnetic resonance image of the lumbar neoplasm. B, Collagen knots and clusters of clear cells (hematoxylin and eosin, 200×). C, Cell surface immunoreactivity for epithelial membrane antigen (200×). D, Electron micrograph showing osmiophilic petaloid deposits.
Pathological Findings
Intraoperative cytologic and frozen section assessment of a portion of the mass showed hypocellular collagenous tissue with no diagnostic cells.
Permanent sections showed a neoplasm with multiple components. Most prominently, there were expanses of dense collagenous tissue arranged in broad bands or small concentric “knots” (Figure 1B). Many of the knots contained irregularly shaped and irregularly sized magenta-colored extracellular deposits. These were negative for calcium by von Kossa stain. There were intervening cellular nests with variably sized round to oval nuclei with variable chromatin density. The pale or clear cytoplasm contained glycogen, as demonstrated by periodic acid–Schiff stain with and without diastase. Cells had membranous positivity for epithelial membrane antigen by immunohistochemistry (Figure 1C). There were no mitotic figures but scattered Ki-67-positive cells.
On electron microscopy, the cells showed interdigitating cell processes and large pale nuclei. There was extensive whorled collagen deposition and the extracellular deposits were osmiophilic and “petaloid” without distinguishable internal structure (Figure 1D).
Discussion
The final diagnosis of clear cell meningioma was based on the clear, glycogen-containing cytoplasm and epithelial membrane antigen positivity. The prominent collagenous stroma is a sclerotic pattern well known in clear cell meningioma, and can predominate over the neoplastic cells.
The unique feature of the present case was the abundance of extracellular deposits. These unusual structures have previously been characterized ultrastructurally only in fibrous meningioma, where they were concluded to represent tyrosine-rich crystals of the type most commonly seen in salivary gland tumors. 1 A case nearly identical to the present one is used to illustrate the sclerotic pattern of clear cell meningioma in the American Forces Institute of Pathology fascicle on central nervous system tumors, although that reference does not provide electron microscopic correlation.2(p343)
Finally, and most misleading clinically, this lesion presented as a nondural-based lumbar spinal tumor. This is an unusual presentation for most types of meningioma but is relatively more common and well documented for the clear cell variant. 3
Recognition of this tumor as a clear cell meningioma, despite misleading clinical features and initially challenging histologic findings, is not only a matter of diagnostic accuracy but also imparts important prognostic information. Clear cell meningioma is defined by the World Health Organization as a grade 2 tumor and has a proclivity to recur belied by its bland appearance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.